
Pediatric Primary Care Perspectives of Mental Health Services Delivery during the COVID-19 Pandemic

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Recruitment
2.2. Study Procedures
3. Data Analysis
4. Results
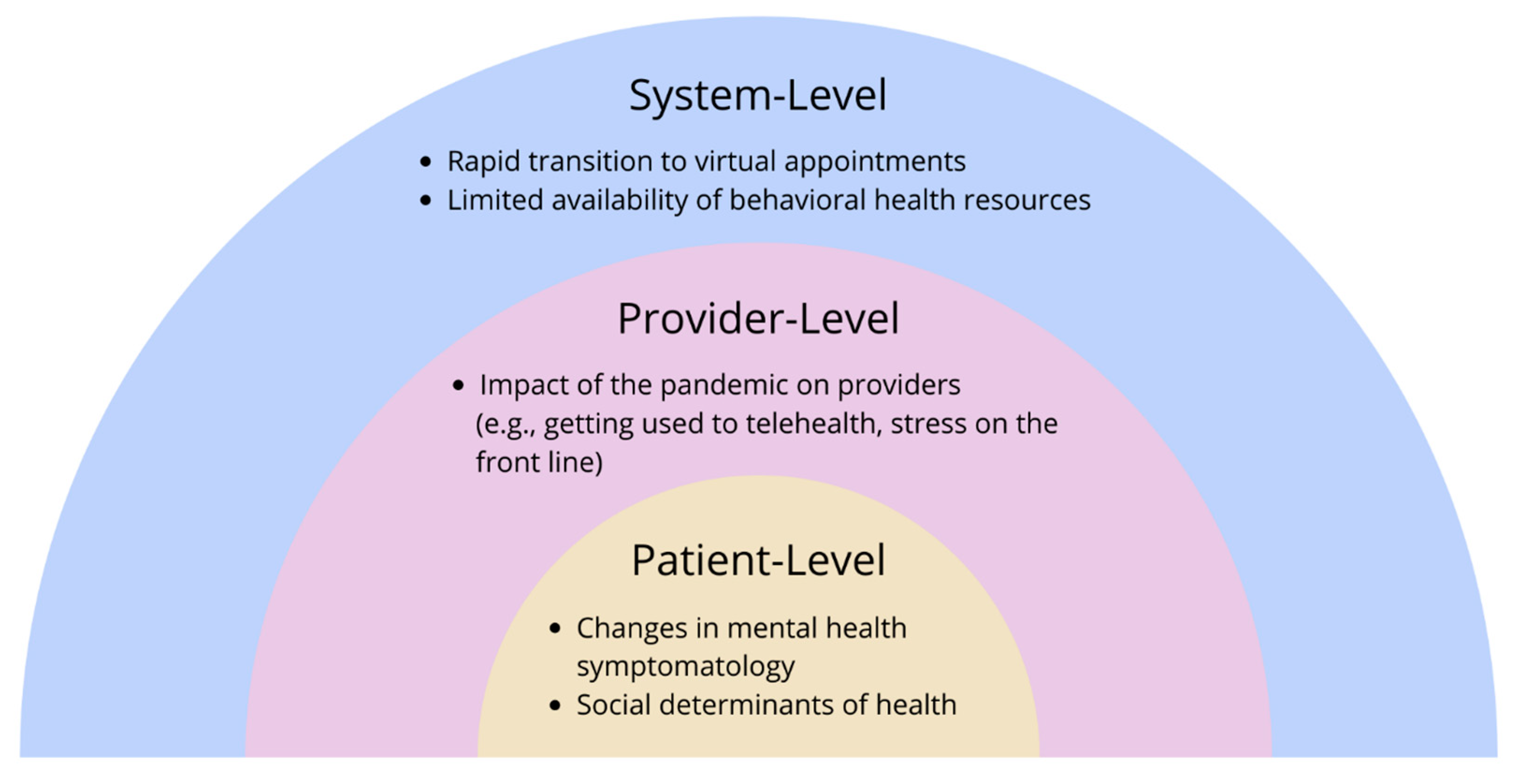
5. System-Level Domain
5.1. Rapid Transition to Virtual Appointments
5.2. Limited Availability of Behavioral Health Resources
6. Provider-Level Domain
Impact of the Pandemic on Providers
7. Patient-Level Domain
7.1. Changes in Mental Health Symptomatology
7.2. Social Determinants of Health
8. Discussion
9. Limitations
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Golberstein, E.; Wen, H.; Miller, B.F. Coronavirus Disease 2019 (COVID-19) and Mental Health for Children and Adolescents. JAMA Pediatr. 2020, 174, 819–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques de Miranda, D.; da Silva Athanasio, B.; Sena Oliveira, A.C.; Simoes, E.S.A.C. How is COVID-19 pandemic impacting mental health of children and adolescents? Int. J. Disaster Risk Reduct. 2020, 51, 101845. [Google Scholar] [CrossRef] [PubMed]
- Samji, H.; Wu, J.; Ladak, A.; Vossen, C.; Stewart, E.; Dove, N.; Long, D.; Snell, G. Review: Mental health impacts of the COVID-19 pandemic on children and youth—A systematic review. Child Adolesc. Ment. Health 2022, 27, 173–189. [Google Scholar] [CrossRef] [PubMed]
- AACAP Releases Workforce Maps Illustrating Severe Shortage of Child and Adolescent Psychiatrists. 2018. Available online: https://www.aacap.org/AACAP/Press/Press_Releases/2018/Severe_Shortage_of_Child_and_Adolescent_Psychiatrists_Illustrated_in_AAACP_Workforce_maps.aspx (accessed on 1 July 2020).
- U.S. Public Health Service. Report of the Surgeon General’s Conference on Children’s Mental Health: A National Action Agenda; Department of Health and Human Services: Washington, DC, USA, 2000.
- McBain, R.K.; Kofner, A.; Stein, B.D.; Cantor, J.H.; Vogt, W.B.; Yu, H. Growth and Distribution of Child Psychiatrists in the United States: 2007–2016. Pediatrics 2019, 144, e20191576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cummings, J.R.; Ji, X.; Druss, B.G. Mental Health Service Use by Medicaid-Enrolled Children and Adolescents in Primary Care Safety-Net Clinics. Psychiatr. Serv. 2020, 71, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Protecting Youth Mental Health: The U.S. Surgeon General’s Advisory; Office of the Surgeon General: Washington, DC, USA, 2021.
- Anderson, L.E.; Chen, M.L.; Perrin, J.M.; Van Cleave, J. Outpatient Visits and Medication Prescribing for US Children With Mental Health Conditions. Pediatrics 2015, 136, e1178–e1185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, R.; Storfer-Isser, A.; Kerker, B. Beyond ADHD: How Well Are We Doing? Acad. Pediatr. 2016, 16, 115–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horwitz, S.M.; Kelleher, K.J.; Stein, R.E.; Storfer-Isser, A.; Youngstrom, E.A.; Park, E.R.; Heneghan, A.M.; Jensen, P.S.; O’Connor, K.G.; Hoagwood, K.E. Barriers to the identification and management of psychosocial issues in children and maternal depression. Pediatrics 2007, 119, e208–e218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Straus, J.; Sarvet, B. Behavioral Health Care For Children: The Massachusetts Child Psychiatry Access Project. Health Aff. 2014, 33, 2153–2161. [Google Scholar] [CrossRef] [PubMed]
- Hilt, R.J.; Romaire, M.A.; McDonell, M.G.; Sears, J.M.; Krupski, A.; Thompson, J.N.; Myers, J.; Trupin, E.W. The Partnership Access Line: Evaluating a child psychiatry consult program in Washington State. JAMA Pediatr. 2013, 167, 162–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malas, N.; Klein, E.; Tengelitsch, E.; Kramer, A.; Marcus, S.; Quigley, J. Exploring the Telepsychiatry Experience: Primary Care Provider Perception of the Michigan Child Collaborative Care (MC3) Program. Psychosomatics 2019, 60, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merriam, S.B.; Grenier, R.S. Qualitative Research in Practice: Examples for Discussion and Analysis, 2nd ed.; Jossey-Bass: San Francisco, CA, USA, 2019. [Google Scholar]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1996. [Google Scholar]
