Light in Orthodontics: Applications of High-Intensity Lasers, Photobiomodulation, and Antimicrobial Photodymanic Therapies in Daily Practice

 , ,
, ,
Abstract
:1. Introduction
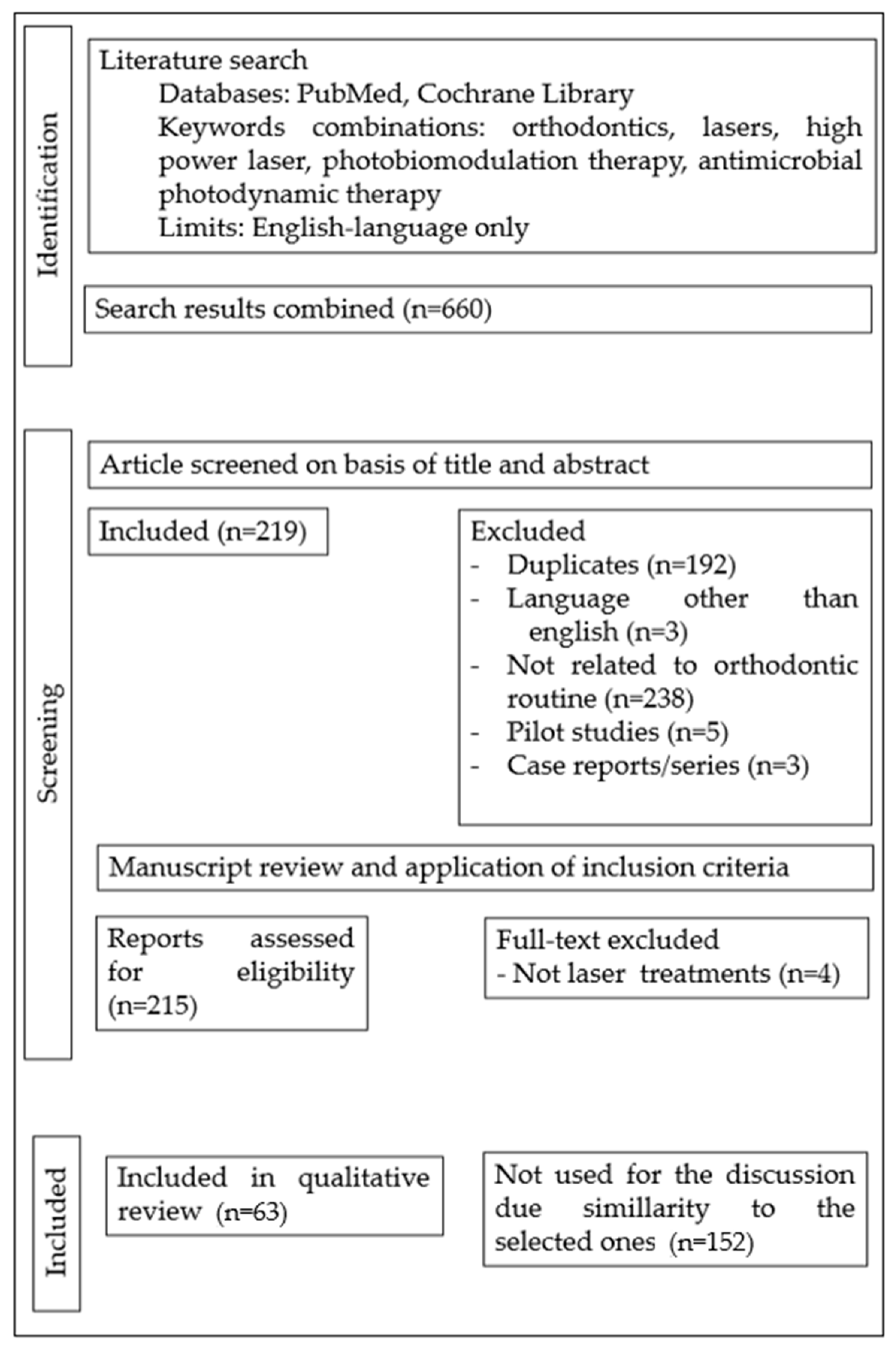
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Inclusion Criteria
- Scientific articles published up to 30 April 2023.
- Scientific articles published in the English language.
- In vitro and in vivo studies that mention tissue reactions to laser light relevant to the orthodontic routine.
- The literature search was not restricted to any specific age interval, gender, duration of orthodontic treatment, or type of appliance.
- Only articles related to laser treatments in connection with orthodontic practice were considered relevant to the purpose of this review.
2.1.2. Exclusion Criteria
- Papers with no clear report or not related to the use of lasers in orthodontic clinical practice.
- Case reports, case series, pilot studies, study protocols, documents, and book chapters.
