
Psychometric Assessment of the Handwriting Proficiency Screening Questionnaire (HPSQ)—Thai Version for Primary School-Aged Children
 ,
,  , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Instrument
2.2. Participants
2.3. Procedures and Data Analysis
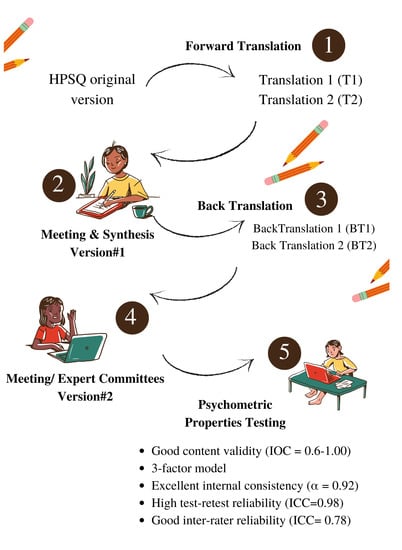
2.3.1. Translation and Cross-Cultural Adaptation Process
2.3.2. Psychometric Assessment of the HPSQ–Thai Version
Content Validity
Internal Consistency
Inter-Rater and Rest–Retest Reliability
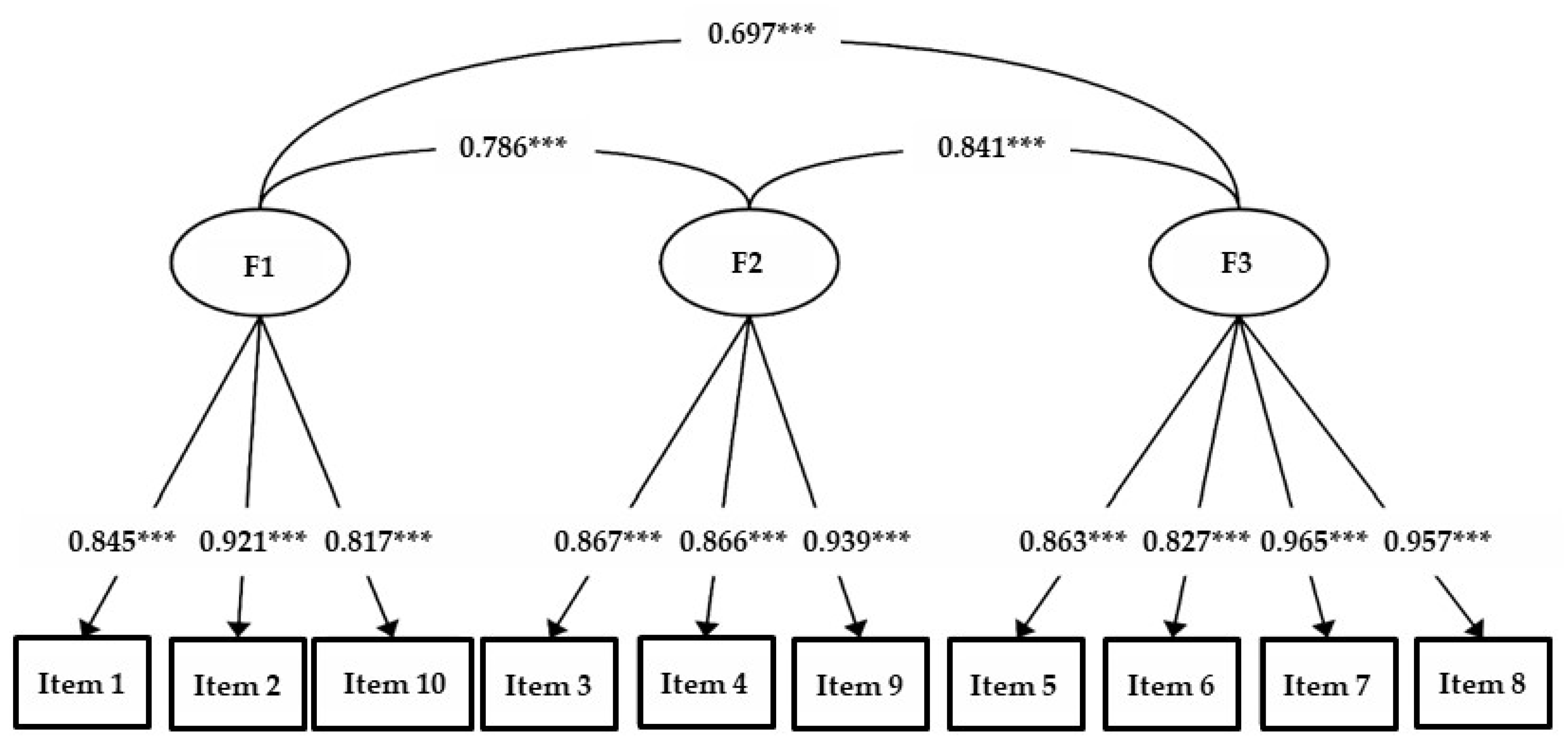
Confirmatory Factor Analysis
Discriminant Validity
3. Results
3.1. Construct Validity
3.2. Internal Consistency, Rest–Retest, and Inter-Rater Reliability
3.3. Sex- and Grade-Related Differences
4. Discussion
4.1. Cross-Cultural Adaptation
4.2. Content Validity and Confirmatory Factor Analysis
4.3. Internal Consistency, Inter-Rater and Intra-Rater Reliability
4.4. Sex- and Grade-Related Differences
4.5. Limitations and Future Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Engel-Yeger, B.; Nagauker-Yanuv, L.; Rosenblum, S. Handwriting Performance, Self-Reports, and Perceived Self-Efficacy Among Children With Dysgraphia. Am. J. Occup. Ther. 2009, 63, 182–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenblum, S.; Aloni, T.; Josman, N. Relationships between handwriting performance and organizational abilities among children with and without dysgraphia: A preliminary study. Res. Dev. Disabil. 2010, 31, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Dinehart, L.H. Handwriting in early childhood education: Current research and future implications. J. Early Child. Lit. 2014, 15, 97–118. [Google Scholar] [CrossRef]
- Dinehart, L.; Manfra, L. Associations Between Low-Income Children’s Fine Motor Skills in Preschool and Academic Performance in Second Grade. Early Educ. Dev. 2013, 24, 138–161. [Google Scholar] [CrossRef]
- Feder, K.; Majnemer, A.; Synnes, A. Handwriting: Current Trends in Occupational Therapy Practice. Can. J. Occup. Ther. 2000, 67, 197–204. [Google Scholar] [CrossRef]
- Puranik, C.S.; AlOtaiba, S. Examining the contribution of handwriting and spelling to written expression in kindergarten children. Read. Writ. 2011, 25, 1523–1546. [Google Scholar] [CrossRef] [Green Version]
- Chung, P.J.; Patel, D.R.; Nizami, I. Disorder of written expression and dysgraphia: Definition, diagnosis, and management. Transl. Pediatr. 2020, 9, S46–S54. [Google Scholar] [CrossRef]
- Nightingale, R.; Sumner, E.; Prunty, M.; Barnett, A.L. Handwriting and typing: Occupational therapy practice when supporting adolescents with handwriting difficulties. Br. J. Occup. Ther. 2022, 03080226221097314. [Google Scholar] [CrossRef]
- Overvelde, A.; Hulstijn, W. Handwriting development in grade 2 and grade 3 primary school children with normal, at risk, or dysgraphic characteristics. Res. Dev. Disabil. 2011, 32, 540–548. [Google Scholar] [CrossRef]
- Cramm, H.; Pollock, N.; Dennis, D.; Subramaniam, K.; Carkner, M. Occupational therapy with school-aged children. Occup Ther Now 2009, 11, 24–26. [Google Scholar]