- Aisbitt, G.M.; Nolte, T.; Fonagy, P. Editorial Perspective: The digital divide—Inequalities in remote therapy for children and adolescents. Child Adolesc. Ment. Health 2022. [Google Scholar] [CrossRef] [PubMed]
- AlRasheed, R.; Woodard, G.S.; Nguyen, J.; Daniels, A.; Park, N.; Berliner, L.; Dorsey, S. Transitioning to Telehealth for COVID-19 and Beyond: Perspectives of Community Mental Health Clinicians. J. Behav. Health Serv. Res. 2022, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hoffnung, G.; Feigenbaum, E.; Schechter, A.; Guttman, D.; Zemon, V.; Schechter, I. Children and Telehealth in Mental Healthcare: What We Have Learned From COVID-19 and 40,000+ Sessions. Psychiatr. Res. Clin. Pract. 2021, 3, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Yonek, J.; Lee, C.M.; Harrison, A.; Mangurian, C.; Tolou-Shams, M. Key Components of Effective Pediatric Integrated Mental Health Care Models: A Systematic Review. JAMA Pediatr. 2020, 174, 487–498. [Google Scholar] [CrossRef]
- Spencer, A.E.; Platt, R.E.; Bettencourt, A.F.; Serhal, E.; Burkey, M.D.; Sikov, J.; Vidal, C.; Stratton, J.; Polk, S.; Jain, S.; et al. Implementation of Off-Site Integrated Care for Children: A Scoping Review. Harv. Rev. Psychiatr. 2019, 27, 342–353. [Google Scholar] [CrossRef]
- Goldman, M.L.; Smali, E.; Richkin, T.; Pincus, H.A.; Chung, H. A novel continuum-based framework for translating behavioral health integration to primary care settings. Transl. Behav. Med. 2020, 10, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Samantaray, N.N.; Kar, N.; Mishra, S.R. A follow-up study on treatment effects of cognitive-behavioral therapy on social anxiety disorder: Impact of COVID-19 fear during post-lockdown period. Psychiatr. Res. 2022, 310, 114439. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Provider Demographics | (N = 50) 1 | |
|---|---|---|
| N | % | |
| Age | ||
| 18–29 | 2 | 4.0 |
| 30–39 | 19 | 38.0 |
| 40–49 | 15 | 30.0 |
| 50–59 | 10 | 20.0 |
| 60–69 | 4 | 8.0 |
| Race/ethnicity | ||
| Asian | 17 | 34.0 |
| Black or African American | 2 | 4.0 |
| Hispanic/Latinx | 4 | 8.0 |
| White | 21 | 42.0 |
| Mixed Race | 4 | 8.0 |
| Other | 1 | 2.0 |
| Decline to state | 1 | 2.0 |
| Gender | ||
| Female | 43 | 86.0 |
| Male | 7 | 14.0 |
| Provider type | ||
| Community Health Worker | 1 | 2.1 |
| MD (pediatrics) | 28 | 58.3 |
| MD (family) | 5 | 10.4 |
| Medical Resident | 1 | 2.1 |
| NP (general) | 3 | 6.3 |
| NP (pediatrics) | 3 | 6.3 |
| NP (psych) | 1 | 2.1 |
| PhD | 1 | 2.1 |
| PsyD | 1 | 2.1 |
| RN | 1 | 2.1 |
| Social Worker | 3 | 6.3 |
| Years of practice/work experience | ||
| 0–5 | 14 | 28.0 |
| 6–10 | 8 | 16.0 |
| 11–15 | 12 | 24.0 |
| 16–20 | 5 | 10.0 |
| 21+ | 11 | 22.0 |
| Patients’ predominant insurance type | ||
| Commercial insurance | 23 | 46.0 |
| Medi-Cal | 21 | 42.0 |
| Other | 4 | 8.0 |
| Unknown | 2 | 4.0 |
| Practice Type | ||
| FQHC | 26 | 54.2% |
| Community Practice | 22 | 45.8% |
| Provider language(s) spoken other than English | ||
| None | 19 | 38.0 |
| Spanish | 18 | 36.0 |
| Hindi | 5 | 10.0 |
| Japanese | 3 | 6.0 |
| Mandarin | 3 | 6.0 |
| French | 2 | 4.0 |
| German | 2 | 4.0 |
| Urdu | 2 | 4.0 |
| Arabic | 1 | 2.0 |
| Hebrew | 1 | 2.0 |
| Kannada | 1 | 2.0 |
| Punjabi | 1 | 2.0 |
| Telugu | 1 | 2.0 |
| Yoruba | 1 | 2.0 |
| System-Level Domain | |
|---|---|
| Theme: Rapid Transition to Virtual Appointments | |
| Subtheme: Increased Convenience | “Since almost everything is virtual, they don’t have to get themselves anywhere, they can just hop on a computer and Zoom with somebody.” (Clinic 1) “I have also seen some positives in the ability of people to access care through telemedicine, that a family doesn’t have to take time off work and get in the car and drive somewhere and find parking, and it actually reduces the stress of them getting the care that they need. And it makes the access to care somewhat easier in many ways. So lots of negatives, but also some positives…the ability of us to do telemedicine I hope stays.” (Clinic 7) “I think in terms of…benefits to be able to have…physical mobility, disabilities, or even related stigma…barriers to walking into a behavioral health building for services. There’s a level of anonymity…that technology affords…as well as thinking in terms of reducing cost and time for the patient, a disability maybe for some of that. So we’ve definitely seen a much lower no-show rate.” (Clinic 8) |
