
Nasal Cannula with Long and Narrow Tubing for Non-Invasive Respiratory Support in Preterm Neonates: A Systematic Review and Meta-Analysis
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
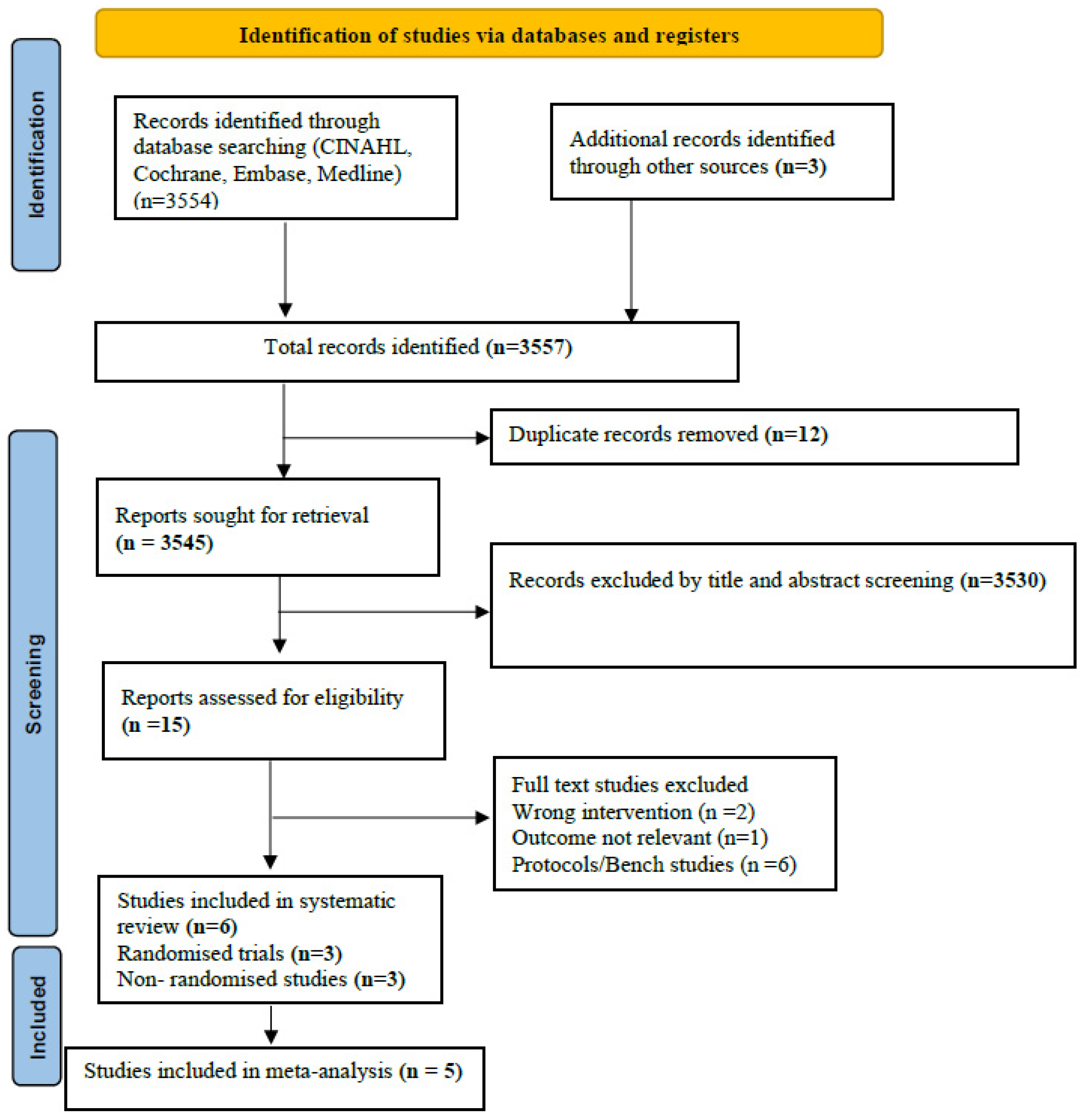
2.1. Literature Search
2.2. Inclusion Criteria
- Intervention: CLNT
- Comparators: SBP or NM
2.3. Outcomes
2.3.1. Primary Outcome
2.3.2. Secondary Outcomes
- Clinical outcomes: receipt of surfactant therapy, air leak (as defined by authors), nasal trauma occurring at any time until the discontinuation of respiratory support (any grade and severity, as defined by the authors), and duration of IMV and NRS (days).