- Hoy, M.M.P.; Egan, M.; Feder, K.P. A Systematic Review of Interventions to Improve Handwriting. Can. J. Occup. Ther. 2011, 78, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Office of the Basic Education Commission. Annual Report 2015 Office of the Basic Education Commission; The Agricultural Cooperative Federation of Thailand, Limited: Bangkok, Thailand, 2015. [Google Scholar]
- Daniel, M.E.; Froude, E.H. Reliability of occupational therapist and teacher evaluations of the handwriting quality of grade 5 and 6 primary school children. Aust. Occup. Ther. J. 2010, 45, 48–58. [Google Scholar] [CrossRef]
- Rubin, N.; Henderson, S.E. Two Sides of the Same Coin: Variations in Teaching Methods and Failure to Learn to Write. Br. J. Spéc. Educ. 2007, 9, 17–24. [Google Scholar] [CrossRef]
- Khamduangdao, S.; Sriphetcharawut, S. Effectiveness of Handwriting Intervention Protocol for Students with Attention-Deficit/Hyperactivity Disorder and Handwriting Difficulties. Acad. Psychiatry Psychol. J. 2018, 34, 104–118. [Google Scholar]
- Rosenblum, S. Development, Reliability, and Validity of the Handwriting Proficiency Screening Questionnaire (HPSQ). Am. J. Occup. Ther. 2008, 62, 298–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Šafárová, K.; Mekyska, J.; Zvončák, V.; Galáž, Z.; Francová, P.; Čechová, B.; Losenická, B.; Smékal, Z.; Urbánek, T.; Havigerová, J.M.; et al. Handwriting Proficiency Screening Questionnaire—Czech Version. Front. Psychol. 2020. [Google Scholar] [CrossRef]
- Cantero-Téllez, R.; Porqueres, M.; Piñel, I.; Orza, J. Cross-cultural Adaptation, internal consistency and validity of the handwriting proficiency screening questionnaire (HPSQ) for Spanish primary school-age children. J. Nov. Physiother. 2015, 5, 10–4172. [Google Scholar] [CrossRef] [Green Version]
- Germano, G.D.; Giaconi, C.; Capellini, S.A. Characterization of Brazilians Students with Dyslexia in Handwriting Proficiency Screening Questionnaire and Handwriting Scale. J. Psychol. Res. 2016, 6, 590–597. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Process of Translation and Adaptation of Instruments. WHO Guidelines on Translations; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [Green Version]
- Muthén, L.; Muthén, B. Mplus. The Comprehensive Modelling Program for Applied Researchers: User’s Guide; Muthén & Muthén: Los Angeles, CA, USA, 2018. [Google Scholar]
- Tongprasert, S.; Rapipong, J.; Buntragulpoontawee, M. The cross-cultural adaptation of the DASH questionnaire in Thai (DASH-TH). J. Hand Ther. 2014, 27, 49–54. [Google Scholar] [CrossRef]
- DeVellis, R.F.; Thorpe, C.T. Scale Development: Theory and Applications; Sage Publications: Thousand Okas, CA, USA, 2003. [Google Scholar]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Flora, D.B.; Curran, P.J. An Empirical Evaluation of Alternative Methods of Estimation for Confirmatory Factor Analysis With Ordinal Data. Psychol. Methods 2004, 9, 466–491. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Chen, F.F. Sensitivity of Goodness of Fit Indexes to Lack of Measurement Invariance. Struct. Equ. Model. A Multidiscip. J. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Butt, M.L.; Pinelli, J.; Boyle, M.H.; Thomas, H.; Hunsberger, M.; Saigal, S.; Lee, D.S.; Fanning, J.K.; Austin, P. Development and Evaluation of an Instrument to Measure Parental Satisfaction With Quality of Care in Neonatal Follow-Up. J. Dev. Behav. Pediatr. 2009, 30, 57–65. [Google Scholar] [CrossRef]
