
Psychosocial Characteristics and Experiences in Patients with Multiple Endocrine Neoplasia Type 2 (MEN2) and Medullary Thyroid Carcinoma (MTC)


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Total Sample
3.1.1. Demographic Characteristics
3.1.2. Clinical and Mental Health Characteristics
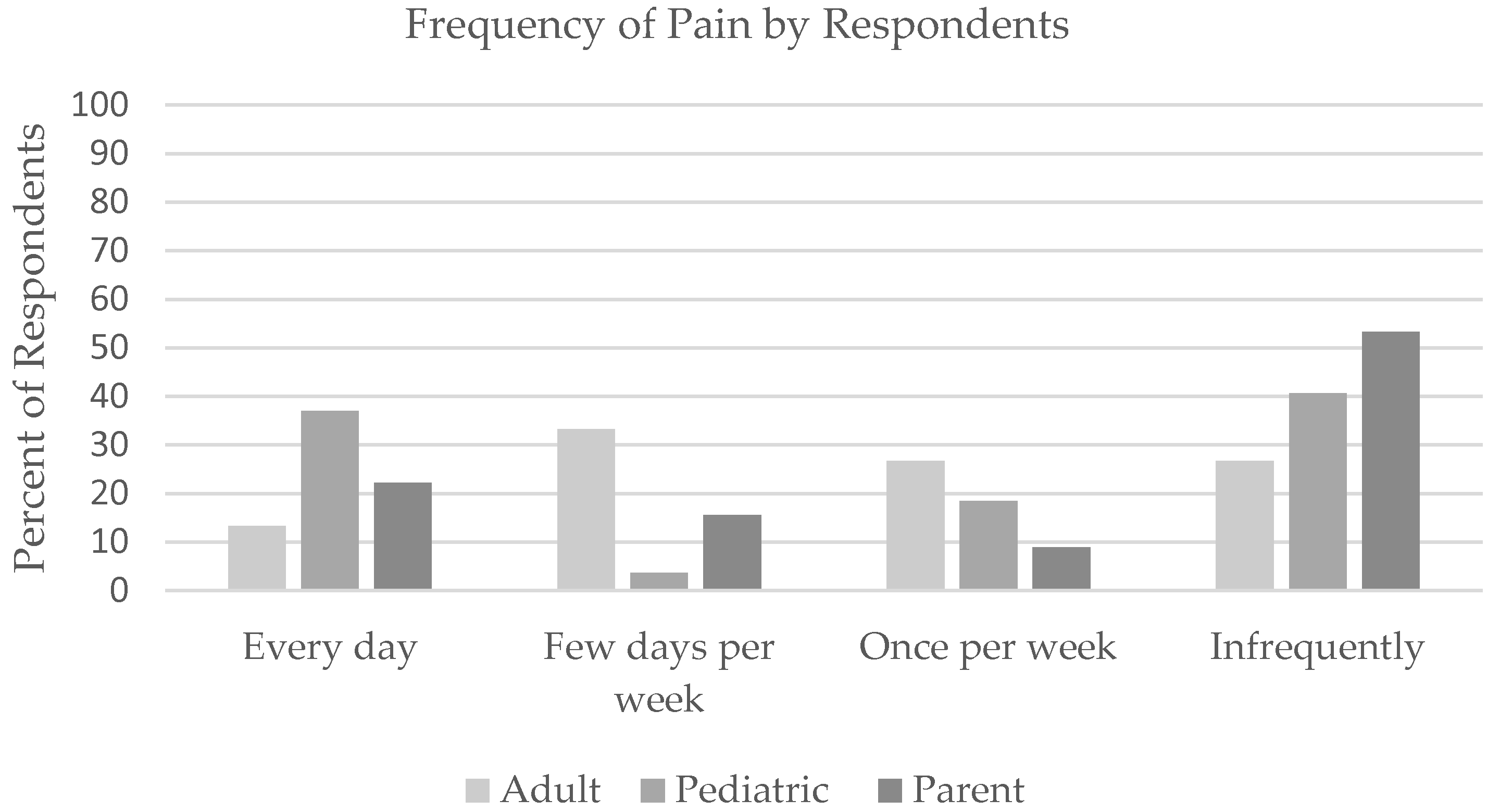
3.2. Perceptions of Physical Health and Pain
3.3. Qualitative Data and Interest in Supportive Resources
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Larouche, V.; Akirov, A.; Thomas, C.M.; Krzyzanowska, M.K.; Ezzat, S. A Primer on the Genetics of Medullary Thyroid Cancer. Curr. Oncol. 2019, 26, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Kebebew, E.; Ituarte, P.H.; Siperstein, A.E.; Duh, Q.Y.; Clark, O.H. Medullary thyroid carcinoma: Clinical characteris-tics, treatment, prognostic factors, and a comparison of staging systems. Cancer 2000, 88, 1139–1148. [Google Scholar] [CrossRef]
- Graves, C.; Gosnell, J.E. Medullary Thyroid Carcinoma in Children. Semin. Pediatr. Surg. 2020, 29, 150921. [Google Scholar] [CrossRef] [PubMed]
- Eng, C.C.D.; Schuffenecker, I.; Schuffenecker, I.; Lenoir, G.; Cote, G.; Gagel, R.F.; van Amstel, H.K.P.; Lips, C.J.M.; Nishisho, I.; Takai, S.; et al. The relationship between specific RET proto-oncogene mutations and disease phenotype in multiple endocrine neoplasia type 2. International RET mutation consortium analysis. JAMA 1996, 276, 1575–1579. [Google Scholar] [CrossRef] [PubMed]
- Kouvaraki, M.A.; Shapiro, S.E.; Perrier, N.D.; Cote, G.J.; Gagel, R.F.; Hoff, A.O.; Sherman, S.I.; Lee, J.E.; Evans, D.B. RETProto-Oncogene: A Review and Update of Genotype–Phenotype Correlations in Hereditary Medullary Thyroid Cancer and Associated Endocrine Tumors. Thyroid 2005, 15, 531–544. [Google Scholar] [CrossRef]
- Eng, C. Multiple Endocrine Neoplasia Type 2. In GeneReviews®; Adam, M.P., Ardinger, H.H., Pagon, R.A., Eds.; University of Washington: Seattle, WA, USA, 1999. [Google Scholar]
- Rajabi, S.; Hedayati, M. Medullary Thyroid Cancer: Clinical Characteristics and New Insights into Therapeutic Strategies Targeting Tyrosine Kinases. Mol. Diagn. Ther. 2017, 21, 607–620. [Google Scholar] [CrossRef]
- Wells, S.A.; Asa, S.; Dralle, H.; Elisei, R.; Evans, D.B.; Gagel, R.F.; Lee, N.Y.; Machens, A.; Moley, J.F.; Pacini, F.; et al. Revised American Thyroid Association Guidelines for the Management of Medullary Thyroid Carcinoma. Thyroid 2015, 25, 567–610. [Google Scholar] [CrossRef]
