Predictive Model of the Effects of Skin Phototype and Body Mass Index on Photobiomodulation Therapy for Orofacial Disorders




Abstract
1. Introduction
2. Materials and Methods
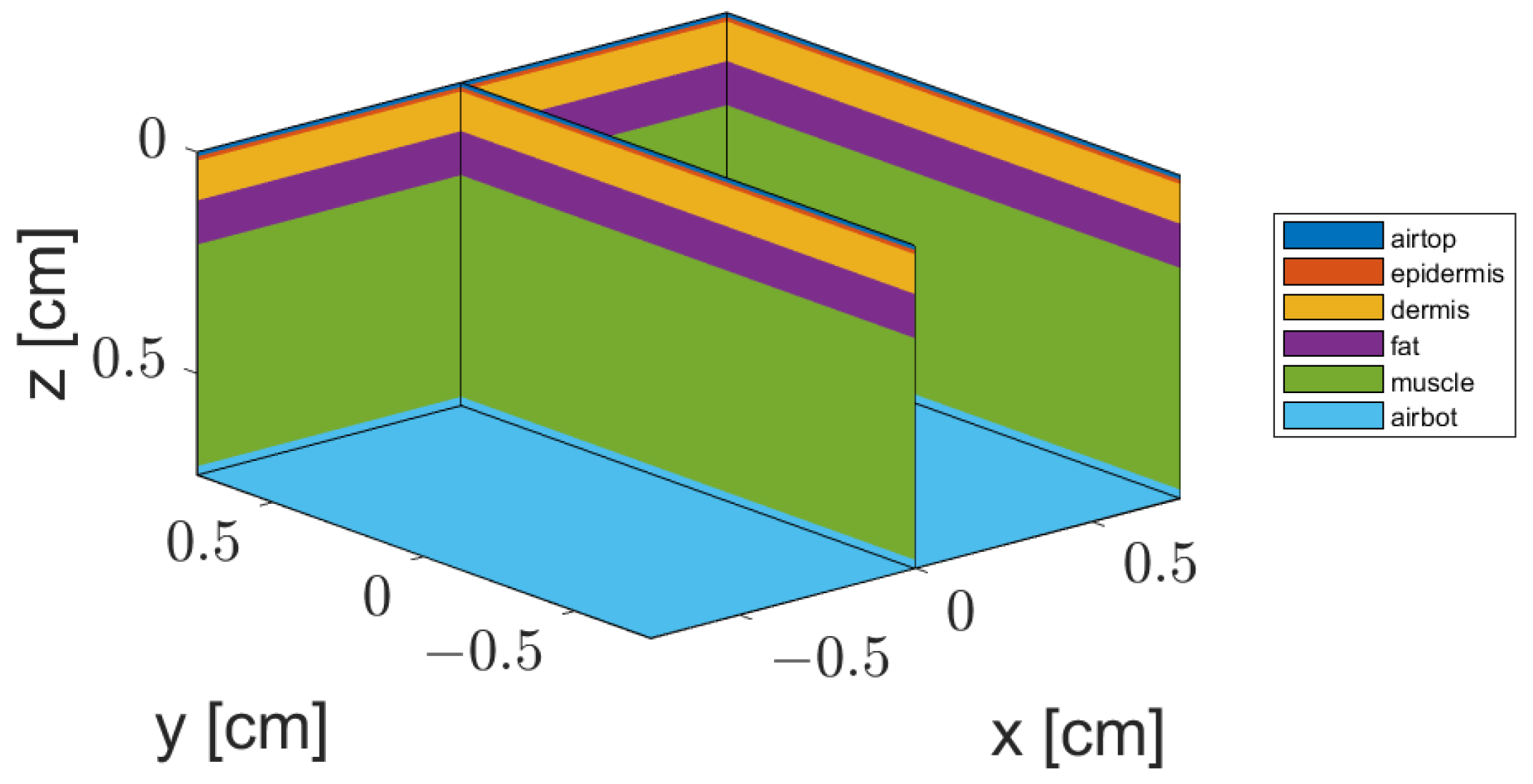
2.1. Tissue Structure and Optical Properties
2.1.1. Skin Thickness
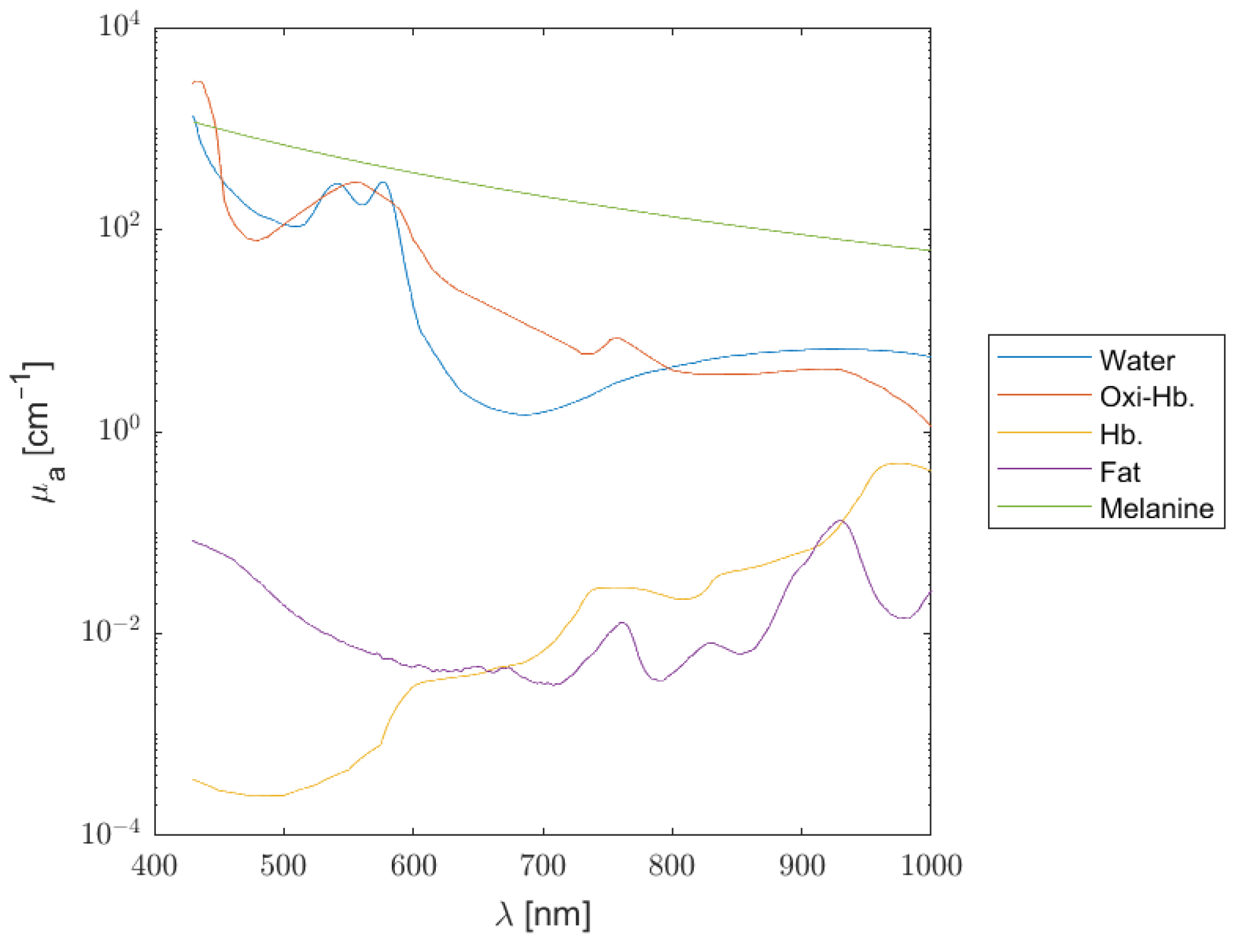
2.1.2. Absorption Coefficient
2.1.3. Scattering, Anisotropy, and Refractive Index
2.2. Monte Carlo Model
Data Set
2.3. Predictive Model of Average Dose
2.3.1. Design of the Predictive Model
2.3.2. Validation and Testing
3. Results
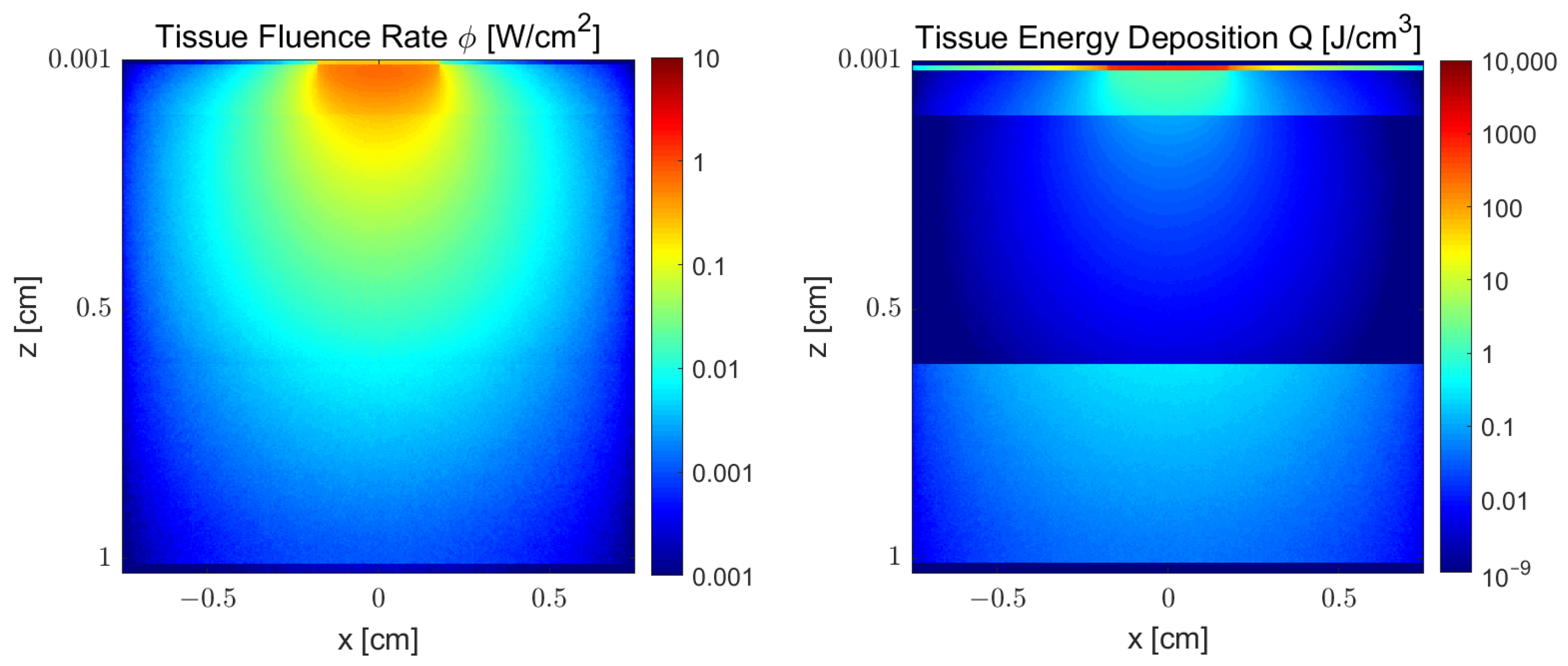
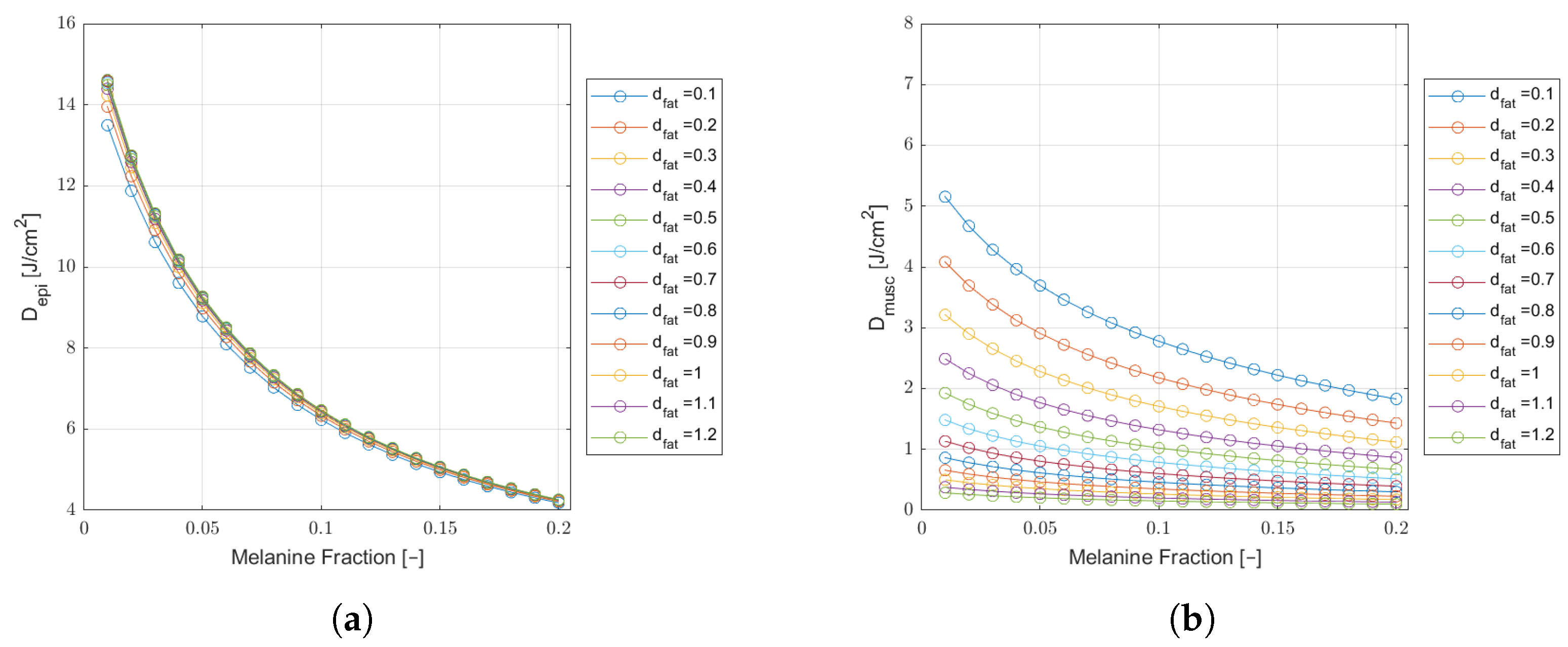
3.1. Monte Carlo Simulation Results
3.2. Predictive Model Results
3.2.1. Performance Assessment
3.2.2. Predicting the Treatment Duration
4. Discussion and Outlook