- Surrogate outcomes: pressure transmission at the level of the pharynx or esophagus and the work of breathing (using an objective and validated scoring technique).
2.4. Data Extraction, Data Synthesis, and Quality of Evidence
2.5. Risk-of-Bias (RoB) Assessment
2.6. Certainty of Evidence (CoE) Assessment
2.7. Subgroup Analysis
- i.
- type of NRS: NCPAP vs. NIPPV
- ii.
- indication for NRS: primary, post-extubation, or both
3. Results
3.1. RoB of the Included Studies
3.2. Outcomes from Randomised Trials
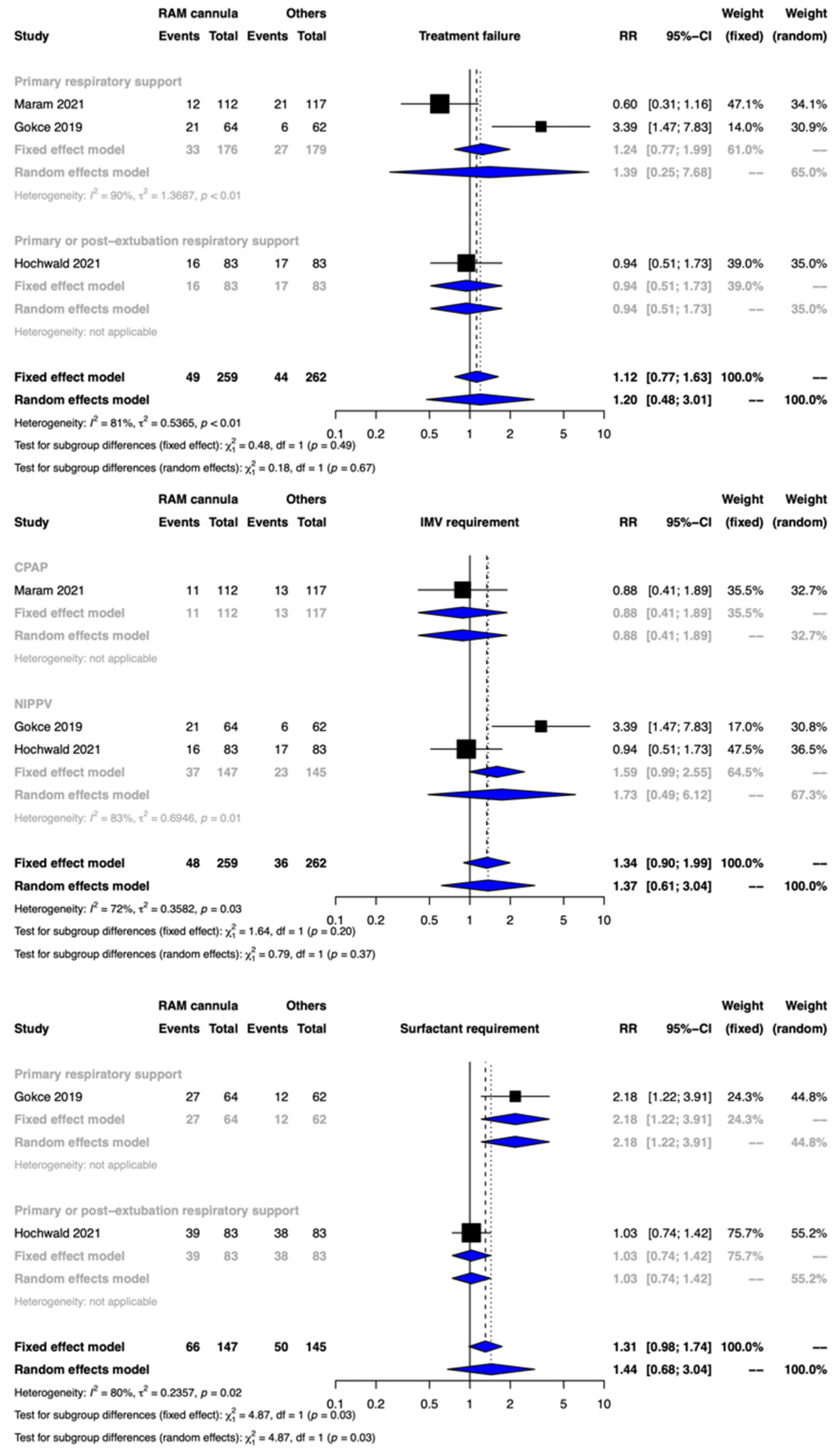
3.2.1. Primary Outcomes
Treatment Failure
Need for IMV
3.3. Secondary Outcomes
3.3.1. Nasal Trauma
3.3.2. Surfactant Treatment
3.3.3. Duration of IMV
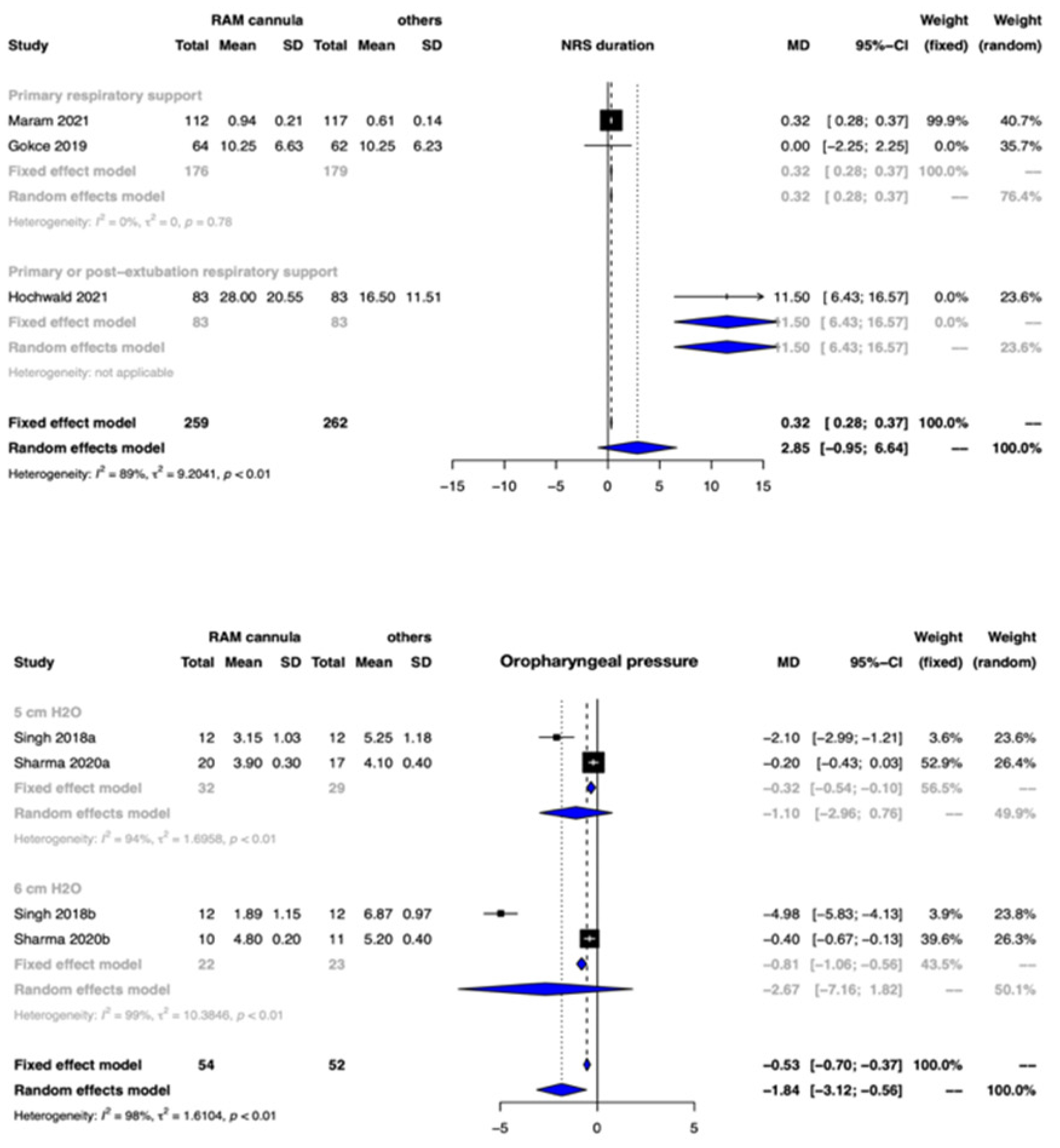
3.3.4. Duration of NRS
3.3.5. Air Leak
3.3.6. Work of Breathing (Using Objective and Validated Scoring Technique) and Pressure Transmission (at the Level of Pharynx or Oesophagus)
3.4. Outcomes from Non-Randomised Trials
3.4.1. Primary Outcomes
Primary Outcomes
Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ramaswamy, V.V.; Bandyopadhyay, T.; Nanda, D.; Bandiya, P.; More, K.; Oommen, V.I.; Gupta, A. Efficacy of noninvasive respiratory support modes as postextubation respiratory support in preterm neonates: A systematic review and network meta-analysis. Pediatr. Pulmonol. 2020, 55, 2924–2939. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.J.; Polin, R.A.; Committee on Fetus and Newborn; American Academy of Pediatrics. Non-invasive respiratory support. Pediatrics 2016, 137, e20153758. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.J.; Subramaniam, P.; Davis, P.G. Continuous positive airway pressure (CPAP) for respiratory distress in preterm neonates. Cochrane Database Syst. Rev. 2020, 10, CD002271. [Google Scholar] [PubMed]
- Bailes, S.A.; Firestone, K.S.; Dunn, D.K.; McNinch, N.L.; Brown, M.F.; Volsko, T.A. Evaluating the effect of flow and interface type on pressures delivered with bubble CPAP in a simulated model. Respir. Care 2016, 61, 333–339. [Google Scholar] [CrossRef]
- Bashir, T.; Murki, S.; Kiran, S.; Reddy, V.K.; Oleti, T.P. ‘Nasal mask’ in comparison with ‘nasal prongs’ or ‘rotation of nasal mask with nasal prongs’ reduces the incidence of nasal injury in preterm neonates supported on nasal continuous positive airway pressure (nCPAP): A randomized controlled trial. PLoS ONE 2019, 14, e0211476. [Google Scholar] [CrossRef]
- De Bonfim, S.F.S.F.; de Vasconcelos, M.G.L.; de Sousa, N.F.C.; da Silva, D.V.C.; Leal, L.P. Nasal septum injury in preterm neonates using nasal prongs. Rev. Lat. Am. Enfermagem. 2014, 22, 826–833. [Google Scholar] [CrossRef]
