
Emotional Intelligence Profiles and Mobbing in Nursing: The Mediating Role of Social Support and Sensitivity to Anxiety

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Ethical Considerations
2.5. Data Analysis
3. Results
3.1. Correlations and Descriptive Statistics
3.2. Emotional Intelligence and Perceived Mobbing: Profiles and Differences
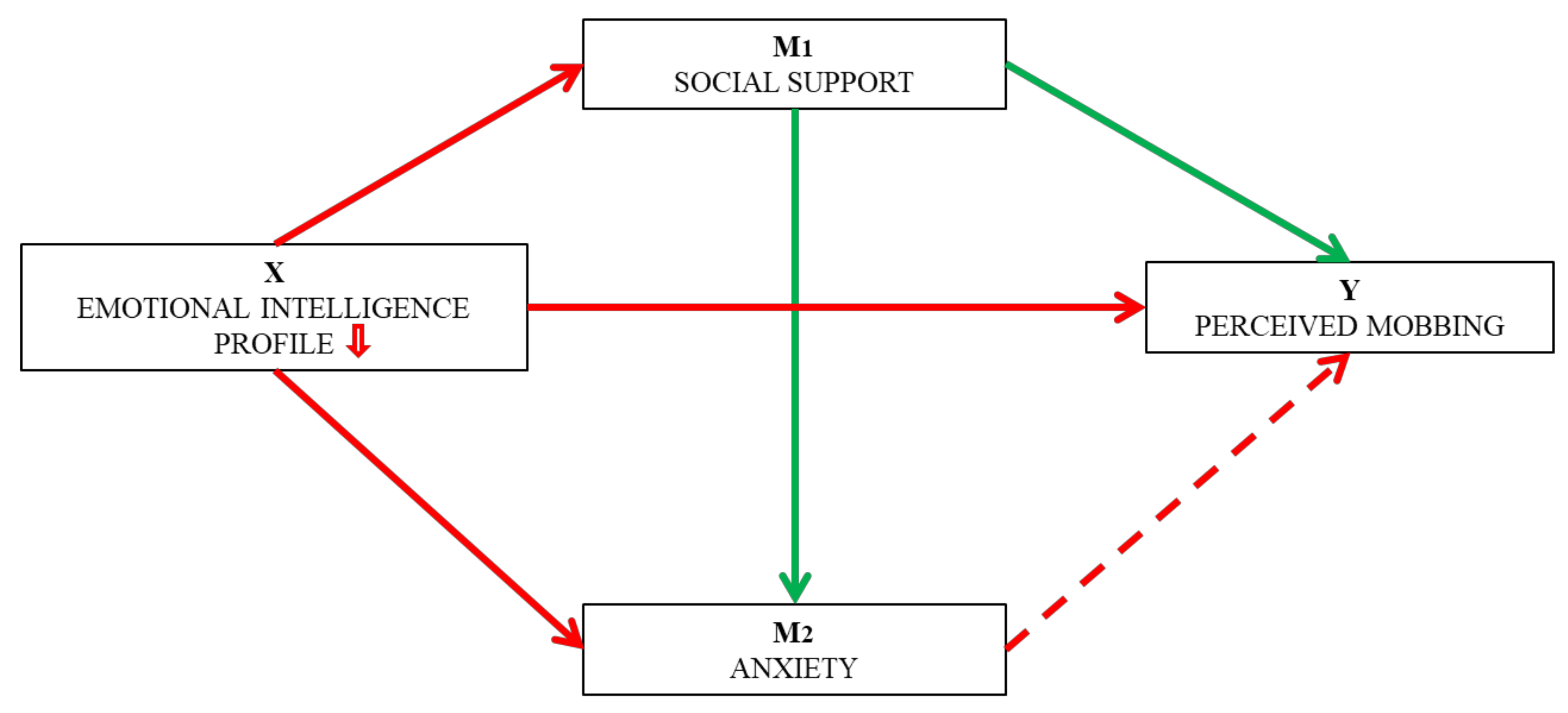
3.3. Model of Social Support and Anxiety Mediation in the Relationship between Emotional Intelligence and Perceived Mobbing
4. Discussion
4.1. Limitations
4.2. Future Investigation
4.3. Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leymann, H. El contenido y desarrollo del mobbing en el trabajo (Mobbing and Victimization at Work). Eur. J. Work Organ. Psychol. 1996, 5, 165–184. [Google Scholar] [CrossRef]
- Munro, C.E.; Phillips, A.W. Bullying in the workplace. Surgery 2020, 10, 653–658. [Google Scholar] [CrossRef]
- Matson, A.; Jordan, T. Workplace bullying investigations: A complex endeavor for a complex problem. Organ. Dyn 2021, in press. [Google Scholar] [CrossRef]
- Lanctôt, N.; Guay, S. The aftermath of workplace violence among healthcare workers: A systematic literature review of the consequences. Aggress. Violent Behav. 2014, 19, 492–501. [Google Scholar] [CrossRef]
- Pérez-Larrazabal, J.; Lopezdelallave, A.; Topa, G. Organizational Tolerance for Workplace Harassment: Development and Validation of the POT Scale. Sustainability 2019, 11, 4078. [Google Scholar] [CrossRef] [Green Version]
- Schlitzkus, L.L.; Vogt, K.N.; Sullivan, M.E.; Schenarts, K.D. Workplace bullying of general surgery residents by nurses. J. Surg. Educ. 2014, 71, e149–e154. [Google Scholar] [CrossRef]
- Samnani, A.; Singh, P. 20 Years of workplace bullying research: A review of the antecedents and consequences of bullying in the workplace. Aggress. Violent Behav. 2012, 17, 581–589. [Google Scholar] [CrossRef]
- Cornoiu, T.S.; Gyorgy, M. Mobbing in organizations. Benefits of identifying the phenomenon. Procedia Soc. Behav. Sci. 2013, 78, 708–712. [Google Scholar] [CrossRef] [Green Version]
- Piñuel, I.; Oñate, A. La incidencia del mobbing o acoso psicológico en enfermería [The incidence of mobbing or psychological harassment in nursing]. In Desigualdad Social y Relaciones de Trabajo; de Elena, J., Ed.; Universidad de Salamanca: Salamanca, Spain, 2004; pp. 187–211. [Google Scholar]
- Molero, M.M.; Pérez-Fuentes, M.C.; Gázquez, J.J. Acoso laboral entre personal de enfermería [Mobbing among nursing staff]. Enferm. Univ. 2016, 13, 114–123. [Google Scholar] [CrossRef] [Green Version]
- Keskin, H.; Akgün, A.E.; Ayar, H.; Kayman, Ş.S. Cyberbullying victimization, counterproductive work behaviours and emotional intelligence at workplace. Procedia Soc. Behav. Sci. 2016, 235, 281–287. [Google Scholar] [CrossRef]