2.2. Literature Search Strategy
Data Sources
3. Results
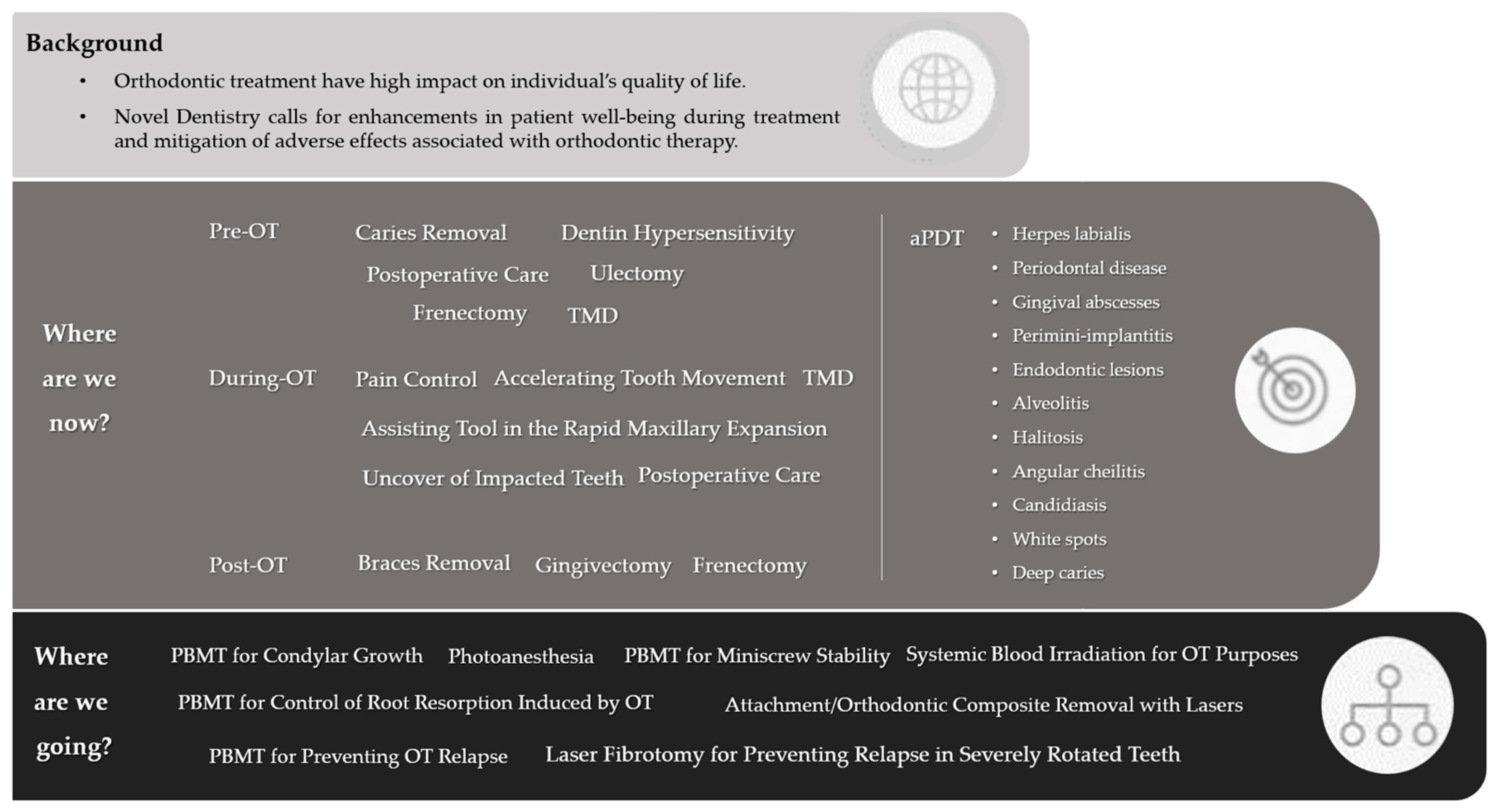
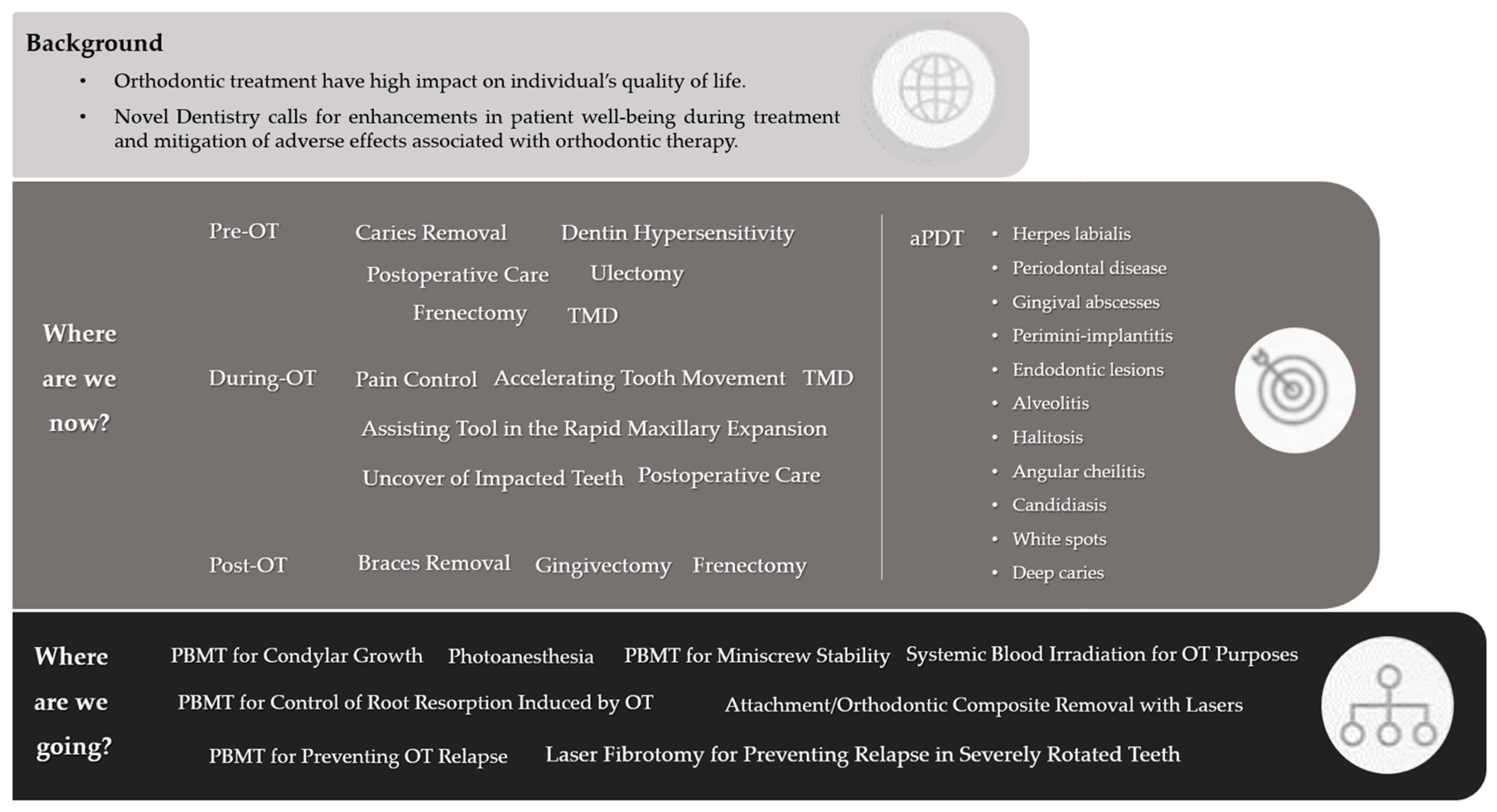
3.1. Where Are We Now?
3.1.1. Pre-Orthodontic Treatment Care
3.1.2. Pain Control of Orthodontic Activation Responses
3.1.3. Photobiomodulation of Tooth Movement
3.1.4. Assisting Tool in Rapid Maxillary Expansion
3.1.5. Postoperative Care with Lasers
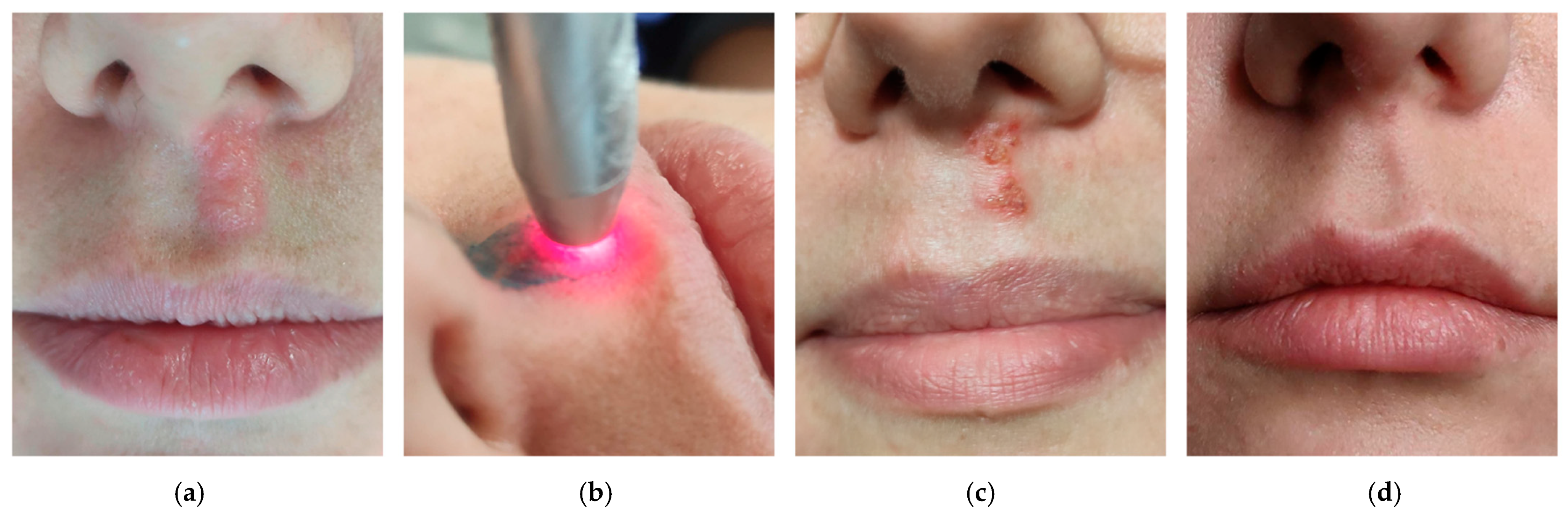
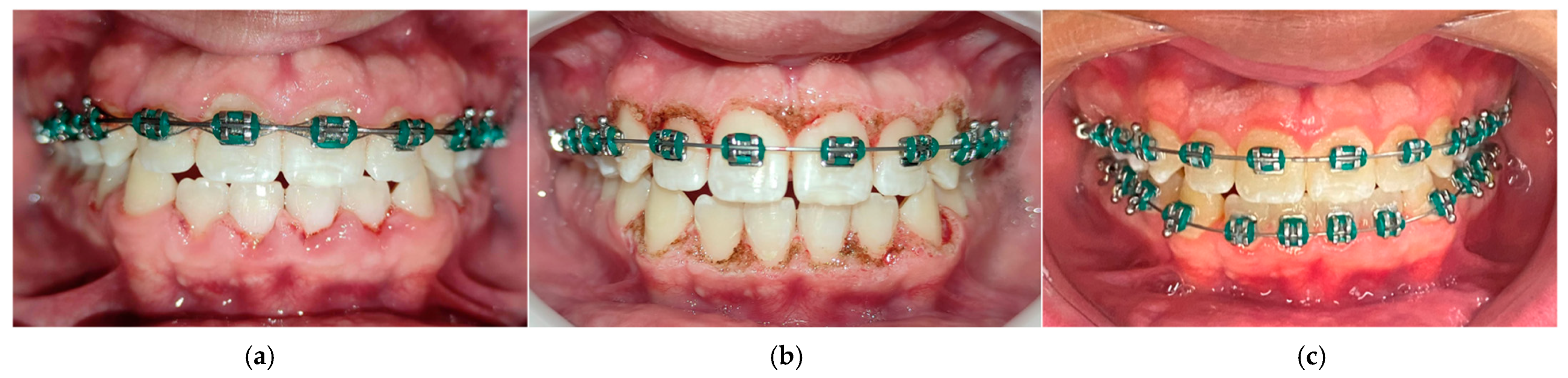
3.1.6. aPDT Easily Solving Infections during Orthodontic Treatment
3.1.7. Soft Tissue Management with High-Intensity Lasers Complementing Orthodontic Therapy
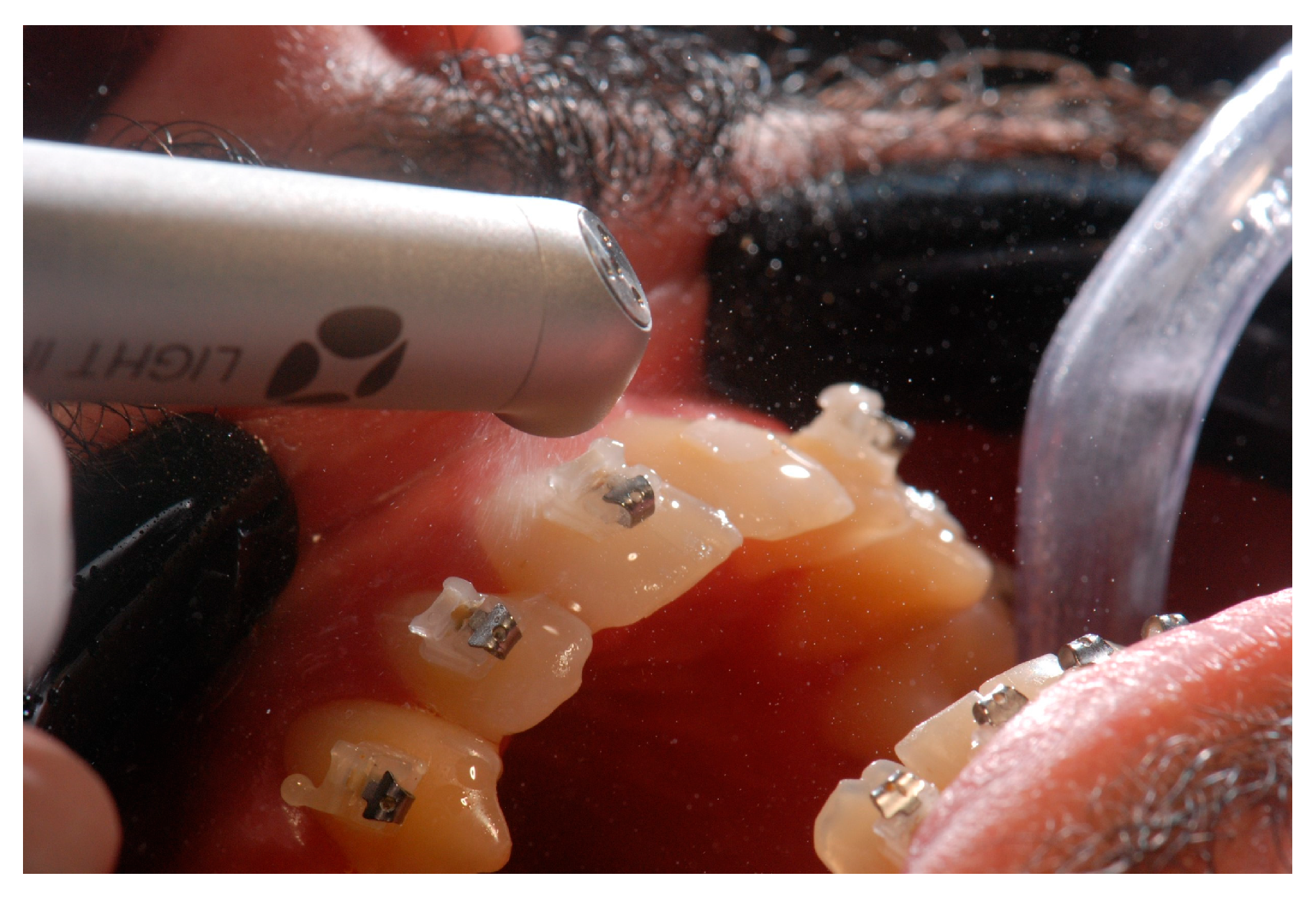
3.1.8. Braces Removal with the Touch of Light
3.2. The “Ideal Protocol” Conjecture
3.3. Where Are We Going?
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alam, M.K.; Abutayyem, H.; Kanwal, B.; Shayeb, M.A.L. Future of Orthodontics—A Systematic Review and Meta-Analysis on the Emerging Trends in This Field. J. Clin. Med. 2023, 12, 532. [Google Scholar] [CrossRef]
- Goldman, L.; Hornby, P.; Meyer, R.; Goldman, B. Impact of the Laser on Dental Caries. Nature 1964, 203, 417. [Google Scholar] [CrossRef]
- Parker, S.; Cronshaw, M.; Anagnostaki, E.; Mylona, V.; Lynch, E.; Grootveld, M. Current Concepts of Laser–Oral Tissue Interaction. Dent. J. 2020, 8, 61. [Google Scholar] [CrossRef] [PubMed]
- Luchian, I.; Budală, D.G.; Baciu, E.-R.; Ursu, R.G.; Diaconu-Popa, D.; Butnaru, O.; Tatarciuc, M. The Involvement of Photobiology in Contemporary Dentistry—A Narrative Review. Int. J. Mol. Sci. 2023, 24, 3985. [Google Scholar] [CrossRef] [PubMed]
- Douchy, L.; Gauthier, R.; Abouelleil-Sayed, H.; Colon, P.; Grosgogeat, B.; Bosco, J. The effect of therapeutic radiation on dental enamel and dentin: A systematic review. Dent. Mater. 2022, 38, e181–e201. [Google Scholar] [CrossRef] [PubMed]
- Pion, L.A.; De Matos, L.L.M.; Gimenez, T.; Palma-Dibb, R.G.; Faraoni, J.J. Treatment outcome for dentin hypersensitivity with laser therapy: Systematic review and meta-analysis. Dent. Med. Probl. 2023, 60, 153–166. [Google Scholar] [CrossRef]
- Zhang, Y.; Qian, Y.; Huo, K.; Liu, J.; Huang, X.; Bao, J. Efficacy of laser therapy for temporomandibular disorders: A systematic review and meta-analysis. Complement. Ther. Med. 2023, 74, 102945. [Google Scholar] [CrossRef]
- Sipiyaruk, K.; Chintavalakorn, R.; Saengfai, N. The protocol of low-level laser therapy in orthodontic practice: A scoping review of literature. J. Int. Soc. Prev. Community Dent. 2022, 12, 267–286. [Google Scholar] [CrossRef]
- Olek, M.; Machorowska-Pieniążek, A.; Stós, W.; Kalukin, J.; Bartusik-Aebisher, D.; Aebisher, D.; Cieślar, G.; Kawczyk-Krupka, A. Photodynamic Therapy in Orthodontics: A Literature Review. Pharmaceutics 2021, 13, 720. [Google Scholar] [CrossRef]
- Demirsoy, K.K.; Kurt, G. Use of Laser Systems in Orthodontics. Turk. J. Orthod. 2020, 33, 133–140. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Li, T.; Zhang, X.; Shi, H.; Ma, Z.; Lv, B.; Xie, M. Er:YAG laser application in caries removal and cavity preparation in children: A meta-analysis. Lasers Med. Sci. 2019, 34, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Cattoni, F.; Ferrante, L.; Mandile, S.; Tetè, G.; Polizzi, E.M.; Gastaldi, G. Comparison of Lasers and Desensitizing Agents in Dentinal Hypersensitivity Therapy. Dent. J. 2023, 11, 63. [Google Scholar] [CrossRef] [PubMed]
- Dawdy, J.; Halladay, J.; Carrasco-Labra, A.; Araya, I.; Yanine, N.; Brignardello-Petersen, R. Efficacy of adjuvant laser therapy in reducing postsurgical complications after the removal of impacted mandibular third molars: A systematic review update and meta-analysis. J. Am. Dent. Assoc. 2017, 148, 887–902.e4. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, R.F.; Da Silva, A.C.; Simões, A.; Youssef, M.N.; De Freitas, P.M. Laser Therapy in the Treatment of Paresthesia: A Retrospective Study of 125 Clinical Cases. Photomed. Laser Surg. 2015, 33, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Kavaliauskiene, A.; Smailiene, D.; Buskiene, I.; Keriene, D. Pain and discomfort perception among patients undergoing orthodontic treatment: Results from one month follow-up study. Stomatologija 2012, 14, 118–125. [Google Scholar]