- Fujii, K.; Sugama, J.; Okuwa, M.; Sanada, H.; Mizokami, Y. Incidence and risk factors of pressure ulcers in seven neonatal intensive care units in Japan: A multisite prospective cohort study. Int. Wound J. 2010, 7, 323–328. [Google Scholar] [CrossRef]
- Ota, N.T.; Davidson, J.; Guinsburg, R. Early nasal injury resulting from the use of nasal prongs in preterm neonates with very low birth weight: A pilot study. Rev. Bras. Ter. Intensiva 2013, 25, 245–250. [Google Scholar] [CrossRef]
- Yong, S.C.; Chen, S.J.; Boo, N.Y. Incidence of nasal trauma associated with nasal prong versus nasal mask during continuous positive airway pressure treatment in very low birthweight neonates: A randomised control study. Arch. Dis. Child. Fetal Neonatal Ed. 2005, 90, F480–F483. [Google Scholar] [CrossRef]
- Ottinger, D.; Hicks, J.; Wilson, S.; Sperber, K.; Power, K. The pressure is on! Neonatal skin and nasal continuous positive airway pressure. Adv. Neonatal Care Off. J. Natl. Assoc. Neonatal Nurses 2016, 16, 420–423. [Google Scholar] [CrossRef]
- Imbulana, D.I.; Manley, B.J.; Dawson, J.A.; Davis, P.G.; Owen, L.S. Nasal injury in preterm neonates receiving non-invasive respiratory support: A systematic review. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F29–F35. [Google Scholar] [CrossRef]
- Nzegwu, N.I.; Mack, T.; DellaVentura, R.; Dunphy, L.; Koval, N.; Levit, O.; Bhandari, V. Systematic use of the RAM nasal cannula in the Yale-New Haven Children’s Hospital Neonatal Intensive Care Unit: A quality improvement project. J. Matern. Fetal Neonatal Med. 2015, 28, 718–721. [Google Scholar] [CrossRef]
- Razak, A.; Patel, W. Nasal mask vs binasal prongs for nasal continuous positive airway pressure in preterm neonates: A systematic review and meta-analysis. Pediatr. Pulmonol. 2020, 55, 2261–2271. [Google Scholar] [CrossRef] [PubMed]
- Ramanathan, R. Nasal respiratory support through the nares: Its time has come. J. Perinatol. 2010, 30, S67–S72. [Google Scholar] [CrossRef]
- Claassen, C.C.; Hillman, N.H.; Brown, K.; Williams, H.L.; Strand, M.L. Comparison of bubble CPAP devices using RAM cannula for extubation failure in very low birth weight neonates: Randomized and cohort studies. Neonatology 2019, 115, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Matlock, D.N.; Bai, S.; Weisner, M.D.; Comtois, N.; Beck, J.; Sinderby, C.; Courtney, S.E. Tidal volume transmission during non-synchronized nasal intermittent positive pressure ventilation via RAM cannula. J. Perinatol. 2019, 39, 723–729. [Google Scholar] [CrossRef]
