

The Effect of Ice on Shoulder Proprioception in Badminton Athletes




Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessment
2.2.1. Anthropometric Parameters Assessment
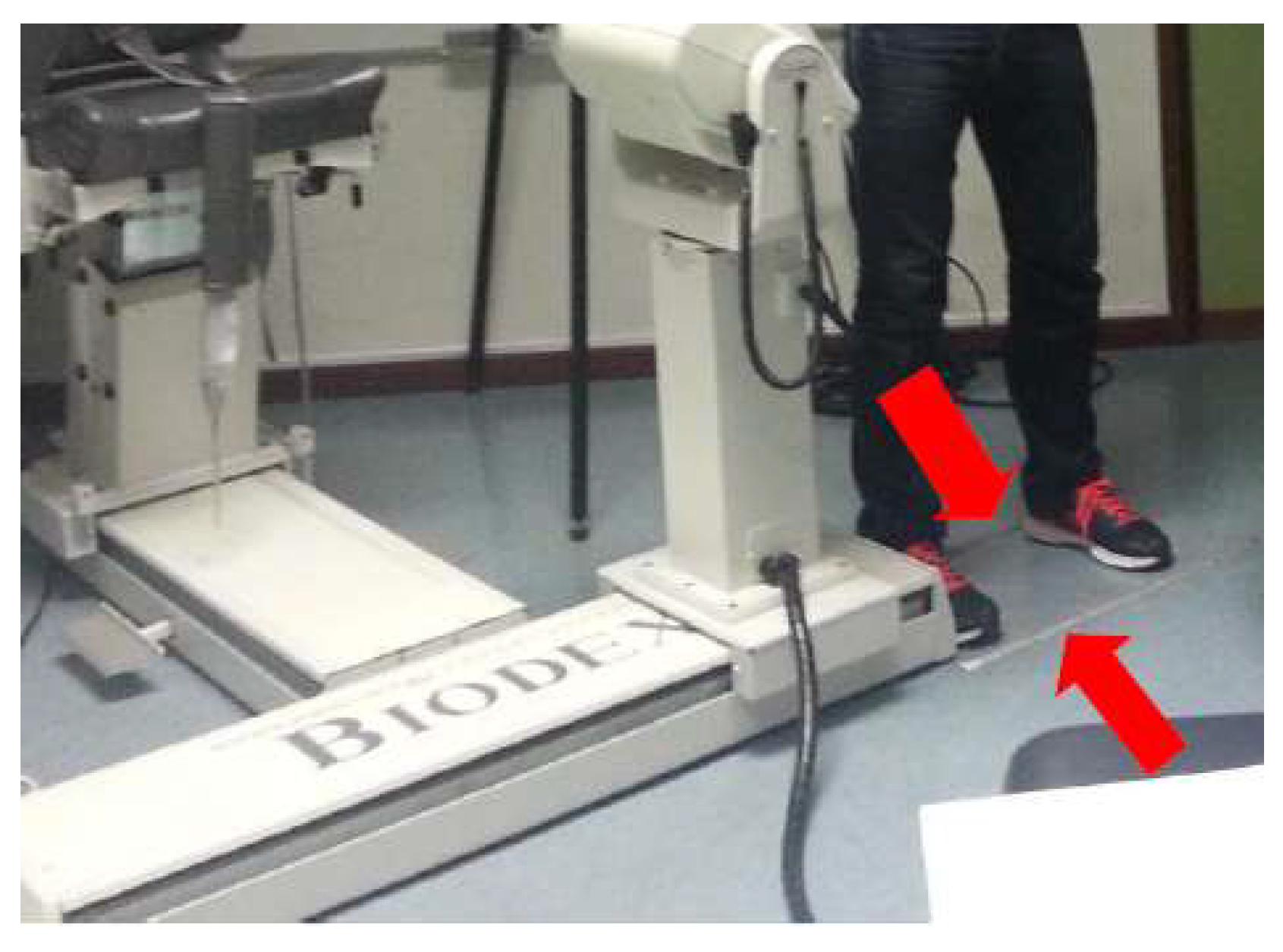
2.2.2. Isokinetic Dynamometer Setup Preparation
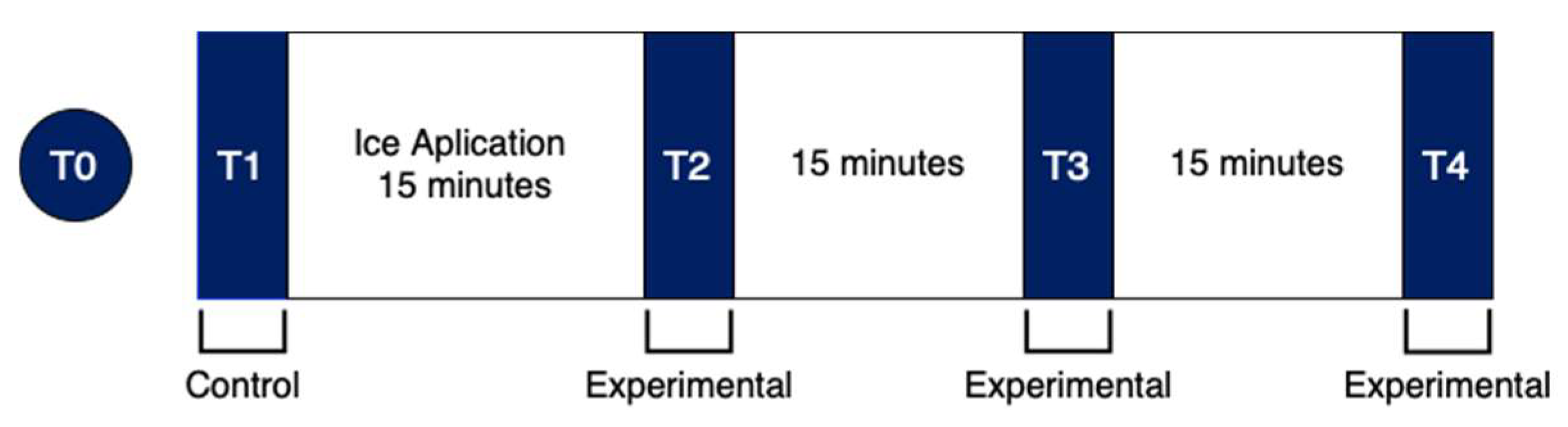
T-Assessment Moment
2.2.3. Maximum Strength Assessment
2.2.4. Proprioception Assessment
2.2.5. Active JPS Assessment
2.2.6. MTS Assessment
2.3. Data Processing and Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Descriptive Analysis
4.2. Changes in Proprioception after Ice Application
4.3. Effect of Ice on Proprioception over Time
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Röijezon, U.; Clark, N.C.; Treleaven, J. Proprioception in musculoskeletal rehabilitation. Part 1: Basic science and principles of assessment and clinical interventions. Man. Ther. 2015, 20, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Clark, N.C.; Röijezon, U.; Treleaven, J. Proprioception in musculoskeletal rehabilitation. Part 2: Clinical assessment and intervention. Man. Ther. 2015, 20, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Waddington, G.; Adams, R.; Anson, J.; Liu, Y. Assessing proprioception: A critical review of methods. J. Sport Health Sci. 2015, 5, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Furmanek, M.P.; Słomka, K.; Juras, G. The effects of cryotherapy on proprioception system. Biomed. Res. Int. 2014, 2014, 696397. [Google Scholar] [CrossRef] [PubMed]
- Proske, U.; Gandevia, S.C. The proprioceptive senses: Their roles in signaling body shape, body position and movement, and muscle force. Physiol. Rev. 2012, 92, 1651–1697. [Google Scholar] [CrossRef]
