1. Introduction
Anemia of prematurity (AOP) is a common condition in growing preterm infants with very low birth weight (VLBW), and the onset of AOP is inversely proportional to the infant’s gestational age (GA) [
1]. The leading cause of AOP is iatrogenic blood loss from phlebotomy; additional factors include impaired erythropoietin (EPO) production, shortened red blood cell life span, and iron deficiency [
2]. Many infants with AOP are symptomatic because of a reduced capacity to maintain adequate oxygenation due to poor compensation for AOP. Symptoms associated with AOP include tachycardia, poor weight gain, increased requirements for supplemental oxygen, and an increased apneic episode or bradycardia.
AOP typically resolves within 3–6 months of age; however, some VLBW preterm infants with AOP require interventions such as packed red blood cell (PRBC) transfusion, iron supplementation, administration of erythropoiesis-stimulating agents, and close laboratory monitoring.
PRBC transfusions are primarily used to treat infants with AOP, but potential adverse effects exist, such as blood-borne infectious disease, graft-versus-host disease, metabolic and cardiovascular complications, hypothermia, iron overload, and increased oxidative stress. Increased oxidative stress may be related to the development of complications in preterm infants, such as bronchopulmonary dysplasia (BPD), retinopathy of prematurity (ROP), necrotizing enterocolitis (NEC), intraventricular hemorrhage (IVH), and periventricular leukomalacia (PVL) [
3,
4,
5].
In 2009, we published a study on the effect of blood transfusions on the outcomes of VLBW preterm infants under two different transfusion criteria, namely restrictive and liberal criteria. The restrictive criteria were as follows for the different types of respiratory support that the infants in our study received: to maintain hematocrit >35% in infants with assisted ventilation; hematocrit >30% in infants with non-invasive respiratory support such as nasal continuous positive airway pressure (CPAP) or high flow nasal cannula (HFNC), and hematocrit >22% in infants breathing room air spontaneously. Applying these restrictive criteria to decrease blood transfusions has achieved better clinical outcomes compared to those obtained with liberal criteria. Strategies to decrease the adverse effects of PRBC transfusion include the application of restrictive criteria for PRBC transfusion and reduction of blood loss resulting from phlebotomy [
6]. The volume of transfusion was 10 mL/kg each time. The restrictive criteria resulted in a lower PRBC transfusion volume and a higher reticulocyte count at day 30 of life; thus, minimizing the amount of PRBC transfusion may be beneficial in preventing BPD in VLBW infants. Therefore, these restrictive criteria for PRBC transfusions have been used in our policy for VLBW infants in the neonatal intensive care unit (NICU) since 2009.
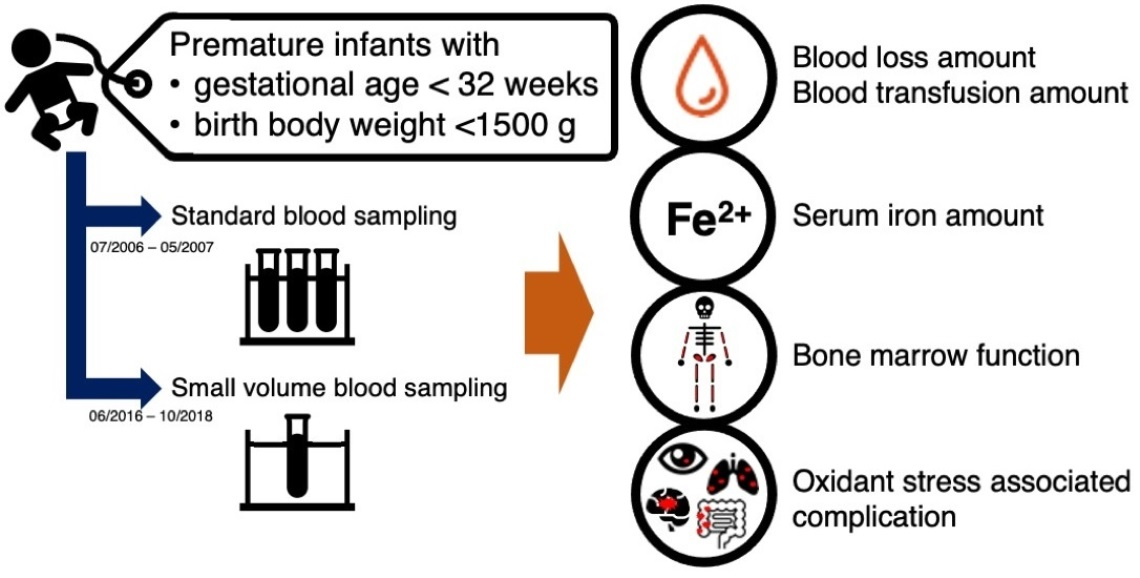
To further decrease the frequency of PRBC transfusion, in 2016, we adopted small volume blood sampling to reduce blood loss from phlebotomy. Because we have different eras in the blood sampling volume, we would compare the outcomes of very low birth weight preterm infants before and after small volume blood sampling. Hence, this study aimed to examine the effect of blood loss reduction due to phlebotomy on the AOP, PRBC transfusion, and outcomes in VLBW preterm infants.
