Efficacy of Photodynamic Inactivation against the Major Human Antibiotic-Resistant Uropathogens

 ,
,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
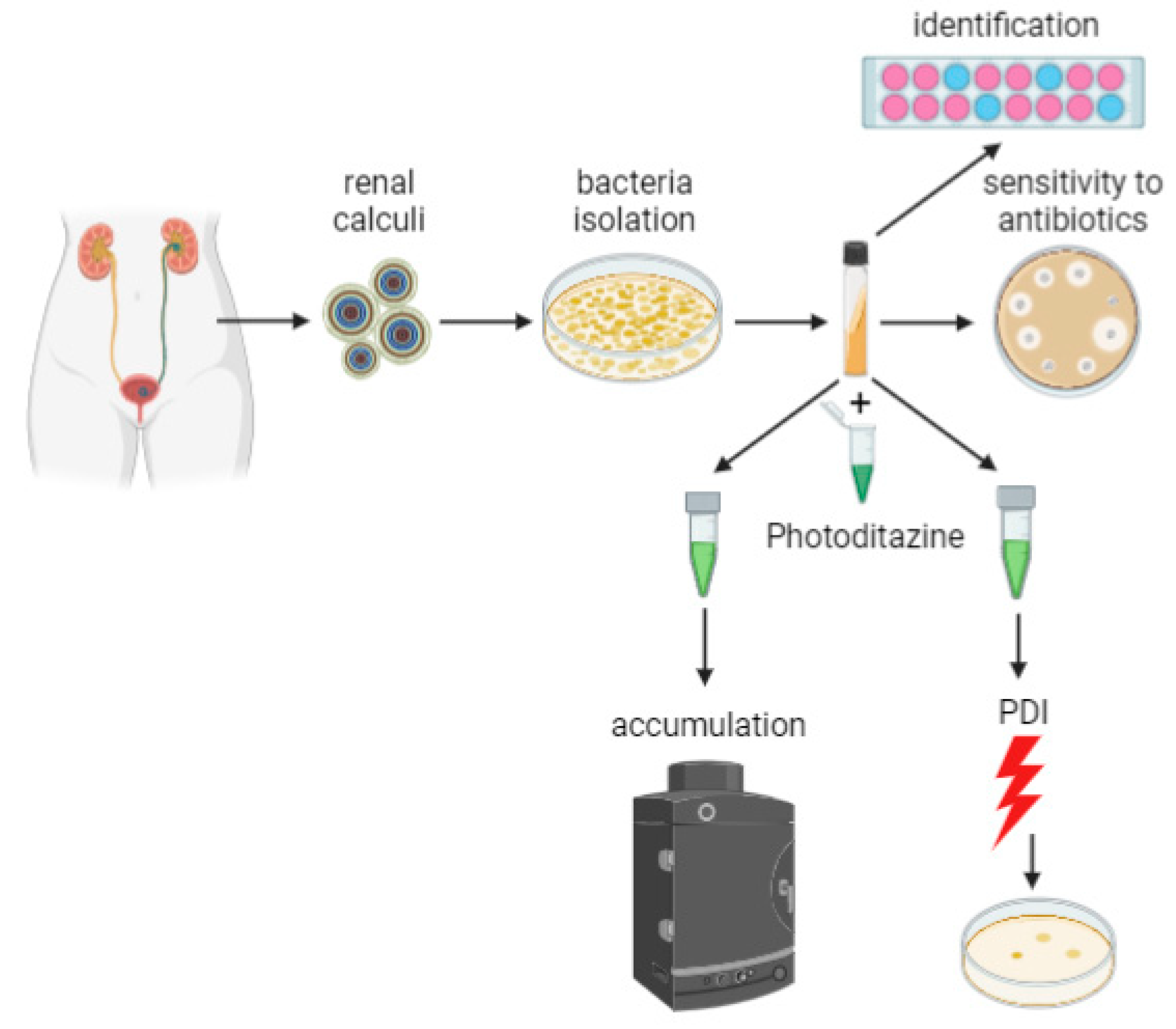
