
Congenital Pseudarthrosis of the Clavicle in Children: A Systematic Review

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Search Strategy
2.2. Eligibility Criteria
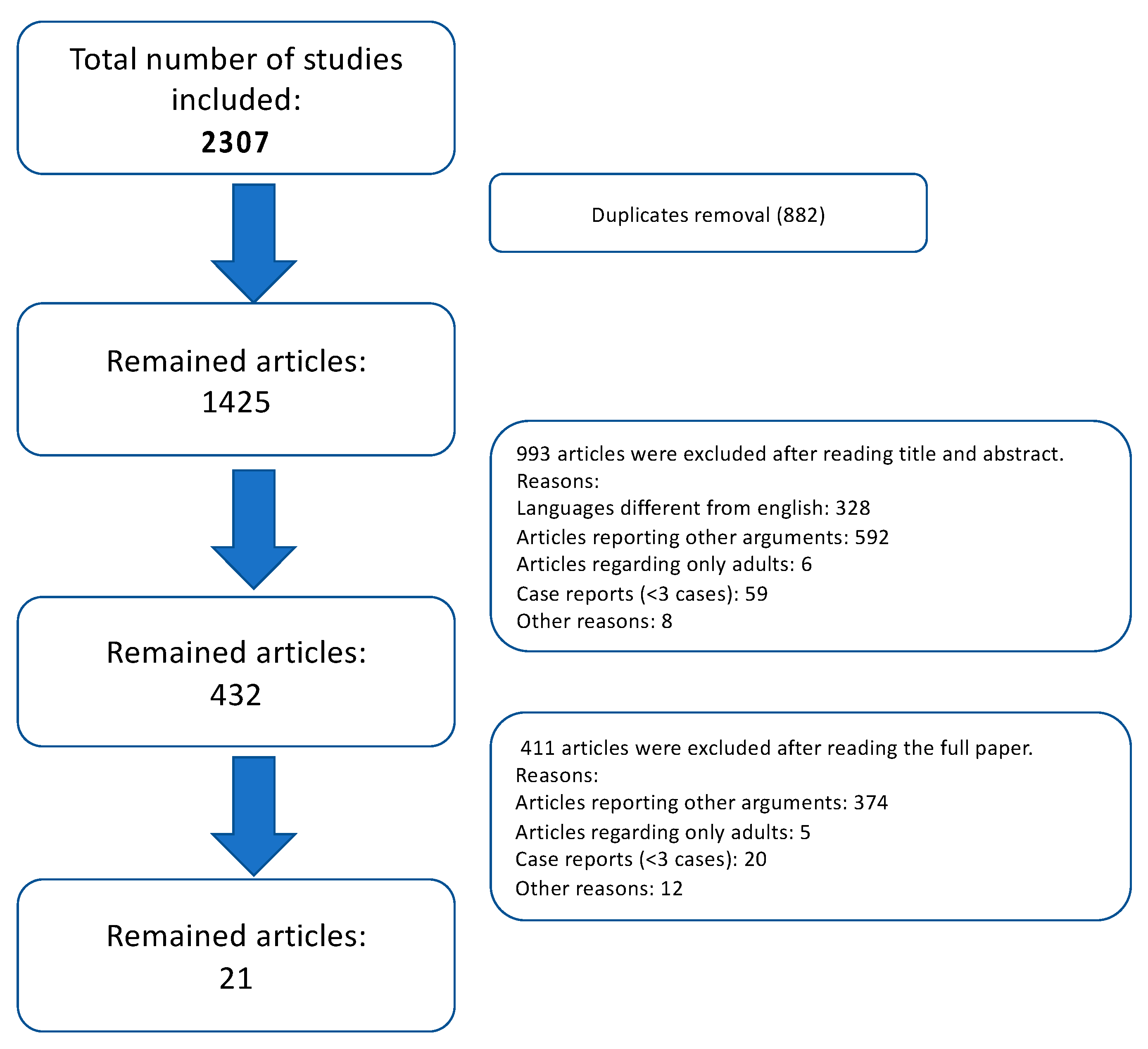
2.3. Article Selection
2.4. Data Extraction and Analysis
2.5. Quality Assessment and Statistical Analysis
3. Results
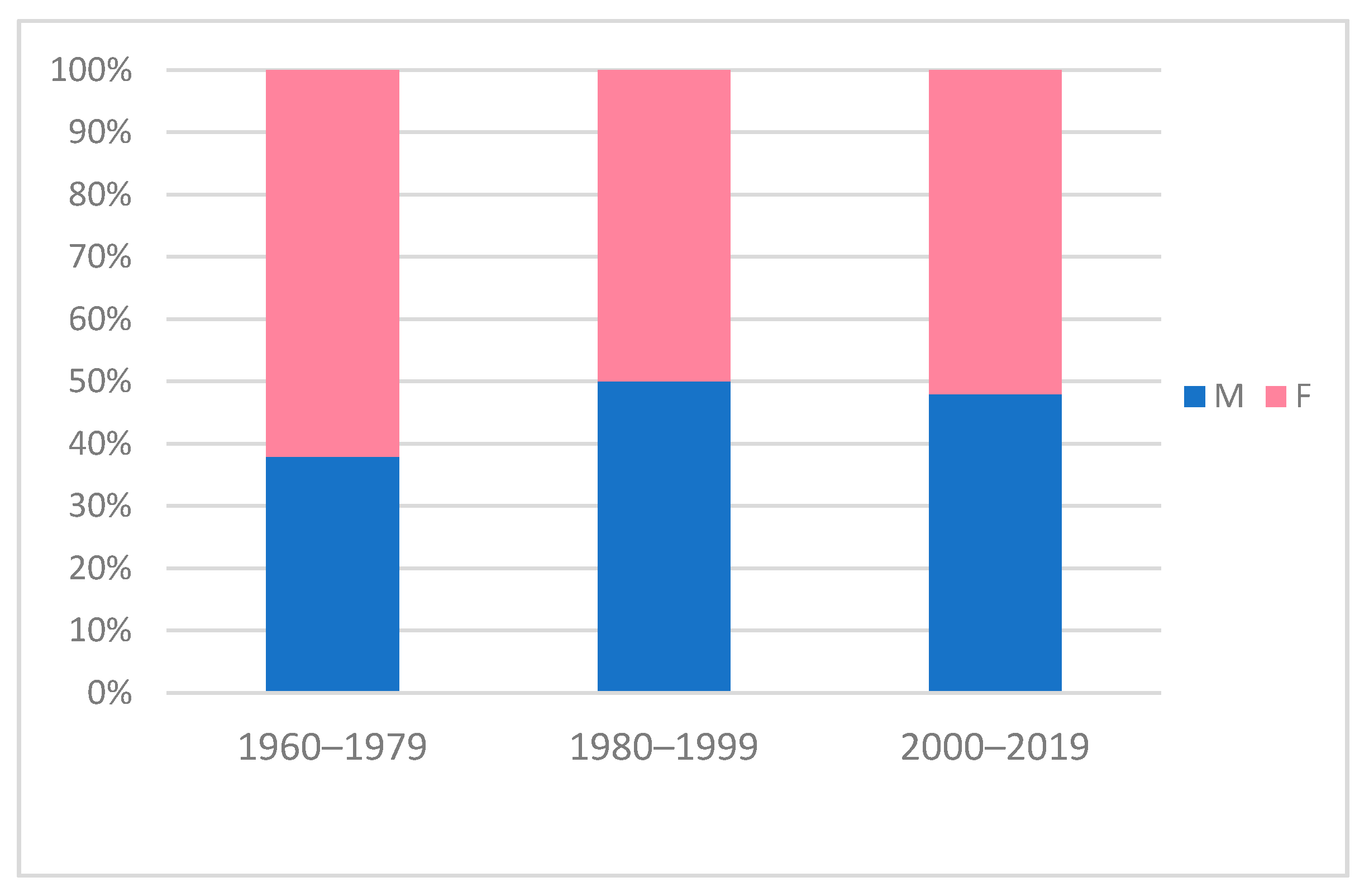
3.1. Demographics and Clinical Characteristics
3.2. Treatment
3.3. Surgical Outcomes
4. Discussion
4.1. Epidemiology, Etiology, Clinical Presentation
4.2. Surgical Treatment
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gibson, D.A.; Carroll, N. Congenital pseudarthrosis of the clavicle. J. Bone Jt. Surg. Br. 1970, 52-B, 629–643. [Google Scholar] [CrossRef] [Green Version]
- Lloyd-Roberts, G.C.; Apley, A.G.; Owen, R. Reflections upon the aetiology of congenital pseudarthrosis of the clavicle. With a note on cranio cleido dysostosis. J. Bone Jt. Surgery. Br. 1975, 57-B, 24–29. [Google Scholar] [CrossRef]
- Fitzwilliams, D. Hereditary cranio-cleido-dysostosis. Lancet 1910, 176, 1466–1475. [Google Scholar] [CrossRef]
- Kite, J.H. Congenital Pseudarthrosis of the Clavicle. South. Med J. 1968, 61, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, D.; Scott, B. The enigmatic role and development of the clavicle. Orthop. Trauma 2016, 30, 273–276. [Google Scholar] [CrossRef]
- Beslikas, T.A.; Dadoukis, D.J.; Gigis, I.P.; Nenopoulos, S.P.; Christoforides, J.E. Congenital Pseudarthrosis of the Clavicle: A Case Report. J. Orthop. Surg. 2007, 15, 87–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Persiani, P.; Molayem, I.; Villani, C.; Cadilhac, C.; Glorion, C. Surgical treatment of congenital pseudarthrosis of the clavicle: A report on 17 cases. Acta Orthop. Belg. 2008, 74, 161. [Google Scholar] [PubMed]
- Wall, J.J. Congenital Pseudarthrosis of the Clavicle. J. Bone Jt. Surg. American 1970, 52, 1003–1009. [Google Scholar] [CrossRef]
- Valcarce, M.F.-C.; Pérez, J.P.; Gabriel, M.L.; López, C.D.H. Seudoartrosis congénital de clavícula en dos gemelos. Anales de Pediatría 2003, 58, 78–79. [Google Scholar] [CrossRef]
- Price, B.D.; Price, C.T. Familial congenital pseudoarthrosis of the clavicle: Case report and literature review. Iowa Orthop. J. 1996, 16, 153–156. [Google Scholar] [PubMed]