- Erdinç, A.M.E. Perception of pain during orthodontic treatment with fixed appliances. Eur. J. Orthod. 2004, 26, 79–85. [Google Scholar] [CrossRef]
- Rakhshan, H.; Rakhshan, V. Pain and discomfort perceived during the initial stage of active fixed orthodontic treatment. Saudi Dent. J. 2015, 27, 81–87. [Google Scholar] [CrossRef] [Green Version]
- Suter, V.G.A.; Sjölund, S.; Bornstein, M.M. Effect of laser on pain relief and wound healing of recurrent aphthous stomatitis: A systematic review. Lasers Med. Sci. 2017, 32, 953–963. [Google Scholar] [CrossRef]
- Chow, R.T.; Armati, P.J. Photobiomodulation: Implications for Anesthesia and Pain Relief. Photomed. Laser Surg. 2016, 34, 599–609. [Google Scholar] [CrossRef]
- Aggarwal, H. Efficacy of Low-Level Laser Therapy in Treatment of Recurrent Aphthous Ulcers—A Sham Controlled, Split Mouth Follow Up Study. J. Clin. Diagn. Res. 2014, 8, 218–221. [Google Scholar] [CrossRef] [PubMed]
- Lalabonova, H.; Daskalov, H. Clinical assessment of the therapeutic effect of low-level laser therapy on chronic recurrent aphthous stomatitis. Biotechnol. Biotechnol. Equip. 2014, 28, 929–933. [Google Scholar] [CrossRef] [PubMed]
- Parra-Moreno, F.; Egido-Moreno, S.; Schemel-Suárez, M.; González-Navarro, B.; Estrugo-Devesa, A.; López-López, J. Treatment of recurrent aphtous stomatitis: A systematic review. Med. Oral Patol. Oral Cirugía Bucal 2023, 28, e87–e98. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Tan, L.; Fu, G.; Chen, L.; Tan, H. Efficacy of Topical Intervention for Recurrent Aphthous Stomatitis: A Network Meta-Analysis. Medicina 2022, 58, 771. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.K.; Jafer, M.; Nayeem, M.; Moafa, I.H.; Quadri, M.F.A.; Gopalaiah, H. Low-Level Laser Therapy and Topical Medications for Treating Aphthous Ulcers: A Systematic Review. J. Multidiscip. Healthc. 2020, 13, 1595–1605. [Google Scholar] [CrossRef]
- Ngan, P.; Kess, B.; Wilson, S. Perception of discomfort by patients undergoing orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 1989, 96, 47–53. [Google Scholar] [CrossRef]
- Bertolini, A.; Ferrari, A.; Ottani, A.; Guerzoni, S.; Tacchi, R.; Leone, S. Paracetamol: New Vistas of an Old Drug. CNS Drug Rev. 2006, 12, 250–275. [Google Scholar] [CrossRef]
- Brito, M.H.; Nogueira, C.Q.; Cotrin, P.; Fialho, T.; Oliveira, R.C.; Oliveira, R.G.; Salmeron, S.; Valarelli, F.P.; Freitas, K.M.S.; Cançado, R.H. Efficacy of Low-Level Laser Therapy in Reducing Pain in the Initial Stages of Orthodontic Treatment. Int. J. Dent. 2022, 2022, 3934900. [Google Scholar] [CrossRef]
- Zhi, C.; Guo, Z.; Wang, T.; Liu, D.; Duan, X.; Yu, X.; Zhang, C. Viability of Photobiomodulaton Therapy in Decreasing Orthodontic-Related Pain: A Systematic Review and Meta-Analysis. Photobiomodul. Photomed. Laser Surg. 2021, 39, 504–517. [Google Scholar] [CrossRef]
- Camacho, A.D.; Reyes, M.B.; Cujar, S.A.V. A systematic review of the effective laser wavelength range in delivering photobiomodulation for pain relief in active orthodontic treatment. Int. Orthod. 2020, 18, 684–695. [Google Scholar] [CrossRef]
- Cronshaw, M.; Parker, S.; Anagnostaki, E.; Lynch, E. Systematic Review of Orthodontic Treatment Management with Photobiomodulation Therapy. Photobiomodul. Photomed. Laser Surg. 2019, 37, 862–868. [Google Scholar] [CrossRef] [Green Version]
- Cambier, D.; Blom, K.; Witvrouw, E.; Ollevier, G.; De Muynck, M.; Vanderstraeten, G. The Influence of Low Intensity Infrared Laser Irradiation on Conduction Characteristics of Peripheral Nerve: A Randomised, Controlled, Double Blind Study on the Sural Nerve. Lasers Med. Sci. 2000, 15, 195–200. [Google Scholar] [CrossRef]
- Hagiwara, S.; Iwasaka, H.; Okuda, K.; Noguchi, T. GaAlAs (830 nm) low-level laser enhances peripheral endogenous opioid an-algesia in rats. Lasers Surg. Med. 2007, 39, 797–802. [Google Scholar] [CrossRef]
