
Video-Assisted Thoracoscopy for Vertebral Body Tethering of Juvenile and Adolescent Idiopathic Scoliosis: Tips and Tricks of Surgical Multidisciplinary Management

 and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preoperative Assessment
2.2. Operative Technique
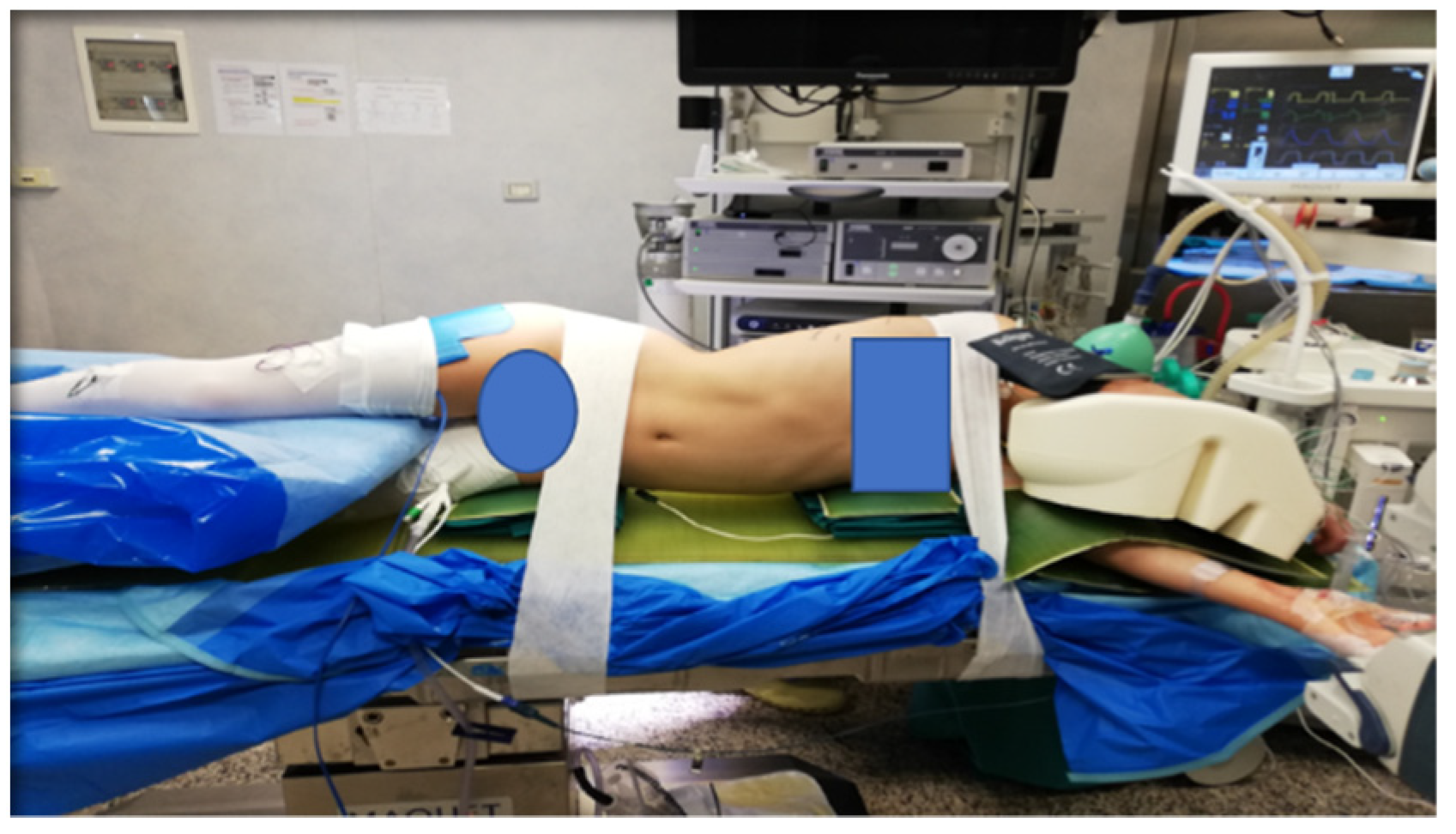
2.2.1. Set-Up
2.2.2. Surgical Technique
2.3. Postoperative Management
3. Results
4. Discussion
Pitfalls, Tips and Tricks
- Adequate trocars positioning is essential in order to correctly place the screws in the vertebral bodies. Fluoroscopy use in anterior and lateral view guides the orthopedist to the correct insertion.