- López-García, C.; Ruiz-Hernández, J.A.; Lor-Zaragoza, L.; Lor-Zaragoza, P.; Jiménez-Barbero, J.A. User Violence and Psychological Well-being in Primary Health-Care Professionals. Eur. J. Psychol. Appl. Leg. Context 2018, 10, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Tang, N.; Thomson, L.E. Workplace violence in Chinese hospitals: The effects of healthcare disturbance on the psychological well-being of Chinese healthcare workers. Int. J. Environ. Res. Public Health 2019, 16, 3687. [Google Scholar] [CrossRef] [Green Version]
- Hirigoyen, M.F.; Valls, N.P. El acoso moral en el trabajo: Distinguir lo verdadero de lo falso [Moral harassment at work: Distinguishing the true from the false]. Rev. Minist. Trab. Asun. Soc. 2001, 41, 154–157. [Google Scholar]
- Piñuel, I. Mobbing. Cómo Sobrevivir al Acoso Psicológico en el Trabajo [Mobbing. How to Survive Psychological Bullying in the Workplace]; Sal Térrae: Bilbao, Spain, 2001. [Google Scholar]
- Wendt, G.W.; Appel-Silva, M.; Jones-Bartoli, A.P. Bullying involvement and psychopathic personality: Disentangling the links among college students. Eur. J. Educ. Psychol. 2019, 12, 125–137. [Google Scholar] [CrossRef]
- García, T.; Rodríguez, C.; Rodríguez, J.; Fernández, A.; Richarte, V.; Ramos-Quiroga, J.A. Psychosocial Profiles of Adults with ADHD: A Comparative Study of Prison and Outpatient Psychiatric Samples. Eur. J. Psychol. Appl. Leg. Context 2019, 11, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Zapf, D.; Gross, C. Conflict escalation and coping with workplace bullying: A replication and extension. Eur. J. Work Organ. Psychol. 2001, 10, 497–522. [Google Scholar] [CrossRef]
- Bar-On, R. Emotional and social intelligence: Insights from the Emotional Quotient Inventory (EQ-i). In Handbook of Emotional Intelligence; Bar-On, R., Parker, J.D.A., Eds.; Jossey-Bass: San Francisco, CA, USA, 2000. [Google Scholar]
- Martins, A.; Ramalho, N.; Morin, E. A comprehensive meta-analysis of the relationship between emotional intelligence and health. Pers. Individ. Differ. 2010, 49, 554–564. [Google Scholar] [CrossRef]
- Trujillo, M.M.; Valderrabano, V.; Hernández, R. Mobbing: Historia, causas, efectos y propuesta de un modelo para las organizaciones mexicanas [Mobbing: History, causes, effects and proposal for a model for Mexican organisations]. Innovar 2007, 17, 71–92. [Google Scholar]
- Ashkanasy, N.M.; Humphrey, R.H.; Huy, Q.N. Integrating emotions and affect in theories of management. Acad. Manag. Rev. 2017, 42, 175–189. [Google Scholar] [CrossRef] [Green Version]
- Akinci, Z.; Yurcu, G.; Ekin, Y. Relationships between Student Personality Traits, Mobbing, and Depression within the Context of Sustainable Tourism Education: The Case of a Faculty of Tourism. Sustainability 2018, 10, 3418. [Google Scholar] [CrossRef] [Green Version]
- Branch, S.; Ramsay, S.; Barker, M. Workplace bullying, mobbing and general harassment: A review. Int. J. Manag. Rev. 2013, 15, 280–299. [Google Scholar] [CrossRef] [Green Version]
- Cropanzano, R.; Dasborough, M.T.; Weiss, H.M. Affective events and the development of leader-member exchange. Acad. Manag. Rev. 2017, 42, 233–258. [Google Scholar] [CrossRef]