- Green, E.A.; Dawson, J.A.; Davis, P.G.; de Paoli, A.G.; Roberts, C.T. Assessment of resistance of nasal continuous positive airway pressure interfaces. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 104, F535–F539. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Murki, S.; Maram, S.; Pratap, T.; Kiran, S.; Venkateshwarlu, V.; Dinesh, P.; Kulkarni, D.; Kamineni, B.T.A.; Singh, G. Comparison of delivered distending pressures in the oropharynx in preterm infant on bubble CPAP and on three different nasal interfaces. Pediatr. Pulmonol. 2020, 55, 1631–1639. [Google Scholar] [CrossRef]
- Gerdes, J.S.; Sivieri, E.M.; Abbasi, S. Factors influencing delivered mean airway pressure during nasal CPAP with the RAM cannula. Pediatr. Pulmonol. 2016, 51, 60–69. [Google Scholar] [CrossRef]
- Mukerji, A.; Belik, J. Neonatal nasal intermittent positive pressure ventilation efficacy and lung pressure transmission. J. Perinatol. 2015, 35, 716–719. [Google Scholar] [CrossRef]
- Iyer, N.P.; Chatburn, R. Evaluation of a nasal cannula in noninvasive ventilation using a lung simulator. Respir. Care 2015, 60, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Drescher, G.S.; Hughes, C.W. Comparison of interfaces for the delivery of noninvasive respiratory support to low birthweight neonates. Respir. Care 2018, 63, 1197–1206. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; McNally, M.J.; Darnall, R.A. Does the RAM cannula provide continuous positive airway pressure as effectively as the Hudson prongs in preterm neonates? Am. J. Perinatol. 2019, 36, 849–854. [Google Scholar] [CrossRef] [PubMed]
- Gokce, I.K.; Kaya, H.; Ozdemir, R. A randomized trial comparing the short binasal prong to the RAM cannula for noninvasive ventilation support of preterm neonates with respiratory distress syndrome. J. Matern. Fetal Neonatal Med. 2019, 34, 1868–1874. [Google Scholar] [CrossRef]
- Hochwald, O.; Riskin, A.; Borenstein-Levin, L.; Shoris, I.; Dinur, G.P.; Said, W.; Jubran, H.; Littner, Y.; Haddad, J.; Mor, M.; et al. Cannula with long and narrow tubing versus short binasal prongs for noninvasive ventilation in preterm neonates: Noninferiority randomized clinical trial. JAMA Pediatr. 2021, 175, 36–43. [Google Scholar] [CrossRef]
- Maram, S.; Murki, S.; Nayyar, S.; Kadam, S.; Oleti, T.P.; Anne, R.P.; Deshobhotla, S.; Sharma, D.; Arun, S.; Vadije, P.R. RAM cannula with Cannulaide versus Hudson prongs for delivery of nasal continuous positive airway pressure in preterm neonates: An RCT. Sci. Rep. 2021, 11, 23527. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 10, 89. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. Available online: https://www.R-project.org/ (accessed on 15 August 2022).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.J.; Montori, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE guidelines 6. Rating the quality of evidence—Imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE guidelines: 7. Rating the quality of evidence—Inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Schünemann, H.J.; Tugwell, P.; Knottnerus, A. GRADE guidelines: A new series of articles in the Journal of Clinical Epidemiology. J. Clin. Epidemiol. 2011, 64, 380–382. [Google Scholar] [CrossRef] [PubMed]