- Costello, J.T.; Algar, L.A.; Donnelly, A.E. Effects of whole-body cryotherapy (−110 °C) on proprioception and indices of muscle damage. Scand. J. Med. Sci. Sports 2012, 22, 190–198. [Google Scholar] [CrossRef]
- Surenkok, O.; Aytar, A.; Akman, M.N.; Tüzün, E.H. Cryotherapy impairs knee joint position sense and balance. Isokinet. Exerc. Sci. 2008, 16, 69–73. [Google Scholar] [CrossRef]
- Shariff, A.H.; George, J.; Ramlan, A.A. Musculoskeletal injuries among malaysian badminton players. Singapore Med. J. 2009, 50, 1095–1097. [Google Scholar]
- Yung, P.S.-H.; Chan, R.H.-K.; Wong, F.C.-Y.; Cheuk, P.W.-L.; Fong, D.T.-P. Epidemiology of injuries in Hong Kong elite badminton athletes. Res. Sport Med. 2007, 15, 133–146. [Google Scholar] [CrossRef]
- Krøner, K.; Schmidt, S.A.; Nielsen, A.B.; Yde, J.; Jakobsen, B.W.; Møller-Madsen, B.; Jensen, J. Badminton injuries. Br. J. Sports Med. 1990, 24, 169–172. [Google Scholar] [CrossRef]
- Høy, K.; Lindblad, B.E.; Terkelsen, C.J.; Helleland, H.E. Badminton injuries—A prospective epidemiological and socioeconomic study. Br. J. Sports Med. 1994, 28, 276–279. [Google Scholar] [CrossRef] [PubMed]
- Fahlström, M.; Björnstig, U.; Lorentzon, R. Acute badminton injuries. Scand. J. Med. Sci. Sports 1998, 8, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Mahmudieh, B.; Faezi, G.; Alizadeh, M.H.; Rahnama, N. Common injuries in iranian female elite badminton players. Glob. J. Sci. Eng. Technol. 2013, 12, 24–28. [Google Scholar]