- Waguespack, S.G.; Rich, T.A.; Perrier, N.D.; Jimenez, C.; Cote, G.J. Management of medullary thyroid carcinoma and MEN2 syndromes in childhood. Nat. Rev. Endocrinol. 2011, 7, 596–607. [Google Scholar] [CrossRef]
- Carney, J.A.S.G.; Hayles, A.B. Multiple endocrine neoplasia, type 2b. Pathobiol. Annu. 1978, 8, 105–153. [Google Scholar]
- Mathiesen, J.S.; Effraimidis, G.; Rossing, M.; Rasmussen, K.; Hoejberg, L.; Bastholt, L.; Godballe, C.; Oturai, P.; Feldt-Rasmussen, U. Multiple endocrine neoplasia type 2: A review. Semin. Cancer Biol. 2022, 79, 163–179. [Google Scholar] [CrossRef]
- Castinetti, F.; Moley, J.; Mulligan, L.M.; Waguespack, S.G. A comprehensive review on MEN2B. Endocr.-Relat. Cancer 2018, 25, T29–T39. [Google Scholar] [CrossRef] [PubMed]
- Brandi, M.L.; Gagel, R.F.; Angeli, A. Guidelines for diagnosis and therapy of MEN type 1 and type 2. J. Clin. Endo-Crinol. Metab. 2001, 86, 5658–5671. [Google Scholar] [CrossRef] [PubMed]
- Di Bartolomeo, M.; Bajetta, E.; Bochicchio, A.M.; Carnaghi, C.; Somma, L.; Mazzaferro, V.; Visini, M.; Gebbia, V.; Tumolo, S.; Ballatore, P. A phase II trial of dacarbazine, fluorouracil and epirubicin in patients with neuroendocrine tumours. A study by the Italian Trials in Medical Oncology (I.T.M.O.) Group. Ann. Oncol. 1995, 6, 77–79. [Google Scholar] [CrossRef] [PubMed]
- Marsh, D.J.; Learoyd, D.L.; Robinson, B.G. Medullary thyroid carcinoma: Recent advances and management update. Thyroid 1995, 5, 407–424. [Google Scholar] [CrossRef] [PubMed]
- Modigliani, E.; Cohen, R.; Campos, J.M.; Conte-Devolx, B.; Maes, B.; Boneu, A.; Schlumberger, M.; Bigorgne, J.; Dumontier, P.; Leclerc, L.; et al. Prognostic factors for survival and for biochemical cure in medullary thyroid carcino-ma: Results in 899 patients. The GETC Study Group.Groupe d’etude des tumeurs a calcitonine. Clin. Endocrinol. 1998, 48, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Nocera, M.B.E.; Pellegriti, G.; Cailleux, A.F.; Mechelany-Corone, C.; Schlumberger, M. Treatment of advanced medullary thyroid cancer with an alternating combination of doxorubicin-streptozocin and 5 FU-dacarbazine. Groupe d’Etude des Tumeurs a Calcitonine (GETC). Br. J. Cancer 2000, 83, 715–718. [Google Scholar] [CrossRef][Green Version]
- Quayle, F.J.; Moley, J.F. Medullary thyroid carcinoma: Including MEN 2A and MEN 2B syndromes. J. Surg. Oncol. 2005, 89, 122–129. [Google Scholar] [CrossRef]
- Wu, L.-T.; Averbuch, S.D.; Ball, D.W.; De Bustros, A.; Baylin, S.B.; McGuire, W.P., 3rd. Treatment of advanced medullary thyroid carcinoma with a combination of cyclophosphamide, vincristine, and dacarbazine. Cancer 1994, 73, 432–436. [Google Scholar] [CrossRef]