- Santesso, N.; Glenton, C.; Dahm, P.; Garner, P.; Akl, E.A.; Alper, B.; Brignardello-Petersen, R.; Carrasco-Labra, A.; de Beer, H.; Hultcrantz, M.; et al. GRADE Working Group. GRADE guidelines 26: Informative statements to communicate the findings of systematic reviews of interventions. J. Clin. Epidemiol. 2020, 119, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Claassen, C.C.; Strand, M.L.; Williams, H.L.; Hillman, N.H. Use of the RAM Cannula with Early Bubble Continuous Positive Airway Pressure Requires Higher Pressures: Clinical and In vitro Evaluations. Am. J. Perinatol. 2021, 38, 1167–1173. [Google Scholar] [CrossRef]
- Chandrasekaran, A.; Thukral, A.; Jeeva Sankar, M.; Agarwal, R.; Paul, V.K.; Deorari, A.K. Nasal masks or binasal prongs for delivering continuous positive airway pressure in preterm neonates-a randomised trial. Eur. J. Pediatr. 2017, 176, 379–386. [Google Scholar] [CrossRef]
- Luistro, C.P.R. Effectiveness of Kangaroo mother care in reducing morbidity and mortality among Preterm Neonates on RAM Cannula continuous positive airway pressure: A randomized controlled trial Pediatrics Healthcare Congress 2020, 15th International Conference on Pediatrics and Neonatal Health. Curr Pediatr Res. 2020, 6, 5. [Google Scholar]
- Conti, G.; Spinazzola, G.; Gregoretti, C.; Ferrone, G.; Cortegiani, A.; Festa, O.; Piastra, M.; Tortorolo, T.; Costa, R. Comparative bench study evaluation of different infant interfaces for non-invasive ventilation. BMC Pulm Med. 2018, 18, 57. [Google Scholar] [CrossRef] [Green Version]
- Providing Nasal Continuous Positive Airway Pressure for Primary Respiratory Support in Preterm Neonates with Respiratory Distress. Available online: https://www.ctri.nic.in/Clinicaltrials/pmaindet2.php?trialid=40220 (accessed on 21 June 2022).
- Neotech RAM Cannula Versus Conventional Binasal Prong Continuous Positive Airway Pressure (CPAP) to Treat Respiratory Distress in Low-Birth-Weight Neonates. Available online: https://clinicaltrials.gov/ct2/show/NCT02168257 (accessed on 21 June 2022).
- Diaphragm Electrical Activity of Preterm Neonates on nCPAP With Binasal Prongs Versus RAM Cannula. Available online: https://Clinicaltrials.Gov/Show/NCT03121781 (accessed on 21 June 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID, Year, Country | Intervention | Comparator | GA (Weeks) Mean ± SD or Median (IQR) | BW (g) Mean ± SD or Median (IQR) | Type of NRS Used | Study Outcomes | Other Comments |