| Subtheme: Barriers to Patient-Provider Connection | “I think our model of care has really changed during COVID I think one of the very unique things of our clinic, it was very much based on an open-door sort of model. Especially for our patient population that people could really stop by. We would tend to see a lot of drop-ins everyday which I think really served our patients. Often it was not necessarily for mental health but it was for something else, but what came up was actually a moment of crisis and needing somebody to talk to, needing somebody to be connected to, and that is just not available anymore. We really have closed our doors. Not in the sense of keeping people out but trying to keep our staff and providers safe, our patients safe, and really only seeing people who need to come into clinic but that’s very hard to figure out. You can’t just walk into clinic anymore. I think that has really changed our ability to connect to patients and connect patients with additional resources.” (Clinic 6) “If you are seeing a patient for the first time, or a patient you’re not familiar with yourself as a primary care provider, which can happen quite a bit, especially in COVID. And so you don’t have a good grasp of the social family dynamics, and it seems like the patient has severe symptoms, and you’re wondering, ‘how do I approach this now, and handle this now, before I fall out with them.’” (Clinic 7) “Working with younger patients through virtual means has been a challenge for our providers who do work with pediatrics; it’s just harder to engage with a five-year-old through video for therapy services.” (Clinic 8) |
| Subtheme: Screening Challenges | “I find it uncomfortable to go down that ACEs [adverse childhood experiences] checklist by phone, so I don’t do it…for a family that’s new to our clinic…for brand new patients to go down a list of potentially traumatic questions, I find very difficult. I don’t know how they perceive it on their end” (Clinic 5) “I also think assessing risk is harder over the phone. Yeah, it’s been scarier for me to do that over the phone.” (Clinic 6) “I think the fact that we’re not doing routine visits on teens anymore, as well. Because they don’t need them for school. Right? And because that’s not an urgent service. It means we’re missing the things that came up on routine physicals in terms of mental health screening and sexual health screening stuff. We’re missing opportunities to get people connected to mental health care or get them birth control or get them other sensitive services that were coming up in the context of sort of general preventative care that we’re just not able to do.” (Clinic 6) |
| Subtheme: Confidentiality Concerns | “Especially for adolescents, the confidentiality piece is just so hard because we have a lot of our families live in shared homes and it’s two families living in a single bedroom home or the whole family is in a room. So at least when they come into the clinic, we have the opportunity to kick the parent out, ask really private questions.” (Clinic 5) ”…that confidentiality piece on the phone—that they might not be willing to be vulnerable when they can’t be or if they—there might be other people around them.” (Clinic 5) |
| Theme: Limited Availability of Behavioral Health Resources | |