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Farshidfar, N.; Farzinnia, G.; Samiraninezhad, N.; Assar, S.; Firoozi, P.; Rezazadeh, F.; Hakimiha, N. The Effect of Photobiomodulation on Temporomandibular Pain and Functions in Patients with Temporomandibular Disorders: An Updated Systematic Review of the Current Randomized Controlled Trials: Photobiomodulation in temporomandibular disorders. J. Lasers Med. Sci. 2023, 14, e24. [Google Scholar] [CrossRef] [PubMed]
- Cronshaw, M.; Parker, S.; Anagnostaki, E.; Mylona, V.; Lynch, E.; Grootveld, M. Photobiomodulation and oral mucositis: A systematic review. Dent. J. 2020, 8, 87. [Google Scholar] [CrossRef] [PubMed]
- Glass, G.E. Photobiomodulation: The clinical applications of low-level light therapy. Aesthetic Surg. J. 2021, 41, 723–738. [Google Scholar] [CrossRef] [PubMed]
- Dompe, C.; Moncrieff, L.; Matys, J.; Grzech-Leśniak, K.; Kocherova, I.; Bryja, A.; Bruska, M.; Dominiak, M.; Mozdziak, P.; Skiba, T.H.I.; et al. Photobiomodulation—Underlying mechanism and clinical applications. J. Clin. Med. 2020, 9, 1724. [Google Scholar] [CrossRef]
