


Ultrasound Imaging-Based Methods for Assessing Biological Maturity during Adolescence and Possible Application in Youth Sport: A Scoping Review
 ,
, 
Abstract
:
1. Introduction
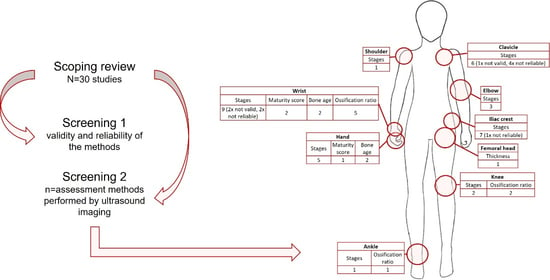
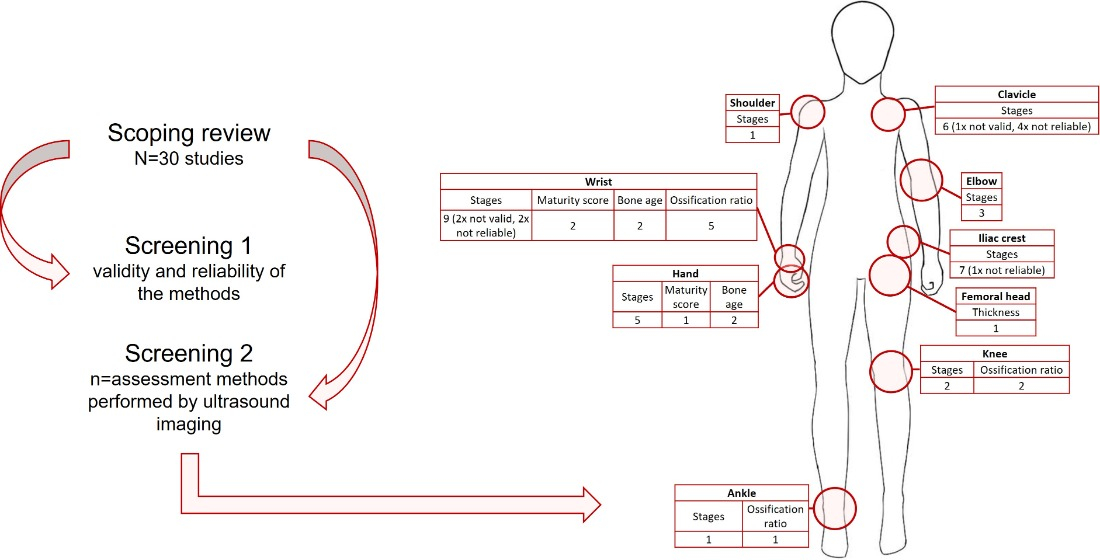
2. Methodology
2.1. Identifying the Research Question
2.2. Identifying Relevant Studies and Study Selection
2.3. Data Charting
3. Results
3.1. Collating, Summarizing the Data and Reporting the Results

{kind=link}
{kind=link}
| Comparator | US Body Region(s) | Study | Year | Country | Intervention and Aim(s) | Population | Domain | Methods | Examiners, Readers and Duration | Results and Conclusion | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| X-ray Iliac bone and left wrist | Iliac bone and left wrist | 1 | Wagner et al. [38] | 1995 | Germany | Sonographic and radiographic examination of the iliac bone apophysis (Risser’s sign) and the left distal radial epiphysis. Determination of skeletal maturity by ultrasound in order to reduce ionizing radiation to the growing skeleton. | 5–19 years of age 49 girls, 15 boys Idiopathic scoliosis | Pediatrics | US of ilium: Risser Grade (0–V) US of left wrist: Radial epiphysis open or closed (yes-no) X-ray of ilium: Risser Grade (0–V) X-ray of left wrist: Greulich and Pyle (atlas) | - | Valid Applicable |
| X-ray Iliac bone | Iliac bone | 2 | Thaler et al. [39] | 2008 | Austria | Determination of the accuracy of ultrasound evaluation of the Risser Grade as compared to plain radiography in patients with adolescent idiopathic scoliosis. | 7–17 years of age 36 females, 8 males Idiopathic scoliosis | Pediatrics | US and X-ray of ilium: Risser Grade (0–V) | US and X-ray: senior staff skeletal radiologists | Valid Applicable |
| X-ray Iliac bone | Iliac bone | 3 | Torlak et al. [40] | 2012 | Turkey | Assessment of the efficiency of ultrasonographic evaluation of Risser Sign compared with radiographic evaluation, and investigation of intraexaminer and interexaminer reliability of ultrasonographic evaluation. | 10–17 years of age 70 females, 72 males Minor pelvic trauma or scoliosis | Pediatrics | US and X-ray of ilium: Risser Grade (0–V) | US and X-ray: two orthopedists | Valid Reliable Applicable |
| X-ray Iliac bone | Iliac bone | 4 | Chauhan et al. [41] | 2019 | India | Sonographic and radiographic examination of the Risser Grade. Comparison of sonographic and radiographic epiphyseal iliac crest ossification for age estimation in living. | 10–22 years of age 28 females, 32 males Healthy | Pediatrics | US and X-ray of ilium: Risser Grade (0–V) | - | Valid Applicable |
| X-ray of left hand and wrist | Femoral head | 5 | Castriota-Scanderbeg et al. [42] | 1998 | Italy | Comparison of sonographically assessed thickness of femoral head cartilage and skeletal age determined by the GP and TW2 left hand radiograph by establishing the level of agreement between methods, the differences between the calculated skeletal age and chronological age, and the sensitivity, specificity, and predictive values of each method. | 1.3–21.3 years of age 56 females, 59 males Proven or suspected growth disorder | Pediatrics | US of hip: Femoral head cartilage thickness, skeletal ages derived from normal values obtained in a healthy Italian population (distance) X-ray of left hand and wrist: Greulich and Pyle, Tanner and Whitehouse II (atlas) | US: pediatric radiologist X-ray: experienced pediatric physician | Valid Applicable |
| X-ray of left hand and wrist | Wrist, knee, ankle | 6 | Wan et al. [43] | 2020 | China | Clarification of the correlations between the sonographic ossification ratios of the wrist, knee, and ankle, and the radiographic bone age in patients from infants to teenagers. Development of a new parameter to evaluate bone age with ossification ratios from bones with relatively higher correlations. | 0–19 years of age 139 females and 132 males No pathologic modifications of the wrist, knee and ankle | Pediatrics | US of wrist, knee and ankle: Ossification ratio X-ray of left hand and wrist: Tanner and Whitehouse III (atlas) | US examination: operators with experience for 1 and 3 years and trained with the protocol. US evaluation: radiologists 2.6 min | Valid Reliable Applicable |
| X-ray of left hand and wrist | Left wrist and knee | 7 | Wan et al. [26] | 2021 | China | Construction of score-for-age normal values and determination of the diagnostic performances of the method. Evaluation of ultrasonic bone age of the left hand and knee of pathologic patients with normal values of score for age. Comparison with X-ray assessment. | 0–19 years of age 511 females, 578 males Normal value group: without clinical diseases potentially affecting skeletal growth Validation group: clinically suspected growth disturbance | Pediatrics | US of left wrist and knee: Ossification ratio and the skeletal maturity score X-ray of left hand and wrist: Tanner and Whitehouse III, Greulich and Pyle (atlas) | US examination and evaluation: radiologists with 20, 6, 5, 1 years of experience and trained with the protocol X-ray: radiologists with 2 and 10 years of experience in bone age radiography evaluation 2 min ± 2 | Valid Reliable Applicable |