|---|---|---|---|---|---|---|---|
| Maram et al. 2021 India [26] | CPAPwith RAM cannulae with cannulaide | CPAP with short binasal prongs | I: 31.4 ± 1.7 C:31.4 ± 1.6 | I: 1491 ± 321 C: 1531 ± 394 | CPAP as primary respiratory support | Primary outcome: Incidence and severity of nasal injury Secondary outcomes: Nasal injury score at discharge Need for IMV Duration of nasal CPAP Need for change in interface Mortality CPAP failure Culture positive sepsis PDA NEC IVH grade 3 or more Cystic PVL ROP needing laser Supplemental oxygen at 28 days Air leak Transfer to other hospital Discharge from hospital Length of hospital stay Weight at discharge Length at discharge Head circumference at discharge | Inclusion criteria: Neonates between 28 to 34 weeks of gestation, stratified based on GA 28 to 30 weeks and 31 to 34 weeks Exclusion criteria: Neonates who required IMV at admission to NICU; those with poor respiratory efforts or apnea, worsening shock, suspected or proven persistent pulmonary hypertension of newborn, severe metabolic acidosis (pH < 7.20 and base deficit > 10), severe respiratory acidosis (pH < 7.20 and PaCO2 > 60 mm Hg), and massive pulmonary haemorrhage. Neonates with major congenital malformations such as congenital diaphragmatic hernia, tracheo-oesophageal fistula, Pierre Robin sequence, and choanal atresia were excluded. |
| Gokce et al. 2019 Turkey [24] | NIPPV(non-synchronised) using RAM cannula | NIPPV using short binasal prongs | All: 29.6 ± 2.0 I: 29.5 ± 2.2 C: 29.8 ± 1.8 | All: 1254 ± 348 I: 1255 ± 348 C: 1253 ± 350 | Non synchronised NIPPV as primary support | Primary outcome: Need for IMV (failure of NIPPV) within the first 72 h of life Need for surfactant Secondary outcomes: Duration of NIPPV Duration of IMV Duration of supplemental oxygen Incidence of nasal injury: nasal septal injury stage 1 or 2 NEC IVH > grade 2 Pneumothorax Pulmonary interstitial emphysema Pulmonary haemorrhage BPD Duration of hospital stay Death | Inclusion criteria: Neonates between 26 to 33+6 weeks gestation stratified from 26 weeks to 29+6 weeks and 30 to 33 +6 weeks Exclusion criteria: Infants who required intubation in the delivery room, those with a major congenital anomaly, or those were transferred to hospital after birth in another center. |
| Hochwald et al. 2021 Israel [25] | Synchronised NIPPV using RAM cannula | NIPPV with short binasal prongs | I: 29.3 ± 2.2 C: 29.2 ±2.5 | I: 1237 ± 414 C: 1254 ±448 | Synchronised NIPPV (Primary respiratory support and post extubation) | Primary outcome: Treatment failure within 72 h after initiation of NIPPV, i.e., need for IMV | Inclusion criteria: Neonates between 24 to 33+6 weeks gestation Exclusion criteria: Infants with significant morbidity apart from RDS, including cardiac disease (not including patent ductus arteriosus), congenital malformation, or if they had cardiovascular or respiratory instability because of sepsis, anaemia, or severe IVH. |