- Farzan, A.; Khaleghi, K. The Effectiveness of Low-Level Laser Therapy in Pain Induced by Orthodontic Separator Placement: A Systematic Review. J. Lasers Med. Sci. 2021, 12, e29. [Google Scholar] [CrossRef] [PubMed]
- Al-Jewair, T.; Farsaii, A. Low-Level Laser Therapy May Reduce Pain Associated with Orthodontic Separator Placement. J. Evid. Based Dent. Pract. 2022, 22, 101752. [Google Scholar] [CrossRef]
- Kaklamanos, E.G.; Makrygiannakis, M.A.; Athanasiou, A.E. Oral Health-Related Quality of Life throughout Treatment with Clear Aligners in Comparison to Conventional Metal Fixed Orthodontic Appliances: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 3537. [Google Scholar] [CrossRef] [PubMed]
- AlShahrani, I.; Togoo, R.A.; Hosmani, J.; Alhaizaey, A. Photobiomodulation in acceleration of orthodontic tooth movement: A systematic review and meta analysis. Complement. Ther. Med. 2019, 47, 102220. [Google Scholar] [CrossRef]
- Huang, T.; Wang, Z.; Li, J. Efficiency of photobiomodulation on accelerating the tooth movement in the alignment phase of orthodontic treatment—A systematic review and meta-analysis. Heliyon 2023, 9, e13220. [Google Scholar] [CrossRef]
- Olmedo-Hernández, O.L.; Mota-Rodríguez, A.N.; Torres-Rosas, R.; Argueta-Figueroa, L. Effect of the photobiomodulation for acceleration of the orthodontic tooth movement: A systematic review and meta-analysis. Lasers Med. Sci. 2022, 37, 2323–2341. [Google Scholar] [CrossRef]
- Yavagal, C.M.; Matondkar, S.P.; Yavagal, P.C. Efficacy of Laser Photobiomodulation in Accelerating Orthodontic Tooth Movement in Children: A Systematic Review with Meta-analysis. Int. J. Clin. Pediatr. Dent. 2021, 14 (Suppl. S1), S94–S100. [Google Scholar] [CrossRef]
- Li, J.; Ge, X.; Guan, H.; Jia, L.; Chang, W.; Ma, W. The Effectiveness of Photobiomodulation on Accelerating Tooth Movement in Orthodontics: A Systematic Review and Meta-Analysis. Photobiomodul. Photomed. Laser Surg. 2021, 39, 232–244. [Google Scholar] [CrossRef] [PubMed]
- Jedliński, M.; Romeo, U.; del Vecchio, A.; Palaia, G.; Galluccio, G. Comparison of the Effects of Photobiomodulation with Different Lasers on Orthodontic Movement and Reduction of the Treatment Time with Fixed Appliances in Novel Scientific Reports: A Systematic Review with Meta-Analysis. Photobiomodul. Photomed. Laser Surg. 2020, 38, 455–465. [Google Scholar] [CrossRef] [PubMed]
- Bakdach, W.M.; Hadad, R. Effectiveness of low-level laser therapy in accelerating the orthodontic tooth movement: A systematic review and meta-analysis. Dent. Med. Probl. 2020, 57, 73–94. [Google Scholar] [CrossRef] [PubMed]
- Ghaffar, Y.K.A.; El Sharaby, F.A.; Negm, I.M. Effect of low-level laser therapy on the time needed for leveling and alignment of mandibular anterior crowding. Angle Orthod. 2022, 92, 478–486. [Google Scholar] [CrossRef]
- Zheng, J.; Yang, K. Clinical research: Low-level laser therapy in accelerating orthodontic tooth movement. BMC Oral Health 2021, 21, 324. [Google Scholar] [CrossRef]
- Bastos, R.T.D.R.M.; Blagitz, M.N.; Aragón, M.L.S.D.C.; Maia, L.C.; Normando, D. Periodontal side effects of rapid and slow maxillary expansion: A systematic review. Angle Orthod. 2019, 89, 651–660. [Google Scholar] [CrossRef] [Green Version]
- Saito, S.; Shimizu, N. Stimulatory effects of low-power laser irradiation on bone regeneration in midpalatal suture during ex-pansion in the rat. Am. J. Orthod. Dentofac. Orthop. 1997, 111, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, A.; Touma, Y.; Ishino, Y.; Tanaka, E.; Aoyama, J.; Hanaoka, K.; Watanabe, M.; Tanne, K. Linear polarized near-infrared irradiation stimulates mechanical expansion of the rat sagittal suture. Luminescence 2003, 18, 58–60. [Google Scholar] [CrossRef]
- Cepera, F.; Torres, F.C.; Scanavini, M.A.; Paranhos, L.R.; Filho, L.C.; Cardoso, M.A.; Siqueira, D.C.; Siqueira, D.F. Effect of a low-level laser on bone regeneration after rapid maxillary expansion. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 444–450. [Google Scholar] [CrossRef]
- Farzan, A.; Khaleghi, K.; Pirayesh, Z. Effect of Low-Level Laser Therapy on Bone Formation in Rapid Palatal Expansion: A Systematic Review. J. Lasers Med. Sci. 2022, 13, e13. [Google Scholar] [CrossRef]