| X-ray of left hand and wrist | Left hand and wrist (GP + stages) | 8 | Ağırman et al. [36] | 2018 | Turkey | Assessment of the fit between the direct radiography and ultrasonography findings from the left hand–wrist and investigation of whether bone age and pubertal growth excretion are detectable with ultrasonography without ionizing radiation. | 10–17 years of age 82 females, 38 males Healthy | Dentistry | US and X-ray of left hand and wrist: Greulich and Pyle (atlas) and scoring system (I–V). | X-ray: technician with at least 5 years of working experience 2–3 min | Valid Reliable Applicable |
| X-ray of left hand and wrist | Left hand and wrist (GP + stages) | 9 | Razak and Meena [37] | 2018 | India | Assessment of the fit between the direct radiography and ultrasonography findings from the left hand–wrist and investigation of whether bone age and pubertal growth excretion are detectable with ultrasonography without ionizing radiation. | 10–17 years of age 82 females, 38 males Healthy | Dentistry | US and X-ray of left hand and wrist: Greulich and Pyle (atlas) and scoring system (I–V). | X-ray: technician with at least 5 years of working experience 2–3 min | Valid Reliable Applicable |
| X-ray of left hand and wrist | Left hand and wrist (SMS and OR) | 10 | Wan et al. [22] | 2019 | China | Assessment of the relationship between ultrasonic determination of ossification ratio and standard radiographic bone age from birth to near adulthood. Potential provision of a quantitative modality for estimation of bone age by conventional ultrasound. | 0.1–19 years of age 94 females and 78 males No pathologic modification of the hand and wrist | Pediatrics | US of left hand and wrist: Ossification ratio and skeletal maturity score. X-ray of the left hand and wrist: Tanner and Whitehouse III (atlas) | US examination: sonographic imaging specialist US evaluation: radiologists with experience in musculoskeletal ultrasound for 1, 2, and 3 years and trained for the protocol X-ray evaluation: radiologists 4–5 min | Valid Reliable Applicable (with caution) |
| X-ray of left hand and wrist | Hand and wrist (stages) | 11 | Nessi et al. [44] | 1997 | Italy | Examinations of the centers of ossification of the hand and wrist in adolescent by ultrasonographic compared to radiographic evaluation. Determination of the growth phases. | 7–16 years of age 26 patients Difference between physical development and chronological age | Dentistry | US and X-ray of the hand and wrist: Fishman stages (0–II) | US and X-ray: radiologists | Not valid Not applicable |
| X-ray of left hand and wrist | Hand and wrist (stages) | 12 | Giuca et al. [45] | 2002 | Italy | Comparison of the results of a sonographic and radiographic evaluation of the left hand and wrist. | 9–18 years of age 11 females, 14 males Delayed or precocious skeletal development | Pediatrics | US and X-ray of left hand and wrist: detection of the presence of growth cartilage (yes or no) | - | Not valid Not applicable |
| CT | Clavicular epiphyses | 13 | Gonsior et al. [46] | 2013 | Germany | Comparison of the staging results for both clavicles of the same subjects by sonography, computed tomography, and macroscopy. | 15.8–28.8 years of age 5 males Corpses without trauma of the clavicular epiphyses or cranial sternum region nor diseases affecting ossification process | Forensic medicine | US of the clavicular epiphyses: Classification following Schulz et al. (I–IV) CT of the clavicular epiphyses: Classification following Webb and Suchey (I–IV) Autopsy of the clavicular epiphyses: Classification following Webb and Suchey (I–IV) | US: one prepared and experienced examiner | Not valid Not applicable |
| MRI | Right knee | 14 | Herrmann et al. [25] | 2021 | Germany | Test of the feasibility of a US-based method for assessment of epiphyseal growth plate closure around the knee for forensic age estimation and comparison of the findings to MRI. | 14.4–19.3 years of age 33 males Healthy | Forensic medicine | US of the knee: Classification by stages (I–III) MRI of the knee: Classification following Jopp et al. (I–III) | US examination: radiologist MRI evaluation: readers with 5 years of experience in forensic medecine 2.65 ± 2.72 | Valid Reliable Applicable |