- Jinkins, W.J. 24 Congenital Pseudarthrosis of the Clavicle. Clin. Orthop. Relat. Res. 1969, 62, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Behringer, B.R. Congenital Pseudarthrosis of the Clavicle. Arch. Pediatr. Adolesc. Med. 1972, 123, 511–517. [Google Scholar] [CrossRef]
- Kim, A.E.; Vuillermin, C.B.; Bae, D.S.; Samora, J.B.; Waters, P.M.; Bauer, A.S. Congenital pseudarthrosis of the clavicle: Surgical decision making and outcomes. J. Shoulder Elb. Surg. 2020, 29, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Alldred, A.J. Congenital pseudarthrosis of the clavicle. J. Bone Jt. Surgery. Br. 1963, 45-B, 312–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owen, R. Congenital pseudarthrosis of the clavicle. J. Bone Jt. Surgery. Br. 1970, 52-B, 644–652. [Google Scholar] [CrossRef]
- Ahmadi, B.; Steel, H.H. Congenital Pseudarthrosis of the Clavicle. Clin. Orthop. Relat. Res. 1977, 126, 129–134. [Google Scholar] [CrossRef]
- Manashil, G.; Laufer, S. Congenital pseudarthrosis of the clavicle: Report of three cases. Am. J. Roentgenol. 1979, 132, 678–679. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Dodwell, E.R.; Pathy, R.; Widmann, R.F.; Green, D.W.; Scher, D.M.; Blanco, J.S.; Doyle, S.M.; Daluiski, A.; Sink, E.L. Reliability of the Modified Clavien-Dindo-Sink Complication Classification System in Pediatric Orthopaedic Surgery. JBJS Open Access 2018, 3, e0020. [Google Scholar] [CrossRef]
- Gummesson, C.; Atroshi, I.; Ekdahl, C. The disabilities of the arm, shoulder and hand (DASH) outcome questionnaire: Longitudinal construct validity and measuring self-rated health change after surgery. BMC Musculoskelet. Disord. 2003, 4, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cella, D.; Riley, W.; Stone, A.; Rothrock, N.; Reeve, B.; Yount, S.; Amtmann, D.; Bode, R.; Buysse, D.; Choi, S.; et al. The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008. J. Clin. Epidemiology 2010, 63, 1179–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocourt, M.H.; Radlinger, L.; Kalberer, F.; Sanavi, S.; Schmid, N.S.; Leunig, M.; Hertel, R. Evaluation of intratester and intertester reliability of the Constant-Murley shoulder assessment. J. Shoulder Elb. Surg. 2008, 17, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Roy, J.