- Kim, M.; Kim, B.H. Current Guidelines for Management of Medullary Thyroid Carcinoma. Endocrinol. Metab. 2021, 36, 514–524. [Google Scholar] [CrossRef]
- Wells, S.A. Advances in the management of MEN2: From improved surgical and medical treatment to novel kinase inhibitors. Endocr.-Relat. Cancer 2018, 25, T1–T13. [Google Scholar] [CrossRef]
- Puerto, M.; Borson-Chazot, F.; Tabarin, A. Updates on therapy for medullary thyroid cancer in 2021. Ann. D’endocrinologie 2022, 83, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Peczkowska, M.J.A. Multiple endocrine neoplasia type 2. Fam. Cancer 2005, 4, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Wells, S.A.J.; Skinner, M.A. Prophylactic thyroidectomy, based on direct genetic testing, in patients at risk for the multiple endocrine neoplasia type 2 syndromes. Exp. Clin. Endocrinol. Diabetes 1998, 106, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Al-Salameh, A.; Baudry, C.; Cohen, R. Update on multiple endocrine neoplasia Type 1 and 2. Presse Med. 2018, 47, 722–731. [Google Scholar] [CrossRef] [PubMed]
- Castinetti, F.; Waguespack, S.G.; Machens, A.; Uchino, S.; Hasse-Lazar, K.; Sanso, G.; Else, T.; Dvorakova, S.; Qi, X.P.; Elisei, R.; et al. Natural history, treatment, and long-term follow up of patients with multiple endocrine neoplasia type 2B: An international, multicentre, retrospective study. Lancet Diabetes Endocrinol. 2019, 7, 213–220. [Google Scholar] [CrossRef]
- Keatts, E.L.; Itano, J. Medullary Thyroid Cancer and the Impact of Genetic Testing. Clin. J. Oncol. Nurs. 2006, 10, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Goncharova, M.; Grey, J.; Druce, M. Impact of gastrointestinal symptoms on quality of life in MEN2. Clin. Endocrinol. 2021, 94, 606–615. [Google Scholar] [CrossRef]
- Freyer, G.; Schlumberger, M.; Conte-Devolx, B.; Ligneau, B.; Trillet-Lenoir, V.; Lenoir, G.M. Psychosocial impact of genetic testing in familial medullary-thyroid carcinoma: A multicentric pilot-evaluation. Ann. Oncol. 1999, 10, 87–95. [Google Scholar] [CrossRef]
- Freyer, G.; Schulumberger, M.; Blandy, C.; Contedevolx, B.; Trillet-Lenoir, V.; Lenoir, G.M.; Chau, N.; Dazord, A. Quality of life in patients at risk of medullary thyroid carcinoma and followed by a comprehensive medical network: Trends for future evalua-tions. Ann. Oncol. 2001, 12, 1461–1465. [Google Scholar] [CrossRef]