| US Body Region(s) | Study | Year | Country | Intervention and Aim(s) | Population | Domain | Methods | Examinators, Readers and Duration | Results and Conclusion | |
|---|---|---|---|---|---|---|---|---|---|---|
| Clavicle | 1 | Benito et al. [35] | 2018 | Spain | Determination of the fusion time of both sternal ends of the clavicle by ultrasonography. Evaluation of whether it may be used to estimate the legal age of adulthood in Spain. Reduction of minors’ exposure to radiation. | 5–30 years of age 146 females, 75 males | Forensic medicine | Sternal end of both clavicle: classification by Schulz et al. (I–IV) | - | Not reliable Applicable (with caution) |
| Clavicle | 2 | Quirmbach et al. [47] | 2009 | Germany | Assessment of whether the system could be used to evaluate the degree of ossification of the medial clavicular epiphyseal plate (both sides). Establish at what age full ossification could be demonstrated. See if this criterion, as proof that 21 years of age had been reached, could be demonstrated with the necessary degree of reliability required by criminal law. | 18–24 years of age 77 males Healthy | Forensic medicine | Both medial clavicular epiphyseal plate: classification by Schulz et al. (I–IV) | Examiners prepared for the experiment and trained for the method | Not reliable Not applicable |
| Clavicle | 3 | Schulz et al. [48] | 2008 | Germany | Determination of whether the ossification stage of the right medial clavicular epiphyses can also be determined by ultrasonography. | 12–30 years of age 39 females, 45 males Healthy | Forensic medicine | Right medial clavicular epiphyses: classification by Webb and Suchey (I–IV) | Physician qualified and certified | Reliable Applicable |
| Clavicle | 4 | Schulz et al. [49] | 2013 | Germany | Examination of the time frame of the ossification of right medial clavicular epiphysis in a large number of cases. | 10–25 years old 307 females, 309 males Healthy | Forensic medicine | Right medial clavicular epiphysis: classification by Schulz et al. (I–IV) | Qualified arthrosonographist | Reliable Applicable |
| Clavicle | 5 | Gonsior et al. [46] | 2016 | Germany | Evaluation of the stage of ossification of the medial clavicular epiphysis for both sides. Assessment of whether the determination of complete union of the medial clavicular epiphysis could be used as a criterion to prove that an individual had attained the age threshold of 18 years. | 14–26 years of age 215 females, 195 males Healthy | Forensic medicine | Both medial clavicular epiphysis: classification by Schulz et al. (I–IV) | Experienced or prepared examiners | Not reliable Not applicable |
| Humerus | 6 | Sánchez et al. [50] | 2017 | Spain | Determination whether the process of ossification of the proximal humeral epiphysis can be observed using the ultrasound technique and whether studying this is of any use in estimating legal age. | 5–30 years of age 146 females, 75 males | Forensic medicine | Proximal humeral epiphysis: classification in stages (0–V) | Forensic anthropologists and researcher | Reliable Applicable |
| Elbow | 7 | Schulz et al. [51] | 2014 | Germany | Examination of whether ultrasound examination of the ossification of the right olecranon could be used for the purposes of age estimation. | 10–25 years of age 307 females, 309 males Healthy | Forensic medicine | Right olecranon: classification by Schulz et al. (I–IV) | Physician qualified and certified in the area of arthrosonography | Reliable Applicable |
| Distal radius | 8 | Ekizoglu et al. [52] | 2021 | Turkey | Ultrasonographic evaluation of ossification of the left distal radius epiphysis to show its utility in forensic age estimation in living individuals. Assessment of the usability of US, as a nonionizing method, for pediatric age groups. Validation of the methodology of Schmidt et al.(2013) and comparison of the result obtained by those authors to Turkish population. | 9–25 years of age 366 females, 322 males Healthy | Forensic medicine | Left distal radius: classification by Schulz et al. (I–IV, modified) | Observers with 10 and 2 years of experience in forensic age estimation | Reliable Applicable |
| Distal radius | 9 | Schmidt et al. [53] | 2013 | Germany | Verify the potential of ultrasound techniques for use in assessing ossification of the right distal radial epiphysis and its chronological dependency as discovered in the course of the pilot study. | 10–25 years of age 306 females, 309 males Healthy | Forensic medicine | Right distal radial epiphysis: classification by Schulz et al. (I–IV) | Physicians with experience in imaging procedures in forensic age estimation and certified | Reliable Applicable |