-S.; MacDermid, J.C.; Woodhouse, L.J. A systematic review of the psychometric properties of the Constant-Murley score. J. Shoulder Elb. Surg. 2010, 19, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Katolik, L.I.; Romeo, A.; Cole, B.J.; Verma, N.N.; Hayden, J.K.; Bach, B.R. Normalization of the Constant score. J. Shoulder Elb. Surg. 2005, 14, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Naunheim, M.R.; Bs, J.B.D.; Rubinstein, B.J.; Goldberg, L.; Weinberg, A.; Courey, M.S. A visual analog scale for patient-reported voice outcomes: The VAS voice. Laryngoscope 2020, 5, 90–95. [Google Scholar] [CrossRef] [Green Version]
- Barbier, O.; Hoogmartens, M. Evidence-based medicine in orthopaedics. Acta Orthop. Belg. 2004, 70, 91–97. [Google Scholar]
- Coleman, B.D.; Khan, K.M.; Maffulli, N.; Cook, J.L.; Wark, J.D. Studies of surgical outcome after patellar tendinopathy: Clinical significance of methodological deficiencies and guidelines for future studies. Scand. J. Med. Sci. Sports 2000, 10, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Chandran, P.; George, H.; James, L.A. Congenital clavicular pseudarthrosis: Comparison of two treatment methods. J. Child. Orthop. 2011, 5, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Toledo, L.C.; MacEwen, G.D. Severe Complication of Surgical Treatment of Congenital Pseudarthrosis of the Clavicle. Clin. Orthop. Relat. Res. 1979, 139, 64–67. [Google Scholar] [CrossRef]
- Quinlan, W.R.; Brady, P.G.; Regan, B.F. Congenital Pseudarthrosis of the Clavicle. Acta Orthop. Scand. 1980, 51, 489–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnall, S.B.; King, J.D.; Marrero, G. Congenital Pseudarthrosis of the Clavicle. J. Pediatr. Orthop. 1988, 8, 316–321. [Google Scholar] [CrossRef]
- Grogan, D.P.; Love, S.M.; Guidera, K.J.; Ogden, J.A. Operative Treatment of Congenital Pseudarthrosis of the Clavicle. J. Pediatr. Orthop. 1991, 11, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Molto, F.J.L.; Lluch, D.J.B.; Garrido, I.M. Congenital Pseudarthrosis of the Clavicle: A Proposal for Early Surgical Treatment. J. Pediatr. Orthop. 2001, 21, 689–693. [Google Scholar] [CrossRef]
- Gomez-Brouchet, A.; De Gauzy, J.S.; Accadbled, F.; Abid, A.; Delisle, M.B.; Cahuzac, J.-P. Congenital pseudarthrosis of the clavicle: A histopathological study in five patients. J. Pediatr. Orthop. B 2004, 13, 399–401. [Google Scholar] [CrossRef]
- Ettl, V.; Wild, A.; Krauspe, R.; Raab, P. Surgical Treatment of Congenital Pseudarthrosis of the Clavicle: A Report of Three Cases and Review of the Literature. Eur. J. Pediatr. Surg. 2005, 15, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Currarino, G.; Herring, J.A. Congenital pseudarthrosis of the clavicle. Pediatr. Radiol. 2009, 39, 1343–1349. [Google Scholar] [CrossRef] [PubMed]
