
Neonatal Hemodynamic Characteristics of the Recipient Twin of Twin-To-Twin Transfusion Syndrome Not Treated with Fetoscopic Laser Surgery

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Population
2.2. Data Collection
2.3. Management Protocol
2.4. Statistics
3. Results
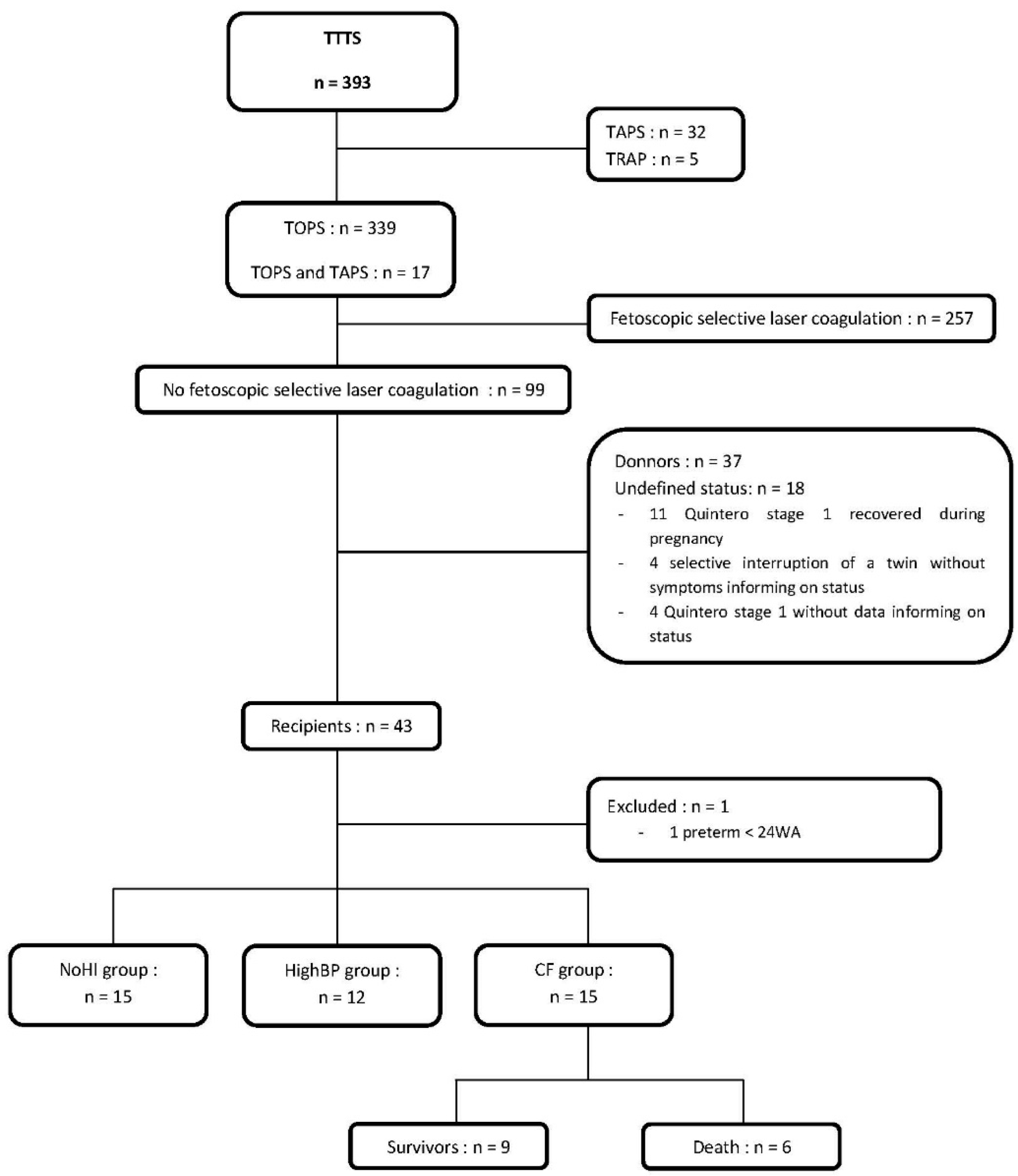
3.1. Study Population and Clinical Characteristics
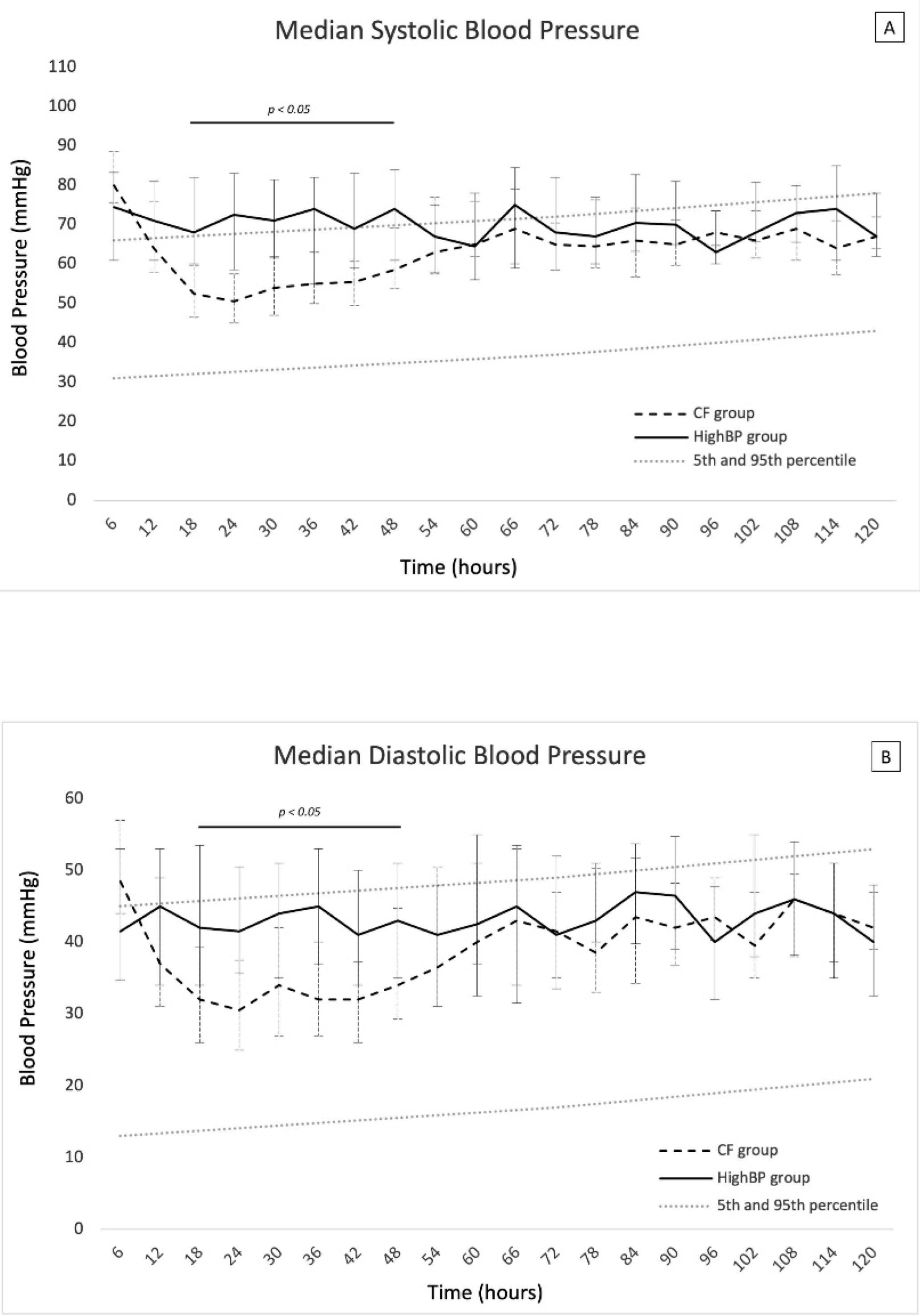
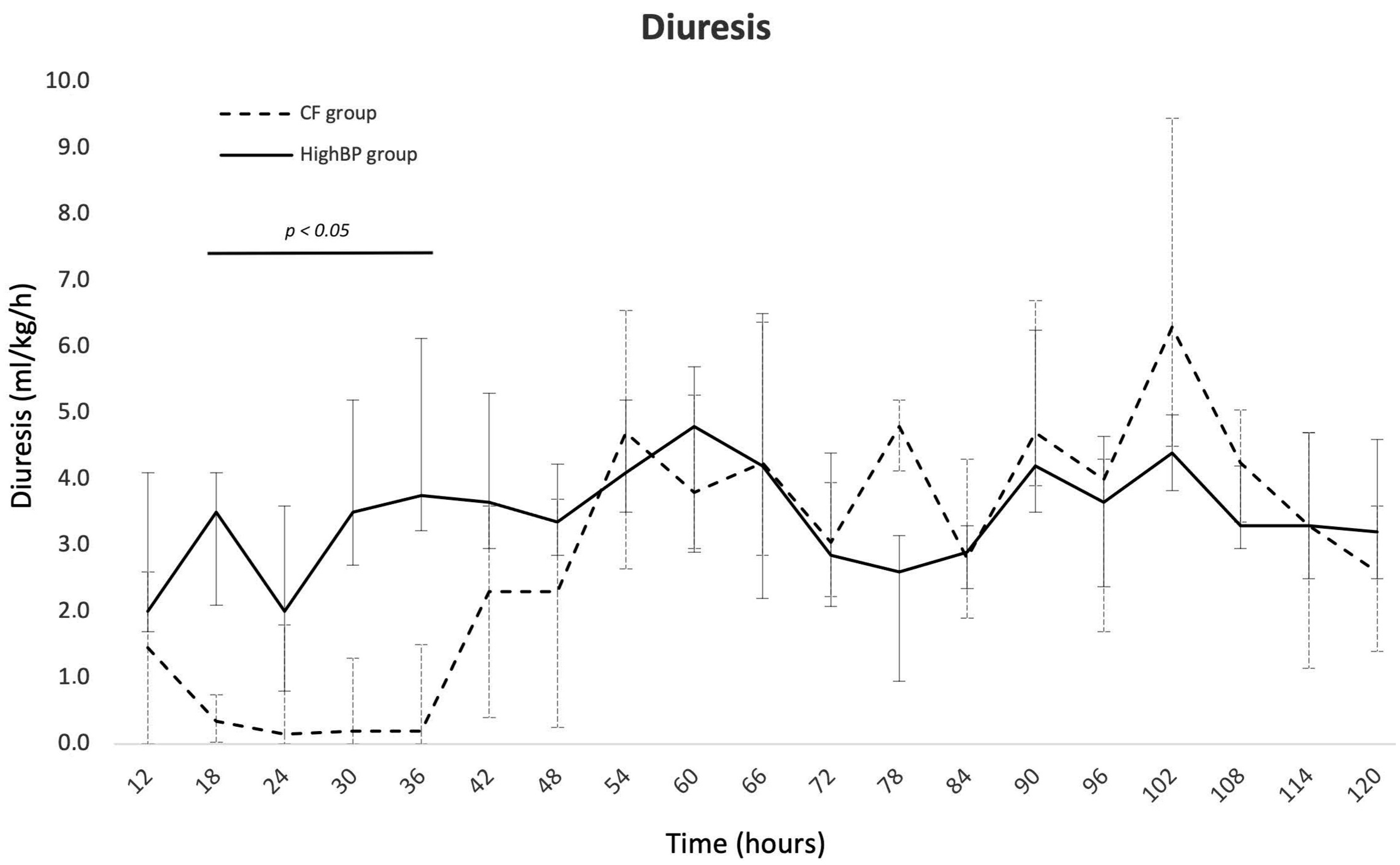
3.2. Characterization of the Hemodynamic Disorders in the Recipient Twins
3.3. Factors Associated with Cardiac Failure (Table 3)

{kind=link}
{kind=link}
{kind=link}
| NoHI + HighBP | CF | OR | 95% CI | p | |||
|---|---|---|---|---|---|---|---|
| n = 27 | n = 15 | ||||||
| Pregnancy | |||||||
| Threatened preterm labor, n (%) | 6 | (22) | 2 | (13) | 0.6 | (0.1–3.4) | 1.00 |
| Prenatal death of the donor twin | |||||||
| Gestational diabetes, n (%) | 1 | (4) | 1 | (7) | 1.9 | (0.1–32.1) | 1.00 |
| Pre-eclampsia, n (%) | 1 | (4) | 0 | (0) | * | 1.00 | |
| Premature rupture of membranes, n (%) | 4 | (15) | 0 | (0) | * | 0.28 | |
| Antenatal corticosteroid therapy, n (%) | 19 | (70) | 10 | (67) | 0.8 | (0.2–3.3) | 1.00 |
| TTTs | |||||||
| Amnioreduction, n (%) | 14 | (52) | 8 | (53) | 1.1 | (0.3–3.8) | 1.00 |
| Gestational age, median (Q1–Q3) | 28 | (26–29) | 28 | (28–29) | 0.65 | ||
| Associated-TAPS, n (%) | 0 | (0) | 4 | (27) | * | 0.012 | |
| Quintero stage | |||||||
| Quintero stage 1 or 2, n (%) | 16 | (59) | 6 | (40) | 0.5 | (0.1–1.7) | 0.34 |
| Quintero stage 3 or 4, n (%) | 8 | (30) | 9 | (60) | 3.6 | (0.9–13.4) | 0.52 |
| Quintero stage 5, n (%) | 3 | (11) | 0 | (0) | * | 0.54 | |
| Selective interruption during pregnancy, n (%) | 6 | (22) | 0 | (0) | * | 0.07 | |
| Birth | |||||||
| Mode of delivery | |||||||
| Elective cesarean section, n (%) | 20 | (74) | 5 | (33) | 0.2 | (0.1–0.7) | 0.020 |
| Emergency cesarean section, n (%) | 7 | (26) | 10 | (67) | 5.7 | (1.4–22.6) | |
| Term | |||||||
| Very preterm, n (%) | 14 | (52) | 13 | (87) | 6.0 | (1.1–32.1) | 0.040 |
| Moderate or late preterm, n(%) | 13 | (48) | 2 | (13) | 0.2 | (0–0.9) | |