- Lai, P.-S.; Fierro, C.; Bravo, L.; Perez-Flores, A. Benefits of Using Low-level Laser Therapy in the Rapid Maxillary Expansion: A Systematic Review. Int. J. Clin. Pediatr. Dent. 2021, 14 (Suppl. S1), S101–S106. [Google Scholar] [CrossRef]
- Davoudi, A.; Amrolahi, M.; Khaki, H. Effects of laser therapy on patients who underwent rapid maxillary expansion; a systematic review. Lasers Med. Sci. 2018, 33, 1387–1395. [Google Scholar] [CrossRef] [PubMed]
- Albertini, R.; Villaverde, A.; Aimbire, F.; Salgado, M.; Bjordal, J.; Alves, L.; Munin, E.; Costa, M. Anti-inflammatory effects of low-level laser therapy (LLLT) with two different red wavelengths (660 nm and 684 nm) in carrageenan-induced rat paw edema. J. Photochem. Photobiol. B Biol. 2007, 89, 50–55. [Google Scholar] [CrossRef]
- Muniz, X.C.; de Assis, A.C.C.; de Oliveira, B.S.A.; Ferreira, L.F.R.; Bilal, M.; Iqbal, H.M.N.; Soriano, R.N. Efficacy of low-level laser therapy in nerve injury repair—A new era in therapeutic agents and regenerative treatments. Neurol. Sci. 2021, 42, 4029–4043. [Google Scholar] [CrossRef] [PubMed]
- Eshghpour, M.; Ahrari, F.; Takallu, M. Is Low-Level Laser Therapy Effective in the Management of Pain and Swelling After Mandibular Third Molar Surgery? J. Oral Maxillofac. Surg. 2016, 74, 1322.e1–1322.e8. [Google Scholar] [CrossRef] [PubMed]
- Camacho, A.D.; Velásquez, S.A.; Marulanda, N.J.B.; Moreno, M. Photobiomodulation as oedema adjuvant in post-orthognathic surgery patients: A randomized clinical trial. Int. Orthod. 2020, 18, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Feslihan, E.; Eroğlu, C.N. Can Photobiomodulation Therapy Be an Alternative to Methylprednisolone in Reducing Pain, Swelling, and Trismus After Removal of Impacted Third Molars? Photobiomodul. Photomed. Laser Surg. 2019, 37, 700–705. [Google Scholar] [CrossRef]
- de Barros, D.D.; Catão, J.S.d.S.B.; Ferreira, A.C.D.; Simões, T.M.S.; Almeida, R.D.A.C.; Catão, M.H.C.D.V. Low-level laser therapy is effective in controlling postoperative pain in lower third molar extractions: A systematic review and meta-analysis. Lasers Med. Sci. 2022, 37, 2363–2377, Erratum in Lasers Med. Sci. 2022. [Google Scholar] [CrossRef]
- de Oliveira, F.J.D.; Brasil, G.M.L.C.; Soares, G.P.A.; Paiva, D.F.F.; Júnior, F.D.A.D.S. Use of low-level laser therapy to reduce postoperative pain, edema, and trismus following third molar surgery: A systematic review and meta-analysis. J. Cranio-Maxillofac. Surg. 2021, 49, 1088–1096. [Google Scholar] [CrossRef]
- Hakimiha, N.; Bassir, S.H.; Romanos, G.E.; Shamshiri, A.R.; Moslemi, N. Efficacy of photobiomodulation therapy on neurosensory recovery in patients with inferior alveolar nerve injury following oral surgical procedures: A systematic review. Quintessence Int. 2021, 52, 140–153. [Google Scholar] [CrossRef]
- Hosseinpour, S.; Tunér, J.; Fekrazad, R. Photobiomodulation in Oral Surgery: A Review. Photobiomodul. Photomed. Laser Surg. 2019, 37, 814–825. [Google Scholar] [CrossRef] [Green Version]
- Ren, Y.; Jongsma, M.A.; Mei, L.; Van Der Mei, H.C.; Busscher, H.J. Orthodontic treatment with fixed appliances and biofilm formation—A potential public health threat? Clin. Oral Investig. 2014, 18, 1711–1718. [Google Scholar] [CrossRef]
- Ozog, D.M.; Rkein, A.M.; Fabi, S.G.; Gold, M.H.; Goldman, M.P.; Lowe, N.J.; Martin, G.M.; Munavalli, G.S. Photodynamic Therapy: A Clinical Consensus Guide. Dermatol. Surg. 2016, 42, 804–827, Erratum in Dermatol. Surg. 2017, 43, 319. [Google Scholar] [CrossRef]
- Baeshen, H.A.; Alshahrani, A.; Kamran, M.A.; Alnazeh, A.A.; Alhaizaey, A.; Alshahrani, I. Effectiveness of antimicrobial photodynamic therapy in restoring clinical, microbial, proinflammatory cytokines and pain scores in adolescent patients having generalized gingivitis and undergoing fixed orthodontic treatment. Photodiagn. Photodyn. Ther. 2020, 32, 101998. [Google Scholar] [CrossRef]