| Distal radius | 10 | Karami et al. [54] | 2014 | Iran | Evaluation of the diagnostic accuracy (with a focus on sensitivity) of the ultrasonography in bone age determination with measuring the thickness of growth plate in the distal radius. Identification of subjects having growth plate width ≤ defined cut-off (positive test) and are actually over the determined age in each category according to the identity documents. | 15–20 years of age 82 males Healthy | Sport | Width of distal radial epiphysis, cut-off point for each category (distance) | Radiographist | Reliable Applicable |
| Distal radius | 11 | Karami et al. [55] | 2016 | Iran | Ultrasonographic examination of the epiphysis of the left distal radius. Evaluation of the effectiveness of ultrasound-based methods in a larger and more diverse socioeconomic group of older children, where the accuracy of this method seems to be least. | 14–18 years of age 100 females, 100 males Healthy | Sport | Width of left distal radial growth plate (distance) | Radiology residents | Reliable Applicable (with caution) |
| Iliac crest and olecranon | 12 | Pitlovic et al. [56] | 2013 | Croatia | Ultrasonographic examination of the iliac crest and the olecranon apophysis. Test of whether assessment of olecranon apophysis ossification by ultrasound has value in prediction of annal growth and peak height velocity. | 10–15 years of age 134 subjects Healthy | Pediatrics | Iliac crest: Risser grade (0–V) In subjects graded as Risser 0, olecranon apophysis: additional classification (0–VI) | Orthopedic surgeon and general surgeon | Not reliable Not applicable |
| Iliac crest | 13 | Schmidt et al. [57] | 2011 | Germany | Pilot-analysis of the forensic applicability of a sonographic evaluation of the apophyseal ossification of the iliac crest for skeletal age assessment. | 11–22 years of age 16 females, 23 males Healthy | Forensic medicine | Iliac crest: classification by Schulz et al. (I–IV) | Examiner certified in the field of skeletal sonography | Reliable Applicable |
| Iliac crest | 14 | Schmidt et al. [53] | 2013 | Germany | Examination of the value of skeletal sonography in assessing the age-dependent process of ossification of the apophysis of the Crista iliaca in a more extensive population. | 10–25 years of age 307 females, 309 males Healthy | Forensic medicine | Iliac crest: classification by Schulz et al. (I–IV) | Physicians with experience in imaging procedures used in forensic age estimation and certified | Reliable Applicable |
| Elbow and wrist | 15 | Shedge et al. [58] | 2021 | India | Establishment of the applicability of US, a non-invasive and safe technique, to visualize ossification centers of the left wrist and elbow joints for their appearance and fusion among boys between 14 and 17 years of age in the Ahmednagar region of India. | 13.73–17.04 years of age 31 males Healthy | Pediatrics | Left wrist and elbow: classification by Schmeling et al. (I–V) | Researcher | Reliable Applicable |
| Wrist, second metacarpophalangeal joint, knee, ankle | 16 | Windschall et al. [59] | 2020 | International | Ultrasonographic examination of the wrist, second metacarpophalangeal joint, knee and ankle vascularization, and their ossification grade. Assessment of the intra- and interobserver reliability of identification of normal joint vascularization in healthy children in different age groups and evaluation of the intra- and interobserver agreement of a new scoring system for assessing the grade of maturation of ossification nuclei in healthy children. | 2–16 years of age 5 females, 7 males Healthy | Pediatrics | Wrist, second metacarpophalangeal joint, knee and ankle: classification in stages (0–IV) | Minimum two years of expertise in pediatrics US | Reliable Applicable |
3.2. Validity, Reliability, and Acceptance
3.3. Usability, Practicability, and Economy
4. Discussion
4.1. Validity, Reliability, and Acceptance
4.2. Usability, Practicability, and Economy
5. Perspectives
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mughal, A.M.; Hassan, N.; Ahmed, A. Bone Age Assessment Methods: A Critical Review. Pak. J. Med. Sci. 2014, 30, 211. [Google Scholar] [CrossRef] [PubMed]
- Satoh, M. Bone Age: Assessment Methods and Clinical Applications. Clin. Pediatr. Endocrinol. 2015, 24, 143–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engebretsen, L.; Steffen, K.; Bahr, R.; Broderick, C.; Dvorak, J.; Janarv, P.-M.; Johnson, A.; Leglise, M.; Mamisch, T.C.; McKay, D.; et al. The International Olympic Committee Consensus Statement on Age Determination in High-Level Young Athletes. Br. J. Sport. Med. 2010, 44, 476–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanner, J.M. Issues and Advances in Adolescent Growth and Development. J. Adolesc. Health Care Off. Publ. Soc. Adolesc. Med. 1987, 8, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, S.; Viswanathan, V.K. Bone Age. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Smith, K.L.; Weir, P.L.; Till, K.; Romann, M.; Cobley, S. Correction to: Relative Age Effects Across and Within Female Sport Contexts: A Systematic Review and Meta-Analysis. Sport. Med. 2018, 48, 1989–1990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaeyens, R.; Lenoir, M.; Williams, A.M.; Philippaerts, R.M. Talent Identification and Development Programmes in Sport: Current Models and Future Directions. Sport. Med. 2008, 38, 703–714. [Google Scholar] [CrossRef] [PubMed]