| Singh et al. 2021 U.S.A [23] | CPAP using RAM cannula | CPAP using short binasal prongs | 28.1 ± 2.1 | 1225 ± 405 | CPAP | Intraoral (pharyngeal) pressures | Inclusion criteria: Any preterm infant with respiratory distress requiring CPAP but not IMV or NIPPV Exclusion criteria: Critically ill or had major congenital anomalies, neuromuscular disorders, or upper airway anomalies. |
| Sharma et al. 2020 India [18] | CPAP using RAM cannula | CPAP using nasal mask or short binasal prongs | I: 32 (29 to 33) C: 32(29 to 33) | I: 1331 ± 228 C: 1382 ± 209 | CPAP | Mean pharyngeal pressure | Inclusion criteria: Preterm neonates with gestation 28 to 34 weeks and BW more than or equal to 1000 g and requiring nasal CPAP for respiratory distress. Exclusion criteria: infants who were critically ill and those who had major congenital anomalies or upper airway malformations. |
| Drescher et al. 2018 USA [22] | NRS which included CPAP, NIPPV and HHHFNC using RAM cannula (with barrier nursing). | NRS using all other interfaces before the implementation of RAM system as interface in 2014. (Historical control). | I: 26.9 ± 1.3 C: 26.4 ± 1.6 | I: 879 ±192.9 C: 866.6 ± 185.4 | NIPPV (Primary respiratory support and post extubation) | Total IMV courses Total IMV duration Initial IMV duration Successful extubation Time until initial re-intubation Total re-intubations NRS failure < 7 days Total duration of CPAP Total duration of NIPPV Total duration of HFNC Total duration of nasal cannula use Total duration of NRS Total duration of respiratory support BPD Skin and/or mucosal breakdown | Inclusion criteria: Neonates < 1500 g and/or less than 29 weeks, gestation Exclusion criteria: any infant who died before the initiation of NRS or who was transferred before 36 weeks’ postmenstrual age. |
| Certainty Assessment | Summary of Findings | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Participants (Studies) Follow-Up | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Overall Certainty of Evidence | Study Event Rates (%) | Relative Effect (95% CI) | Anticipated Absolute Effects | ||
| With Other Interfaces (Binasal Prongs and/or Nasal Mask) | With RAM Cannula | Risk with other Interfaces (Binasal Prongs and/or Nasal Mask) | Risk Difference with RAM Cannula | ||||||||
| Treatment failure | |||||||||||
| 521 (3 RCTs) | not serious | very serious a | serious b | serious c | none | ⨁◯◯◯ Very low | 44/262 (16.8%) | 49/259 (18.9%) | RR 1.20 (0.48 to 3.01) | 168 per 1000 | 34 more per 1000 (from 87 fewer to 338 more) |