4. Discussion
Our study revealed that small volume sampling was associated with a lower PRBC transfusion volume, less severe anemia, and greater bone marrow function for red blood cell production at 30 days of age in VLBW preterm infants. Reducing blood loss from phlebotomy through small volume blood sampling would reduce the potential adverse effects of PRBC transfusion in VLBW preterm infants.
Growing preterm infants frequently develop AOP, primarily caused by iatrogenic blood loss due to phlebotomy for blood testing [
7]. PRBC transfusions are the primary intervention used to treat infants with AOP; more than half of preterm infants with a birth weight less than 1250 g receive at least one PRBC transfusion during their hospitalization in the NICU [
8]. Although PRBC transfusion promptly and temporarily resolves AOP, there are complications and potential adverse effects, such as metabolic and cardiovascular complications, blood-borne infection, graft-versus-host disease, iron overload, increased oxidative stress, and neurodevelopmental impairment [
9]. Complications such as BPD, ROP, NEC, and IVH are associated with increased oxidative stress by PRBC transfusion [
3,
4,
5].
Low blood hematocrit levels in the blood may result in inadequate tissue oxygenation, leading to symptomatic anemia [
10] that causes the need for more advanced respiratory support with increased oxygen demands, further increases oxidative stress, which is thought to be the origin of complications related to preterm infants, such as BPD and ROP [
3,
5,
8]. In our study, sampling a small volume of blood resulted in less severe anemia, which could decrease the volume of PRBC transfusions required and further reduce oxidative stress and its associated complications. Although our results showed that VLBW preterm infants in the study group had higher hematocrit and lower volume of PRBC transfusions at 30 days old, there were no significant differences in the rate of BPD and ROP between the two groups. The development of BPD may be due to the excessive oxygen supplementation and the positive pressure with a higher volume delivered by the mechanical ventilator besides oxidative stress from PRBC transfusion [
11]. To prevent the development of BPD in VLBW preterm infants, optimizing the mechanical ventilators with supplemental oxygen and also reducing PRBC transfusions are both important [
12].
ROP may be influenced by several factors. Shohat et al. first proposed that blood transfusion was a risk factor for ROP [
13]; this association was later confirmed by other studies. Recent studies have demonstrated that GA and frequency of blood transfusion are independent risk factors for ROP [
14,
15,
16]. However, in our study, there was no significant difference between the proportion of ROP in the study group and the control group.
NEC in preterm infants may be associated with recent exposure to PRBC transfusion [
17], while a higher number and the total volume of PRBC transfusion are associated with an increased risk of confirmed NEC in VLBW infants [
18,
19,
20,
21]. Preterm infants who develop transfusion-associated NEC are at a higher risk of mortality, and surgical NEC is more prevalent following PRBC transfusion [
19,
20,
21]. Furthermore, recent data suggest that severe anemia may influence the risk of gut injury [
22]; therefore, following care approaches such as delayed cord clamping and reducing blood loss due to phlebotomy are suggested [
23]. In our study, the incidence of confirmed NEC was significantly lower in the study group compared to the control group. However, we did not perform delayed cord clamping in both groups. When considering possible risk factors, no association was found between NEC and the following factors: GA, birth weight, sex, Apgar scores at one and five minutes of life, RDS, or PDA. Multiple regression analysis revealed that the risk associated with NEC development in VLBW infants was directly proportional to the overall volume of transfused blood over 30 days (
p = 0.018) (
Table 5), which is consistent with previous reports [
18,
21].