- Fransen, J.; Skorski, S.; Baxter-Jones, A.D.G. Estimating Is Not Measuring: The Use of Non-Invasive Estimations of Somatic Maturity in Youth Football. Sci. Med. Footb. 2021, 5, 261–262. [Google Scholar] [CrossRef] [PubMed]
- Malina, R.M.; Rogol, A.D.; Cumming, S.P.; Coelho e Silva, M.J.; Figueiredo, A.J. Biological Maturation of Youth Athletes: Assessment and Implications. Br. J. Sport. Med. 2015, 49, 852–859. [Google Scholar] [CrossRef] [Green Version]
- Paśko, W.; Śliż, M.; Paszkowski, M.; Zieliński, J.; Polak, K.; Huzarski, M.; Przednowek, K. Characteristics of Cognitive Abilities among Youths Practicing Football. Int. J. Environ. Res. Public Health 2021, 18, 1371. [Google Scholar] [CrossRef]
- Dvorak, J.; George, J.; Junge, A.; Hodler, J. Age Determination by Magnetic Resonance Imaging of the Wrist in Adolescent Male Football Players. Br. J. Sport. Med. 2006, 41, 45–52. [Google Scholar] [CrossRef]
- Malina, R.M. Skeletal Age and Age Verification in Youth Sport. Sports Med. 2011, 41, 925–947. [Google Scholar] [CrossRef] [PubMed]
- Fransen, J.; Bush, S.; Woodcock, S.; Novak, A.; Deprez, D.; Baxter-Jones, A.D.G.; Vaeyens, R.; Lenoir, M. Improving the Prediction of Maturity From Anthropometric Variables Using a Maturity Ratio. Pediatr. Exerc. Sci. 2018, 30, 296–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khamis, H.J.; Roche, A.F. Predicting Adult Stature without Using Skeletal Age: The Khamis-Roche Method. Pediatrics 1994, 94 (4 Pt 1), 504–507. [Google Scholar] [PubMed]
- Mirwald, R.L.; Baxter-Jones, A.D.G.; Bailey, D.A.; Beunen, G.P. An Assessment of Maturity from Anthropometric Measurements. Med. Sci. Sport. Exerc. 2002, 34, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.A.; Mckay, H.A.; Macdonald, H.; Nettlefold, L.; Baxter-Jones, A.D.G.; Cameron, N.; Brasher, P.M.A. Enhancing a Somatic Maturity Prediction Model. Med. Sci. Sport. Exerc. 2015, 47, 1755–1764. [Google Scholar] [CrossRef]
- Malina, R.M.; Cumming, S.P.; Rogol, A.D.; Coelho-e-Silva, M.J.; Figueiredo, A.J.; Konarski, J.M.; Kozieł, S.M. Bio-Banding in Youth Sports: Background, Concept, and Application. Sport. Med. 2019, 49, 1671–1685. [Google Scholar] [CrossRef]
- Doyle, E.; Márquez-Grant, N.; Field, L.; Holmes, T.; Arthurs, O.J.; van Rijn, R.R.; Hackman, L.; Kasper, K.; Lewis, J.; Loomis, P.; et al. Guidelines for Best Practice: Imaging for Age Estimation in the Living. J. Forensic Radiol. Imaging 2019, 16, 38–49. [Google Scholar] [CrossRef] [Green Version]
- Mettler, F.A.; Huda, W.; Yoshizumi, T.T.; Mahesh, M. Effective Doses in Radiology and Diagnostic Nuclear Medicine: A Catalog. Radiology 2008, 248, 254–263. [Google Scholar] [CrossRef]
- Prokop-Piotrkowska, M.; Marszałek-Dziuba, K.; Moszczyńska, E.; Szalecki, M.; Jurkiewicz, E. Traditional and New Methods of Bone Age Assessment-An Overview. J. Clin. Res. Pediatr. Endocrinol. 2021, 13, 251–262. [Google Scholar] [CrossRef]
- Spârchez, M.; Fodor, D. What’s New in Musculoskeletal Ultrasound in Pediatric Rheumatology? Med. Ultrason. 2018, 20, 371. [Google Scholar] [CrossRef]
- Wan, J.; Zhao, Y.; Feng, Q.; Sun, Z.; Zhang, C. Potential Value of Conventional Ultrasound in Estimation of Bone Age in Patients from Birth to Near Adulthood. Ultrasound Med. Biol. 2019, 45, 2878–2886. [Google Scholar] [CrossRef] [PubMed]
- Rachmiel, M.; Naugolni, L.; Mazor-Aronovitch, K.; Koren-Morag, N.; Bistritzer, T. Bone Age Assessments by Quantitative Ultrasound (SonicBone) and Hand X-Ray Based Methods Are Comparable. Isr. Med. Assoc. J. 2017, 19, 5. [Google Scholar] [PubMed]
- Shimura, N.; Koyama, S.; Arisaka, O.; Imataka, M.; Sato, K.; Matsuura, M. Assessment of Measurement of Children’s Bone Age Ultrasonically with Sunlight BonAge. Clin. Pediatr. Endocrinol. 2005, 14 (Suppl. S24), S24_17–S24_20. [Google Scholar] [CrossRef] [Green Version]
- Herrmann, J.; Säring, D.; Auf der Mauer, M.; Groth, M.; Jopp-van Well, E. Forensic Age Assessment of the Knee: Proposal of a New Classification System Using Two-Dimensional Ultrasound Volumes and Comparison to MRI. Eur. Radiol. 2021, 31, 3237–3247. [Google Scholar] [CrossRef]
- Wan, J.; Zhao, Y.; Feng, Q.; Lv, P.; Hong, K.; Zhang, C. Statistical Confirmation of a Method of US Determination of Bone Age. Radiology 2021, 300, 176–183. [Google Scholar] [CrossRef]