- Walter, F.; Cole, M.S.; Humphrey, R.H. Emotional intelligence: Sine qua non of leadership or folderol? Acad. Manag. Perspect. 2011, 25, 45–59. [Google Scholar] [CrossRef] [Green Version]
- Miao, C.; Humphrey, R.H.; Qian, S. Leader emotional intelligence and subordinate job satisfaction: A meta-analysis of main, mediator, and moderator effects. Pers. Individ. Differ. 2016, 102, 13–24. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Fuentes, M.C.; Molero, M.M.; Gázquez, J.J.; Oropesa, N.F. The role of emotional intelligence in engagement in nurses. Int. J. Environ. Res. Public Health 2018, 15, 1915. [Google Scholar] [CrossRef]
- Molero, M.J.; Pérez-Fuentes, M.C.; Soriano, J.G.; Oropesa, N.F.; Simón, M.M.; Gázquez, J.J. Personality and job creativity in relation to engagement in nursing. An. Psicol. 2020, 36, 533–542. [Google Scholar] [CrossRef]
- Wan, H.C.; Downey, L.A.; Stough, C. Understanding non-work presenteeism: Relationships between emotional intelligence, boredom, procrastination and job stress. Pers. Individ. Differ. 2014, 65, 86–90. [Google Scholar] [CrossRef]
- Cabanach, R.; Souto-Gestal, A.; Fernández, R. Perfiles de regulación emocional y estrés académico en estudiantes de fisioterapia [Emotion regulation profiles and academic stress in Physiotherapy students]. Eur. J. Educ. Psychol. 2017, 10, 57–67. [Google Scholar] [CrossRef]
- Sharma, J.; Dhar, R.L.; Tyagi, A. Stress as a mediator between work–family conflict and psychological health among the nursing staff: Moderating role of emotional intelligence. Appl. Nurs. Res. 2016, 30, 268–275. [Google Scholar] [CrossRef]
- Menéndez-Aller, Á.; Postigo, Á.; Montes-Álvarez, P.; González-Primo, J.G.; García-Cueto, E. Humor as a protective factor against anxiety and depression. Int. J. Clin. Health Psychol. 2020, 20, 38–45. [Google Scholar] [CrossRef]
- Killgore, W.D.; Sonis, L.A.; Rosso, I.M.; Rauch, S.L. Emotional Intelligence Partially Mediates the Association between Anxiety Sensitivity and Anxiety Symptoms. Psychol. Rep. 2016, 118, 23–40. [Google Scholar] [CrossRef]
- Littlejohn, P. The missing link: Using emotional intelligence to reduce workplace stress and workplace violence in our nursing and other health care professions. J. Prof. Nurs. 2012, 28, 360–368. [Google Scholar] [CrossRef]
- Choi, K.; Vickers, K.; Tassone, A. Trait emotional intelligence, anxiety sensitivity, and experiential avoidance in stress reactivity and their improvement through psychological methods. Eur. J. Psychol. 2014, 10, 376–404. [Google Scholar] [CrossRef]
- Pagnini, F.; Cavalera, C.; Rovaris, M.; Mendozzi, L.; Molinari, E.; Phillips, D.; Langer, E. Longitudinal associations between mindfulness and well-being in people with multiple sclerosis. Int. J. Clin. Health Psychol. 2019, 19, 22–30. [Google Scholar] [CrossRef]
- Soriano, J.G.; Pérez-Fuentes, M.-C.; Molero, M.M.; Tortosa, B.M.; González, A. Benefits of psychological intervention related to stress and anxiety: Systematic review and meta-analysis. Eur. J. Educ. Psychol. 2019, 12, 191–206. [Google Scholar] [CrossRef]