- Rodrigues, K.C.; Toledo, R.A.; Coutinho, F.L.; Nunes, A.B.; Maciel, R.M.; Hoff, A.O.; Tavares, M.C.; Toledo, S.P.A.; Lourenço, D.M. Assessment of Depression, Anxiety, Quality of Life, and Coping in Long-Standing Multiple Endocrine Neoplasia Type 2 Patients. Thyroid. Off. J. Am. Thyroid. Assoc. 2017, 27, 693–706. [Google Scholar] [CrossRef]
- Correa, F.A.; Farias, E.C.; Castroneves, L.A.; Lourenço, D.M., Jr.; Hoff, A.O. Quality of Life and Coping in Multiple Endocrine Neoplasia Type 2. J. Endocr. Soc. 2019, 3, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Grey, J.; Winter, K. Patient quality of life and prognosis in multiple endocrine neoplasia type 2. Endocr.-Relat. Cancer 2018, 25, T69–T77. [Google Scholar] [CrossRef] [PubMed]
- Wiener, L.B.H.; Zadeh, S.; Smith, C.J.; Helman, L.J.; Kim, S.Y. Gastrointestinal stromal tumor: Psychosocial characteristics and con-siderations. Support Care Cancer 2012, 20, 1343–1349. [Google Scholar] [CrossRef]
- Jacobsen, P.B.; Donovan, K.A.; Trask, P.C.; Fleishman, S.B.; Zabora, J.; Baker, F.; Holland, J.C. Screening for psychologic distress inambulatory cancer patients. Cancer 2005, 103, 1494–1502. [Google Scholar] [CrossRef] [PubMed]
- Zwahlen, D.; Hagenbuch, N.; Carley, M.I.; Recklitis, C.J.; Buchi, S. Screening cancer patients’ families with the distress thermometer (DT): A validation study. Psycho-Oncology 2008, 17, 959–966. [Google Scholar] [CrossRef]
- Ransom, S.; Jacobsen, P.B.; Booth-Jones, M. Validation of the Distress Thermometer with bone marrow transplant patients. Psycho-Oncology 2006, 15, 604–612. [Google Scholar] [CrossRef]
- Patel, S.K.; Mullins, W.; Turk, A.; Dekel, N.; Kinjo, C.; Sato, J.K. Distress screening, rater agreement, and services in pediatric oncology. Psycho-Oncology 2011, 20, 1324–1333. [Google Scholar] [CrossRef]
- National Center for Education Statistics. Available online: https://nces.ed.gov/programs/coe/pdf/2021/cgg_508c.pdf (accessed on 10 February 2022).
- Berglund, G.; Lidén, A.; Hansson, M.G.; Öberg, K.; Sjöden, P.O.; Nordin, K. Quality of life in patients with multiple endocrine neoplasia type 1 (MEN 1). Fam. Cancer 2003, 2, 27–33. [Google Scholar] [CrossRef]
- Mongelli, M.N.; Peipert, B.J.; Goswami, S.; Helenowski, I.; Yount, S.E.; Sturgeon, C. Quality of life in multiple endocrine neoplasia type 2A compared with normative and disease populations. Surgery 2018, 164, 546–552. [Google Scholar] [CrossRef]
- Hetherington, K.; Hunter, J.; Lockridge, R.; Warby, M.; Raygada, M.; Wakefield, C.; Wiener, L. The psychosocial impacts of FECS on the patient and caregiver. In Familial Endocrine Cancer Syndromes: Navigating the Transition of Care for Pediatric and Adolescent Patients. in press.