- Castriota-Scanderbeg, A.; De Micheli, V. Ultrasound of Femoral Head Cartilage: A New Method of Assessing Bone Age. Skelet. Radiol. 1995, 24, 197–200. [Google Scholar] [CrossRef]
- Spannow, A.; Stenboeg, E.; Pfeiffer-Jensen, M.; Fiirgaard, B.; Haislund, M.; Ostergaard, M.; Andersen, N.; Herlin, T. Ultrasound and MRI Measurements of Joint Cartilage in Healthy Children: A Validation Study. Ultraschall Med. Eur. J. Ultrasound 2010, 32 (Suppl. S1), 110–116. [Google Scholar] [CrossRef]
- Trauzeddel, R.; Windschall, D.; Trauzeddel, R.; Nirschl, C.; Ganser, G.; Palm-Beden, K.; Berendes, R.; Haller, M.; Krumrey-Langkammerer, M.; Nimtz-Talaska, A.; et al. Arthrosonographic Reference Values of the Shoulder Joint in Healthy Children and Adolescents: A Cross-Sectional Multicentre Ultrasound Study. Klin. Pädiatr. 2017, 229, 293–301. [Google Scholar] [CrossRef]
- Trauzeddel, R.; Lehman, H.; Trauzeddel, R.F.; Haller, M.; Palm-Beden, K.; Ganser, G.; Berendes, R.; Nirschl, C.; Nimtz-Talaska, A.; Krumrey-Langkammerer, M.; et al. Age Dependent Ultrasound B-Mode Findings of the Elbow Joint in Healthy Children and Adolescents. Rheumatol. Int. 2019, 39, 1007–1018. [Google Scholar] [CrossRef]
- Windschall, D.; Trauzeddel, R.; Haller, M.; Krumrey-Langkammerer, M.; Nimtz-Talaska, A.; Berendes, R.; Ganser, G.; Nirschl, C.; Schoof, P.; Trauzeddel, R.F.; et al. Pediatric Musculoskeletal Ultrasound: Age- and Sex-Related Normal B-Mode Findings of the Knee. Rheumatol. Int. 2016, 36, 1569–1577. [Google Scholar] [CrossRef]
- Żuber, Z.; Owczarek, A.; Sobczyk, M.; Migas-Majoch, A.; Turowska-Heydel, D.; Sternal, A.; Michalczak, J.; Chudek, J. Establishing Percentile Charts for Hip Joint Capsule and Synovial Cavity Thickness in Apparently Healthy Children. Pediatr. Rheumatol. 2017, 15, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Muir, A. Precocious Puberty. Pediatr. Rev. 2006, 27, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Benito, M.; Muñoz, A.; Beltrán, I.; Labajo, E.; Perea, B.; Sánchez, J.A. Assessment of Adulthood in the Living Spanish Population Based on Ossification of the Medial Clavicle Epiphysis Using Ultrasound Methods. Forensic Sci. Int. 2018, 284, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Ağırman, K.T.; Bilge, O.M.; Miloğlu, O. Ultrasonography in Determining Pubertal Growth and Bone Age. Dentomaxillofacial Radiol. 2018, 47, 20170398. [Google Scholar] [CrossRef]
- Meena, G. The Importance of Conventional Radiography and Ultrasound in Determining Bone Age. Orthop. Res. Online J. 2018, 4, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Wagner, U.A.; Diedrich, V.; Schmitt, O. Determination of Skeletal Maturity by Ultrasound: A Preliminary Report. Skelet. Radiol. 1995, 24, 417–420. [Google Scholar] [CrossRef]
- Thaler, M.; Kaufmann, G.; Steingruber, I.; Mayr, E.; Liebensteiner, M.; Bach, C. Radiographic versus Ultrasound Evaluation of the Risser Grade in Adolescent Idiopathic Scoliosis: A Prospective Study of 46 Patients. Eur. Spine J. 2008, 17, 1251–1255. [Google Scholar] [CrossRef] [Green Version]
- Torlak, G.; Kiter, E.; Oto, M.; Akman, A. Ultrasonographic Evaluation of the Risser Sign. Spine 2012, 37, 316–320. [Google Scholar] [CrossRef]
- Chauhan, M.; Agrawal, A.; Dikshit, P.C.; Pradhan, G.S. Sonography Touchstone Testing Gold Standard Radiography for Medico-Legal Age Estimation in Living: A Prospective Triple Blind Study. J. Forensic Med. Toxicol. 2019, 36, 64. [Google Scholar] [CrossRef]
- Castriota-Scanderbeg, A.; Sacco, M.C.; Emberti-Gialloreti, L.; Fraracci, L. Skeletal Age Assessment in Children and Young Adults: Comparison between a Newly Developed Sonographic Method and Conventional Methods. Skelet. Radiol. 1998, 27, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Wan, J.; Zhao, Y.; Feng, Q.; Zhang, C. Summation of Ossification Ratios of Radius, Ulna and Femur: A New Parameter to Evaluate Bone Age by Ultrasound. Ultrasound Med. Biol. 2020, 46, 1761–1768. [Google Scholar] [CrossRef] [PubMed]
- Nessi, R.; Garattini, G.; Bazzini, E.; Zaffaroni, R.; Lazzerini, F. Ultrasonography assessment of ossification foci of the wrist and pubertal growth spurt. Radiol. Med. 1997, 94, 43–46. [Google Scholar]
- Giuca, M.R.; Mazza, P.; Marrapese, E.; Cesaretti, G.; Calderazzi, A.; Carafoli, D.; Saggese, G. A Comparison between Radiographic and Sonographic Assessment of Hand and Wrist Bones for the Estimation of Skeletal Age in the Child Patient. Eur. J. Paediatr. Dent. 2002, 3, 6. [Google Scholar]
- Gonsior, M.; Ramsthaler, F.; Gehl, A.; Verhoff, M.A. Morphology as a Cause for Different Classification of the Ossification Stage of the Medial Clavicular Epiphysis by Ultrasound, Computed Tomography, and Macroscopy. Int. J. Leg. Med. 2013, 127, 1013–1021. [Google Scholar] [CrossRef]