2.1. Isolation and Identification of Pathogenic Microorganisms
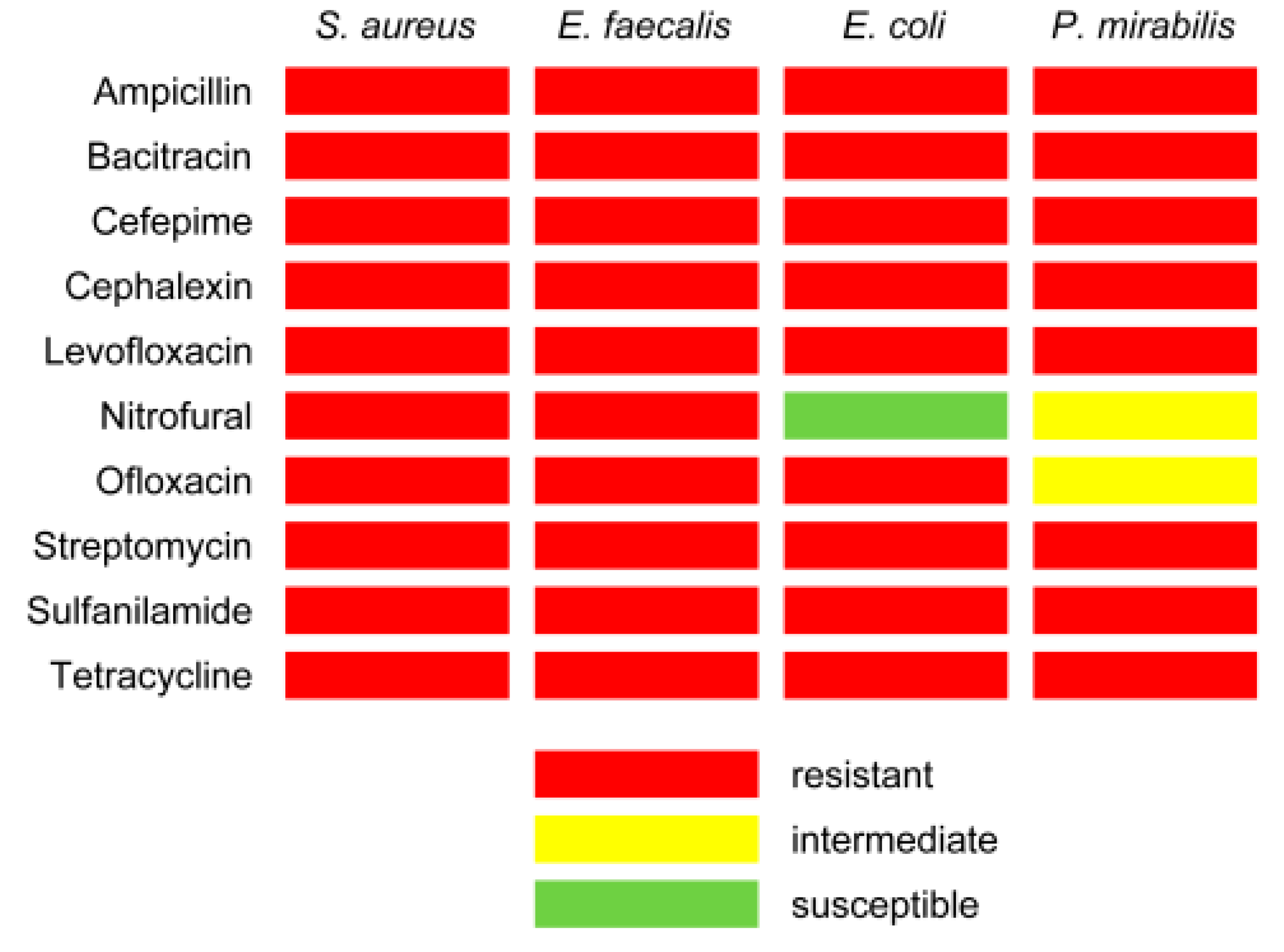
2.2. Antibiotic Susceptibility Testing
2.3. Multiple Antibiotic Resistance (MAR) Index