- Alshahrani, A.A.; Alhaizaey, A.; Kamran, M.A.; Alshahrani, I. Efficacy of antimicrobial photodynamic therapy against halitosis in adolescent patients undergoing orthodontic treatment. Photodiagn. Photodyn. Ther. 2020, 32, 102019. [Google Scholar] [CrossRef] [PubMed]
- Eduardo, C.D.P.; Aranha, A.C.C.; Simões, A.; Bello-Silva, M.S.; Ramalho, K.M.; Esteves-Oliveira, M.; de Freitas, P.M.; Marotti, J.; Tunér, J. Laser treatment of recurrent herpes labialis: A literature review. Lasers Med. Sci. 2014, 29, 1517–1529. [Google Scholar] [CrossRef]
- Zanella, P.A.; Onuchic, L.F.; Watanabe, E.H.; Azevedo, L.H.; Aranha, A.C.C.; Ramalho, K.M.; Eduardo, C.D.P. Photobiomodulation for Preventive Therapy of Recurrent Herpes Labialis: A 2-Year In Vivo Randomized Controlled Study. Photobiomodul. Photomed. Laser Surg. 2022, 40, 682–690. [Google Scholar] [CrossRef] [PubMed]
- Woźniak, A.; Matys, J.; Grzech-Leśniak, K. Effectiveness of lasers and aPDT in elimination of intraoral halitosis: A systematic review based on clinical trials. Lasers Med. Sci. 2022, 37, 3403–3411. [Google Scholar] [CrossRef]
- Ferrisse, T.M.; Dias, L.M.; de Oliveira, A.B.; Jordão, C.C.; Mima, E.G.D.O.; Pavarina, A.C. Efficacy of curcumin-mediated antibacterial photodynamic therapy for oral antisepsis: A systematic review and network meta-analysis of randomized clinical trials. Photodiagn. Photodyn. Ther. 2022, 39, 102876. [Google Scholar] [CrossRef] [PubMed]
- Sales, L.S.; Miranda, M.L.; de Oliveira, A.B.; Ferrisse, T.M.; Fontana, C.R.; Milward, M.; Brighenti, F.L. Effect of the technique of photodynamic therapy against the main microorganisms responsible for periodontitis: A systematic review of in-vitro studies. Arch. Oral Biol. 2022, 138, 105425. [Google Scholar] [CrossRef]
- Al-Shammery, D.; Michelogiannakis, D.; Ahmed, Z.U.; Ahmed, H.B.; Rossouw, P.E.; Romanos, G.E.; Javed, F. Scope of antimicrobial photodynamic therapy in Orthodontics and related research: A review. Photodiagn. Photodyn. Ther. 2019, 25, 456–459. [Google Scholar] [CrossRef]
- Ahmed, A.; Fida, M.; Javed, F.; Maaz, M.; Ali, U.S. Soft tissue lasers: An innovative tool enhancing treatment outcomes in orthodontics—A narrative review. J. Pak. Med. Assoc. 2023, 73, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Sarver, D.M. Use of the 810 nm diode laser: Soft tissue management and orthodontic applications of innovative technology. Pract. Proced. Aesthetic Dent. PPAD 2006, 18, suppl 7–13. [Google Scholar]
- Inchingolo, A.M.; Malcangi, G.; Ferrara, I.; Viapiano, F.; Netti, A.; Buongiorno, S.; Latini, G.; Azzollini, D.; De Leonardis, N.; de Ruvo, E.; et al. Laser Surgical Approach of Upper Labial Frenulum: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 1302. [Google Scholar] [CrossRef] [PubMed]
- Sadiq, M.S.K.; Maqsood, A.; Akhter, F.; Alam, M.K.; Abbasi, M.S.; Minallah, S.; Vohra, F.; Alswairki, H.J.; Abutayyem, H.; Mussallam, S.; et al. The Effectiveness of Lasers in Treatment of Oral Mucocele in Pediatric Patients: A Systematic Review. Materials 2022, 15, 2452. [Google Scholar] [CrossRef]
- Khosraviani, F.; Ehsani, S.; Fathi, M.; Saberi-Demneh, A. Therapeutic effect of laser on pediatric oral soft tissue problems: A systematic literature review. Lasers Med. Sci. 2019, 34, 1735–1746. [Google Scholar] [CrossRef]
- Bornstein, E.S.; Lomke, M.A. The safety and effectiveness of dental Er:YAG lasers. A literature review with specific reference to bone. Dent. Today 2003, 22, 129–133. [Google Scholar] [PubMed]
- Ahn, J.H.; Power, S.; Thickett, E. Application of the diode laser for soft-tissue surgery in orthodontics: Case series. J. Orthod. 2021, 48, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Dumbryte, I.; Vebriene, J.; Linkeviciene, L.; Malinauskas, M. Enamel microcracks in the form of tooth damage during orthodontic debonding: A systematic review and meta-analysis of in vitro studies. Eur. J. Orthod. 2018, 40, 636–648. [Google Scholar] [CrossRef]
- Ghazanfari, R.; Nokhbatolfoghahaei, H.; Alikhasi, M. Laser-Aided Ceramic Bracket Debonding: A Comprehensive Review. J. Lasers Med. Sci. 2016, 7, 2–11. [Google Scholar] [CrossRef]
