
Adverse Effects of Surgically Accelerated Orthodontic Techniques: A Systematic Review

 ,
,  , and
, and
Abstract
:1. Introduction
1.1. Rationale
1.2. Objectives
2. Materials and Methods
2.1. Design
2.2. Eligibility Criteria
2.2.1. Types of Participants
2.2.2. Types of Interventions
2.2.3. Comparisons
2.2.4. Types of Outcome Measures
2.2.5. Study Design
2.2.6. Exclusion Criteria
2.3. Information Sources
2.4. Search Strategy
2.5. Study Selection
2.6. Data Collection and Data Items
2.7. Risk of Bias Assessment in Included Studies
2.8. Effect Measures and Data Synthesis
3. Results
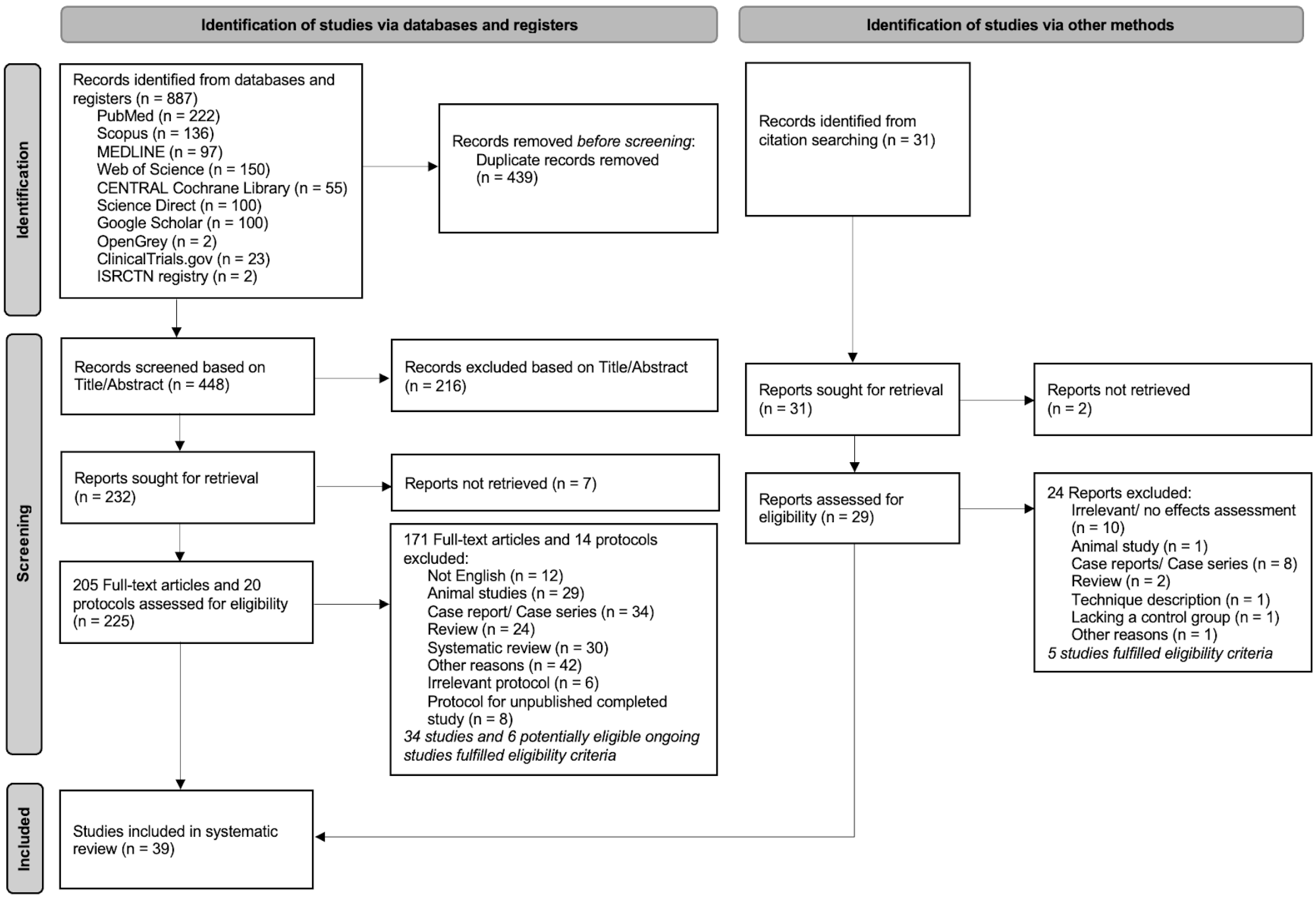
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias within Studies
3.4. Synthesis of Results
3.4.1. Description of Interventions
3.4.2. Results of Individual Studies
Periodontal Evaluation
Root Resorption
Tooth Vitality
4. Discussion
4.1. Discussion of the Results
4.2. Summary of Evidence
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
Appendix A

{kind=link}
| Authors, Publication Year, Study Setting | Study Design | Treatment Comparison | Participants Sample Size, Gender, Age (Years) | Malocclusion | Outcomes | Follow-Up Period |
|---|---|---|---|---|---|---|
| Abbas et al., 2012 Egypt [40] | RCT, parallel study | Alveolar corticotomy using PES vs. conventional OT | Patients (F/M): 8 (8/0) Control: 4 Exp.: 4 Mean age: 22.30 ± 2.26 (19–25) | Class I with minor to moderate mandibular crowding. | No PD > 3 mm, interdental papillae preservation, no GR. No significant reduction in the radiographic height of the crestal bone. No radiographic evidence of any significant apical RR. No loss of tooth vitality. | Until the completion of the decrowding of mandibular teeth. |
| Abbas et al., 2016 Egypt [41] | split-mouth RCT, multi-arm | Corticotomy vs. piezocision, corticotomy vs. conventional OT, and piezocision vs. conventional OT | Patients (F/M): 20 (NA) Corticotomy group:10 Piezocision group:10 Mean age: 15–25 | Class II Division 1 with mild or no crowding. | No differences in the periodontal parameters in either group at the start of canine retraction and after 3 months (p > 0.05). No difference between the 2 exp. sides in canine RR. Greater canine RR in the control than the exp. side in both groups. | 3 months |
| Abdelqader 2019 Egypt [45] | split-mouth RCT | Corticision vs. corticotomy | Patients (F/M): 10 (10/0) Control: 10 Exp.: 10 Dropouts: None Mean age: 17–30 | Malocclusions requiring maxillary 1st premolar extractions, with subsequent maxillary canine retraction. | Significant canine RR in both groups; however, the difference between both interventions was non-significant. | 5 months |
| Abed and Al-Bustani 2013 Iraq [67] | split-mouth CCT, prospective study | Corticotomy vs. conventional OT | Patients (F/M): 12 (8/4) Dropouts: None Control: 12 Exp.: 12 Mean age: 21.7 (17–28) | Malocclusions requiring maxillary 1st premolar extractions, with subsequent maxillary canine retraction. | No significant difference between pre- and post-surgery on the exp. side (p < 0.05) on gingival sulcus depth and tooth vitality. No sign of gingival inflammation according to the BoP index. | 1 month |
| Aboalnaga et al., 2019 Egypt [60] | split-mouth RCT | MOPs vs. conventional OT | Patients (F/M): 18 (18/0) Dropouts: None Control: 18 Exp.: 18 Mean age: 20.5 ± 3.85 (16–30) | Malocclusions requiring bilateral 1st premolar extractions. | No significant difference in RR between the MOP and control sides (p > 0.05). No significant difference in RR before and after canine retraction in both groups (p > 0.05). | 4 months |
| Aboul-Ela et al., 2011 Egypt [34] | split-mouth RCT | Corticotomy vs. conventional OT | Patients: 15 Dropouts: 2 (1 lost to follow-up, 1 due to poor oral hygiene) Patients (F/M): 13 (8/5) Control: 13 Exp.: 13 Mean age: 19 | Class II Division 1 requiring maxillary 1st premolar extractions, with subsequent maxillary canine retraction. | No statistically significant differences (p > 0.05) in PI, PD, AL, and GR between the exp. and control sides pre- and postoperatively. GI scores higher on the exp. compared with the control side (p < 0.05). | 4 months |
| Agrawal et al., 2018 India [65] | split-mouth RCT | MOPs vs. corticotomy | Patients (F/M): 10 (8/2) Dropouts: None Corticotomy group: 10 MOP group: 10 Mean age: 21.9 ± 2.13 (18–25) | Class I and Class II requiring 1st premolar extractions. | No significant changes in periodontal parameters and root length pre- and post-operatively in both groups (p > 0.05). Significant increase after performing both interventions in bone thickness at a coronal level (p < 0.05). DF after corticotomy presented in 40% of the sample, while 30% had DF after MOP. | 6 months |
| Aksakalli et al., 2016 Turkey [48] | split-mouth RCT | Piezocision vs. conventional OT | Patients (F/M): 10 (6/4) Dropouts: None Control:10 Exp.: 10 Mean age: 16.3 ± 2.4 | Class II requiring maxillary 1st premolar extractions and bilateral canine distalization. | No significant difference in gingival indices and mobility scores between the control and exp. sides pre- and postdistalization (p > 0.05). | Until Class I canine relationships were established. |
| Alkebsi et al., 2018 Jordan [59] | split-mouth RCT | MOPs vs. conventional OT | Patients (F/M): 35 (25/10) Dropouts: 3 subjects were excluded after MOP intervention due to either irregular attendance (Lost to follow-up) or poor oral hygiene. Patients completed the study (F/M): 32 (24/8) Control: 32 Exp.: 32 Mean age: 19.26 ± 2.48 (16 to 24.6) | Class II Division 1 requiring 1st premolar extractions. | No statistically significant difference in PI, GR, GI, AL, and PD between the MOP and control sides at any time point (p > 0.05). No adverse effect on periodontal health. No statistically significant difference between the control and MOP sides at baseline T0 (p = 0.59) and after 3 months T3 (p = 0.48). | 3 months |
| Alqadasi et al., 2019 China [57] | split-mouth, three-dimensional RCT | MOPs vs. conventional OT | Patients (F/M): 8, (F/M NA) Dropouts: None Control: 8 Exp.: 8 Mean age: 15–40 | Class II Division 1 | No statistically significant difference between the groups in periodontal index, bone height, RR, and PI. | 3 months |