- Di Gennaro, G.L.; Cravino, M.; Martinelli, A.; Berardi, E.; Rao, A.; Stilli, S.; Trisolino, G. Congenital pseudarthrosis of the clavicle: A report on 27 cases. J. Shoulder Elb. Surg. 2017, 26, e65–e70. [Google Scholar] [CrossRef] [PubMed]
- Studer, K.; Baker, M.P.; Krieg, A.H. Operative treatment of congenital pseudarthrosis of the clavicle: A single-centre experience. J. Pediatr. Orthop. B 2017, 26, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Giwnewer, U.; Rubin, G.; Dohovni, E.; Rozen, N.; Bor, N. Congenital pseudoarthrosis of the clavicle: Should we reconsider timing and fixation method? J. Orthop. Surg. 2018, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddad, B.; Zribi, S.; Haraux, E.; Deroussen, F.; Gouron, R.; Klein, C. Induced membrane technique for clavicle reconstruction in paediatric patients: Report of four cases. Orthop. Traumatol. Surg. Res. 2019, 105, 733–737. [Google Scholar] [CrossRef] [PubMed]
- De Gauzy, J.S.; Baunin, C.; Puget, C.; Fajadet, P.; Cahuzac, J.P. Congenital Pseudarthrosis of the Clavicle and Thoracic Outlet Syndrome in Adolescence. J. Pediatr. Orthop. B 1999, 8, 299–301. [Google Scholar] [CrossRef]
- Glotzbecker, M.P.; Shin, E.K.; Chen, N.C.; Labow, B.I.; Waters, P.M. Salvage Reconstruction of Congenital Pseudarthrosis of the Clavicle With Vascularized Fibular Graft After Failed Operative Treatment. J. Pediatr. Orthop. 2009, 29, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Murai, A.; Tada, K.; Nakada, M.; Matsuta, M.; Hayashi, K.; Tsuchiya, H. Use of a Free Vascularized Medial Femoral Condyle Flap for Revision Surgery in a Pediatric Patient with Congenital Pseudarthrosis of the Clavicle. Case Rep. Orthop. 2020, 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Elliot, R.R.; Richards, R.H. Failed operative treatment in two cases of pseudarthrosis of the clavicle using internal fixation and bovine cancellous xenograft (Tutobone). J. Pediatr. Orthop. B 2011, 20, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Dzupa, V.; Bartonicek, J.; Zídka, M. Fracture of the clavicle after surgical treatment for congenital pseudarthrosis. Med. Sci. Monit. 2004, 10, 1–4. [Google Scholar]