| Subtheme: Warm Hand-off Model | “Warm hand off model has sort of disintegrated.” (Clinic 6) “Now with COVID that our behavioral health clinicians are working remotely, and our medical providers are onsite, and that we’ve been understaffed for behavioral health for quite a while, that system has broken down a little bit. So, it’s a little more challenging to do warm hand off and to really get that in the moment collaboration that we would like.” (Clinic 6) “Our warm hand off model—I think it feels very disconnected for patients that they don’t associate necessarily me with [name] because we’re calling at two different times. So, I think the connection between your routine health care and your mental health services is kind of getting broken apart.” (Clinic 6) |
| Subtheme: Referrals | “All of us don’t feel comfortable once the kid is complicated in family medicine, or suicidal. I don’t think that’s where pediatricians are supposed to be managing patients, and we’re always trying to refer them on. It’s been really really hard to get them [families] to use the system. And then when they do try to use the system, the system doesn’t always work.” (Clinic 1) “It does sort of feel like the therapists and the psychiatrists are becoming less available. I think there’s definitely a greater need.” (Clinic 1) “I haven’t noticed a difference because it is still—I haven’t noticed it worsen but I don’t think it was very likely that I could have a patient call [a behavioral health access line] and get an appointment any sooner than 3–6 months. I don’t think that’s changed. I don’t think we’ve been in COVID long enough for me to see a change because it was already taking so long.” (Clinic 5) “Sometimes somebody is out sick, and the referral doesn’t get processed or on the other side with people receiving the referrals, their front desk is out sick. Just with normal, maybe not with COVID illness, but taking care of their kids. We—a lot of people—now that school is going to start up, moms are calling out sick, taking FMLA. Staffing just in general in the medical system I think is lower. And so, while I haven’t seen it yet, I would predict that wait times do get longer just because of overwhelm from those things.” (Clinic 5) “…Seeing how other agencies are understandably impacted by COVID—either not being able to provide telehealth services, or clinicians and staff being out on EDD, things like that. That’s also just been a huge adjustment…” (Clinic 7) “Even though tele-medicine and tele-video visits are available by the psychiatrist, I think it took them a few months to initially set it up. Probably with the insurances, with the reimbursements and so on. We couldn’t get access for at least from March to June and then we were able to get some access. Even with that. Now, they are completely booked out until October or so.” (Clinic 9) |
| Subtheme: School-based Resources | “Parents are really stressed with the younger kids and having to work full-time, be a teacher, manage kids who are having ADHD [attention deficit hyperactivity disorder] or behavioral issues, and not getting as much support from the schools for kids that have learning disabilities.” (Clinic 1) “The school systems, particularly in the high schools, created a wellness center within our high school districts. And that was gaining acceptance among our students, and they were definitely using it, definitely I would encourage students who either they themselves, their parents were resistant, or they were worried about finances, that this was a great resource. Obviously, with COVID, that disappeared—or, it didn’t completely disappear, but the ease of getting to it just was convoluted.” (Clinic 1) |
| Provider-Level Domain | |
| Theme: Impact of the Pandemic on Providers | |