- Einarsen, S.; Hoel, H.; Zapf, D.; Cooper, C. The concept of bullying and harassment at work: The European tradition. In Bullying and Harassment in the Workplace: Developments in Theory, Research, and Practice, 2nd ed.; Einarsen, S., Hoel, H., Zapf, D., Cooper, C., Eds.; CRC Press: Boca Raton, FL, USA, 2011; pp. 3–40. [Google Scholar]
- Morán, C.; González, M.T.; Landero, R. Valoración psicométrica del Cuestionario de Acoso Psicológico Percibido [Psychometric evaluation of the Perceived Moobing Questionnaire]. J. Occup. Organ. Psychol. 2009, 25, 7–16. [Google Scholar]
- Oh, J.K.; Farh, C.I.C. An emotional process theory of how subordinates appraise, experience, and respond to abusive supervision over time. Acad. Manag. Rev. 2017, 42, 207–232. [Google Scholar] [CrossRef]
- Ball, T.M.; Sullivan, S.; Flagan, T.; Hitchcock, C.A.; Simmons, A.; Paulus, M.P.; Stein, M.B. Selective effects of social anxiety, anxiety sensitivity, and negative affectivity on the neural bases of emotional face processing. Neuroimage 2012, 59, 1879–1887. [Google Scholar] [CrossRef]
- Paulus, M.P.; Stein, M.B. An insular view of anxiety. Biol. Psychiatry 2006, 60, 383–387. [Google Scholar] [CrossRef]
- Desrumaux, P.; Gillet, N.; Nicolas, C. Direct and indirect effects of belief in a just world and supervisor support on burnout via bullying. Int. J. Environ. Res. Public Health 2018, 15, 2330. [Google Scholar] [CrossRef] [Green Version]
- Arnáez, S.; García-Soriano, G.; López-Santiago, J.; Belloch, A. The Spanish validation of the Short Health Anxiety Inventory: Psychometric properties and clinical utility. Int. J. Clin. Health Psychol. 2019, 19, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Grzywacz, J.G.; Marks, N.F. Reconceptualizing the work-family interface: And ecological perspective on the correlates of positive and negative spillover between work and family. J. Occup. Health Psychol. 2000, 5, 111–126. [Google Scholar] [CrossRef] [PubMed]
- Topa, G.; Moriano, J.A. Stress and nurses’ horizontal mobbing: Moderating effects of group identity and group support. Nurs. Outlook 2013, 61, e25–e31. [Google Scholar] [CrossRef]
- Montes-Berges, B.; Augusto, J.M. Exploring the relationship between perceived emotional intelligence, coping, social support and mental health in nursing students. J. Psychiatry Ment. Health Nurs. 2007, 14, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Lasarte, O.; Ramos-Díaz, E.; Sáez, I.A. Rendimiento académico, apoyo social percibido e inteligencia emocional en la universidad [Academic performance, perceived social support and emotional intelligence at the university]. Eur. J. Investig. Health Psychol. Educ. 2019, 9, 39–49. [Google Scholar] [CrossRef] [Green Version]
- Molero, M.M.; Pérez-Fuentes, M.C.; Gázquez, J.J.; Barragán, A.B. Burnout in health professionals according to their self-esteem, social support and empathy profile. Front. Psychol. 2018, 9, 424. [Google Scholar] [CrossRef] [PubMed]