- Spadliński, Ł.; Cecot, T.; Majos, A.; Stefańczyk, L.; Pietruszewska, W.; Wysiadecki, G.; Topol, M.; Polguj, M. The Epidemiological, Morphological, and Clinical Aspects of the Cervical Ribs in Humans. BioMed Res. Int. 2016, 2016, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khu, K.J.; Midha, R. Clavicle Pseudarthrosis: A Rare Cause of Thoracic Outlet Syndrome. Can. J. Neurol. Sci. J. Can. des Sci. Neurol. 2010, 37, 863–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lozano-Vilardell, P.; Díaz, M.; Riera, R.; Gomez, F. Venous thoracic outlet syndrome secondary to congenital pseudoarthrosis of the clavicle. Presentation in the fourth decade of life. Eur. J. Vasc. Endovasc. Surg. 2003, 25, 592–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, M.C.; Richards, R.R.; Hudson, A.R. Thoracic outlet syndrome with congenital pseudarthrosis of the clavicle: Treatment by brachial plexus decompression, plate fixation and bone grafting. Can. J. Surg. 1988, 31, 131–133. [Google Scholar] [PubMed]
- Hahn, K.; Shah, R.; Shalev, Y.; Schmidt, D.H.; Bajwa, T. Congenital clavicular pseudoarthrosis associated with vascular thoracic outlet syndrome: Case presentation and review of the literature. Catheter. Cardiovasc. Diagn. 1995, 35, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Huntley, J.S. Evidence-Based Treatment of Congenital Clavicular Pseudarthrosis. In Paediatric Orthopaedics; Springer: Singapore, 2017; pp. 279–285. [Google Scholar]

{kind=link}
{kind=link}
| Author and Year | Study Design | Patients * | Details | CEBM | mCMS |
|---|---|---|---|---|---|
| Alldred [14] 1963 | Case series | 9/9 | 4 conservative 1 excision 1 local autograft 3 autograft from donor site + pin | 4 | 16 |
| Gibson and Carroll [1] 1970 | Case series | 15/27 4 bilateral | 6 conservative (1 bilateral) 2 graft (2 bilateral) 6 graft + pin (1 bilateral) 1 graft + plate | 4 | 7 |
| Owen [15] 1970 | Case series | 33/33 | 13 conservative 4 excision 7 autograft from donor site 8 autograft from donor site + pin 1 graft with beef bone peg | 4 | 16 |
| Wall [8] 1970 | Case series | 5/5 | 5 conservative | 4 | 4 |
| Ahmadi and Steel [16] 1977 | Case series | 5/5 | 3 conservative 1 cancellous autograft + pin 1 graft + pin | 4 | 12 |
| Manashil and Laufer [17] 1979 | Case series | 3/3 | 3 conservative | 4 | 0 |
| Toledo and MacEwen [30] 1979 | Case series | 10/10 | 6 conservative 4 autograft from donor site + pin | 4 | 25 |
| Quinlan et al. [31] 1980 | Case series | 4/4 | 1 conservative 2 autograft from donor site 1 autograft from donor site + wire | 4 | 17 |