| Alqadasi et al., 2020 China [58] | split-mouth RCT, parallel-group | MOPs vs. conventional OT, piezocision vs. conventional OT | Patients (F/M): 24 MOPs: 12 Piezo: 12 Dropouts: lost to follow-up 3 (2 in MOPs and 1 in Piezo group) Patients completed the study (F/M): 21 (12/9) MOPs: 10 (6F/4M) Piezo: 11 (6F/5M) Mean age: 20.89 ± 4.46 (15–40) | Class II Division 1 | No significant differences in either technique regarding RR (p = 0.087), buccal (p = 0.286), and palatal bone height (p = 0.127). MOPs caused more RR than Piezo (p = 0.024). | 3 months |
| Arana et al., 2022 Colombia [68] | CCT, prospective study | Piezocision and/or a 3D collagen matrix vs. conventional OT | Patients (F/M): 32 (8/24) Dropouts: None Control: 8 Exp. Group 1: 7 Exp. Group 2: 9 Exp. Group 3: 8 Mean age: 26.9 ± 5.8 (19–38) | Class I or mild Class II or III, and moderate irregularity according to the Little Irregularity Index. | No significant difference in root length observed among the four groups (p > 0.05). | Until the completion of orthodontic treatment. |
| Aristizabal et al., 2016 Colombia [38] | RCT | PAOO vs. conventional OT | Patients (F/M):10 (0/10) Dropouts: None Control: 5 Exp.: 5 Mean age: 18–40 (Control: 28.5 ± 6.3, Exp.: 29.6 ± 9.8) | Class I and II, mild crowding. | Each type of treatment showed no difference in the initial (T1) and final (T2) periodontal conditions. | Treatment time Exp.: 8.2 ± 3.3 months, Control: 13.4 ± 7.3 months. |
| Bahammam 2016 Saudi Arabia [42] | RCT, prospective study | Corticotomy vs. corticotomy + bovine xenograft vs. Corticotomy + bioactive glass | Patients (F/M): 33 (20/13) Group 1: 11 (7F/4M) Group 2: 11 (6F/5M) Group 3: 11 (7F/4M) Dropouts: 4 lost to follow-up and due to poor oral hygiene. After 9 months: 27 patients follow-up records available Mean age: 21.2 ± 1.43 (18–27) | Class I, moderate crowding. | No significant differences in PD between the study groups (p > 0.05). Good interdental papillae preservation, no loss of tooth vitality, and no evidence of significant apical RR at any time interval. Statistically significant greater increase in BD in groups 2 and 3, where grafts were incorporated at T3. | 9 months |
| Bansal et al., 2019 India [61] | RCT, prospective, two-arm, parallel-group study | MOPs vs. conventional OT | Patients (F/M): 30 (16/14) Dropouts: None Control: 15 Exp.: 15 Mean age: 14–19 | Mandibular crowding. | No statistically significant differences in RR and marginal alveolar bone height loss around mandibular incisors between the groups (p > 0.05). | 15 weeks |
| Chan et al., 2018 Australia [69] | split-mouth CCT, prospective study | MOPs vs. conventional OT | Patients (F/M): 20 (12/8) Dropouts: None Control: 20 Exp.: 20 Mean age: 15.4 (12–25) | Malocclusions requiring 1st premolar extractions. | MOPs resulted in 0.170 mm3 or 42% statistically significant greater RR compared with traditional OT (p > 0.001). | 28 days |
| Charavet et al., 2016 Belgium [49] | RCT | Piezocision vs. conventional OT | Patients (F/M): 24 (15/9) Control:12 Exp. (piezocision):12 Dropouts: 2 lost to follow-up (1 in each group) failed to attend the post-treatment CT scan. Patients completed the study: 22 Mean age: 30 ± 8 | Mild overcrowdings. | Periodontal parameters (recession depth, PD, PI, papilla bleeding index) and the thickness of the buccal alveolar plate, and the buccolingual dimensions of the alveolar crest remained stable between the baseline and treatment completion time points in both groups. Neither GR nor increases in RR were reported in either group. No significant increases in fenestration or dehiscence were observed in either group (p = 0.67). Scars were observed in 50% of the patients in the piezocision group, mainly as points (33%) rather than lines (17%). | N/A |
| Charavet et al., 2019 Belgium [50] | RCT, parallel group | Piezocision vs. conventional OT | Patients (F/M): 24 (15/9) Control: 12 (8/4) Exp.: 12 (7/5) Except for CBCT Control: 11, Exp.: 11 Dropouts: 2 lost to follow-up (1 in each group) failed to attend the post-treatment CBCT scan. Patients completed the study: 22 Mean age: Control: 27 ± 7, Exp.: 29 ± 8 | Mild-to-moderate overcrowding. | All periodontal and radiographic parameters remained unchanged from the start to the end of the treatment in both groups. No increase in fenestration (p = 0.86) or DF (p = 0.12) was observed between the two groups. Minor scars were detected in 66% of cases, mainly as points (58%) rather than lines (8%). | Until treatment completion |
| Elkalza et al., 2018 Egypt [56] | split-mouth RCT | MOPs vs. conventional OT, piezocision vs. conventional OT | Patients (F/M): 16 (NA) Dropouts: None MOPs: 8 Piezo: 8 Control: 8 Exp.: 8 Mean age: 16–25 | Malocclusions requiring maxillary 1st premolar extractions, with subsequent maxillary canine retraction. | No significant difference in canine root length between the MOP and control sides after canine retraction (p > 0.05). Statistically significant decrease in root length on the Piezo side compared to the control side (p < 0.05). | N/A |
| Gulduren et al., 2020 Northern Cyprus [62] | split-mouth RCT, single-center, prospective study | MOPs vs. conventional OT | Patients: 20 Control: 10 Exp.: 10 Dropouts: 2 lost to follow-up (due to missing follow-up data) Patients completed the study (F/M): 18 (7/11) Control: 9 Exp.: 9 Mean age: 16.5–23.8 | Class II molar relationship, skeletal Class I or mild Class II relationship. | No differences between the groups in PI, GI, PD, and the gingival bleeding of the maxillary 2nd premolars, 1st molars, and 2nd molars. No AL, GR, furcation defect, or mobility observed in these teeth from the start to the end of the experiment. No indication of RR or alveolar bone resorption. | 12 weeks |