- Treister, N.S.; London, W.B.; Guo, D.; Malsch, M.; Verrill, K.; Brewer, J.; Margossian, S.; Duncan, C. A feasibility study evaluating extraoral photobiomodulation therapy for prevention of mucositis in pediatric hematopoietic cell transplantation. Photomed. Laser Surg. 2016, 34, 178–184. [Google Scholar] [CrossRef]
- Fitzpatrick, T.B. The validity and practicality of sun-reactive skin types I through VI. Arch. Dermatol. 1988, 124, 869–871. [Google Scholar] [CrossRef]
- Jeong, K.M.; Seo, J.Y.; Kim, A.; Kim, Y.C.; Baek, Y.S.; Oh, C.H.; Jeon, J. Ultrasonographic analysis of facial skin thickness in relation to age, site, sex, and body mass index. Ski. Res. Technol. 2023, 29, e13426. [Google Scholar] [CrossRef]
- Liao, Y.H.; Chen, S.Y.; Chou, S.Y.; Wang, P.H.; Tsai, M.R.; Sun, C.K. Determination of chronological aging parameters in epidermal keratinocytes by in vivo harmonic generation microscopy. Biomed. Opt. Express 2012, 4, 77–88. [Google Scholar] [CrossRef]
- Kobayashi, R.; Haga, S.; Umehara, A.; Takakaze, M.; Akatsuka, K.; Nakano, H. Quantitative and qualitative evaluation of the masseter muscle by ultrasonography and correlation with whole body health status. J. Phys. Ther. Sci. 2024, 36, 136–141. [Google Scholar] [CrossRef]
- Flock, S.T.; Patterson, M.S.; Wilson, B.C.; Wyman, D.R. Monte Carlo modeling of light propagation in highly scattering tissues. I. Model predictions and comparison with diffusion theory. IEEE Trans. Biomed. Eng. 1989, 36, 1162–1168. [Google Scholar] [CrossRef]
- Boonya-Ananta, T.; Rodriguez, A.J.; Du Le, V.; Ramella-Roman, J.C. Monte Carlo analysis of optical heart rate sensors in commercial wearables: The effect of skin tone and obesity on the photoplethysmography (PPG) signal. Biomed. Opt. Express 2021, 12, 7445–7457. [Google Scholar] [CrossRef]
- Souza-Barros, L.; Dhaidan, G.; Maunula, M.; Solomon, V.; Gabison, S.; Lilge, L.; Nussbaum, E.L. Skin color and tissue thickness effects on transmittance, reflectance, and skin temperature when using 635 and 808 nm lasers in low intensity therapeutics. Lasers Surg. Med. 2018, 50, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Yaroslavsky, A.N.; Juliano, A.F.; Adnan, A.; Selting, W.J.; Iorizzo, T.W.; Carroll, J.D.; Sonis, S.T.; Duncan, C.N.; London, W.B.; Treister, N.S. Validation of a monte carlo modelling based dosimetry of extraoral photobiomodulation. Diagnostics 2021, 11, 2207. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.Y.; Chen, A.C.H.; Carroll, J.D.; Hamblin, M.R. Biphasic dose response in low level light therapy. Dose-Response 2009, 7. [Google Scholar] [CrossRef] [PubMed]
- ANSI Z136.1—2007; American National Standard for Safe Use of Lasers. Laser Institute of America: Orlando, FL, USA, 2007.