{kind=link}
| Total Sample | Pediatric (<12 Years) | Pediatric (12–17 Years) | Adult Sample (≥18 Years) | |||||
|---|---|---|---|---|---|---|---|---|
| Characteristic | n | % | n | % | n | % | n | % |
| Total N | 63 | 100 | 15 | 23.8 | 31 | 49.2 | 17 | 26.9 |
| Diagnosis MEN2B MEN2A | ||||||||
| 49 | 77.8 | 10 | 66.7 | 27 | 87.1 | 12 | 70.6 | |
| 14 | 22.2 | 5 | 33.3 | 4 | 12.9 | 5 | 29.4 | |
| MTC Diagnosis Yes No | ||||||||
| 52 | 82.5 | 10 | 66.7 | 28 | 90.3 | 14 | 82.4 | |
| 11 | 17.5 | 5 | 33.3 | 3 | 9.7 | 3 | 17.6 | |
| Age | ||||||||
| Mean (M) | 16.4 | 8.5 | 14.9 | 26.0 | ||||
| Standard Deviation (SD) | 8.2 | 2.4 | 1.4 | 9.5 | ||||
| Range | 2.7–49.1 | 2.7–11.9 | 12.1–17.9 | 18.2–49.1 | ||||
| Gender | ||||||||
| n | 63 | 15 | 31 | 17 | ||||
| % Male | 31 | 49.2 | 8 | 53.3 | 14 | 45.2 | 9 | 52.9 |
| % Female | 32 | 50.8 | 7 | 46.7 | 17 | 54.8 | 8 | 47.1 |
| Race | ||||||||
| n | 63 | 15 | 31 | 17 | ||||
| % White | 45 | 71.4 | 12 | 80.0 | 22 | 71.0 | 11 | 64.7 |
| % Black/African American | 5 | 7.9 | 0 | 0 | 3 | 9.7 | 2 | 11.8 |
| % Latino/a | 8 | 12.7 | 1 | 6.7 | 4 | 12.9 | 3 | 17.6 |
| % Asian/Pacific Islander | 3 | 4.8 | 2 | 13.3 | 0 | 0 | 1 | 5.9 |
| % Other | 2 | 3.2 | 0 | 0 | 2 | 6.5 | 0 | 0 |
| Received Special Education | ||||||||
| n | 59 | 14 | 30 | 15 | ||||
| % Yes | 15 | 25.4 | 4 | 28.6 | 7 | 23.3 | 4 | 26.7 |
| % No | 44 | 74.6 | 10 | 71.4 | 23 | 76.7 | 11 | 73.3 |
| Highest Education Completed * | ||||||||
| n | 14 | |||||||
| % Less than high school | 1 | 7.1 | ||||||
| % Graduated high school/GED ** | 4 | 28.6 | ||||||
| % Some college/vocational | 3 | 21.4 | ||||||
| % Graduated college/vocational | 4 | 28.6 | ||||||
| % Some professional/graduate | 0 | 0 | ||||||
| % Graduate/professional degree | 2 | 14.3 | ||||||
| Symptom | Adult Self Report 1 ≥18 Years (n = 15) | |
|---|---|---|
| n | % | |
| Mood shifts | 3 | 20.0 |
| Attention difficulties | 3 | 20.0 |
| Cries or upset easily | 6 | 40.0 |
| Difficulty concentrating | 5 | 33.3 |
| Anxiety or panic attacks | 4 | 26.7 |
| Sad/Depressed | 5 | 33.3 |
| Loss of interest or pleasure in activities | 2 | 13.3 |
| Feeling hopeless | 1 | 6.7 |
| Difficulty making friends | 1 | 6.7 |
| Difficulty keeping friends | 3 | 20.0 |
| Pediatric (n = 46) 1 | Adult (n = 17) | |||
|---|---|---|---|---|
| n | % 2 | n | % | |
| Receiving mental health treatment | 10 | 21.7 | 3 | 17.6 |
| Taking medication for anxiety | 5 | 10.9 | 2 | 11.8 |
| Taking medication for depression | 3 | 6.5 | 3 | 17.6 |
| Taking medication for attention difficulties | 2 | 4.3 | 2 | 11.8 |
| Symptom | Pediatric Self Report 1 12–17 Years (n = 26) | Parents of 1 Child 12–17 (n = 30) | Parents of Child <12 Years (n = 15) | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Mood shifts | 7 | 26.9 | 17 | 56.7 | 7 | 46.7 |
| Attention difficulties | 13 | 50.0 | 9 | 30.0 | 3 | 20.0 |
| Cries or upset easily | 10 | 38.5 | 12 | 40.0 | 6 | 40.0 |
| Difficulty concentrating | 17 | 65.4 | 10 | 33.3 | 3 | 20.0 |
| Anxiety or panic attacks | 8 | 30.8 | 8 | 26.7 | 3 | 20.0 |
| Sad/Depressed | 8 | 30.8 | 6 | 20.0 | 5 | 33.3 |
| Loss of interest or pleasure in activities | 7 | 26.9 | 4 | 13.3 | 0 | 0 |
| Feeling hopeless | 2 | 7.7 | 4 | 13.3 | 3 | 20.0 |
| Difficulty making friends | 3 | 11.5 | 8 | 26.7 | 5 | 33.3 |
| Difficulty keeping friends | 5 | 19.2 | 6 | 20.0 | 4 | 26.7 |
| Theme | Code | Sample |
|---|---|---|