| Hatrom et al., 2021 Saudi Arabia [52] | RCT, prospective parallel study | Piezocision vs. conventional en masse retraction | Patients (F/M): 26 (13/13) Control: 13 (7/6) Exp.: 13 (6/7) Dropouts-lost to follow-up: 3 due to mini-screw failure Patients completed the study (F/M): 23 Control: 11 Exp.: 12 Mean age: Control: 20.38 ± 3.64, Exp.: 19.27 ± 3.38 | Class II Division I, with mild or no crowding, requiring bimaxillary 1st premolar extractions and subsequent en masse retraction. | Statistically significant RR at the end of en masse retraction in both groups. Only the right and left central incisors and right canine showed statistically significant more RR in the control group compared to the Piezo group (p < 0.05). | Until the completion the of en masse retraction phase (mean = 122.74 ± 3.06 days, approx. 4 months) |
| Karci and Baka 2021 Turkey [53] | split-mouth RCT | Piezocision vs. conventional OT, PRF injection vs. conventional OT | Patients (F/M): 12 (7/5) Control: 12 Exp.: 12 Dropouts: None Mean age: 16.84 ± 0.33 | Class II with dentoalveolar protrusion or moderate crowding. | No significant differences in the periodontal readings between the exp. and control sides. | 12 weeks |
| Khlef et al., 2020 Syria [46] | RCT, single-centered, parallel-group | Traditional corticotomy vs. flapless corticotomy (corticision) | Patients (F/M): 40 (36/4) Dropouts: None TCG: 20 FCG: 20 Mean age: TCG: 22.44 ± 3.55 FCG: 21.90 ± 3.60 | Class II Division 1, requiring maxillary 1st premolar extractions. | No significant differences in the amount of EARR in maxillary anterior teeth (p = 0.31). The proportion of the detected EARR ranged from 1% to 6% of the root length in both corticotomy groups. | Until canines reached Class I relationship with normal overjet and overbite. |
| Khlef et al., 2022 Syria [47] | RCT, single-centered, two-arm parallel-group | Traditional corticotomy vs. flapless corticotomy (corticision) | Patients (F/M): 38 (35/3) TCG: 19 FCG: 19 Dropouts: 2, 1 in each group Patients completed the study (F/M): 36 (35/3) TCG: 18 FCG: 18 Mean age: TCG: 22.44 ± 3.55 FCG: 21.90 ± 3.60 | Class II Division 1, requiring maxillary 1st premolar extractions followed by en masse retraction. | No significant differences in GI, PI, and papillary bleeding between FGC and TCG at T0 and T1 (p > 0.017), but significant differences between both groups at T2 (p < 0.017). No GR at examined teeth in both groups at T0, T1, and T2. All teeth preserved their vitality following both corticotomies. | Until canines reached Class I relationship with a correct incisor relationship. |
| Mahmoudzadeh et al., 2020 Iran [66] | split-mouth RCT, parallel study | Lasercision vs. conventional OT | Patients (F/M): 12 (9/3) Dropouts: None Control: 12 Exp.: 12 Mean age:18.91 ± 3.87 (15–30) | Malocclusions requiring bilateral maxillary 1st premolar extractions. | No significant difference in GI between the laser and control groups at baseline and 1 month after the intervention (p = 0.55). No significant difference between the laser and control sides in WAG neither before nor after the retraction. | 1 month |
| Patterson et al., 2017 Australia and Greece [70] | split-mouth CCT | Piezocision vs. conventional OT | Patients (F/M): 14 (8/6) Dropouts: None Control: 14 Exp.: 14 Mean age: 16.2 (13.1–19) | Malocclusions requiring maxillary 1st premolars extractions. | Statistically greater RR (p < 0.05) on the Piezo sides than the control sides (p = 0.029). Piezocision resulted in an average of 0.133 mm3, or 44%, increase in RR. | 4 weeks |
| Raj et al., 2020 India [51] | split-mouth RCT, prospective study | Piezocision vs. conventional OT | Patients (F/M): 26 Did not receive the intervention: 2 (1 in each group) Lost to follow-up: 4 (2 in each group due to lack of attendance) Excluded due to incomplete data: 6 (3 in each group) Patients completed the study (F/M): 20 (14/6) Control: 20 Exp.: 20 Mean age: 23.18 ± 1.41 (20–25) | Class II, requiring 1st premolar extractions, with subsequent maxillary canine retraction. | No statistically significant difference in PI. Increase in PD in both groups between the baseline and 6 months and statistically significant increase in RAL (p < 0.05). Statistically significant greater increase in buccal and mesial ABL in the Piezo side (p < 0.05). Statistically significant increase in RR after 6 months in both groups (p < 0.001). | 6 months |
| Ravi et al., 2022 India [55] | split-mouth RCT | Piezocision vs. conventional OT | Patients (F/M): 15 (NA) Piezo (Group II): 15 Control (Group I): 15 Mean age: 18–26 | Malocclusions requiring maxillary 1st premolar extractions, with subsequent maxillary canine retraction. | No statistically significant difference in the RR between the two groups. | 90 days |
| Raza et al., 2021 India [37] | split-mouth RCT, single-centered, parallel-group | Corticotomy vs. conventional OT | Patients (F/M): 10 (4/2) Dropouts: None Control: 10 Exp.: 10 Mean age: 18–25 | Malocclusions requiring maxillary 1st premolar extractions, with subsequent maxillary canine retraction. | Statistically significant (p < 0.05) decreased RR at the corticotomy sides compared with the control sides. | Until the completion of canine retraction. (Exp.: 5.7 months, Control: 7.1 months) |
| Salman and Ali 2014 Iraq [22] | split-mouth CCT | Lasercision vs. conventional OT | Patients (F/M): 15 (10/5) Dropouts: None Control: 15 Exp.: 15 Mean age: 21.7 (17–28) | Class I or II, requiring bilateral maxillary 1st premolar extractions, with subsequent maxillary canine retraction. | No significant change in gingival sulcus depth around maxillary canines (<4 mm pre- and post-surgery). No pathologic changes in PDL on periapical radiograph; no change in tooth vitality. No sign of gingival inflammation or scar formation. | 6 weeks |
| Shahrin et al., 2021 Malaysia [63] | RCT, prospective, single-center, two-arm parallel study | MOPs vs. conventional OT | Patients (F/M): 30 (25/5) Dropouts: 2 (1 lost to follow-up in the control group, 1 discontinued MOPs due to pregnancy) Patients completed the study: 28 Control: 14 Exp.: 14 Mean age: 22.66 ± 3.27 | Moderate maxillary anterior crowding of 5–8 mm. | No significant difference in root length between the MOP and control groups. | 6 months |