- Stein, S.; Wenzler, J.; Hellak, A.; Schauseil, M.; Korbmacher-Steiner, H.; Braun, A. Intrapulpal Temperature Increases Caused by 445-nm Diode Laser-Assisted Debonding of Self-Ligating Ceramic Brackets During Simulated Pulpal Fluid Circulation. Photomed. Laser Surg. 2018, 36, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Hoteit, M.; Nammour, S.; Zeinoun, T. Evaluation of Enamel Topography after Debonding Orthodontic Ceramic Brackets by Different Er,Cr:YSGG and Er:YAG Lasers Settings. Dent. J. 2020, 8, 6. [Google Scholar] [CrossRef] [Green Version]
- Mesaroș, A.; Mesaroș, M.; Buduru, S. Orthodontic Bracket Removal Using LASER-Technology—A Short Systematic Literature Review of the Past 30 Years. Materials 2022, 15, 548. [Google Scholar] [CrossRef]
- Ajwa, N.; Alfayez, H.; Al-Oqab, H.; Melibary, R.; Alzamil, Y. The Effect of Erbium-Doped Yttrium Aluminum Garnet Laser in Debonding of Orthodontic Brackets: A Systematic Review of the Literature. Photobiomodul. Photomed. Laser Surg. 2021, 39, 725–733. [Google Scholar] [CrossRef]
- Francisco, I.; Travassos, R.; Nunes, C.; Ribeiro, M.; Marques, F.; Pereira, F.; Marto, C.M.; Carrilho, E.; Oliveiros, B.; Paula, A.B.; et al. What Is the Most Effective Technique for Bonding Brackets on Ceramic—A Systematic Review and Meta-Analysis. Bioengineering 2022, 9, 14. [Google Scholar] [CrossRef]
- Zein, R.; Selting, W.; Hamblin, M.R. Review of light parameters and photobiomodulation efficacy: Dive into complexity. J. Biomed. Opt. 2018, 23, 120901. [Google Scholar] [CrossRef] [Green Version]
- Parker, S.; Cronshaw, M.; Anagnostaki, E.; Bordin-Aykroyd, S.R.; Lynch, E. Systematic Review of Delivery Parameters Used in Dental Photobiomodulation Therapy. Photobiomodul. Photomed. Laser Surg. 2019, 37, 784–797. [Google Scholar] [CrossRef]
- Franco, W.F.; Galdino, M.V.B.; Capeletti, L.R.; Sberowsky, B.H.; Vieira, R.A.; Figueiredo, A.C.; Ramalho, K.M.; dos Santos, F.C.A.; Biancardi, M.F.; de Marco, J.P.; et al. Photobiomodulation and Mandibular Advancement Modulates Cartilage Thickness and Matrix Deposition in the Mandibular Condyle. Photobiomodul. Photomed. Laser Surg. 2020, 38, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Sobouti, F.; Chiniforush, N.; Saravani, H.J.; Noroozian, M.; Cronshaw, M.; Navaei, R.A.; Rakhshan, V.; Dadgar, S. Efficacy of compound topical anesthesia combined with photobiomodulation therapy in pain control for placement of orthodontic miniscrew: A double-blind, randomized clinical trial. Lasers Med. Sci. 2022, 37, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Razaghi, P.; Haghgou, J.M.; Khazaei, S.; Farhadian, N.; Fekrazad, R.; Gholami, L. The Effect of Photobiomodulation Therapy on the Stability of Orthodontic Mini-implants in Human and Animal Studies: A Systematic Review and Meta-analysis. J. Lasers Med. Sci. 2022, 13, e27. [Google Scholar] [CrossRef] [PubMed]
- Nayyer, N.; Tripathi, T.; Ganesh, G.; Rai, P. Impact of photobiomodulation on external root resorption during orthodontic tooth movement in humans—A systematic review and meta-analysis. J. Oral Biol. Craniofacial Res. 2022, 12, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Jahanbin, A.; Ramazanzadeh, B.; Ahrari, F.; Forouzanfar, A.; Beidokhti, M. Effectiveness of Er:YAG laser-aided fiberotomy and low-level laser therapy in alleviating relapse of rotated incisors. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Miresmæili, A.F.; Mollabashi, V.; Gholami, L.; Farhadian, M.; Rezaei-Soufi, L.; Javanshir, B.; Malekshoar, M. Comparison of conventional and laser-aided fiberotomy in relapse tendency of rotated tooth: A randomized controlled clinical trial. Int. Orthod. 2019, 17, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Salehi, P.; Heidari, S.; Tanideh, N.; Torkan, S. Effect of low-level laser irradiation on the rate and short-term stability of rotational tooth movement in dogs. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 578–586. [Google Scholar] [CrossRef]
- Amasyalİ, M.; Sabuncuoglu, F.A.; Ersahan, S.; Oktay, E.A. Comparison of the Effects of Various Methods Used to Remove Adhesive from Tooth Surfaces on Surface Roughness and Temperature Changes in the Pulp Chamber. Turk. J. Orthod. 2019, 32, 132–138. [Google Scholar] [CrossRef]