- Quirmbach, F.; Ramsthaler, F.; Verhoff, M.A. Evaluation of the Ossification of the Medial Clavicular Epiphysis with a Digital Ultrasonic System to Determine the Age Threshold of 21 Years. Int. J. Leg. Med. 2009, 123, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; Zwiesigk, P.; Schiborr, M.; Schmidt, S.; Schmeling, A. Ultrasound Studies on the Time Course of Clavicular Ossification. Int. J. Leg. Med. 2008, 122, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; Schiborr, M.; Pfeiffer, H.; Schmidt, S.; Schmeling, A. Sonographic Assessment of the Ossification of the Medial Clavicular Epiphysis in 616 Individuals. Forensic Sci. Med. Pathol. 2013, 9, 351–357. [Google Scholar] [CrossRef]
- Sánchez, M.B.; Codinha, S.; García, A.M.; Sánchez, J.A.S. Estimating Legal Age Based on Fusion of The Proximal Humeral Epiphysis. Int. J. Leg. Med. 2017, 131, 1133–1140. [Google Scholar] [CrossRef]
- Schulz, R.; Schiborr, M.; Pfeiffer, H.; Schmidt, S.; Schmeling, A. Forensic Age Estimation in Living Subjects Based on Ultrasound Examination of the Ossification of the Olecranon. J. Forensic Leg. Med. 2014, 22, 68–72. [Google Scholar] [CrossRef]
- Ekizoglu, O.; Er, A.; Buyuktoka, A.D.; Bozdag, M.; Karaman, G.; Moghaddam, N.; Grabherr, S. Ultrasonographic Assessment of Ossification of the Distal Radial Epiphysis for Estimating Forensic Age. Int. J. Leg. Med. 2021, 135, 1573–1580. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.; Schiborr, M.; Pfeiffer, H.; Schmeling, A.; Schulz, R. Sonographic Examination of the Apophysis of the Iliac Crest for Forensic Age Estimation in Living Persons. Sci. Justice 2013, 53, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Karami, M.; Moshirfatemi, A.; Daneshvar, P. Age Determination Using Ultrasonography in Young Football Players. Adv. Biomed. Res. 2014, 3, 174. [Google Scholar] [CrossRef] [PubMed]
- Karami, M.; Moradi, M.; Khazaei, M.; Modaresi, M.-R.; Asadi, K.; Soleimani, M. Detection of Secondary Ossification Centers by Sonography. Adv. Biomed. Res. 2016, 5, 12. [Google Scholar] [PubMed]
- Pitlovi, V. A Correlation of Peak Height Velocity and Olecranon Apophysis Ossification Assessed by Ultrasound. Coll. Antropol. 2013, 37, 1285–1289. [Google Scholar]
- Schmidt, S.; Schmeling, A.; Zwiesigk, P.; Pfeiffer, H.; Schulz, R. Sonographic Evaluation of Apophyseal Ossification of the Iliac Crest in Forensic Age Diagnostics in Living Individuals. Int. J. Leg. Med. 2011, 125, 271–276. [Google Scholar] [CrossRef]
- Shedge, R.; Kanchan, T.; Kushwaha, K.P.S.; Krishan, K. Ultrasonographic Evaluation of the Wrist and Elbow Joints: A Pilot Study to Explore a Non-Invasive Technique for Age Estimation. Med. Sci. Law 2021, 61, 14–22. [Google Scholar] [CrossRef]
- Windschall, D.; Collado, P.; Vojinovic, J.; Magni-Manzoni, S.; Balint, P.; Bruyn, G.A.W.; Hernandez-Diaz, C.; Nieto, J.C.; Ravagnani, V.; Tzaribachev, N.; et al. Age-Related Vascularization and Ossification of Joints in Children: An International Pilot Study to Test Multiobserver Ultrasound Reliability. Arthritis Care Res. 2020, 72, 498–506. [Google Scholar] [CrossRef] [Green Version]
- Martin, D.D.; Calder, A.D.; Ranke, M.B.; Binder, G.; Thodberg, H.H. Accuracy and Self-Validation of Automated Bone Age Determination. Sci. Rep. 2022, 12, 6388. [Google Scholar] [CrossRef]
- Pyle, S.I.; Waterhouse, A.M.; Greulich, W.W. Attributes of the Radiographic Standard of Reference for the National Health Examination Survey. Am. J. Phys. Anthropol. 1971, 35, 331–337. [Google Scholar] [CrossRef]
- Gonsior, M.; Ramsthaler, F.; Birngruber, C.; Obert, M.; Verhoff, M.A. The Completely Fused Medial Clavicular Epiphysis in High-Frequency Ultrasound Scans as a Diagnostic Criterion for Forensic Age Estimations in the Living. Int. J. Leg. Med. 2016, 130, 1603–1613. [Google Scholar] [CrossRef] [PubMed]
- European Asylum Support Office. EASO Practical Guide on Age Assessment, 2nd ed.; European Asylum Support Office: Valletta, Malta, 2018; p. 116. [Google Scholar]
- The Federal Assembly of the Swiss Confederation. Federal Act on Research Involving Human Beings (Human Research Act, HRA) 810.30; The Federal Assembly of the Swiss Confederation: Bern, Switzerland, 2011. [Google Scholar]
- Shahbazi-Gahrouei, D.; Setayandeh, S.; Gholami, M. A Review on Natural Background Radiation. Adv. Biomed. Res. 2013, 2, 65. [Google Scholar] [CrossRef] [PubMed]
- Hojreh, A.; Gamper, J.; Schmook, M.T.; Weber, M.; Prayer, D.; Herold, C.J.; Noebauer-Huhmann, I.-M. Hand MRI and the Greulich-Pyle Atlas in Skeletal Age Estimation in Adolescents. Skelet. Radiol. 2018, 47, 963–971. [Google Scholar] [CrossRef] [PubMed]