| Subtheme: Provider Stress | “I also think some of the therapists are getting a little overwhelmed themselves, and some I know have cut back hours because they’re personally having trouble managing all of it.” (Clinic 1) “As clinicians, you have your own fear—I mean I’m just going to put it out there, I don’t want to catch it. I don’t want to die from COVID. And we don’t have PPE.” (Clinic 3) “So, you’ve got the clinician’s stress, you’ve got the family’s stress, you’ve got the child’s stress…We count ourselves fortunate that we’re still open. I know lot of other practices are not and so there is that stress. It’s a tough time. So I think asking PCPs to take on managing something for which we didn’t necessarily sign up for in medical school—it’s a delicate ask right now.” (Clinic 3) “I was going to say, my entire bandwidth is on surviving the next six months. That’s my entire bandwidth. I have nothing left.” (Clinic 3) “There’s no national unified message from anyone so we are the de facto trusted reference.” (Clinic 3) |
| Subtheme: Adapting Services to the Pandemic | “And a few that kind of have more involved depression and anxiety—I was doing some like—I would check up on them weekly because some of them couldn’t get in to see their therapist or their anxiety got worse being at home with their family, so I was doing a weekly telemed check-in. That worked until they got in to see their own therapist.” (Clinic 2) “I think all of us have noticed our that all of our well-checks are 5–10 min longer because we have to start with the impact of the pandemic on the families. So all the wellness pieces that we normally do are emphasized even more because we are trying to help people get through an unusual time and with all these restrictions. So, I think all of us have noticed that that has just added to what we were doing already.” (Clinic 3) “Before, if anyone had tested positive for COVID, we had an internal process where someone would call and offer direct counseling to the families, to the parents as well….I know I had a lot of patients who—mom or dad was very stressed with someone in the house who tested positive, or the patient tested positive and wanted someone to talk to. So we had a direct internal way to refer families right after they got their COVID diagnosis.” (Clinic 7) “We have been responsive on multiple levels, including improving our workflows to speed access to care; certainly improving access through remote services, providing both telephone- and video-based responses, so that people can maintain shelter-in-place or social distancing; and then more expanded programming as well…it’s kind of a mix of prevention and clinical services.” (Clinic 8) |
| Patient-Level Domain | |
| Theme: Changes in Mental Health Symptomatology | |
| Subtheme: Anxiety & Depression | “Their anxiety got worse being at home with their family.” (Clinic 2) “As this has gone along further without a clear end sight, I think it has brought up a lot more feelings of being detached from peers, loneliness, depression.” (Clinic 5) “I have seen a lot of anxiety increasing in kids due to living inside. Fears of going outside, but also just not being able to have outdoors activities. I have moms who will call me and tell me that “my child’s anxiety levels are getting worse.” Also, due to online classes, it’s affecting some of our families, our children; they’re struggling more with classes online. Just the anxiety of not knowing or not having what they need at home.” (Clinic 7) “We’ve done some surveying of community needs after COVID hit and shelter-in-place, and those surveys have, as would be expected, revealed a heightened level of anxiety and recurring trauma, depressive feelings, sense of chaos and shortage in the world, and just in general a heightened need.” (Clinic 8) “I’ve seen increased loneliness for kids. Especially the ones who don’t have close relationships with their parents or their family members.” (Clinic 9) |