- Molero, M.M.; Pérez-Fuentes, M.C.; Gázquez, J.J.; Simón, M.M.; Martos, Á. Burnout risk and protection factors in certified nursing aides. Int. J. Environ. Res. Public Health 2018, 15, 1116. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Fuentes, M.C.; Molero, M.M.; Gázquez, J.J.; Simón, M.M. Analysis of burnout predictors in nursing: Risk and protective psychological factors. Eur. J. Psychol. Appl. Leg. Context 2019, 11, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Castellano, E.; Muñoz-Navarro, R.; Toledo, M.S.; Spontón, C.; Medrano, L.A. Cognitive processes of emotional regulation, burnout and work engagement. Psicothema 2019, 31, 73–80. [Google Scholar] [CrossRef]
- Extremera, N.; Mérida-López, S.; Sánchez-Álvarez, N.; Quintana-Orts, C.; Rey, L. Un amigo es un tesoro: Inteligencia emocional, apoyo social organizacional y engagement docente [A friend is a treasure: Emotional intelligence, workplace social support and teacher engagement]. Prax. Saber 2019, 10, 69–92. [Google Scholar] [CrossRef] [Green Version]
- Morán, C. Acoso psicológico y burnout en profesionales de recursos humanos [Psychological harassment and burnout in human resources professionals]. In Perspectivas y Retrospectivas de la Psicología Social en Los Albores del Siglo XXI; Romay, J., Ed.; Biblioteca Nueva: Madrid, Spain, 2007; pp. 249–256. [Google Scholar]
- Pérez-Fuentes, M.C.; Gázquez, J.J.; Mercader, I.; Molero, M.M. Brief emotional intelligence inventory for senior citizens (EQ-I-M20). Psicothema 2014, 26, 524–530. [Google Scholar] [CrossRef]
- Bar-On, R.; Parker, J.D.A. BarOn Emotional Quotient Inventory: Youth Version; Multi-Health System, Incorporated: North Tonawanda, NY, USA, 2000. [Google Scholar]
- Calvo, F.; Díaz, M.D. Apoyo social percibido: Características psicométricas del cuestionario Caspe en una población urbana geriátrica [Perceived social support: Psychometric properties of CASPE questionnaire in urban not institutionalized elderly populatio]. Psicothema 2004, 16, 570–575. [Google Scholar]
- Taylor, S.; Zvolensky, M.J.; Cox, B.J.; Deacon, B.; Heimberg, R.G.; Ledley, D.R.; Abramowitz, J.S.; Holaway, R.M.; Sandin, B.; Stewart, S.H.; et al. Robust dimensions of anxiety sensitivity: Development and initial validation of the Anxiety Sensitivity Index-3 (ASI-3). Psychol. Assess. 2007, 19, 176–188. [Google Scholar] [CrossRef] [Green Version]
- Sandín, B.; Valiente, R.M.; Chorot, P.; Santed, M.A. ASI-3: Nueva escala para la evaluación de la sensibilidad a la ansiedad [ASI-3: A new scale for the assessment of anxiety sensitivity]. Rev. Psicopatol. Psicol. Clin. 2007, 12, 91–104. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Mahwah, NJ, USA, 1988. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression Based Approach; The Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Pérez-Fuentes, M.C.; Gázquez, J.J.; Molero, M.M.; Oropesa, N.F.; Martos, Á. Violence and Job Satisfaction of Nurses: Importance of a Support Network in Healthcare. Eur. J. Psychol. Appl. Leg. Context 2021, 13, 21–28. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Perceived Mobbing | - | ||||||||||