| Schnall et al. [32] 1988 | Case series | 6/6 | 1 autograft from donor site + pin 5 autograft from donor site + plate | 4 | 24 |
| Grogan et al. [33] 1991 | Case series | 8/8 | 8 local autograft + bone suture | 4 | 40 |
| Lorente Molto et al. [34] 2001 | Case series | 6/6 1 bilateral | 1 conservative 5 autograft from donor site + pin (1 bilateral) | 4 | 22 |
| Gomez-Brouchet et al. [35] 2004 | Case series | 5/5 | 5 autograft from donor site + pin | 4 | 20 |
| Ettl et al. [36] 2005 | Case series | 3/3 | 3 autograft from donor site + pin | 4 | 32 |
| Persiani et al. [7] 2008 | Retrospective comparative study | 17/17 | 1 pin 4 plate 7 autograft from donor site + pin 5 autograft from donor site + plate | 3b | 26 |
| Currarino et al. [37] 2009 | Case series | 4/4 | 1 conservative (indicated surgery, lost at F.U.) 1 plate 2 local autograft + plate | 4 | 21 |
| Chandran et al. [29] 2011 | Retrospective comparative study | 12/12 1 bilateral | 2 conservative 5 autograft from donor site + pin 5 autograft from donor site + plate (1 bilateral) | 3b | 17 |
| Di Gennaro et al. [38] 2016 | Case series | 26/27 | 7 conservative 15 autograft from donor site + pin 3 allograft + pin 1 allograft + plate | 4 | 26 |
| Studer et al. [39] 2017 | Case series | 7/7 1 bilateral | 7 autograft from donor site + plate (1 bilateral) | 4 | 50 |
| Giwnewer et al. [40] 2018 | Case series | 3/3 | 3 autograft from donor site + plate | 4 | 37 |
| Haddad et al. [41] 2019 | Case series | 3/4 | 3 Masquelet technique | 4 | 34 |
| Kim et al. [13] 2020 | Retrospective comparative study | 47/47 2 bilateral | 23 conservative 3 bone suture 5 local autograft + bone suture 1 allograft + bone suture 7 autograft from donor site + plate 4 local autograft + plate 3 allograft and local autograft + plate 1 N/S graft + plate | 3b | 41 |
| Patients (n.) | Procedures (n.) | Mean Age at Treatment (Years, Range) | Mean Weeks of Immobilization (Range) | Mean Weeks of Consolidation (Range) | Mean Months of Follow-up (Range) | Nonunions (by Procedures %) | Complications (Minor + Major, by Procedures %) | Post-Op Symptoms (by Procedures %) | |
|---|---|---|---|---|---|---|---|---|---|
| Excision | 5 | 5 | 16.0 (1 patient) | N/S | N/S | 36.0 (36–36) | 5 (100.0%) | 0 (0 + 0) * 0.0% * | 5/5 (100.0%) |
| Fixation | 9 | 9 | 6.0 (4.5–8.0) | 6.5 (6.5–6.5) | 8.0 (8–8) | 58.0 (24–120) | 2 (22.2%) | 2 (0 + 2) 22.2% | 0/6 (0.0%) |