- Jørgensen, U.; Winge, S. Injuries in badminton. Sports Med. 1990, 10, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Miyake, E.; Yatsunami, M.; Kurabayashi, J.; Teruya, K.; Sekine, Y.; Endo, T.; Nishida, R.; Takano, N.; Sato, S.; Kyung, H.J. A prospective epidemiological study of injuries in japanese national tournament-level badminton players from junior high school to university. Asian J. Sports Med. 2016, 7, e29637. [Google Scholar] [CrossRef]
- Duarte, A.; Neto, F.; Proença, A.; Torres, R. Efeito da crioterapia na noção de posição articular activa do ombro: Um estudo comparativo entre o género masculino e feminino. Rev. Port. Fisioter No Desporto 2008, 2, 38–45. [Google Scholar]
- Dover, G.; Powers, M.E. Cryotherapy does not impair shoulder joint position sense. Arch. Phys. Med. Rehabil. 2004, 85, 1241–1246. [Google Scholar] [CrossRef]
- Wassinger, C.A.; Myers, J.B.; Gatti, J.M.; Conley, K.M.; Lephart, S.M. Proprioception and throwing accuracy in the dominant shoulder after cryotherapy. J. Athl. Train. 2007, 42, 84–89. [Google Scholar]
- Costello, J.T.; Donnelly, A.E. Cryotherapy and joint position sense in healthy participants: A systematic review. J. Athl. Train. 2010, 45, 306–316. [Google Scholar] [CrossRef]
- Beelen, P.E.; van Dieën, J.H.; Prins, M.R.; Nolte, P.A.; Kingma, I. The effect of cryotherapy on postural stabilization assessed by standardized horizontal perturbations of a movable platform. Gait Posture 2022, 94, 32–38. [Google Scholar] [CrossRef]
- Costello, J.T.; Donnelly, A.E. Effects of cold water immersion on knee joint position sense in healthy volunteers. J. Sports Sci. 2011, 29, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Eftekhari, F.; Sadeghi, H.; Rajabi, H.; Memar, R.; Leili, A.K. The effect of local cooling on knee joint position sense in healthy trained young females. Int. J. Sport Stud. 2015, 5, 700–707. [Google Scholar]