| Invasive mechanical ventilation requirement | |||||||||||
| 521 (3 RCTs) | not serious | serious d | not serious e | serious f | none | ⨁⨁◯◯ Low | 16/262 (6.1%) | 36/259 (13.9%) | RR 1.37 (0.67 to 3.04) | 61 per 1000 | 23 more per 1000 (from 20 fewer to 125 more) |
| Surfactant requirement | |||||||||||
| 292 (2 RCTs) | not serious | very serious a | serious b | serious c | none | ⨁◯◯◯ Very low | 66/145 (45.5%) | 66/147 (44.9%) | RR 1.44 (0.68 to 3.04) | 455 per 1000 | 200 more per 1000 (from 146 fewer to 929 more) |
| Air leak | |||||||||||
| 521 (3 RCTs) | not serious | not serious | serious b | serious c | none | ⨁⨁◯◯ Low | 6/262 (2.3%) | 7/259 (2.7%) | RR 1.20 (0.36 to 4.00) | 23 per 1000 | 5 more per 1000 (from 15 fewer to 69 more) |
| Duration of invasive mechanical ventilation | |||||||||||
| 292 (2 RCTs) | serious g | very serious a | not serious e | serious h | none | ⨁◯◯◯ Very low | 145 | 147 | - | MD 5.07 days higher (1.04 lower to 11.19 higher) | |
| Duration of non-invasive respiratory support | |||||||||||
| 521 (3 RCTs) | not serious i | very serious a | not serious e | serious h | none | ⨁◯◯◯ Very low | 262 | 259 | - | MD 2.85 days higher (0.95 lower to 6.64 higher) | |
| Oropharyngeal pressure | |||||||||||
| 106 (2 observational studies) | serious j | very serious a | not serious | serious f | none | ⨁◯◯◯ Very low | 52 | 54 | - | MD 1.84 cm H2O lower (3.12 lower to 0.56 lower) | |
| Nasal Trauma | |||||||||||
| 521 (3 RCTs) | not serious | serious a | not serious | serious c | none | ⨁⨁◯◯ Low | 67/262 (25.6%) | 31/259 (12.0%) | RR 0.49 (0.21 to 1.11) | 256 per 1000 | 130 fewer per 1000 (from 202 fewer to 28 more) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anand, P.; Kaushal, M.; Ramaswamy, V.V.; Pullattayil S., A.K.; Razak, A.; Trevisanuto, D. Nasal Cannula with Long and Narrow Tubing for Non-Invasive Respiratory Support in Preterm Neonates: A Systematic Review and Meta-Analysis. Children 2022, 9, 1461. https://doi.org/10.3390/children9101461
Anand P, Kaushal M, Ramaswamy VV, Pullattayil S. AK, Razak A, Trevisanuto D. Nasal Cannula with Long and Narrow Tubing for Non-Invasive Respiratory Support in Preterm Neonates: A Systematic Review and Meta-Analysis. Children. 2022; 9(10):1461. https://doi.org/10.3390/children9101461
Chicago/Turabian StyleAnand, Pratima, Monika Kaushal, Viraraghavan Vadakkencherry Ramaswamy, Abdul Kareem Pullattayil S., Abdul Razak, and Daniele Trevisanuto. 2022. "Nasal Cannula with Long and Narrow Tubing for Non-Invasive Respiratory Support in Preterm Neonates: A Systematic Review and Meta-Analysis" Children 9, no. 10: 1461. https://doi.org/10.3390/children9101461