| Shoreibah et al., 2012 a Egypt [35] | RCT, prospective, parallel arms | Corticotomy vs. conventional OT | Patients (F/M): 20 (17/3) Dropouts: None Group I (Corticotomy): 10 Group II (Conventional): 10 Mean age: 18.4–25.6 | Class I skeletal pattern with moderate mandibular anterior crowding of 3–5 mm. | Six months post-treatment, both groups showed a decrease in PD, which was non-significant. No statistically significant difference in BD between the two groups from baseline to six months post-treatment. | 6 months |
| Shoreibah et al., 2012 b Egypt [36] | RCT, prospective, parallel arms | Corticotomy vs. corticotomy + bioactive glass | Patients (F/M): 20 (16/4) Group I: 10 Group II: 10 Dropouts: 3 lost to follow-up After 6 months: 17 patients follow-up records available Mean age: 24.5 | Class I skeletal pattern with moderate mandibular anterior crowding of 3–5 mm. | Six months post-treatment, both groups demonstrated a decrease in PD, which was non-significant. Statistically significant difference between groups in BD from the baseline to six months post-orthodontic treatment. No statistically significant difference in root length in both groups. | 6 months |
| Singh and Jayan 2019 India [39] | RCT | PAOO vs. conventional OT | Patients (F/M): 30 (NA) Dropouts: None Group I (PAOO): 15 Group II (Conventional): 15 Mean age: 18–40 | Bimaxillary dentoalveolar protrusion. | Statistically significant difference in PD, PI, and GI between the groups, with Group I displaying better results than Group II. No statistically significant difference in the gingival bleeding index and RR. | Until the completion of retraction. (Group I: 12.7 months, Group II: 21.2 months) |
| Sirri et al., 2020 Syria [43] | RCT, two-arm parallel-group | Corticision vs. conventional OT | Patients (F/M): 60 (41/19) Dropouts: None Control: 30 (20/10) Exp.: 30 (21/9) Mean age: 21.40 ± 1.63 | Mild and moderate crowding (<6 mm according to Little’s index). | No significant differences in the periodontal parameters (PD, PI, GI, WAG). Increase in the PI on the buccal surface in corticision and control groups. Increase in PD on the buccal surface in the corticision and control groups, which were statistically insignificant. Increase in GI on the buccal surface in the corticision and control groups. WAG on the buccal surface in the corticision and control groups. | Until leveling and alignment (Little’s index < 1 mm). |
| Sirri et al., 2021 Syria [44] | RCT, two-arm parallel-group | Corticision vs. conventional OT | Patients (F/M): 52 (38/14) Dropouts: None Control: 26 (18/8) Exp.: 26 (20/6) Mean age: 21.38 | Mild to moderate crowding of the lower anterior teeth (2–6 mm according to Little’s index). | No statistically significant difference was observed between the two groups concerning the overall mean value of EARR after the alignment (p = 0.436). No statistically significant difference between the two groups regarding the distribution of DF (p = 0.780). | Until leveling and alignment (Little’s index < 1 mm). |
| Sultana et al., 2022 Malaysia [54] | RCT, single-centered, two-arm parallel-group | Piezocision vs. conventional OT | Patients (F/M): 16 (NA) Piezo: 8 Control: 8 Dropouts: 3 (2 in Piezo, 1 in the control group) due to COVID-19 pandemic restrictions. Patients completed the study (F/M): 13 (NA) Piezo: 6 Control: 7 Mean age: Piezo: 20.83 ± 2.32, Control: 21.14 ± 2.97 | Severe anterior maxillary crowding, requiring bilateral 1st premolar extractions (7–9 mm according to Little’s index). | No significant change in PD and AL between T3–T0 in both groups (p > 0.05), and all teeth preserved their vitality during the study. | Until complete leveling and alignment |
| Suryavanshi et al., 2015 India [71] | split-mouth CCT | Corticotomy vs. conventional OT | Patients (F/M): 10 Control: 10 Exp.: 10 Mean age: 18–35 | Class II Division 1, large overjet, requiring maxillary 1st premolar extractions | No clinical evidence of GR or any periodontal damage, tooth mobility, or radiographic evidence of RR. No loss of vitality was noted. | Until the completion of canine retraction. 6 months follow-up. |
| Thomas et al., 2021 India [64] | split-mouth RCT | MOPs vs. conventional OT | Patients (F/M): 33 (24/9) Dropouts: 3 (lost to follow-up) Patients completed the study: 30 Control: 30 Exp.: 30 Mean age: 22.1 ± 2.19 (19–25) | Class I or Class II Division I bilateral maxillary protrusion, requiring 1st premolar extractions, with subsequent maxillary canine retraction. | Statistically significant increase in the PD following 90 days of retraction on both sides. No significant change in AL in intragroup and intergroup comparisons. No significant change in root length between the sides. ABL showed no statistically significant difference in any surfaces. | 90 days |
| Study | Methods | Participants | Interventions | Outcomes | Notes | ||||
|---|---|---|---|---|---|---|---|---|---|
| ID | Setting | Trial Name/Title | Study Design | Treatment Comparison | Sample Size, Gender, Age, Malocclusion | Type and Site of Intervention/Technical Aspects of Interventions & Orthodontic Aspects | Duration/Follow-Up Period | Primary and Secondary | |
| NCT04631419 Register: Clinical.Trials.gov | Orthodontic department, Faculty of dentistry, Suez Canal University, Ismailia, Egypt | Effects of Flapless Laser Corticotomy in Canine Retraction |
| Flapless laser corticotomy vs. conventional OT (canine retraction) | N = 14 Both (F and M) 18 and older Dental malocclusion, bimaxillary protrusion. |
| 3 months | Primary outcomes: Rate of canine retraction. Secondary outcomes: Canine rotation, 1st molar anchorage loss, root resorption, periodontal condition, pulp vitality. | Status: Active, not recruiting Starting date: 1 June 2018 Completion date: June 2021 |
| NCT05265416 Register: Clinical.Trials.gov | University of Damascus, Damascus, Syrian Arab Republic | Pain and Discomfort and Periodontal Status in Two Acceleration Methods of Canine Retraction |
| Piezocision vs. conventional OT (canine retraction) | N = 58 Both (F and M) 17 to 28 years Class II malocclusion. |
| 3–4 months | Primary outcomes: change in the levels of pain, discomfort, swelling, levels of eating difficulty, change in the levels of satisfaction. Secondary outcomes: Plaque index, gingival index, bleeding index, Probing depth. | Status: Recruiting Starting date: 22 October 2021 Completion date: 30 November 2022 |