- Hopper, D.; Whittington, D.; Davies, J.; Chartier, J.D. Does ice immersion influence ankle joint position sense? Physiother. Res. Int. 1997, 2, 223–236. [Google Scholar] [CrossRef] [PubMed]
- Khanmohammadi, R.; Someh, M.; Ghafarinejad, F. The effect of cryotherapy on the normal ankle joint position sense. Asian J. Sports Med. 2011, 2, 91. [Google Scholar] [CrossRef]
- LaRiviere, J.; Osternig, L.R. The effect of ice immersion on joint position sense. J. Sport Rehabil. 1994, 3, 58–67. [Google Scholar] [CrossRef]
- Lins, C.A.D.A.; Macedo, L.B.; Silveira, R.A.G.; Borges, D.T.; Brasileiro, J.S. Influence of cryotherapy on balance and joint position sense in healthy subjects: Randomized clinical trial. Man. Ther. Posturology Rehabil. J. 2015, 13, 276. [Google Scholar] [CrossRef]
- Ozmun, J.; Thieme, H.; Ingersoll, C.; Knight, K. Cooling does not affect knee proprioception. J. Athl. Train. 1996, 51, 455–461. [Google Scholar]
- Selkow, N.M.; Rivas, S. The effect of two cooling modalities on knee joint position sense. J. Athl. Enhanc 2014, 3, 3–5. [Google Scholar]
- Alexander, J.; Selfe, J.; Oliver, B.; Mee, D.; Carter, A.; Scott, M.; Richards, J.; May, K. An exploratory study into the effects of a 20 minute crushed ice application on knee joint position sense during a small knee bend. Phys. Ther. Sport 2016, 18, 21–26. [Google Scholar] [CrossRef]
- Balakrishnan, R.; Charles, W. The effect of cold water immersion cryotherapy on normal ankle joint position sense in young adults among AMU students. Int. J. Phys. Educ. Sport Health 2016, 3, 293–298. [Google Scholar]