| Graft alone | 13 | 15 | 5.6 (2.0–6.5) | N/S | N/S | 48.0 (12–84) | 1 (6.7%) | 2 (1 + 1) 13.3% | 1/16 (6.3%) |
| Graft + BS | 14 | 14 | 2.6 (0.8–6.0) | 6.0 (6.0–6.0) | N/S | 94.5 (24–168) | 3 (21.4%) | 4 (1 + 3) 28.6% | 0/8 (0.0%) |
| Graft + pin | 65 | 67 | 6.3 (1.5–16.6) | 10.1 (6.0–18.6) | 10.2 (4–24) | 34.9 (2–214) | 9 (13.4%) | 20 (9 + 11) 29.9% | 1/60 (1.7%) |
| Graft + plate | 46 | 49 | 7.0 (1.5–16.0) | 4.3 (2.0–11.4) | 23.7 (8–100) | 50.2 (3–120) | 5 (10.2%) | 8 (2 + 6) 16.3% | 3/28 (10.7%) |
| Masquelet | 3 | 3 | 8.8 (7.4–9.5) | 6.0 (6.0–6.0) | 42.0 (42–42) | 42.4 (24–120) | 0 (0.0%) | 2 (0 + 2) 66.7% | 0/3 (0.0%) |
| N/S | 1 | 2 | N/S | N/S | N/S | N/S | N/S | N/S | N/S |
| Total | 156 | 164 | 5.9 (0.5–16.6) | 7.1 (2.0–18.6) | 21.2 (4–100) | 46.1 (0–214) | 25 (15.4%) | 38 (13 + 25) 23.9% ** (8.2% + 15.7% **) | 10/126 (7.9%) |
| Procedures (n.) | Nonunions (by Procedures %) | Complications (Minor + Major) | |
|---|---|---|---|
| Local autograft | 20 | 3 (15.0%) | 4 (1 + 3) |
| Autograft from donor site | 102 | 11 (10.8%) | 24 (10 + 14) |
| Allograft | 9 | 4 (44.4%) | 5 (1 + 4) |
| Others | 14 | 0 (0.0%) | 1 (1 + 0) |
| Total | 145 | 18 (12.4%) | 34 (13 + 21) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Depaoli, A.; Zarantonello, P.; Gallone, G.; Di Gennaro, G.L.; Ferrari, D.; Marchesini Reggiani, L.; Manca, A.; Trisolino, G. Congenital Pseudarthrosis of the Clavicle in Children: A Systematic Review. Children 2022, 9, 147. https://doi.org/10.3390/children9020147
Depaoli A, Zarantonello P, Gallone G, Di Gennaro GL, Ferrari D, Marchesini Reggiani L, Manca A, Trisolino G. Congenital Pseudarthrosis of the Clavicle in Children: A Systematic Review. Children. 2022; 9(2):147. https://doi.org/10.3390/children9020147
Chicago/Turabian StyleDepaoli, Alessandro, Paola Zarantonello, Giovanni Gallone, Giovanni Luigi Di Gennaro, Daniele Ferrari, Leonardo Marchesini Reggiani, Aniello Manca, and Giovanni Trisolino. 2022. "Congenital Pseudarthrosis of the Clavicle in Children: A Systematic Review" Children 9, no. 2: 147. https://doi.org/10.3390/children9020147
APA StyleDepaoli, A., Zarantonello, P., Gallone, G., Di Gennaro, G. L., Ferrari, D., Marchesini Reggiani, L., Manca, A., & Trisolino, G. (2022). Congenital Pseudarthrosis of the Clavicle in Children: A Systematic Review. Children, 9(2), 147. https://doi.org/10.3390/children9020147