| CTRI/2018/05/013550 Register: Cochrane Library | Department of Orthodontics, Nair Hospital Dental College, Mumbai, India | A study to find out effect of small perforations in gums for faster teeth movement using braces |
| MOPs vs. conventional OT | N = 40 Both (F and M) 18 to 30 years Class I malocclusion, bimaxillary protrusion, less than 4 mm crowding in each arch. |
| 18 months | Primary outcomes: Rates of maxillary and mandibular anterior teeth en masse retraction in the intervention and control groups, Total duration of en masse retraction. Secondary outcomes: Root resorption of anterior teeth in both groups, Pain assessment after placement of MOPs. | Status: Open to Recruitment Starting date: 1 May 2018 Completion date: NA |
| CTRI/2021/05/033657 Register: Cochrane Library | Department of Orthodontics, Coorg Institute of Dental Sciences, Karnataka, India | A study used to determine in which among the two methods of fastest orthodontic tooth movement have more amount of root resorption |
| Group A: Piezocision vs. conventional OT Group B: Platelet rich plasma (PRP) vs. conventional OT | N = 20 Both (F and M) 18 to 45 years Class I malocclusion indicated for bilateral maxillary 1st premolar extraction. |
| 6 months | Primary outcomes: Rate of root resorption in the piezocision and PRP groups. Secondary outcomes: Compare the rate of root resorption between the piezocision and PRP groups. | Status: Not Yet Recruiting Starting date: 15 June 2021 Completion date: NA |
| CTRI/2018/10/015894 Register: Cochrane Library | Department of Orthodontics and Dentofacial Orthopaedics, Surendera Dental College and Research Institute, Sriganganagar, Rajasthan, India | Comparison of different methods of canine movement |
| Group 1: Corticotomy vs. conventional OT Group 2: Low level laser irradiation vs. conventional OT Group 3: Piezocision vs. conventional OT | N = 45 Both (F and M) 14 to 25 years Class I malocclusion with large overjet or bimaxillary protrusion, or Class II Division 1 malocclusion, with large overjet, requiring therapeutic bilateral 1st premolar extractions with the subsequent retraction of canine. |
| 63 days | Primary outcomes: Amount of tooth movement, rate of tooth movement, or treatment time. Secondary outcomes: amount of root resorption of canine in the 3 interventions. | Status: Not Yet Recruiting Starting date: 10 May 2018 Completion date: NA |
| CTRI/2022/01/039459 Register: Cochrane Library | Department of Orthodontics and Dentofacial Orthopedics, Saveetha Dental College and Hospital, India | A clinical trial to compare the speed of alignment of lower front teeth using two different methods of accelerating tooth movement |
| MOP vs. conventional OT Lasercision vs. conventional OT | N = 33 Both (F and M) 16 to 35 years Moderate crowding (Littles irregularity index > 4 mm) requiring therapeutic mandibular 1st premolar extractions. |
| 6–7 months | Primary outcomes: Rate of decrowding in lower anterior regions. Secondary outcomes: Bone changes- cortical bone height and thickness, root resorption. | Status: Not Yet Recruiting Starting date: 20 January 2022 Completion date: NA |
| Study | Randomization | Deviations from Intended Interventions | Missing Outcome Data | Measurement of the Outcome | Selection of the Reported Result | Overall |
|---|---|---|---|---|---|---|
| Abbas et al., 2012 [40] | Some concerns | Some concerns | Low | High | Low | High |
| Abbas et al., 2016 [41] | Low | Some concerns | Low | Low | Low | Some concerns |
| Abdelqader 2019 [45] | Some concerns | Some concerns | Low | Low | Low | Some concerns |
| Aboalnaga et al., 2019 [60] | Low | Some concerns | Low | Low | Low | Some concerns |
| Aboul-Ela et al., 2011 [34] | Some concerns | Some concerns | Low | Some concerns | Low | Some concerns |
| Agrawal et al., 2018 [65] | Some concerns | Some concerns | Low | Some concerns | Low | Some concerns |
| Aksakalli et al., 2016 [48] | Some concerns | Some concerns | Low | Low | Low | Some concerns |
| Alkebsi et al., 2018 [59] | Low | Some concerns | Low | Low | Low | Some concerns |
| Alqadasi et al., 2019 [57] | Low | Some concerns | Low | Low | Some concerns | Some concerns |
| Alqadasi et al., 2020 [58] | Low | Some concerns | Low | Low | Low | Some concerns |
| Aristizabal et al., 2016 [38] | Some concerns | Some concerns | Low | Some concerns | Low | Some concerns |
| Bahammam 2016 [42] | Low | Some concerns | High | High | Low | High |
| Bansal et al., 2019 [61] | Low | Some concerns | Low | Low | Low | Some concerns |
| Charavet et al., 2016 [49] | Some concerns | Some concerns | Low | Some concerns | Some concerns | Some concerns |
| Charavet et al., 2019 [50] | Low | Some concerns | Low | Low | Some concerns | Some concerns |
| Elkalza et al., 2018 [56] | Low | Some concerns | Low | Low | Low | Some concerns |
| Gulduren et al., 2020 [62] | Low | Low | Low | Low | Low | Low |
| Hatrom et al., 2021 [52] | Low | Some concerns | Low | Low | Low | Some concerns |
| Karci and Baka 2021 [53] | Some concerns | Some concerns | Low | Some concerns | Low | Some concerns |
| Khlef et al., 2020 [46] | Low | Some concerns | Low | High | Low | High |
| Khlef et al., 2022 [47] | Low | Some concerns | Low | Low | Low | Some concerns |
| Mahmoudzadeh et al., 2020 [66] | Low | Some concerns | Low | Low | Low | Some concerns |
| Raj et al., 2020 [51] | Low | Some concerns | Low | Low | Low | Some concerns |
| Ravi et al., 2022 [55] | Some concerns | Some concerns | Low | Low | Low | Some concerns |
| Raza et al., 2021 [37] | Low | Some concerns | Low | Low | Low | Some concerns |
| Shahrin et al., 2021 [63] | Low | Some concerns | Low | High | Low | High |
| Shoreibah et al., 2012 a [35] | Some concerns | Some concerns | Low | High | Low | High |
| Shoreibah et al., 2012 b [36] | Some concerns | Some concerns | Low | High | Low | High |
| Singh and Jayan 2019 [39] | Some concerns | Some concerns | Low | High | Low | High |
| Sirri et al., 2020 [43] | Low | Some concerns | Low | Low | Low | Some concerns |
| Sirri et al., 2021 [44] | Low | Some concerns | Low | Low | Low | Some concerns |
| Sultana et al., 2022 [54] | Low | Some concerns | Low | Low | Low | Some concerns |