- Oliveira, R.; Ribeiro, F.; Oliveira, J. Cryotherapy impairs knee joint position sense. Int. J. Sports Med. 2010, 31, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, F.; Moreira, S.; Neto, J.; Oliveira, J. Is the deleterious effect of cryotherapy on proprioception mitigated by exercise? Int. J. Sports Med. 2013, 34, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Uchio, Y.; Ochi, M.; Fujihara, A.; Adachi, N.; Iwasa, J.; Sakai, Y. Cryotherapy influences joint laxity and position sense of the healthy knee joint. Arch. Phys. Med. Rehabil. 2003, 84, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Terabayashi, N.; Shi, B.; Shin, S.; Kasuga, K.; Yabumoto, T.; Shimizu, K.; Matsuoka, T. Effects of cryotherapy on joint position sense and intraarticular blood flow volume in healthy knee joints. J. Phys. Fit. Sport Med. 2013, 2, 243–250. [Google Scholar] [CrossRef]
- Haupenthal DP dos, S.; de Noronha, M.; Haupenthal, A.; Ruschel, C.; Nunes, G.S. Skin cooling and force replication at the ankle in healthy individuals: A crossover randomized controlled trial. J. Athl. Train. 2015, 50, 621–628. [Google Scholar] [CrossRef]
- Rubley, M.D.; Denegar, C.R.; Buckley, W.E.; Newell, K.M. Cryotherapy, sensation, and isometric-force variability. J. Athl. Train. 2003, 38, 113–119. [Google Scholar]
- Tremblay, F.; Estephan, L.; Legendre, M.; Sulpher, S. Influence of local cooling on proprioceptive acuity in the quadriceps muscle. J. Athl. Train. 2001, 36, 119–123. [Google Scholar]
- Holt, G.R. Declaration of Helsinki—The World’s Document of Conscience and Responsibility. South. Med. J. 2014, 107, 407. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Strobe Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef]