| Subtheme: Somatization | “I feel like I’m seeing somatization if that’s the right word. I mean the number of kids in the past two and a half weeks who have had stomach aches or accidents, and those are probably the main two, but I mean just the last two and a half weeks is probably more than the previous three months put together. And it’s not 14-year-olds necessarily, it’s like 7-year-olds, 8-year-olds, 5-year-olds who I don’t think have the—to put it together to say that it’s the specter of COVID but it’s being at home, being at home, and being at home, and then still being at home and mom and dad are working, and not seeing their friends, and not going outside and playing.” (Clinic 3) “There is a lot more somatization but we’re pediatricians so I don’t know if your stomach[ache] is because of COVID or we’ve still had appendectomies, we still have kids diagnosed with brain tumors, we still have diabetes.” (Clinic 3) “We have seen patients coming in not only with anxiety and depression, but we are also seeing diabetics getting worse, blood pressure, hypertension’s getting worse; we have kids who otherwise are really healthy but exhibiting anxiety-like symptoms; noncompliance with medications, noncompliance with their usual health care, dietary noncompliance. So we’re seeing some effects of what we feel, or what we think, is more behavioral health-related, even in the medical aspect, just showing up on the blood work, and things like that.” (Clinic 8) |
| Subtheme: Other Symptoms | “I’m seeing a lot of video addiction, video gaming addiction, especially when there’s shelter in place” (Clinic 4) “Three year olds, four year olds, and five year olds, are really starting to act out and say kind of troubling things about wanting to die and wanting to kill themselves.” (Clinic 4) “I felt like we were seeing especially in the beginning of more intense cases like [unknown] psychotic breaks for some of our young adults, or [unknown] manic episodes, and suicide.” (Clinic 6) “I have about three patients—three to four patients a month running away from home. Because they were just—they just felt stuck… In the beginning I just didn’t know what to do. They run away and then they come back three or four days later. Or just walk away from home, take an Uber and go from home for a few hours or half a day then come back. That was something new…But just running away from home. That was something new I saw.” (Clinic 9) |
| Subtheme: Symptomatic Improvement | “They’re certainly not overwhelmed with having to stay up until 2am to finish their schoolwork, and they don’t have all those extracurriculars, so it has been an opportunity for people [to access mental health care].” (Clinic 1) “A lot of the kids who are suffering from some social anxiety because they were going to school, all of a sudden they felt great! It was really kind of sad to me that going to high school was more stressful than a pandemic… The anxiety levels were just dropping way down. Kids were so happy just being with their families… Initially these kids felt great, and now that social anxiety has really ballooned and the thought of going back to school, though they’re not going back to school, but the thought of it was kind of horrifying to them…” (Clinic 5) “…to cite one case and example—a 12-year-old girl with [disease] who’d had a surgical procedure and still had issues…and was being bullied for her obesity. Had been told she was a Chinese with Coronavirus even though she’s actually African American. She was just being bullied left and right including being kicked—physically injured on [the appendage] that she’d had surgery on. The school was not intervening…her life was just so peaceful after [shelter in place]. There were several like that because they deal with a lot of bullying and school anxiety. I do a lot of letter writing to teachers and principals regarding these issues that just don’t seem to be addressed adequately. So, I did see that improvement which was sort of sad like you said.” (Clinic 5) “I have not faced the level of anxiety or depression I expected with patients who are in social isolation or missing friends… I have not had to refer anybody, specifically, for significant enough anxiety or depression related to COVID anytime recently.” (Clinic 5) “I think there’s a subset of patients who are actually thriving in this pandemic, for I think the wrong reasons, not having to go to school, not having to constantly face the challenges that they were having academically.” (Clinic 7) |