| Thomas et al., 2021 [64] | Low | Some concerns | Low | Low | Low | Some concerns |
| Study | Bias Due to/in… | |||||||
|---|---|---|---|---|---|---|---|---|
| Confounding | Selection of Participants into the Study | Classification of Interventions | Deviations from Intended Interventions | Missing Data | Measurement of Outcomes | Selection of the Reported Result | Overall | |
| Abed and Al Bustani 2013 [67] | Serious | Low | Low | Low | Low | Moderate | No Information | Serious |
| Arana et al., 2022 [68] | Low | Low | Serious | Low | Low | Moderate | Low | Serious |
| Chan et al., 2018 [69] | Low | Low | Serious | Low | Low | Low | Low | Serious |
| Patterson et al., 2017 [70] | Low | Low | Serious | Low | Low | Low | Low | Serious |
| Salman and Ali 2014 [22] | Serious | Low | Serious | Low | Low | Moderate | No Information | Serious |
| Suryavanshi et al., 2015 [71] | Serious | Low | Serious | Low | Low | Moderate | No Information | Serious |
References
- Tsichlaki, A.; Chin, S.Y.; Pandis, N.; Fleming, P.S. How long does treatment with fixed orthodontic appliances last? A systematic review. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Talic, N.F. Adverse effects of orthodontic treatment: A clinical perspective. Saudi Dent. J 2011, 23, 55–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segal, G.R.; Schiffman, P.H.; Tuncay, O.C. Meta analysis of the treatment-related factors of external apical root resorption. Orthod. Craniofac. Res 2004, 7, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Rodd, H.D.; Baker, S.R.; Marshman, Z.; Robinson, P.G.; Benson, P.E. Are social judgements made by children in relation to orthodontic appliances? J. Orthod. 2010, 37, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Jeremiah, H.G.; Bister, D.; Newton, J.T. Social perceptions of adults wearing orthodontic appliances: A cross-sectional study. Eur. J. Orthod. 2011, 33, 476–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosvall, M.D.; Fields, H.W.; Ziuchkovski, J.; Rosenstiel, S.F.; Johnston, W.M. Attractiveness, acceptability, and value of orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 276–277. [Google Scholar] [CrossRef]
- Fleming, P.S.; Fedorowicz, Z.; Johal, A.; El-Angbawi, A.; Pandis, N. Surgical adjunctive procedures for accelerating orthodontic treatment. Cochrane Database Syst. Rev. 2015, 2015, CD010572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uribe, F.; Padala, S.; Allareddy, V.; Nanda, R. Patients’, parents’, and orthodontists’ perceptions of the need for and costs of additional procedures to reduce treatment time. Am. J. Orthod. Dentofac. Orthop. 2014, 145, S65–S73. [Google Scholar] [CrossRef]
- Fathimani, M.; Melenka, G.W.; Romanyk, D.L.; Toogood, R.W.; Heo, G.; Carey, J.P.; Major, P.W. Development of a standardized testing system for orthodontic sliding mechanics. Prog. Orthod. 2015, 16, 14. [Google Scholar] [CrossRef] [Green Version]
- McGorray, S.P.; Dolce, C.; Kramer, S.; Stewart, D.; Wheeler, T.T. A randomized, placebo-controlled clinical trial on the effects of recombinant human relaxin on tooth movement and short-term stability. Am. J. Orthod. Dentofacial. Orthop. 2012, 141, 196–203. [Google Scholar] [CrossRef]
- Kau, C.H.; Kantarci, A.; Shaughnessy, T.; Vachiramon, A.; Santiwong, P.; de la Fuente, A.; Skrenes, D.; Ma, D.; Brawn, P. Photobiomodulation accelerates orthodontic alignment in the early phase of treatment. Prog. Orthod. 2013, 14, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz, D.R.; Kohara, E.K.; Ribeiro, M.S.; Wetter, N.U. Effects of low-intensity laser therapy on the orthodontic movement velocity of human teeth: A preliminary study. Lasers Surg. Med. 2004, 35, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Nimeri, G.; Kau, C.H.; Abou-Kheir, N.S.; Corona, R. Acceleration of tooth movement during orthodontic treatment–a frontier in orthodontics. Prog. Orthod. 2013, 14, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kole, H. Surgical operations on the alveolar ridge to correct occlusal abnormalities. Oral Surg. Oral Med. Oral Pathol. 1959, 12, 515–529. [Google Scholar] [CrossRef] [PubMed]
- Wilcko, W.M.; Wilcko, T.; Bouquot, J.E.; Ferguson, D.J. Rapid orthodontics with alveolar reshaping: Two case reports of decrowding. Int. J. Period. Restor. Dent. 2001, 21, 9–19. [Google Scholar]
- Frost, H.M. The regional acceleratory phenomenon: A review. Henry Ford Hosp. Med. J. 1983, 31, 3–9. [Google Scholar]
- Hassan, A.H.; Al-Fraidi, A.A.; Al-Saeed, S.H. Corticotomy-assisted orthodontic treatment: Review. Open Dent. J. 2010, 4, 159–164. [Google Scholar] [CrossRef] [Green Version]
- Alghamdi, A.S. Corticotomy facilitated orthodontics: Review of a technique. Saudi Dent. J. 2010, 22, 8. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.J.; Park, Y.G.; Kang, S.G. Effects of Corticision on paradental remodeling in orthodontic tooth movement. Angle Orthod. 2009, 79, 284–291. [Google Scholar] [CrossRef]
- Dibart, S.; Sebaoun, J.D.; Surmenian, J. Piezocision: A minimally invasive, periodontally accelerated orthodontic tooth movement procedure. Compend. Contin. Educ. Dent. 2009, 30, 342–344, 346, 348–350. [Google Scholar]
- Alikhani, M.; Raptis, M.; Zoldan, B.; Sangsuwon, C.; Lee, Y.B.; Alyami, B.; Corpodian, C.; Barrera, L.M.; Alansari, S.; Khoo, E.; et al. Effect of micro-osteoperforations on the rate of tooth movement. Am. J. Orthod. Dentofacial. Orthop. 2013, 144, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Salman, L.H.; Ali, F.A. Acceleration of canine movement by laser assisted flapless corticotomy [An innovative approach in clinical orthodontics]. J. Baghdad Coll. Dent. 2014, 26, 133–137. [Google Scholar] [CrossRef]
- Gantes, B.; Rathbun, E.; Anholm, M. Effects on the periodontium following corticotomy-facilitated orthodontics. Case reports. J Periodontol. 1990, 61, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Gil, A.P.S.; Haas, O.L., Jr.; Mendez-Manjon, I.; Masia-Gridilla, J.; Valls-Ontanon, A.; Hernandez-Alfaro, F.; Guijarro-Martinez, R. Alveolar corticotomies for accelerated orthodontics: A systematic review. J. Craniomaxillofac. Surg. 2018, 46, 438–445. [Google Scholar] [CrossRef]