- Tavares, N.; Castro, M.A. Estudo piloto: Posição Angular de Flexão do Ombro no Momento de Impacto no Volante nos Batimentos de Badminton Clear, Amortie e Remate. Master’s Thesis, Departamento de Engenharia Mecanica–Universidade do Minho, Braga, Portugal, 2017. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample (n = 30) | Male (n = 15) | Female (n = 15) | ||||||
|---|---|---|---|---|---|---|---|---|
| Min | Max | Mean | SD | Mean | SD | Mean | SD | |
| Age (years) | 15.00 | 34.00 | 21.00 | 5.60 | 21.47 | 5.71 | 20.53 | 5.64 |
| Weight (kg) | 47.00 | 96.40 | 64.77 | 11.33 | 72.39 | 10.16 | 57.15 | 6.18 |
| Height (cm) | 1.52 | 1.87 | 1.70 | 0.10 | 1.78 | 0.05 | 1.62 | 0.05 |
| IMC (kg/m2) | 17.00 | 27.00 | 21.83 | 2.34 | 22.33 | 2.58 | 21.33 | 2.02 |
| Weekly training sessions | 1.00 | 6.00 | 2.93 | 1.26 | 3.33 | 1.35 | 2.53 | 1.06 |
| Years of badminton practice | 1.00 | 27.00 | 8.40 | 6.93 | 10.00 | 7.08 | 6.80 | 6.62 |
| Control | Experimental | Wilcoxon Test | ||||
|---|---|---|---|---|---|---|
| Z | p-Value | |||||
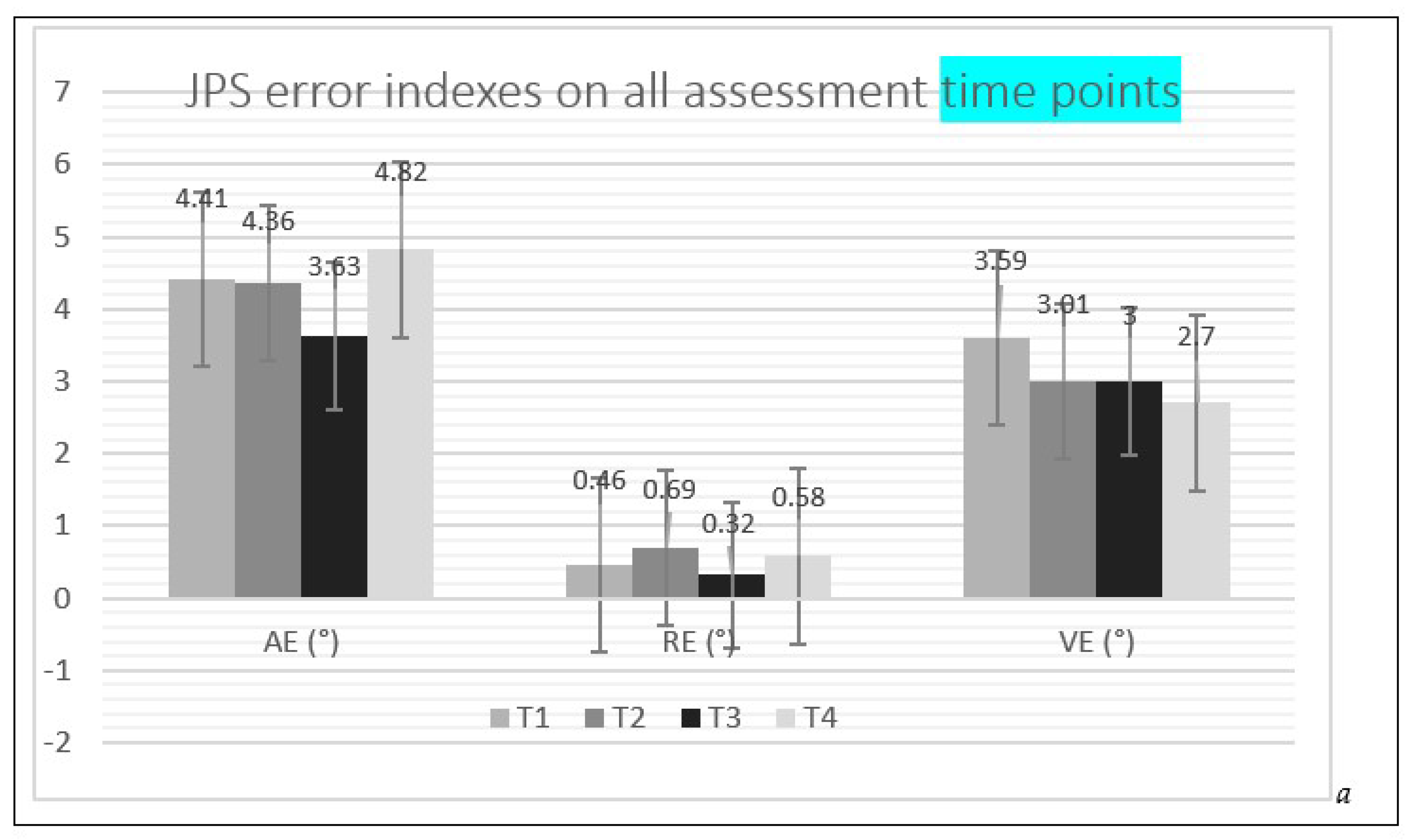
| JPS | T1–T2 Before ice application – after ice application | AE (°) | 4.41 ± 3.04 | 4.36 ± 3.33 | −0.173 | 0.863 |
| RE (°) | 0.46 ± 4.96 | 0.69 ± 5.16 | −0.010 | 0.992 | ||
| VE (°) | 3.59 ± 1.94 | 3.01 ± 1.70 | −1.583 | 0.113 | ||
| T1–T3 15 min After ice application | AE (°) | 4.41 ± 3.04 | 3.63 ± 2.23 | −1.310 | 0.190 | |
| RE (°) | 0.46 ± 4.96 | 0.32 ± 3.72 | −0.134 | 0.894 | ||
| VE (°) | 3.59 ± 1.94 | 3.00 ± 1.82 | −1.321 | 0.187 | ||
| T1–T4 30 min After ice application | AE (°) | 4.41 ± 3.04 | 4.82 ± 3.40 | −0.878 | 0.380 | |
| RE (°) | 0.46 ± 4.96 | 0.58 ± 5.68 | −0.260 | 0.795 | ||
| VE (°) | 3.59 ± 1.94 | 2.70 ± 1.76 | −2.283 | 0.022 | ||
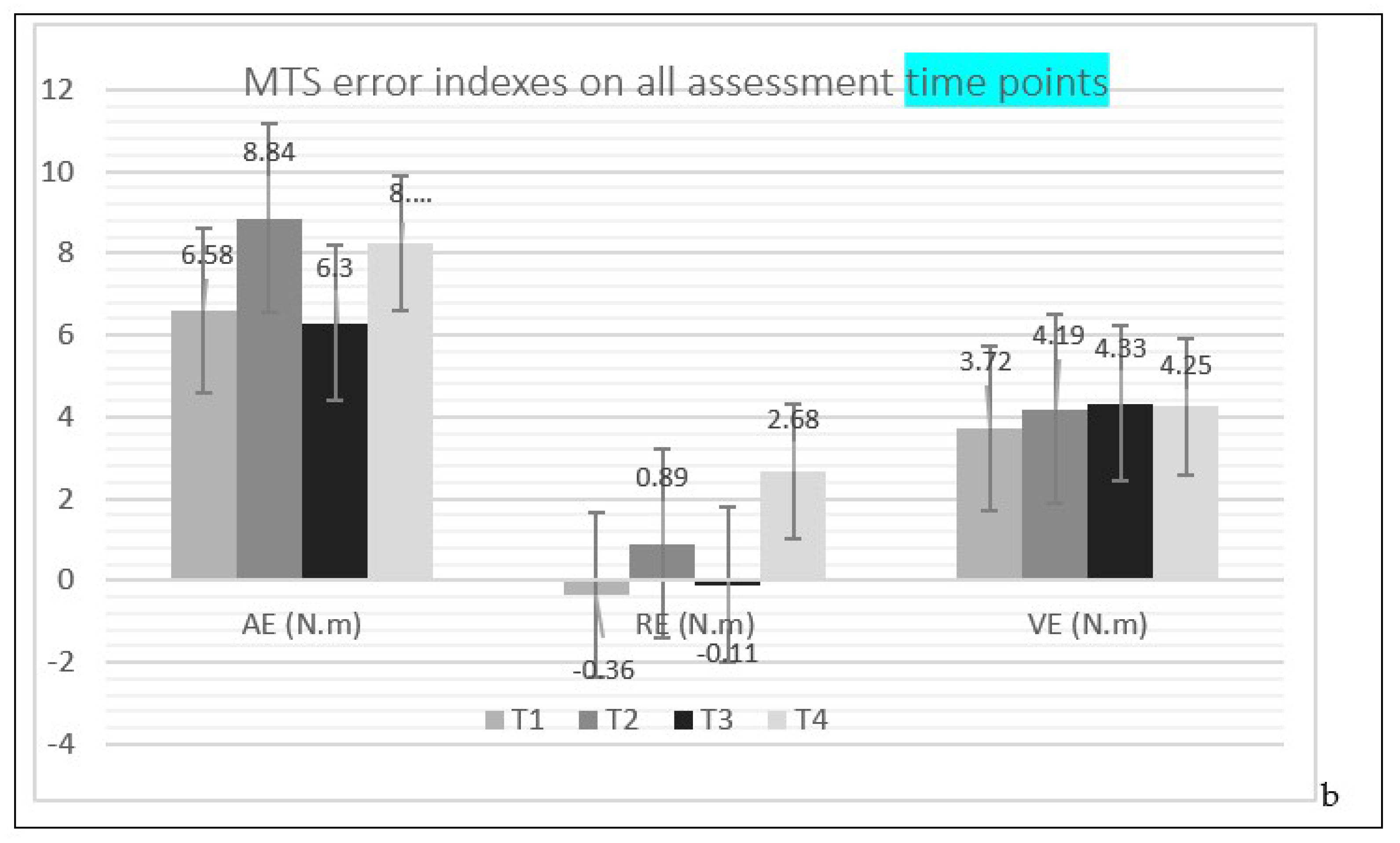