- Leyhr, D.; Murr, D.; Basten, L.; Eichler, K.; Hauser, T.; Lüdin, D.; Romann, M.; Sardo, G.; Höner, O. Biological Maturity Status in Elite Youth Soccer Players: A Comparison of Pragmatic Diagnostics With Magnetic Resonance Imaging. Front. Sport. Act. Living 2020, 2, 587861. [Google Scholar] [CrossRef]
- Baxter-Jones, A.D.G.; Barbour-Tuck, E.N.; Dale, D.; Sherar, L.B.; Knight, C.J.; Cumming, S.P.; Ferguson, L.J.; Kowalski, K.C.; Humbert, M.L. The Role of Growth and Maturation during Adolescence on Team-Selection and Short-Term Sports Participation. Ann. Hum. Biol. 2020, 47, 316–323. [Google Scholar] [CrossRef]
- Cobley, S.; Baker, J.; Wattie, N.; McKenna, J. Annual Age-Grouping and Athlete Development: A Meta-Analytical Review of Relative Age Effects in Sport. Sport. Med. 2009, 39, 235–256. [Google Scholar] [CrossRef]
- Dimundo, F.; Cole, M.; Blagrove, R.C.; McAuley, A.B.T.; Till, K.; Kelly, A.L. Talent Identification in an English Premiership Rugby Union Academy: Multidisciplinary Characteristics of Selected and Non-Selected Male Under-15 Players. Front. Sport. Act. Living 2021, 3, 688143. [Google Scholar] [CrossRef]
- Lüdin, D.; Donath, L.; Cobley, S.; Romann, M. Effect of Bio-Banding on Physiological and Technical-Tactical Key Performance Indicators in Youth Elite Soccer. Eur. J. Sport Sci. 2021, 22, 1–9. [Google Scholar] [CrossRef]
- Cumming, S.P.; Searle, C.; Hemsley, J.K.; Haswell, F.; Edwards, H.; Scott, S.; Gross, A.; Ryan, D.; Lewis, J.; White, P.; et al. Biological Maturation, Relative Age and Self-Regulation in Male Professional Academy Soccer Players: A Test of the Underdog Hypothesis. Psychol. Sport Exerc. 2018, 39, 147–153. [Google Scholar] [CrossRef]
- Greydanus, D.E.; Omar, H.; Pratt, H.D. The Adolescent Female Athlete: Current Concepts and Conundrums. Pediatr. Clin. North Am. 2010, 57, 697–718. [Google Scholar] [CrossRef]
- Monasterio, X.; Bidaurrazaga-Letona, I.; Larruskain, J.; Lekue, J.A.; Diaz-Beitia, G.; Santisteban, J.M.; Martin-Garetxana, I.; Gil, S.M. Relative Skeletal Maturity Status Affects Injury Burden in U14 Elite Academy Football Players. Scand. J. Med. Sci. Sport. 2022, 32, 1400–1409. [Google Scholar] [CrossRef] [PubMed]
- Malina, R.M. Secular Trends in Growth, Maturation and Physical Performance: A Review. Anthropol. Rev. 2004, 67, 29. [Google Scholar]
- Toselli, S.; Mauro, M.; Grigoletto, A.; Cataldi, S.; Benedetti, L.; Nanni, G.; Di Miceli, R.; Aiello, P.; Gallamini, D.; Fischetti, F.; et al. Maturation Selection Biases and Relative Age Effect in Italian Soccer Players of Different Levels. Biology 2022, 11, 1559. [Google Scholar] [CrossRef] [PubMed]
- Grgic, O.; Shevroja, E.; Dhamo, B.; Uitterlinden, A.G.; Wolvius, E.B.; Rivadeneira, F.; Medina-Gomez, C. Skeletal Maturation in Relation to Ethnic Background in Children of School Age: The Generation R Study. Bone 2020, 132, 115180. [Google Scholar] [CrossRef] [PubMed]
- Ontell, F.K.; Ivanovic, M.; Ablin, D.S.; Barlow, T.W. Bone Age in Children of Diverse Ethnicity. Am. J. Roentgenol. 1996, 167, 1395–1398. [Google Scholar] [CrossRef]
- Tricco, A. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]

| Technique | US | RX | MRI | CT | Autopsy | N Assessments/ Body Regions | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Method | Stages | Bone Age (Atlas) | Maturity Score | Distance and Ossification Ratio | Stages | Bone Age | Stages | Stages | Stage | ||
| Body Region | |||||||||||
| Ankle | 1 | 1 | 2 | ||||||||
| Clavicula | 6 | 1 | 1 | 8 | |||||||
| Elbow | 3 | 3 | |||||||||
| Femoral head | 1 | 1 | |||||||||
| Hand | 5 | 2 | 1 | 4 | 8 | 20 | |||||
| Iliac bone | 7 | 4 | 11 | ||||||||
| Knee | 2 | 2 | 1 | 5 | |||||||
| Shoulder | 1 | 1 | |||||||||
| Wrist | 9 | 2 | 2 | 5 | 4 | 8 | 30 | ||||
| N assessments | 34 | 4 | 3 | 9 | 12 | 16 | 1 | 1 | 1 | 81 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rüeger, E.; Hutmacher, N.; Eichelberger, P.; Löcherbach, C.; Albrecht, S.; Romann, M. Ultrasound Imaging-Based Methods for Assessing Biological Maturity during Adolescence and Possible Application in Youth Sport: A Scoping Review. Children 2022, 9, 1985. https://doi.org/10.3390/children9121985
Rüeger E, Hutmacher N, Eichelberger P, Löcherbach C, Albrecht S, Romann M. Ultrasound Imaging-Based Methods for Assessing Biological Maturity during Adolescence and Possible Application in Youth Sport: A Scoping Review. Children. 2022; 9(12):1985. https://doi.org/10.3390/children9121985
Chicago/Turabian StyleRüeger, Eva, Nicole Hutmacher, Patric Eichelberger, Claus Löcherbach, Silvia Albrecht, and Michael Romann. 2022. "Ultrasound Imaging-Based Methods for Assessing Biological Maturity during Adolescence and Possible Application in Youth Sport: A Scoping Review" Children 9, no. 12: 1985. https://doi.org/10.3390/children9121985