- Patterson, B.M.; Dalci, O.; Darendeliler, M.A.; Papadopoulou, A.K. Corticotomies and Orthodontic Tooth Movement: A Systematic Review. J. Oral Maxillofac. Surg. 2016, 74, 453–473. [Google Scholar] [CrossRef]
- Gkantidis, N.; Mistakidis, I.; Kouskoura, T.; Pandis, N. Effectiveness of non-conventional methods for accelerated orthodontic tooth movement: A systematic review and meta-analysis. J. Dent. 2014, 42, 1300–1319. [Google Scholar] [CrossRef] [PubMed]
- Dab, S.; Chen, K.; Flores-Mir, C. Short- and long-term potential effects of accelerated osteogenic orthodontic treatment: A systematic review and meta-analysis. Orthod. Craniofac. Res. 2019, 22, 61–68. [Google Scholar] [CrossRef]
- Alfawal, A.M.; Hajeer, M.Y.; Ajaj, M.A.; Hamadah, O.; Brad, B. Effectiveness of minimally invasive surgical procedures in the acceleration of tooth movement: A systematic review and meta-analysis. Prog. Orthod. 2016, 17, 33. [Google Scholar] [CrossRef] [Green Version]
- Higgins, T.J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3; Updated February 2022; Cochrane: London, UK, 2022. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.; Hernan, M.A.; Reeves, B.C.; Savovic, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aboul-Ela, S.M.; El-Beialy, A.R.; El-Sayed, K.M.; Selim, E.M.; El-Mangoury, N.H.; Mostafa, Y.A. Miniscrew implant-supported maxillary canine retraction with and without corticotomy-facilitated orthodontics. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Shoreibah, E.A.; Salama, A.E.; Attia, M.S.; Abu-Seida, S.M. Corticotomy-facilitated orthodontics in adults using a further modified technique. J. Int. Acad. Periodontol. 2012, 14, 97–104. [Google Scholar]
- Shoreibah, E.A.; Ibrahim, S.A.; Attia, M.S.; Diab, M.M. Clinical and radiographic evaluation of bone grafting in corticotomy-facilitated orthodontics in adults. J. Int. Acad. Periodontol. 2012, 14, 105–113. [Google Scholar]
- Raza, M.; Sharma, P.; Kumar, P.; Vaish, S.; Pathak, B. Comparison of canine retraction by conventional and corticotomy-facilitated methods: A split mouth clinical study. J. Orthod. Sci. 2021, 10, 9. [Google Scholar] [CrossRef]
- Aristizabal, J.F.; Bellaiza, W.; Ortiz, M.A.; Franco, L. Clinical and Systemic Effects of Periodontally Accelerated Osteogenic Orthodontics: A Pilot Study. Int. J. Odontostomatol. 2016, 10, 119–127. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Jayan, B. Comparative Evaluation of Periodontally Accelerated Osteogenic Orthodontics (PAOO) Versus Conventional Orthodontic Tooth Movement in Adult Patients with Bimaxillary Dentoalveolar Protrusion. Int. J. Period. Restor. Dent. 2019, 39, 571–577. [Google Scholar] [CrossRef]
- Abbas, I.T.; Moutamed, G.M. Acceleration of orthodontic tooth movement by alveolar corticotomy using piezosurgery. J. Am Sci. 2012, 8, 13–19. [Google Scholar]
- Abbas, N.H.; Sabet, N.E.; Hassan, I.T. Evaluation of corticotomy-facilitated orthodontics and piezocision in rapid canine retraction. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 473–480. [Google Scholar] [CrossRef]
- Bahammam, M.A. Effectiveness of bovine-derived xenograft versus bioactive glass with periodontally accelerated osteogenic orthodontics in adults: A randomized, controlled clinical trial. BMC Oral Health 2016, 16, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sirri, M.; Burhan, A.; Hajeer, M.Y.; Nawaya, F.; Abdulhadi, A. Efficiency of Corticision in Accelerating Leveling and Alignment of Crowded Lower Anterior Teeth in Young Adult Patients: A Randomised Controlled Clinical Trial. J. Clin. Diagn. Res. 2020, 14, 4149. [Google Scholar] [CrossRef]
- Sirri, M.R.; Burhan, A.S.; Hajeer, M.Y.; Nawaya, F.R. Evaluation of corticision-based acceleration of lower anterior teeth alignment in terms of root resorption and dehiscence formation using cone-beam computed tomography in young adult patients: A randomized controlled trial. Int. Orthod. 2021, 19, 580–590. [Google Scholar] [CrossRef] [PubMed]
- Abdelqader, N.V. Comparison between Corticision versus Corticotomy Assisted Canine Retraction in Adult Patients: A Randomized Clinical Trial (Split Mouth Design, Thesis Submitted as a Fullfilment of Requirements for the MSc in Orthodontics). Master’s Thesis, Cairo University, Cairo, Egypt, 2021. [Google Scholar]
- Khlef, H.N.; Hajeer, M.Y.; Ajaj, M.A.; Heshmeh, O.; Youssef, N.; Mahaini, L. The effectiveness of traditional corticotomy vs flapless corticotomy in miniscrew-supported en-masse retraction of maxillary anterior teeth in patients with Class II Division 1 malocclusion: A single-centered, randomized controlled clinical trial. Am. J. Orthod. Dentofac. Orthop. 2020, 158, e111–e120. [Google Scholar] [CrossRef] [PubMed]
- Khlef, H.N.; Hajeer, M.Y. Is It Possible to Achieve Favorable Accelerated Dental Changes with No Periodontal Complications When Retracting Upper Anterior Teeth Assisted by Flapless Corticotomy Compared to Traditional Corticotomy? A Two-Arm Randomized Controlled Trial. Sci. World J. 2022, 2022, 4261248. [Google Scholar] [CrossRef]
- Aksakalli, S.; Calik, B.; Kara, B.; Ezirganli, S. Accelerated tooth movement with piezocision and its periodontal-transversal effects in patients with Class II malocclusion. Angle Orthod. 2016, 86, 59–65. [Google Scholar] [CrossRef]
- Charavet, C.; Lecloux, G.; Bruwier, A.; Rompen, E.; Maes, N.; Limme, M.; Lambert, F. Localized Piezoelectric Alveolar Decortication for Orthodontic Treatment in Adults: A Randomized Controlled Trial. J. Dent. Res. 2016, 95, 1003–1009. [Google Scholar] [CrossRef]
- Charavet, C.; Lecloux, G.; Jackers, N.; Albert, A.; Lambert, F. Piezocision-assisted orthodontic treatment using CAD/CAM customized orthodontic appliances: A randomized controlled trial in adults. Eur. J. Orthod. 2019, 41, 495–501. [Google Scholar] [CrossRef]
- Raj, S.C.; Praharaj, K.; Barik, A.K.; Patnaik, K.; Mahapatra, A.; Mohanty, D.; Katti, N.; Mishra, D.; Panda, S.M. Retraction With and Without Piezocision-Facilitated Orthodontics: A Randomized Controlled Trial. Int. J. Periodont. Restor. Dent. 2020, 40, e19–e26. [Google Scholar] [CrossRef]