- The risk of bleeding is possible especially near the Azygos vein. The vascular dissection must be delicate and precise, using a bipolar forceps or a thin instrument combined with a bipolar coagulation device. The parietal pleura must be incised carefully along the marginal spine and a good exposure of the veins must be achieved. Small branches of the paravertebral veins need accurate hemostasis.
- Lesion of the phrenic nerve must be avoided, through a proper exposure and visualization of its course.
- The thoracic duct must be soon identified and avoided.
- Keep in mind any possible anatomic variations of the vascular, nerve and thoracic duct conformation and course.
- A correct interaction between pediatric and orthopedic surgeon, integrated by the combined use of thoracoscopic visualization and fluoroscopy, allow the orthopedist to correctly position the devices at the level of the vertebrae to be treated.
- The presence of a pediatric surgeon with advanced skills in thoracoscopic technique is required. This type of procedure should only be carried out in a third-level center where different professionals are present: expert radiology staff, pediatric orthopedist, pediatric thoracic surgeon, pediatric anesthetist, neurologist, expert physiotherapist.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Konieczny, M.R.; Senyurt, H.; Krauspe, R. Epidemiology of adolescent idiopathic scoliosis. J. Child Orthop. 2013, 7, 3–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altaf, F.; Gibson, A.; Dannawi, Z.; Noordeen, H. Adolescent idiopathic scoliosis. BMJ 2013, 346, f2508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinstein, S.L.; Dolan, L.A.; Cheng, J.C.; Danielsson, A.; Morcuende, J.A. Adolescent idiopathic scoliosis. Lancet 2008, 371, 1527–1537. [Google Scholar] [CrossRef] [Green Version]
- Hoernschemeyer, D.G.; Boeyer, M.E.; Robertson, M.E.; Loftis, C.M.; Worley, J.R.; Tweedy, N.M.; Gupta, S.U.; Duren, D.L.; Holzhauser, C.M.; Ramachandran, V.M. Anterior vertebral body tethering for adolescent scoliosis with growth remaining: A retrospective review of 2 to 5-year postoperative results. J. Bone Joint Surg. Am. 2020, 102, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Newton, P.O.; Bartley, C.E.; Bastrom, T.P.; Kluck, D.G.; Saito, W.; Yaszay, B. Anterior spinal growth modulation in skeletally immature patients with idiopathic scoliosis: A comparison with posterior spinal fusion at 2 to 5 years postoperatively. J. Bone Joint Surg. Am. 2020, 102, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Baker, C.E.; Milbrandt, T.A.; Larson, A.N. Anterior vertebral body tethering for adolescent idiopathic scoliosis: Early results and future directions. Orthop. Clin. N. Am. 2021, 52, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Yucekul, A.; Akpunarli, B.; Durbas, A.; Zulemyan, T.; Havlucu, I.; Ergene, G.; Senay, S.; Yalinay Dikmen, P.; Turgut Balci, S.; Karaarslan, E.; et al. Does vertebral body tethering cause disc and facet joint degeneration? A preliminary MRI study with minimum two years follow-up. Spine J. 2021, 21, 1793–1801. [Google Scholar] [CrossRef] [PubMed]
- Helenius, I.J. Standard and magnetically controlled growing rods for the treatment of early onset scoliosis. Ann. Transl. Med. 2020, 8, 26. [Google Scholar] [CrossRef] [PubMed]