| Male, n (%) | 12 | (44) | 7 | (47) | 1.1 | (0.3–3.9) | 1.00 |
| Weight discordance with the twin > 25%, n (%) | 7 | (26) | 3 | (20) | 0.7 | (0.2–3.3) | 1.00 |
| APGAR score | |||||||
| Low 1-min APGAR score, n (%) | 9 | (33) | 12 | (80) | 8.0 | (1.8–35.8) | 0.009 |
| Low 5-min APGAR score, n (%) | 3 | (11) | 7 | (47) | 7.0 | (1.5–33.7) | 0.020 |
| Umbilical cord acidosis, n (%) | 0 | (0) | 3 | (20) | * | 0.040 | |
| Hemoglobin at birth > 20 g/dL, n (%) | 2 | (7) | 8 | (53) | 14.3 | (2.5–83.2) | 0.002 |
| Hematocrit at birth > 65%, n (%) | 1 | (4) | 4 | (27) | 9.5 | (1.0–94.4) | 0.047 |
3.4. Mortality Rate
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harkness, U.F.; Crombleholme, T.M. Twin–Twin Transfusion Syndrome: Where Do We Go from Here? Semin. Perinatol. 2005, 29, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; Cooper, E.; Townsend, R.; Thilaganathan, B. Evolution of Stage 1 Twin-to-Twin Transfusion Syndrome (TTTS): Systematic Review and Meta-Analysis. Twin Res. Hum. Genet. 2016, 19, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Djaafri, F.; Stirnemann, J.; Mediouni, I.; Colmant, C.; Ville, Y. Twin–Twin Transfusion Syndrome—What We Have Learned from Clinical Trials. Semin. Fetal Neonatal Med. 2017, 22, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Manning, N.; Archer, N. Cardiac Manifestations of Twin–to–Twin Transfusion Syndrome. Twin Res. Hum. Genet. 2016, 19, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Stirnemann, J.J.; Nasr, B.; Proulx, F.; Essaoui, M.; Ville, Y. Evaluation of the CHOP Cardiovascular Score as a Prognostic Predictor of Outcome in Twin-Twin Transfusion Syndrome after Laser Coagulation of Placental Vessels in a Prospective Cohort. Ultrasound Obstet. Gynecol. 2010, 36, 52–57. [Google Scholar] [CrossRef]
- Mahieu-Caputo, D.; Muller, F.; Joly, D.; Gubler, M.-C.; Lebidois, J.; Fermont, L.; Dumez, Y.; Dommergues, M. Pathogenesis of Twin-Twin Transfusion Syndrome: The Renin-Angiotensin System Hypothesis. Fetal Diagn. Ther. 2001, 16, 241–244. [Google Scholar] [CrossRef]