| MTS | T1–T2 Before ice application – after ice application | AE (N.m) | 6.58 ± 6.27 | 8.84 ± 8.07 | −0.812 | 0.417 |
| RE (N.m) | −0.36 ± 8.89 | 0.89 ± 11.89 | −0.370 | 0.711 | ||
| VE (N.m) | 3.72 ± 2.17 | 4.19 ± 2.81 | −0.319 | 0.750 | ||
| T1–T3 15 min After ice application | AE (N.m) | 6.58 ± 6.27 | 6.30 ± 4.53 | −0.216 | 0.829 | |
| RE (N.m) | −0.36 ± 8.89 | −0.11 ± 7.37 | −0.103 | 0.918 | ||
| VE (N.m) | 3.72 ± 2.17 | 4.33 ± 2.91 | −0.792 | 0.428 | ||
| T1–T4 30 min After ice application | AE (N.m) | 6.58 ± 6.27 | 8.23 ± 5.70 | −1.399 | 0.162 | |
| RE (N.m) | −0.36 ± 8.89 | 2.68 ± 9.34 | −1.471 | 0.141 | ||
| VE (N.m) | 3.72 ± 2.17 | 4.25 ± 3.17 | −0.442 | 0.658 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marouvo, J.; Tavares, N.; Dias, G.; Castro, M.A. The Effect of Ice on Shoulder Proprioception in Badminton Athletes. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 671-683. https://doi.org/10.3390/ejihpe13030051
Marouvo J, Tavares N, Dias G, Castro MA. The Effect of Ice on Shoulder Proprioception in Badminton Athletes. European Journal of Investigation in Health, Psychology and Education. 2023; 13(3):671-683. https://doi.org/10.3390/ejihpe13030051
Chicago/Turabian StyleMarouvo, Joel, Nuno Tavares, Gonçalo Dias, and Maria António Castro. 2023. "The Effect of Ice on Shoulder Proprioception in Badminton Athletes" European Journal of Investigation in Health, Psychology and Education 13, no. 3: 671-683. https://doi.org/10.3390/ejihpe13030051
APA StyleMarouvo, J., Tavares, N., Dias, G., & Castro, M. A. (2023). The Effect of Ice on Shoulder Proprioception in Badminton Athletes. European Journal of Investigation in Health, Psychology and Education, 13(3), 671-683. https://doi.org/10.3390/ejihpe13030051