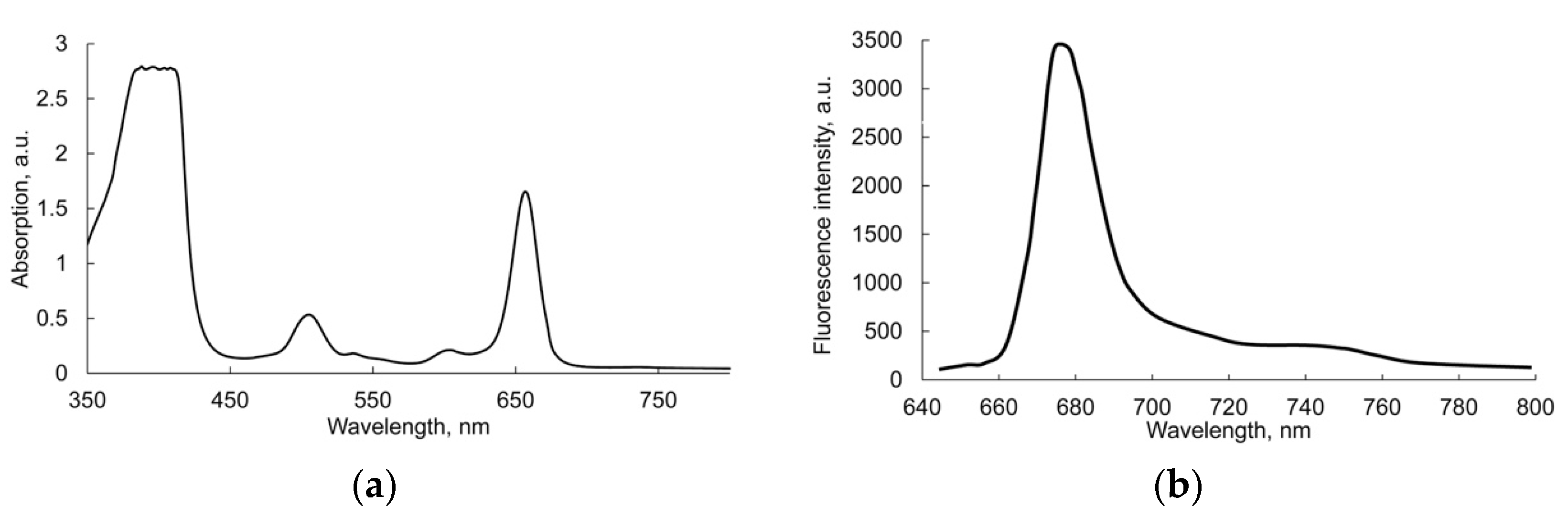
2.4. Accumulation of Photosensitizer by Microorganisms
2.5. Preparation of Competent Bacterial Cells
2.6. PDI Assay In Vitro
2.7. Statistical Analysis
3. Results
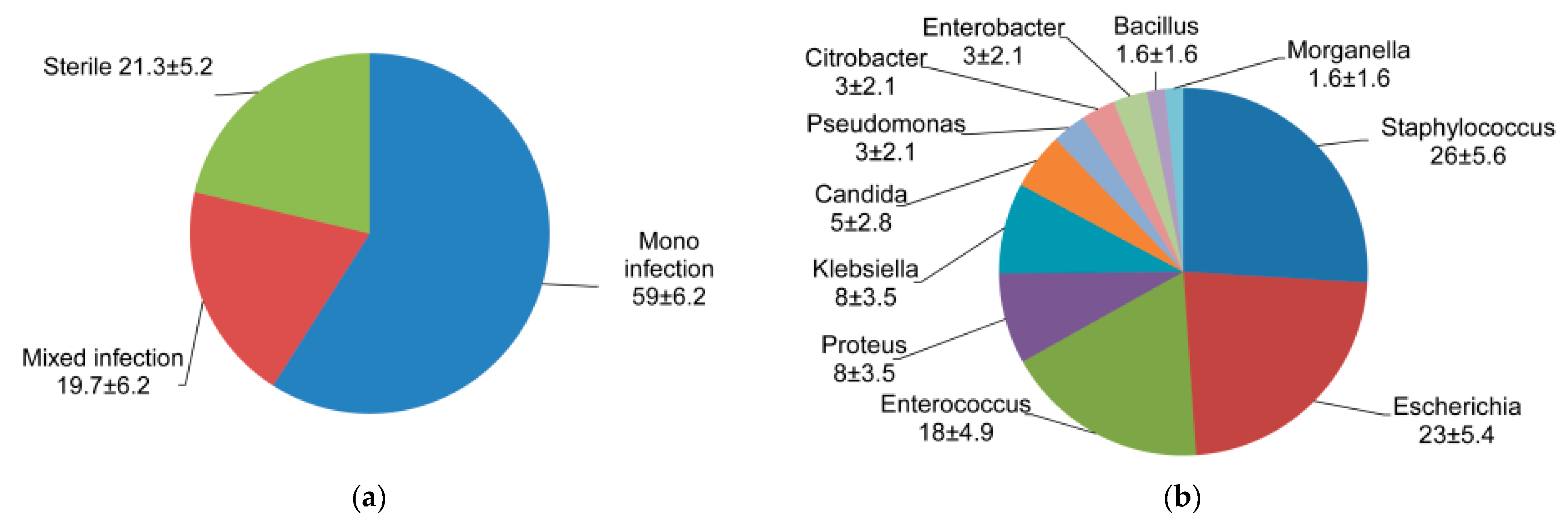