Plasma non-transferrin bound iron has increased significantly in preterm infants after a blood transfusion. It may also be associated with GA in preterm infants, feeding volume, and iron supplementation [
24,
25]. Although preterm infants with small volume blood sampling received a significantly lower PRBC transfusion volume at 30 days of age than infants with standard blood sampling in our study, serum iron levels were significantly higher in the study group than in the control group (
p = 0.003). There were no differences in GA between the two groups, and infants in the study group received a smaller PRBC transfusion volume; therefore, we hypothesized that the higher serum iron levels among infants in the study group were affected by lower blood loss from phlebotomy, and the nutritional support. We adopted a more aggressive feeding policy for infants in the study group due to our advanced knowledge of preterm infant care. As a result, infants in the study group received a significantly larger volume of milk than those in the control group, regardless of the type of milk administered (human milk, donor human milk, or preterm formula) (
Table 4). A more aggressive feeding policy also allows the decreased duration of parental nutrition and intravenous access, which may have contributed to the lower incidence of sepsis in the study group. The study group regained the birth weight significantly faster than the control group (
p = 0.003). Iron supplementation is not used regularly for preterm infants in our NICU, so most of the iron supply comes from human milk or preterm formula. Based on our multiple regression analysis, we postulated that higher serum iron levels among infants in the study group were caused by the increased feeding volume (
Table 4). Higher serum iron levels in the study group may be attributed to the advanced nutritional support provided in the NICU. Simultaneously, significantly lower blood loss volume during phlebotomy in infants with small blood volume sampling as compared to infants with previous standard blood volume sampling may increase serum iron level due to the corresponding decrease in iron loss.
In our study, higher lactate levels were found in the study group than in the control group (
p = 0.043) (
Table 2), despite being within the normal range. Possible causes reasons for increased serum lactate levels include a high concentration of amino acids in parenteral nutrition and an aggressive respiratory weaning strategy. A high serum lactate level indicates tissue hypoxia, and an aggressive respiratory weaning strategy may lead to intermittent hypoxia. However, there were no significant differences between the two groups in duration of the ventilator or nasal CPAP use (
p = 0.073). We further analyzed the potential factors associated with increased lactate levels using multiple regression analysis. This showed that the duration of ventilator/nasal CPAP usage or the duration of supplemental oxygen usage had no effects on serum lactate levels (data not shown).
By using small volume blood sampling with restrictive PRBC transfusion criteria, we increased the quality of care for VLBW preterm infants. The infants in the study group had higher hematocrit, lower volume of PRBC transfusions, and higher reticulocyte levels at 30 days of life. Although there were no differences in the BPD rate and the days of total respiratory support (
Table 5), we found that a higher volume of transfused PRBC over 30 days was associated with the development of NEC in VLBW infants.
The strength of this study is that we provide evidence that small blood sampling could lead to a better quality of VLBW preterm care. The limitations of this study were the small sample size and the inclusion of a historical control group (data of premature infants 10 years ago). Due to advances in preterm care, such as a more aggressive feeding policy, a high concentration of amino acids in parenteral nutrition, and an aggressive respiratory weaning strategy, the care for the historical control group was different from the study group. However, conducting a randomized controlled trial in two groups with standard and small blood sampling is unethical because of advances in preterm care. Therefore, we chose the historical control group from the study conducted 10 years ago to complete this study. The concern for including the historical group is about the inequality between these two groups. The condition after birth was determined by the APGAR scores. In this study, we showed no statistical differences in the first minute and fifth minute APGAR scores of the study group and the control group (
Table 1). Moreover, no significant differences were observed in the proportion of infants with respiratory distress syndrome (RDS) with the need for surfactant therapy between the two groups (
Table 6). Therefore, respiratory condition at birth was comparable to the need for analytical blood determinations. In addition, determining the sample size is challenging because this is a retrospective study. Perhaps due to the sample size, no differences were found in the morbidities of prematurity. We did not exclude those expired infants from this study. However, our institution’s mortality rate has declined compared with 10 years ago; some preterm infants who survived would lead to a higher complication rate such as bronchopulmonary dysplasia than the historical control group.





{kind=link}