- Hatrom, A.A.; Howait, M.S.; Zawawi, K.H.; Al-Turki, G.A.; Alansari, R.A.; Almehayawi, N.F.; Alammari, S.H.; Mohammed, R.A.; Hassan, A.H. Pulp volume changes after piezocision-assisted tooth movement: A randomized clinical trial. BMC Oral Health 2021, 21, 28. [Google Scholar] [CrossRef]
- Cagli Karci, I.; Baka, Z.M. Assessment of the effects of local platelet-rich fibrin injection and piezocision on orthodontic tooth movement during canine distalization. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Sultana, S.; Ab Rahman, N.; Zainuddin, S.L.A.; Ahmad, B. Effect of piezocision procedure in levelling and alignment stage of fixed orthodontic treatment: A randomized clinical trial. Sci. Rep. 2022, 12, 6230. [Google Scholar] [CrossRef] [PubMed]
- Ravi, M.S.; Murali, P.S.; Kumari, V.; Hamidi, W.; Sneha, K.; Soans, C. Radiographic and histochemical assessment of root resorption during canine retraction through piezocision site. Indian. J. Dent. Res. 2021, 32, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Elkalza, A.; Hashem, A.; Alam, M. Comparative study of root resorption between two methods for accelerated orthodontic tooth movement. J. Oral Res. 2018, 7, 348–353. [Google Scholar] [CrossRef] [Green Version]
- Alqadasi, B.; Aldhorae, K.; Halboub, E.; Mahgoub, N.; Alnasri, A.; Assiry, A.; Xia, H.Y. The Effectiveness of Micro-osteoperforations during Canine Retraction: A Three-dimensional Randomized Clinical Trial. J. Int. Soc. Prev. Community Dent. 2019, 9, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Alqadasi, B.; Xia, H.Y.; Alhammadi, M.S.; Hasan, H.; Aldhorae, K.; Halboub, E. Three-dimensional assessment of accelerating orthodontic tooth movement-micro-osteoperforations vs piezocision: A randomized, parallel-group and split-mouth controlled clinical trial. Orthod. Craniofac. Res. 2021, 24, 335–343. [Google Scholar] [CrossRef]
- Alkebsi, A.; Al-Maaitah, E.; Al-Shorman, H.; Abu Alhaija, E. Three-dimensional assessment of the effect of micro-osteoperforations on the rate of tooth movement during canine retraction in adults with Class II malocclusion: A randomized controlled clinical trial. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 771–785. [Google Scholar] [CrossRef]
- Aboalnaga, A.A.; Salah Fayed, M.M.; El-Ashmawi, N.A.; Soliman, S.A. Effect of micro-osteoperforation on the rate of canine retraction: A split-mouth randomized controlled trial. Prog. Orthod. 2019, 20, 21. [Google Scholar] [CrossRef] [Green Version]
- Bansal, M.; Sharma, R.; Kumar, D.; Gupta, A. Effects of mini-implant facilitated micro-osteoperforations in alleviating mandibular anterior crowding: A randomized controlled clinical trial. J. Orthod. Sci. 2019, 8, 19. [Google Scholar] [CrossRef]
- Gulduren, K.; Tumer, H.; Oz, U. Effects of micro-osteoperforations on intraoral miniscrew anchored maxillary molar distalization: A randomized clinical trial. J. Orofac. Orthop. 2020, 81, 126–141. [Google Scholar] [CrossRef]
- Shahrin, A.A.; Ghani, S.H.A.; Norman, N.H. Effect of micro-osteoperforations on external apical root resorption: A randomized controlled trial. Korean J. Orthod. 2021, 51, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Das, S.K.; Barik, A.K.; Raj, S.C.; Rajasekaran, A.; Mishra, M. Evaluation of physiodispenser assisted micro-osteoperforation on the rate of tooth movement and associated periodontal tissue status during individual canine retraction in first premolar extraction cases: A split-mouth randomized controlled clinical trial. J. World Fed. Orthod. 2021, 10, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.A.; Kolte, A.P.; Kolte, R.A.; Vaswani, V.; Shenoy, U.; Rathi, P. Comparative CBCT analysis of the changes in buccal bone morphology after corticotomy and micro-osteoperforations assisted orthodontic treatment–Case series with a split mouth design. Saudi Dent. J. 2019, 31, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudzadeh, M.; Poormoradi, B.; Alijani, S.; Farhadian, M.; Kazemisaleh, A. Efficacy of Er,Cr Laser incision Corticotomy in Rapid Maxillary Canine Retraction: A Split-Mouth Randomized Clinical Trial. J. Lasers Med. Sci. 2020, 11, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Albustani, A.; Abed, S. Corticotomy Assisted Orthodontic Canine Retraction. J. Baghdad Coll. Dent. 2013, 25, 5134. [Google Scholar] [CrossRef]
- Arana, J.G.; Rey, D.; Rios, H.; Alvarez, M.A.; Cevidanes, L.; Ruellas, A.C.; Aristizabal, J.F. Root resorption in relation to a modified piezocision technique. Angle Orthod. 2022, 92, 347–352. [Google Scholar] [CrossRef]
- Chan, E.; Dalci, O.; Petocz, P.; Papadopoulou, A.K.; Darendeliler, M.A. Physical properties of root cementum: Part 26. Effects of micro-osteoperforations on orthodontic root resorption: A microcomputed tomography study. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 204–213. [Google Scholar] [CrossRef]
- Patterson, B.M.; Dalci, O.; Papadopoulou, A.K.; Madukuri, S.; Mahon, J.; Petocz, P.; Spahr, A.; Darendeliler, M.A. Effect of piezocision on root resorption associated with orthodontic force: A microcomputed tomography study. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 53–62. [Google Scholar] [CrossRef]
- Suryavanshi, H.; Das, V.; Deshmukh, A.; Rai, R.; Vora, M. Comparison of rate of maxillary canine movement with or without modified corticotomy facilitated orthodontic treatment: A prospective clinical trial. APOS Trends Orthod. 2015, 5, 9410. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pouliezou, I.; Xenou, A.; Vavetsi, K.; Mitsea, A.; Sifakakis, I. Adverse Effects of Surgically Accelerated Orthodontic Techniques: A Systematic Review. Children 2022, 9, 1835. https://doi.org/10.3390/children9121835
Pouliezou I, Xenou A, Vavetsi K, Mitsea A, Sifakakis I. Adverse Effects of Surgically Accelerated Orthodontic Techniques: A Systematic Review. Children. 2022; 9(12):1835. https://doi.org/10.3390/children9121835
Chicago/Turabian StylePouliezou, Ioanna, Angeliki Xenou, Konstantina Vavetsi, Anastasia Mitsea, and Iosif Sifakakis. 2022. "Adverse Effects of Surgically Accelerated Orthodontic Techniques: A Systematic Review" Children 9, no. 12: 1835. https://doi.org/10.3390/children9121835