| Subtheme: Cascade of Stress from Parent to Child | “I was talking with a friend this weekend about just a regular old 6-month check up that for the most part are generally straight forward are inescapable to go through without addressing the burden that is put upon the family—that is being put on families and then parents and then transferred to the kids. Not necessarily like the 6-month-old but the simple things. It’s just—I think it’s just massive.” (Clinic 3) “The stress that the family is going through certainly bleeds onto the children.” (Clinic 5) “And then I also have a subset of kids and families as a whole that are very directly impacted by this. I think in our country, we see a lot of disparity in the way that COVID is really impacting our community, and, to me, it has been surprising to see how much that is directly impacting the kids themselves… It has been a pretty rude awakening to see that these disparities do trickle down, even to young kids; even when they’re not discussed directly, they feel the limits some way or another. And that’s been pretty evident due to this pandemic.” (Clinic 7) |
| Subtheme: Increased Utilization of Behavioral Health Resources | “I’ve definitely seen more patients who… yeah, their stress levels went up, and they requested some kind of therapy, or their parents requested some kind of therapy directly related to their COVID diagnosis.” (Clinic 7) “We’ve seen a 25% increase in utilization of behavioral health services in our system across our three primary clinics.” (Clinic 8) |
| Theme: Social Determinants of Health | |
| Subtheme: Socioeconomic Status | “I feel like a lot of our families and their kids seem to be coping really well and that might be kind of our demographics. Where – it’s easier. They have houses with yards and some of them are still having help come in…it has been certainly challenging but not to the point where it’s devastating.” (Clinic 2) “I also think there are huge national events and huge international event like what happened in Minneapolis is adding another layer of trauma to what people are already struggling with in terms of economic uncertainty and COVID.” (Clinic 3) “For many families this is a medical crisis but even almost more pressing an economic crisis.” (Clinic 5) “We’re getting a lot of new referrals because people have lost insurance.” (Clinic 5) [Regarding barriers affecting the referral process] “Getting people on the phone. Not being able to pay their bill so then their phone number changes. Then they’re not coming in in-person and are they not answering the phone because they’re working, because their phone is not working anymore, because they lost it, because it’s broken?” (Clinic 6) “…kids worrying for their parents having to go out and work, experiencing severe anxiety around their parents working too much or coming home with the virus, and just a lot of it being that the community that we are in are forced to go to work…it adds these different layers of complexity when you work in a community that has deprivation in the services that are available to families.” (Clinic 7) “For those without homes, having a reliable communication technology and service [would help them engage in care].” (Clinic 8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.M.; Lutz, J.; Khau, A.; Lin, B.; Phillip, N.; Ackerman, S.; Steinbuchel, P.; Mangurian, C. Pediatric Primary Care Perspectives of Mental Health Services Delivery during the COVID-19 Pandemic. Children 2022, 9, 1167. https://doi.org/10.3390/children9081167
Lee CM, Lutz J, Khau A, Lin B, Phillip N, Ackerman S, Steinbuchel P, Mangurian C. Pediatric Primary Care Perspectives of Mental Health Services Delivery during the COVID-19 Pandemic. Children. 2022; 9(8):1167. https://doi.org/10.3390/children9081167
Chicago/Turabian StyleLee, Chuan Mei, Jessica Lutz, Allyson Khau, Brendon Lin, Nathan Phillip, Sara Ackerman, Petra Steinbuchel, and Christina Mangurian. 2022. "Pediatric Primary Care Perspectives of Mental Health Services Delivery during the COVID-19 Pandemic" Children 9, no. 8: 1167. https://doi.org/10.3390/children9081167