- Mercanti, I.; Boivin, A.; Wo, B.; Vlieghe, V.; Le Ray, C.; Audibert, F.; Fouron, J.-C.; Leduc, L.; Nuyt, A.M. Blood Pressures in Newborns with Twin–Twin Transfusion Syndrome. J. Perinatol. 2011, 31, 417–424. [Google Scholar] [CrossRef]
- Wohlmuth, C.; Boudreaux, D.; Moise, K.J., Jr.; Johnson, A.; Papanna, R.; Bebbington, M.; Gardiner, H.M. Cardiac Pathophysiology in Twin-Twin Transfusion Syndrome: New Insights into Its Evolution. Ultrasound Obstet. Gynecol. 2018, 51, 341–348. [Google Scholar] [CrossRef]
- Verbeek, L.; Joemmanbaks, F.A.; Quak, J.M.E.; Sukhai, R.N.; Middeldorp, J.M.; Oepkes, D.; Lopriore, E. Renal Function in Neonates with Twin-Twin Transfusion Syndrome Treated with or without Fetoscopic Laser Surgery. Eur. J. Pediatr. 2017, 176, 1209–1215. [Google Scholar] [CrossRef]
- Lopriore, E.; Slaghekke, F.; Verweij, E.; Haak, M.; Middeldorp, A.; Lopriore, E. Neonatal Outcome in Twin-to-Twin Transfusion Syndrome Not Treated with Fetoscopic Laser Surgery. Twin Res. Hum. Genet. 2022, 25, 45–49. [Google Scholar] [CrossRef]
- Cho, H.; Shin, S.H.; Jun, J.K.; Shin, S.H.; Kim, Y.-J.; Kim, S.H.; Kim, E.-K.; Kim, H.-S. Early Postnatal Cardiac Manifestations Are Associated with Perinatal Brain Injury in Preterm Infants with Twin to Twin Transfusion Syndrome. Sci. Rep. 2019, 9, 18505. [Google Scholar] [CrossRef] [PubMed]
- Lenclen, R.; Ciarlo, G.; Paupe, A.; Bussieres, L.; Ville, Y. Neurodevelopmental Outcome at 2 Years in Children Born Preterm Treated by Amnioreduction or Fetoscopic Laser Surgery for Twin-to-Twin Transfusion Syndrome: Comparison with Dichorionic Twins. Am. J. Obstet. Gynecol. 2009, 201, 291.e1–291.e5. [Google Scholar] [CrossRef] [PubMed]
- Salomon, L.J.; Örtqvist, L.; Aegerter, P.; Bussieres, L.; Staracci, S.; Stirnemann, J.J.; Essaoui, M.; Bernard, J.-P.; Ville, Y. Long-Term Developmental Follow-up of Infants Who Participated in a Randomized Clinical Trial of Amniocentesis vs. Laser Photocoagulation for the Treatment of Twin-to-Twin Transfusion Syndrome. Am. J. Obstet. Gynecol. 2010, 203, 444.e1–444.e7. [Google Scholar] [CrossRef] [PubMed]
- Lopriore, E.; Oepkes, D. Fetal and Neonatal Haematological Complications in Monochorionic Twins. Semin. Fetal Neonatal Med. 2008, 13, 231–238. [Google Scholar] [CrossRef]