| Disease related experiences and challenges | Diagnosis specific concerns | “general sense of illness” (parent) “he will never be cured” (parent) “stress of knowing I have a rare disease” (patient 12–17) |
| Treatment Impact | “needles, iv, doctors’ visits all the time” (parent) “keeping my medicine organized” (patient 18+) “all the tests, especially needles” (patient 12–17) | |
| Symptom Impact | “the constant pain” (parent) “physical issues of colon/urinary problems” (parent) “sleep (not sleeping well)” (patient 12–17) | |
| Physical Limitations | “unable to do things—physical weakness” (parent) “not able to follow the rhythm of peers of my age (physical activity)” (patient 18+) “Not as physically strong as I’d like to be” (patient 12–17) | |
| Internalized experiences of living with MTC (e.g., sadness, depression) | Mental Health Impact | “sadness” (parent) “social/emotional wellbeing” (parent) “overthinking, stress” (patient 18+) “constant worries” (patient 12–17) |
| Coping with Uncertainty | “wondering what’s going to happen” (parent) “not knowing what will happen from scan to scan” (parent) “doubt with testing and what comes next” (patient 18+) “don’t know what the future will bring” (patient 12–17) | |
| Being and feeling different | inside his mouth that its visible, teeth difference” (parent) “noticing that he is different (physically)” (parent) “people looking and staring” (patient 12–17) | |
| External experiences and challenges of living with MTC (e.g., relationships and school/work environment) | Social Impact | “he has to deal with bedwetting with his friends” (parent) “embarrassment of gas” (parent) “sacrificing a lot of time with friends and family” (patient 18+) “I hate people feeling sorry for me” (patient 12–17) |
| Family Impact | “worries about how it affects parents” (parent) “feel guilty for having more attention than my brothers- take up my parents time” (patient 18+) “stress on my family (siblings)” (patient 12–17) | |
| School/Work-Related Impact | “ struggling with ADHD * and school” (parent) “maintaining school alongside doctor visits” (patient 18+) “miss school- make up work, if I miss too many classes I have to repeat 9th grade” (patient 12–17) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lockridge, R.; Bedoya, S.; Allen, T.; Widemann, B.C.; Akshintala, S.; Glod, J.; Wiener, L. Psychosocial Characteristics and Experiences in Patients with Multiple Endocrine Neoplasia Type 2 (MEN2) and Medullary Thyroid Carcinoma (MTC). Children 2022, 9, 774. https://doi.org/10.3390/children9060774
Lockridge R, Bedoya S, Allen T, Widemann BC, Akshintala S, Glod J, Wiener L. Psychosocial Characteristics and Experiences in Patients with Multiple Endocrine Neoplasia Type 2 (MEN2) and Medullary Thyroid Carcinoma (MTC). Children. 2022; 9(6):774. https://doi.org/10.3390/children9060774
Chicago/Turabian StyleLockridge, Robin, Sima Bedoya, Taryn Allen, Brigitte C. Widemann, Srivandana Akshintala, John Glod, and Lori Wiener. 2022. "Psychosocial Characteristics and Experiences in Patients with Multiple Endocrine Neoplasia Type 2 (MEN2) and Medullary Thyroid Carcinoma (MTC)" Children 9, no. 6: 774. https://doi.org/10.3390/children9060774
APA StyleLockridge, R., Bedoya, S., Allen, T., Widemann, B. C., Akshintala, S., Glod, J., & Wiener, L. (2022). Psychosocial Characteristics and Experiences in Patients with Multiple Endocrine Neoplasia Type 2 (MEN2) and Medullary Thyroid Carcinoma (MTC). Children, 9(6), 774. https://doi.org/10.3390/children9060774