- Weersink, R.; White, R.; Lilge, L. Light dosimetry for low-level laser therapy: Accounting for differences in tissue and depth. In Proceedings of the Mechanisms for Low-Light Therapy II, San Jose, CA, USA, 21 January 2007; SPIE: Bellingham, DC, USA, 2007; Volume 6428, pp. 23–30. [Google Scholar]
- Yaroslavsky, A.N.; Iorizzo, T.W.; Juliano, A.F.; Adnan, A.; Carroll, J.D.; Sonis, S.T.; Duncan, C.N.; London, W.B.; Treister, N.S. Monte Carlo based dosimetry of extraoral photobiomodulation for prevention of oral mucositis. Sci. Rep. 2023, 13, 20425. [Google Scholar] [CrossRef]
- Jacques, S.L. Optical properties of biological tissues: A review. Phys. Med. Biol. 2013, 58, R37. [Google Scholar] [CrossRef]
- Colas, V.; Blondel, W.; Khairallah, G.; Daul, C.; Amouroux, M. Proposal for a skin layer-wise decomposition model of spatially-resolved diffuse reflectance spectra based on maximum depth photon distributions: A numerical study. Photonics 2021, 8, 444. [Google Scholar] [CrossRef]
- Karsten, A.E.; Smit, J.E. Modeling and verification of melanin concentration on human skin type. Photochem. Photobiol. 2012, 88, 469–474. [Google Scholar] [CrossRef]
- Saager, R.B.; Balu, M.; Crosignani, V.; Sharif, A.; Durkin, A.J.; Kelly, K.M.; Tromberg, B.J. In vivo measurements of cutaneous melanin across spatial scales: Using multiphoton microscopy and spatial frequency domain spectroscopy. J. Biomed. Opt. 2015, 20, 066005. [Google Scholar] [CrossRef]
- Salomatina, E.; Jiang, B.; Novak, J.; Yaroslavsky, A.N. Optical properties of normal and cancerous human skin in the visible and near-infrared spectral range. J. Biomed. Opt. 2006, 11, 064026. [Google Scholar] [CrossRef]
- Simpson, C.R.; Kohl, M.; Essenpreis, M.; Cope, M. Near-infrared optical properties of ex vivo human skin and subcutaneous tissues measured using the Monte Carlo inversion technique. Phys. Med. Biol. 1998, 43, 2465. [Google Scholar] [CrossRef] [PubMed]
- Bashkatov, A.N.; Genina, E.A.; Tuchin, V.V. Optical properties of skin, subcutaneous, and muscle tissues: A review. J. Innov. Opt. Health Sci. 2011, 4, 9–38. [Google Scholar] [CrossRef]
- Tran, A.P.; Jacques, S.L. Modeling voxel-based Monte Carlo light transport with curved and oblique boundary surfaces. J. Biomed. Opt. 2020, 25, 2. [Google Scholar] [CrossRef] [PubMed]
- Marti, D.; Aasbjerg, R.N.; Andersen, P.E.; Hansen, A.K. MCmatlab: An open-source, user-friendly, MATLAB-integrated three-dimensional Monte Carlo light transport solver with heat diffusion and tissue damage. J. Biomed. Opt. 2018, 23, 1. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Feng, Z.; Wang, P.; Song, Y.; Wang, H.; Jin, Z.; Xiong, D. Photobiomodulation for knee osteoarthritis: A model-based dosimetry study. Biomed. Opt. Express 2023, 14, 1800–1817. [Google Scholar] [CrossRef]
- Schuler, S.; Campos, M.; Lacerda, A.; Mazzoni, A.; Silva, T.; Silva, F.; Martins, M.; Fernandes, K.; Fonseca, E.; Mesquita-Ferrari, R.; et al. Dosimetry model for photobiomodulation based on anthropometric and hemodynamic variables in patients with orofacial pain post-Covid-19: Study protocol for randomized clinical trial. PLoS ONE 2024, 19, e0309073. [Google Scholar] [CrossRef]