- Quintero, R.A.; Morales, W.J.; Allen, M.H.; Bornick, P.W.; Johnson, P.K.; Kruger, M. Staging of Twin-Twin Transfusion Syndrome. J. Perinatol. 1999, 19, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Allanson, E.; Waqar, T.; White, C.; Tunçalp, Ö.; Dickinson, J. Umbilical Lactate as a Measure of Acidosis and Predictor of Neonatal Risk: A Systematic Review. BJOG Int. J. Obstet. Gynecol. 2017, 124, 584–594. [Google Scholar] [CrossRef] [PubMed]
- Gutbir, Y.; Wainstock, T.; Sheiner, E.; Segal, I.; Sergienko, R.; Landau, D.; Walfisch, A. Low Apgar Score in Term Newborns and Long-Term Infectious Morbidity: A Population-Based Cohort Study with up to 18 Years of Follow-Up. Eur. J. Pediatr. 2020, 179, 959–971. [Google Scholar] [CrossRef]
- Lewi, L.; Jani, J.; Blickstein, I.; Huber, A.; Gucciardo, L.; Van Mieghem, T.; Doné, E.; Boes, A.-S.; Hecher, K.; Gratacós, E.; et al. The Outcome of Monochorionic Diamniotic Twin Gestations in the Era of Invasive Fetal Therapy: A Prospective Cohort Study. Am. J. Obstet. Gynecol. 2008, 199, 514.e1–514.e8. [Google Scholar] [CrossRef]
- Mamelle, N.; Munoz, F.; Grandjean, H. Fetal growth from the AUDIPOG study. I. Establishment of reference curves. J. Gynecol. Obstet. Biol. Reprod. 1996, 25, 61–70. [Google Scholar]
- Frey, H.A.; Klebanoff, M.A. The Epidemiology, Etiology, and Costs of Preterm Birth. Semin. Fetal Neonatal Med. 2016, 21, 68–73. [Google Scholar] [CrossRef]
- Zubrow, A.; Hulman, S.; Kushner, H.; Falkner, B.; Zubrow, A.B.; Hulman, S.; Kushner, H.; Falkner, B. Determinants of Blood Pressure in Infants Admitted to Neonatal Intensive Care Units: A Prospective Multicenter Study. J. Perinatol. 1995, 15, 470–479. [Google Scholar] [PubMed]
- Tissot, C.; Singh, Y.; Sekarski, N. Echocardiographic Evaluation of Ventricular Function—For the Neonatologist and Pediatric Intensivist. Front. Pediatr. 2018, 6, 79. [Google Scholar] [CrossRef] [PubMed]
- Abushaban, L.; Vel, M.; Rathinasamy, J.; Sharma, P. Normal Reference Ranges for Left Ventricular Dimensions in Preterm Infants. Ann. Pediatr. Card. 2014, 7, 180. [Google Scholar] [CrossRef] [PubMed]