| 2. Intrapersonal | −0.12 *** | - | |||||||||
| 3. Interpersonal | −0.11 *** | 0.47 *** | - | ||||||||
| 4. Stress Management | −0.21 *** | 0.06 * | 0.11 *** | - | |||||||
| 5. Adaptability | −0.18 *** | 0.58 *** | 0.70 *** | 0.15 *** | - | ||||||
| 6. Mood | −0.23 *** | 0.51 *** | 0.54 *** | 0.21 *** | 0.66 *** | - | |||||
| 7. Social Support | −0.30 *** | 0.31 *** | 0.38 *** | 0.17 *** | 0.38 *** | 0.50 *** | - | ||||
| 8. Global Anxiety | 0.24 *** | −0.06 * | −0.04 | −0.34 *** | −0.10 *** | −0.18 *** | −0.22 *** | - | |||
| 9. Physical anxiety | 0.20 *** | −0.03 | −0.06 * | −0.29 *** | −0.10 *** | −0.16 *** | −0.21 *** | 0.92 *** | - | ||
| 10. Cognitive anxiety | 0.21 *** | −0.04 | −0.08 ** | −0.35 *** | −0.12 *** | −0.20 *** | −0.26 *** | 0.92 *** | 0.83 *** | - | |
| 11. Social anxiety | 0.24 *** | −0.09 *** | 0.02 | −0.27 *** | −0.06 * | −0.14 *** | −0.15 *** | 0.87 *** | 0.67 *** | 0.68 *** | - |
| M | 26.45 | 2.70 | 3.11 | 3.26 | 2.96 | 3.11 | 30.05 | 12.97 | 3.69 | 2.81 | 6.47 |
| SD | 9.24 | 0.70 | 0.52 | 0.53 | 0.56 | 0.64 | 4.05 | 11.80 | 4.53 | 4.04 | 4.45 |
| Emotional Intelligence | t | d | ||||||
|---|---|---|---|---|---|---|---|---|
| c1 | c2 | |||||||
| N | Mean | SD | N | Mean | SD | |||
| Perceived mobbing | 525 | 24.34 | 9.04 | 832 | 27.34 | 9.13 | −6.80 *** | 0.38 |
| Social support | 525 | 31.81 | 2.83 | 832 | 28.92 | 4.31 | 14.82 *** | 0.83 |
| Global Anxiety | 525 | 10.62 | 11.67 | 832 | 14.46 | 11.65 | −5.90 *** | 0.33 |
| Physical anxiety | 525 | 2.88 | 4.46 | 832 | 4.21 | 4.50 | −5.32 *** | 0.30 |
| Cognitive anxiety | 525 | 2.01 | 3.87 | 832 | 3.32 | 4.06 | −5.97 *** | 0.33 |
| Social anxiety | 525 | 5.74 | 4.46 | 832 | 6.93 | 4.39 | −4.85 *** | 0.27 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molero Jurado, M.d.M.; Martos Martínez, Á.; Barragán Martín, A.B.; Simón Márquez, M.d.M.; Oropesa Ruiz, N.F.; Sisto, M.; Pérez-Fuentes, M.d.C.; Gázquez Linares, J.J. Emotional Intelligence Profiles and Mobbing in Nursing: The Mediating Role of Social Support and Sensitivity to Anxiety. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 345-357. https://doi.org/10.3390/ejihpe11020026
Molero Jurado MdM, Martos Martínez Á, Barragán Martín AB, Simón Márquez MdM, Oropesa Ruiz NF, Sisto M, Pérez-Fuentes MdC, Gázquez Linares JJ. Emotional Intelligence Profiles and Mobbing in Nursing: The Mediating Role of Social Support and Sensitivity to Anxiety. European Journal of Investigation in Health, Psychology and Education. 2021; 11(2):345-357. https://doi.org/10.3390/ejihpe11020026
Chicago/Turabian StyleMolero Jurado, María del Mar, África Martos Martínez, Ana Belén Barragán Martín, María del Mar Simón Márquez, Nieves Fátima Oropesa Ruiz, Maria Sisto, María del Carmen Pérez-Fuentes, and José Jesús Gázquez Linares. 2021. "Emotional Intelligence Profiles and Mobbing in Nursing: The Mediating Role of Social Support and Sensitivity to Anxiety" European Journal of Investigation in Health, Psychology and Education 11, no. 2: 345-357. https://doi.org/10.3390/ejihpe11020026