- Bekmez, S.; Dede, O.; Yazici, M. Advances in growing rods treatment for early onset scoliosis. Curr. Opin. Pediatr. 2017, 29, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Crawford, C.H.; Lenke, L.G. Growth modulation by means of anterior tethering resulting in progressive correction of juvenile idiopathic scoliosis: A case report. J. Bone Joint Surg. Am. 2010, 92, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Joshi, V.; Cassivi, S.D.; Milbrandt, T.A.; Larson, A.N. Video-assisted thoracoscopic anterior vertebral body tethering for the correction of adolescent idiopathic scoliosis of the spine. Eur. J. Cardiothorac. Surg. 2018, 54, 1134–1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parent, S.; Shen, J. Anterior vertebral body growth-modulation tethering in idiopathic scoliosis: Surgical technique. J. Am. Acad. Orthop. Surg. 2020, 28, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Samdani, A.F.; Ames, R.J.; Kimball, J.S.; Pahys, J.M.; Grewal, H.; Pelletier, G.J.; Betz, R.R. Anterior vertebral body tethering for immature adolescent idiopathic scoliosis: One-year results on the first 32 patients. Eur. Spine J. 2015, 24, 1533–1539. [Google Scholar] [CrossRef] [PubMed]
- Ergene, G. Early-term postoperative thoracic outcomes of videothoracoscopic vertebral body tethering surgery. Turk Gogus Kalp Damar Cerrahisi Derg. 2019, 27, 526–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stokes, I.A.; Spence, H.; Aronsson, D.D.; Kilmer, N. Mechanical modulation of vertebral body growth. Implications for scoliosis progression. Spine 1996, 21, 1162–1167. [Google Scholar] [CrossRef] [PubMed]
- Mehlman, C.T.; Araghi, A.; Roy, D.R. Hyphenated history: The Hueter-Volkmann law. Am. J. Orthop. 1997, 26, 798–800. [Google Scholar] [PubMed]
- Bonsignore-Opp, L.; Murphy, J.; Skaggs, D.; Cahill, P.; Blakemore, L.; Parent, S.; Samdani, A.; St. Hilaire, T.; Vitale, M. Growth modulation for childhood scoliosis: Where have we come from and where are we going? JPOSNA 2019, 1, 1–8. [Google Scholar]
- Miyanji, F.; Pawelek, J.; Nasto, L.A.; Rushton, P.; Simmonds, A.; Parent, S. Safety and efficacy of anterior vertebral body tethering in the treatment of idiopathic scoliosis. Bone Joint J. 2020, 102-B, 1703–1708. [Google Scholar] [CrossRef] [PubMed]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costanzo, S.; Pansini, A.; Colombo, L.; Caretti, V.; Popovic, P.; Lanfranchi, G.; Camporesi, A.; Pelizzo, G. Video-Assisted Thoracoscopy for Vertebral Body Tethering of Juvenile and Adolescent Idiopathic Scoliosis: Tips and Tricks of Surgical Multidisciplinary Management. Children 2022, 9, 74. https://doi.org/10.3390/children9010074
Costanzo S, Pansini A, Colombo L, Caretti V, Popovic P, Lanfranchi G, Camporesi A, Pelizzo G. Video-Assisted Thoracoscopy for Vertebral Body Tethering of Juvenile and Adolescent Idiopathic Scoliosis: Tips and Tricks of Surgical Multidisciplinary Management. Children. 2022; 9(1):74. https://doi.org/10.3390/children9010074
Chicago/Turabian StyleCostanzo, Sara, Andrea Pansini, Luca Colombo, Valentina Caretti, Petar Popovic, Giulia Lanfranchi, Anna Camporesi, and Gloria Pelizzo. 2022. "Video-Assisted Thoracoscopy for Vertebral Body Tethering of Juvenile and Adolescent Idiopathic Scoliosis: Tips and Tricks of Surgical Multidisciplinary Management" Children 9, no. 1: 74. https://doi.org/10.3390/children9010074