- Selewski, D.T.; Charlton, J.R.; Jetton, J.G.; Guillet, R.; Mhanna, M.J.; Askenazi, D.J.; Kent, A.L. Neonatal Acute Kidney Injury. Pediatrics 2015, 136, e463–e473. [Google Scholar] [CrossRef]
- Ancel, P.-Y.; Goffinet, F.; Kuhn, P.; Langer, B.; Matis, J.; Hernandorena, X.; Chabanier, P.; Joly-Pedespan, L.; Lecomte, B.; Vendittelli, F.; et al. Survival and Morbidity of Preterm Children Born at 22 Through 34 Weeks’ Gestation in France in 2011: Results of the EPIPAGE-2 Cohort Study. JAMA Pediatr. 2015, 169, 230. [Google Scholar] [CrossRef]
- Gan, H.; Cannesson, M.; Chandler, J.R.; Ansermino, J.M. Predicting Fluid Responsiveness in Children: A Systematic Review. Anesth. Analg. 2013, 117, 1380–1392. [Google Scholar] [CrossRef]
- Lopriore, E.; Bökenkamp, R.; Rijlaarsdam, M.; Sueters, M.; Vandenbussche, F.P.; Walther, F.J. Congenital Heart Disease in Twin-to-Twin Transfusion Syndrome Treated with Fetoscopic Laser Surgery. Congenit. Heart Dis. 2007, 2, 38–43. [Google Scholar] [CrossRef]
- Mahieu-Caputo, D.; Salomon, L.J.; Le Bidois, J.; Fermont, L.; Brunhes, A.; Jouvet, P.; Dumez, Y.; Dommergues, M. Fetal Hypertension: An Insight into the Pathogenesis of the Twin-Twin Transfusion Syndrome. Prenat. Diagn. 2003, 23, 640–645. [Google Scholar] [CrossRef]
- Michelfelder, E.; Gottliebson, W.; Border, W.; Kinsel, M.; Polzin, W.; Livingston, J.; Khoury, P.; Crombleholme, T. Early Manifestations and Spectrum of Recipient Twin Cardiomyopathy in Twin-Twin Transfusion Syndrome: Relation to Quintero Stage. Ultrasound Obstet. Gynecol. 2007, 30, 965–971. [Google Scholar] [CrossRef]



| NoHI | HighBP | CF | ||||
|---|---|---|---|---|---|---|
| n = 15 | n = 12 | n = 15 | ||||
| Pregnancy | ||||||
| Threatened preterm labor, n (%) | 3 | (20) | 3 | (25) | 2 | (13) |
| Prenatal death of the donor twin, n (%) | 8 | (53) | 1 | (8) | 0 | (0) |
| Gestational diabetes, n (%) | 0 | (0) | 1 | (8) | 1 | (7) |
| Pre-eclampsia, n (%) | 0 | (0) | 1 | (8) | 0 | (0) |
| Premature rupture of membranes, n (%) | 2 | (13) | 2 | (17) | 0 | (0) |