- Almeida-Lopes, L.; Rigau, J.; Amaro Zângaro, R.; Guidugli-Neto, J.; Marques Jaeger, M.M. Comparison of the low level laser therapy effects on cultured human gingival fibroblasts proliferation using different irradiance and same fluence. Lasers Surg. Med. Off. J. Am. Soc. Laser Med. Surg. 2001, 29, 179–184. [Google Scholar] [CrossRef]
- de Lima Luna, C.A.; Guimarães, D.M.; e Silva, E.S.; do Couto, M.F.N.; Oliveira, G.L.; Alves, M.S.A.; Brazão-Silva, M.T.; de Andrade Hage, C. Photobiomodulation in the treatment of oral diseases. Res. Soc. Dev. 2023, 12, e9512338070. [Google Scholar] [CrossRef]
- de França, A.; Borges, A.G.; Daitx, R.B.; Ferrer, R.M.; Dohnert, M.B.; Durigan, J.L.Q. Photobiomodulation in Temporomandibular Dysfunction: A Systematic Review. Muscles Ligaments Tendons J. 2021, 11, 463. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Layer | d (mm) | HbO2 (µM) | Hb (µM) | W | F | M |
|---|---|---|---|---|---|---|
| Epidermis | 0.1 | 0 | 0 | 0.60 | 0.15 | 0.01–0.20 |
| Dermis | 1.0 | 2.87 | 1.83 | 0.60 | 0.17 | 0 |
| Fat | 0–12 | 0 | 0 | 0.05 | 0.75 | 0 |
| Muscle | 2–8 | 0.50 | 0.50 | 0.70 | 0 | 0 |
| Layer | a (cm−1) | b | g | n |
|---|---|---|---|---|
| Epidermis | 68.7 | 1.161 | 1.4 | |
| Dermis | 45.3 | 1.292 | 1.4 | |
| Fat | 18.4 | 0.672 | 1.34 | |
| Muscle | 11.6 | 1.045 | 1.4 |
| Phototype | M | (cm−1) | (cm−1) |
|---|---|---|---|
| I | 0.05 | 13.1 | 6.5 |
| II | 0.06 | 15.7 | 7.8 |
| III | 0.07 | 18.3 | 9.1 |
| IV | 0.09 | 23.6 | 11.7 |
| V | 0.11 | 28.8 | 14.3 |
| VI | 0.15 | 39.3 | 19.4 |
| Response Variable | RMSE660 | MAE660 | RMSE808 | MAE808 | ||||
|---|---|---|---|---|---|---|---|---|
| Val. | Test | Val. | Test | Val. | Test | Val. | Test | |
| Epidermis | 0.0075 | 0.0072 | 0.0063 | 0.0059 | 0.0032 | 0.0032 | 0.0026 | 0.0026 |
| Muscle | 0.0059 | 0.0059 | 0.0049 | 0.0049 | 0.0032 | 0.0028 | 0.0026 | 0.0023 |
(J/cm2) | (min) | (J/cm2) | (min) | |
|---|---|---|---|---|
| 0.1 | ||||
| 0.3 | ||||
| 0.5 | ||||
| 0.7 | ||||
| 0.9 | ||||
| 1.1 |
| Phot. | M | (J/cm2) | (min) | (J/cm2) | (min) |
|---|---|---|---|---|---|
| I | 0.05 | ||||
| II | 0.06 | ||||
| III | 0.07 | ||||
| IV | 0.09 | ||||
| V | 0.11 | ||||
| VI | 0.15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cassemiro, A.; Motta, L.J.; Fiadeiro, P.; Fonseca, E. Predictive Model of the Effects of Skin Phototype and Body Mass Index on Photobiomodulation Therapy for Orofacial Disorders. Photonics 2024, 11, 1038. https://doi.org/10.3390/photonics11111038
Cassemiro A, Motta LJ, Fiadeiro P, Fonseca E. Predictive Model of the Effects of Skin Phototype and Body Mass Index on Photobiomodulation Therapy for Orofacial Disorders. Photonics. 2024; 11(11):1038. https://doi.org/10.3390/photonics11111038
Chicago/Turabian StyleCassemiro, Alice, Lara Jansiski Motta, Paulo Fiadeiro, and Elsa Fonseca. 2024. "Predictive Model of the Effects of Skin Phototype and Body Mass Index on Photobiomodulation Therapy for Orofacial Disorders" Photonics 11, no. 11: 1038. https://doi.org/10.3390/photonics11111038
APA StyleCassemiro, A., Motta, L. J., Fiadeiro, P., & Fonseca, E. (2024). Predictive Model of the Effects of Skin Phototype and Body Mass Index on Photobiomodulation Therapy for Orofacial Disorders. Photonics, 11(11), 1038. https://doi.org/10.3390/photonics11111038