- Rosenblum, S.; Gafni-Lachter, L. Handwriting Proficiency Screening Questionnaire for Children (HPSQ–C): Development, Reliability, and Validity. Am. J. Occup. Ther. 2015, 69, 6903220030. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Model | CFI | TLI | RMSEA | SRMR | χ2 | Δχ2 | ΔCFI | ΔRMSEA |
|---|---|---|---|---|---|---|---|---|
| 1-factor | 0.934 | 0.915 | 0.232 | 0.105 | 412.129 * | |||
| 2-factor | 0.951 | 0.935 | 0.203 | 0.090 | 313.922 * | 60.239 * | 0.017 | 0.029 |
| 3-factor | 0.961 | 0.945 | 0.187 | 0.075 | 255.015 * | 52.382 * | 0.010 | 0.016 |
| ICC Value | Questionnaire | Questionnaire Item |
|---|---|---|
| 0.69 | Is the child’s writing unreadable? | 1 |
| 0.46 | Is the child unsuccessful in reading his/her own handwriting? | 2 |
| 0.77 | Does the child not have enough time to copy tasks from the blackboard? | 3 |
| 0.66 | Does the child often erase while writing? | 4 |
| 0.74 | Does the child often feel he/she does not want to write? | 5 |
| 0.66 | Does the child not do his/her homework? | 6 |
| 0.70 | Does the child complain about pain while writing? | 7 |
| 0.64 | Does the child tire while writing? | 8 |
| 0.67 | Does the child need to look at the page/blackboard often when copying? | 9 |
| 0.53 | Is the child not satisfied with his/her handwriting? | 10 |
| 0.78 | HPSQ final score | |
| Grade | n | M | SD | ||
|---|---|---|---|---|---|
| 1 | 50 | 13.67 | 7.03 | ||
| 2 | 50 | 6.10 | 5.81 | ||
| 3 | 50 | 7.26 | 6.56 | ||
| 4 | 50 | 7.63 | 5.71 | ||
| Analysis of Variance | |||||
| Source | Sum of Squares | df | Mean Square | F | Sig. |
| Between Groups | 1707.56 | 3 | 569.18 | 12.30 | 0.000 |
| Within Groups | 9070.22 | 196 | 46.27 | ||
| Total | 10,777.79 | 199 | |||
| Pair-wise comparison—Fischer’s LSD test | |||||
| Grade | 1 | 2 | 3 | 4 | |
| 1 | 7.57 *** | 6.41 *** | 6.01 *** | ||
| 2 | −1.16 | −1.56 | |||
| 3 | −0.41 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thichanpiang, P.; Kaunnil, A.; Lee, K.; Gao, X.; Nopparat, C.; Permpoonputtana, K. Psychometric Assessment of the Handwriting Proficiency Screening Questionnaire (HPSQ)—Thai Version for Primary School-Aged Children. Children 2022, 9, 1580. https://doi.org/10.3390/children9101580
Thichanpiang P, Kaunnil A, Lee K, Gao X, Nopparat C, Permpoonputtana K. Psychometric Assessment of the Handwriting Proficiency Screening Questionnaire (HPSQ)—Thai Version for Primary School-Aged Children. Children. 2022; 9(10):1580. https://doi.org/10.3390/children9101580
Chicago/Turabian StyleThichanpiang, Peeradech, Anuchart Kaunnil, Kerry Lee, Xiaozi Gao, Chutikorn Nopparat, and Kannika Permpoonputtana. 2022. "Psychometric Assessment of the Handwriting Proficiency Screening Questionnaire (HPSQ)—Thai Version for Primary School-Aged Children" Children 9, no. 10: 1580. https://doi.org/10.3390/children9101580