| Antenatal corticosteroid therapy, n (%) | 9 | (60) | 10 | (83) | 10 | (67) |
| Birth | ||||||
| Gestational age, median (Q1–Q3) | 33 | (32–34) | 29 | (28–30) | 29 | (28–31) |
| Male, n (%) | 5 | (33) | 7 | (58) | 7 | (47) |
| Weight (g), median (Q1–Q3) | 1800 | (1665–2082) | 1293 | (1168–1533) | 1265 | (1150–1607) |
| Weight (percentile), median (Q1–Q3) | 53 | (31–77) | 71 | (55–79) | 66 | (34–75) |
| % difference of weight with the twin, median (Q1–Q3) | 20.1 | (8.7–28) | 22.8 | (11.8–30.1) | 18.2 | (12.9–22.8) |
| APGAR score | ||||||
| 1 min, median (Q1–Q3) | 8 | (8–9) | 6 | (4–8) | 5 | (2–6) |
| 5 min, median (Q1–Q3) | 10 | (9–10) | 9 | (8–9) | 8 | (4–9) |
| Umbilical cord pH, median (Q1–Q3) | 7.36 | (7.31–7.39) | 7.37 | (7.36–7.39) | 7.30 | (7.26–7.37) |
| Hemodynamic morbidity | ||||||
| High systolic blood pressure, n (%) | 0 | (0) | 12 | (100) | 15 | (100) |
| Ventricular hypertrophy, n (%) | 2/11 | (33) | 12 | (100) | 15 | (100) |
| Patent ductus arteriosus requiring treatment, n (%) | 0 | (0) | 0 | (0) | 1 | (7) |
| Other neonatal morbidities | ||||||
| Hemodilution, n (%) | 0 | (0) | 1 | (8) | 4/15 | (27) |
| Bronchopulmonary dysplasia, n (%) * | 0 | (0) | 2 | (17) | 1/9 | (11) |
| Severe intraventricular hemorrhage (>2), n (%) | 0 | (0) | 1 | (8) | 3/15 | (20) |
| Periventricular leukomalacia, n (%) * | 0 | (0) | 1 | (8) | 4/9 | (44) |
| Secondary sepsis, n (%) * | 2 | (13) | 2 | (17) | 4/9 | (44) |
| Necrotizing enterocolitis, n (%) * | 1 | (7) | 1 | (8) | 0/9 | (0) |
| Acute kidney injury, n (%) | 0 | (0) | 3 | (25) | 14/15 | (93) |
| Death | ||||||
| Death in the first five days of life, n (%) | 0 | (0) | 0 | (0) | 6 | (40) |
| Age at death (hours), median (Q1–Q3) | 47 | (26–65) | ||||
| HighBP | CF | p | |||
|---|---|---|---|---|---|
| n = 12 | n = 15 | ||||
| Birth | |||||
| Gestational age, median (Q1–Q3) | 29 | (28–30) | 29 | (28–31) | 0.77 |
| Weight (g), median (Q1–Q3) | 1293 | (1168–1533) | 1265 | (1150–1607) | 0.98 |
| Weight (percentile), median (Q1–Q3) | 71 | (55–79) | 66 | (34–75) | 0.26 |
| % difference of weight with the twin, median (Q1–Q3) | 22.8 | (11.8–30.1) | 18.2 | (12.9–22.8) | 0.51 |