- Lizarelli, R.d.F.; Moriyama, L.T.; Bagnato, V.S. Ablation of composite resins using Er:YAG laser—Comparison with enamel and dentin. Lasers Surg. Med. 2003, 33, 132–139. [Google Scholar] [CrossRef]
- Grocholewicz, K.; Janiszewska-Olszowska, J.; Szatkiewicz, T.; Tomkowski, R.; Tandecka, K. Effect of Orthodontic Debonding and Adhesive Removal on the Enamel—Current Knowledge and Future Perspectives—A Systematic Review. Med. Sci. Monit. 2014, 20, 1991–2001. [Google Scholar] [CrossRef] [Green Version]
- Weber, M.H.; Fußgänger-May, T.; Wolf, T. The intravenous laser blood irradiation. Introduction of a new therapy. Ger. J. Acupunct. Relat. Tech. 2007, 50, 12–23. [Google Scholar]
- da Silva, L.A.; Pinheiro, S.L. Clinical Evaluation of Intravascular Blood Irradiation with Laser, Photobiomodulation, and Photodynamic Therapy in Cancer Patients with Mucositis. Photobiomodul. Photomed. Laser Surg. 2021, 39, 687–695. [Google Scholar] [CrossRef]
- Rangel, C.R.G.; Pinheiro, S.L. Laser acupuncture and intravascular laser irradiation of blood for management of pediatric dental anxiety. J. Oral Sci. 2021, 63, 355–357. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| INDICATIONS vs. PARAMETERS | Source of Light | Wavelenght (nm) | Power (mW) | Energy (J/point) | Energy Density (J/cm2) | Exposure Durantion (s/point) | Points of Irradiation | Frequency of Irradiation | Main Outcome | Novel Systematic Reviews |
|---|---|---|---|---|---|---|---|---|---|---|
| Traumatic Ulcers | Diode | 658–980 | 27–2000 | 0.2–1 | 3–110.67 | 5–180 | Over and around the ulcers | Single or daily until complete healing | Pain relief, faster healing | 23–25 |
| Post-Activation Pain | Diode | 780–980 | 20–300 | 0.2–8 | 2.25–189 | 5–60 | Along the periodontium, buccally | Single | Pain relief | 29–31, 34, 35 |
| Orthodontic Tooth Movement | Diode | 810–980 | 20–200 | 0.2–2.3 | 5–216 | 20–40 | Along the periodontium, buccal and ligually | Day 0, 3, 7, 14, every 15 days | Accelerated tooth movement, reduced treatment time | 31, 37–43 |
| Rapid Maxillary Expansion | Diode | 780–830 | 10–100 | 0.1–2 | 10–140 | 10–84 | 4–10 distributed to the palatum | Once a week to daily during activation; weekly during retention | Accelerated bone repair | 50–52 |
| Post-Operative Care | Diode | 660–980 | 100–300 | * | * | * | * | * | Pain relief, edema reduction, faster healing | 58–61 |
| Infeccted Lesions | Diode; CO2; Nd:YAG; Er:YAG; Er,Cr:YSGG | * | * | * | * | * | Over the lesion | Single or multiple (if necessary) | (aPDT/HILT) Desinfection, faster healing | 9, 68–76 |
| Soft Tissue Surgeries | Diode; CO2; Nd:YAG; Er:YAG; Er,Cr:YSGG | * | * | * | * | * | * | Single | Better homeostasis, reduction of operation time and post-operative complications, faster healing | 72–76 |
| Bracket Removal | Diode; CO2; Nd:YAG; Er,Cr:YSGG | 445–10,600 | * | * | * | * | Around metalic brackets; sweeping ceramic bracket surface | Single | Bracket debonding | 82–85 |
| Er:YAG | 2940 | 2.5–5 | 0.125–0.6 | 4–8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dantas, C.M.G.; Vivan, C.L.; Dominguez, G.C.; de Fantini, S.M.; de Freitas, P.M. Light in Orthodontics: Applications of High-Intensity Lasers, Photobiomodulation, and Antimicrobial Photodymanic Therapies in Daily Practice. Photonics 2023, 10, 689. https://doi.org/10.3390/photonics10060689
Dantas CMG, Vivan CL, Dominguez GC, de Fantini SM, de Freitas PM. Light in Orthodontics: Applications of High-Intensity Lasers, Photobiomodulation, and Antimicrobial Photodymanic Therapies in Daily Practice. Photonics. 2023; 10(6):689. https://doi.org/10.3390/photonics10060689
Chicago/Turabian StyleDantas, Caroline Maria Gomes, Carolina Lapaz Vivan, Gladys Cristina Dominguez, Solange Mongelli de Fantini, and Patricia Moreira de Freitas. 2023. "Light in Orthodontics: Applications of High-Intensity Lasers, Photobiomodulation, and Antimicrobial Photodymanic Therapies in Daily Practice" Photonics 10, no. 6: 689. https://doi.org/10.3390/photonics10060689