| APGAR score | |||||
| 1 min, median (Q1–Q3) | 6 | (4–8) | 5 | (2–6) | 0.35 |
| 5 min, median (Q1–Q3) | 9 | (8,9) | 8 | (4–9) | 0.15 |
| Umbilical cord pH, median (Q1–Q3) | 7.37 | (7.36–7.39) | 7.30 | (7.26–7.37) | 0.05 |
| Hemodynamic characteristics | |||||
| High systolic blood pressure, n (%) | 12 | (100) | 15 | (100) | 1.00 |
| Ventricular hypertrophy, n (%) | 12 | (100) | 15 | (100) | 1.00 |
| Maximum IVSd (mm), median (Q1–Q3) | 4.2 | (3.8–5.1) | 5.0 | (4.2–5.3) | 0.32 |
| Hydrocortisone hemisuccinate, n (%) | 2 | (17) | 6 | (40) | 0.41 |
| Renal-dose dopamine, n (%) | 0 | (0) | 4 | (27) | 0.10 |
| Fluid expension with saline solution, n (%) | 1 | (8) | 8 | (53) | 0.019 |
| Antihypertensive treatment | |||||
| Nicardipine, n (%) | 12 | (100) | 15 | (100) | 1.00 |
| Starting time (hours of life), median (Q1–Q3) | 4 | (4–23) | 3 | (2–16) | 0.18 |
| Maximal dose (μg/kg/min), median (Q1–Q3) | 0.6 | (0.5–1.2) | 1.0 | (0.7–1.8) | 0.08 |
| Inotropic treatment (Milrinone, Dobutamine), n (%) | 0 | (0) | 14 | (93) | |
| Milrinone, n (%) | 5 | (33) | |||
| Starting time (hours of life), median (Q1–Q3) | 22 | (16–39) | |||
| Maximal dose (μg/kg/min), median (Q1–Q3) | 0.2 | (0.2–0.2) | |||
| Dobutamine, n (%) | 13 | (87) | |||
| Starting time (hours of life), median (Q1–Q3) | 13 | (6–26) | |||
| Maximal dose (μg/kg/min), median (Q1–Q3) | 20.0 | (15.0–20.0) | |||
| Biological parameters | |||||
| pH in the first 2 days of life, median (Q1–Q3) | 7.33 | (7.29–7.37) | 7.26 | (7.23–7.29) | <0.001 |
| Lactate in the first 2 days of life, median (Q1–Q3) | 1.6 | (1.2–2.2) | 2.1 | (1.5–3.3) | 0.07 |
| Acute kidney injury, n (%) | 3 | (25) | 14 | (93) | <0.001 |
| Stage 1 of KDIGO classification, n (%) | 2 | (17) | 1 | (7) | 0.57 |
| Stage 2 of KDIGO classification, n (%) | 1 | (8) | 0 | (0) | 0.44 |
| Stage 3 of KDIGO classification, n (%) | 0 | (0) | 13 | (87) | <0.001 |
| Maximum serum blood urea nitrogen (mmol/L), median (Q1–Q3) | 6.7 | (6.1–8.0) | 13.3 | (8.8–17.9) | 0.003 |
| Maximum serum creatinine (µmol/L), median (Q1–Q3) | 77.0 | (62.3–87.5) | 134.0 | (90.8–157.8) | 0.005 |
| Urinary examinations, n (%) | 9 | (75) | 5 | (33) | |
| Urinary sodium excretion (mmol/L), median (Q1–Q3) | 38.0 | (33.0–54.0) | 28.5 | (13.0–36.0) | 0.011 |
| Proteinuria (g/L), median (Q1–Q3) | 0.15 | (0.08–0.24) | 0.30 | (0.18–0.49) | 0.032 |
| Urinary to serum ratio of urea nitrogen, median (Q1–Q3) | 8.34 | (7.08–8.70) | 5.74 | (3.28–6.51) | 0.017 |
| Urinary to serum ratio of creatinine, median (Q1–Q3) | 10.74 | (9.24–13.17) | 11.92 | (6.30–19.34) | 0.44 |
| Urinary sodium to potassium excretion ratio, median (Q1–Q3) | 5.17 | (3.26–8.65) | 1.44 | (0.99–1.62) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chambon, E.; Hachem, T.; Salvador, E.; Rigourd, V.; Bellanger, C.; Stirnemann, J.; Kermorvant-Duchemin, E.; Tissieres, P.; Ville, Y.; Lapillonne, A. Neonatal Hemodynamic Characteristics of the Recipient Twin of Twin-To-Twin Transfusion Syndrome Not Treated with Fetoscopic Laser Surgery. Children 2022, 9, 1766. https://doi.org/10.3390/children9111766
Chambon E, Hachem T, Salvador E, Rigourd V, Bellanger C, Stirnemann J, Kermorvant-Duchemin E, Tissieres P, Ville Y, Lapillonne A. Neonatal Hemodynamic Characteristics of the Recipient Twin of Twin-To-Twin Transfusion Syndrome Not Treated with Fetoscopic Laser Surgery. Children. 2022; 9(11):1766. https://doi.org/10.3390/children9111766
Chicago/Turabian StyleChambon, Edouard, Taymme Hachem, Elodie Salvador, Virginie Rigourd, Claire Bellanger, Julien Stirnemann, Elsa Kermorvant-Duchemin, Pierre Tissieres, Yves Ville, and Alexandre Lapillonne. 2022. "Neonatal Hemodynamic Characteristics of the Recipient Twin of Twin-To-Twin Transfusion Syndrome Not Treated with Fetoscopic Laser Surgery" Children 9, no. 11: 1766. https://doi.org/10.3390/children9111766
APA StyleChambon, E., Hachem, T., Salvador, E., Rigourd, V., Bellanger, C., Stirnemann, J., Kermorvant-Duchemin, E., Tissieres, P., Ville, Y., & Lapillonne, A. (2022). Neonatal Hemodynamic Characteristics of the Recipient Twin of Twin-To-Twin Transfusion Syndrome Not Treated with Fetoscopic Laser Surgery. Children, 9(11), 1766. https://doi.org/10.3390/children9111766