3.1. Spectrum of Uropathogenic Bacteria Associated with Renal Calculi
3.2. Antibiotic Susceptibility Testing
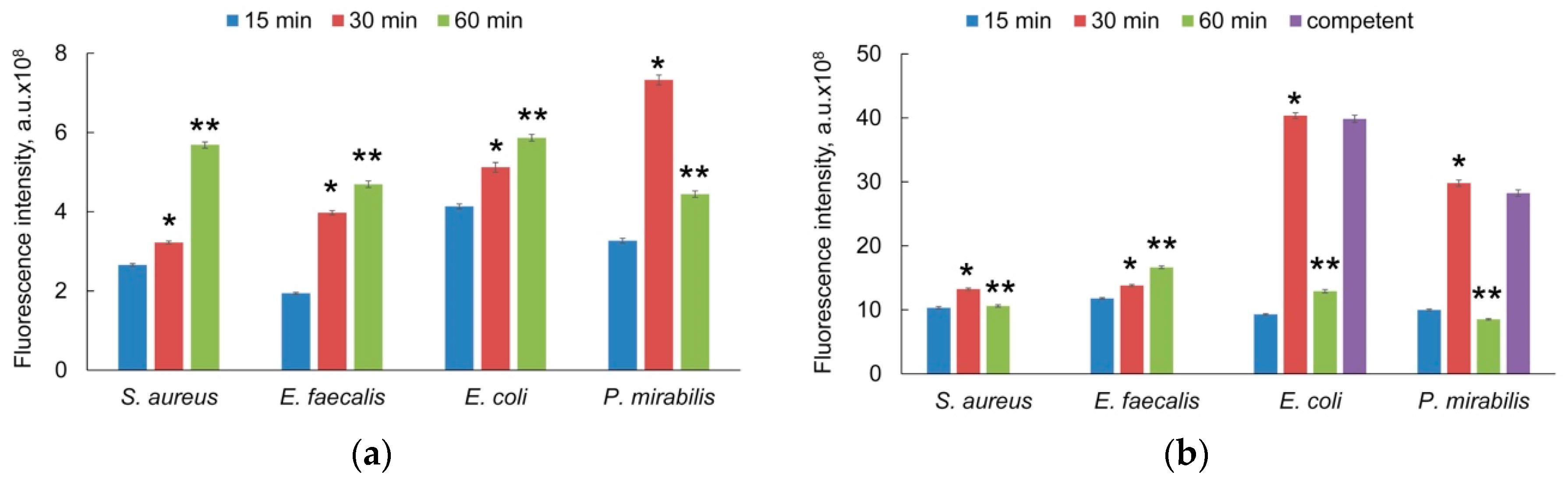
3.3. Photosensitizer Accumulation
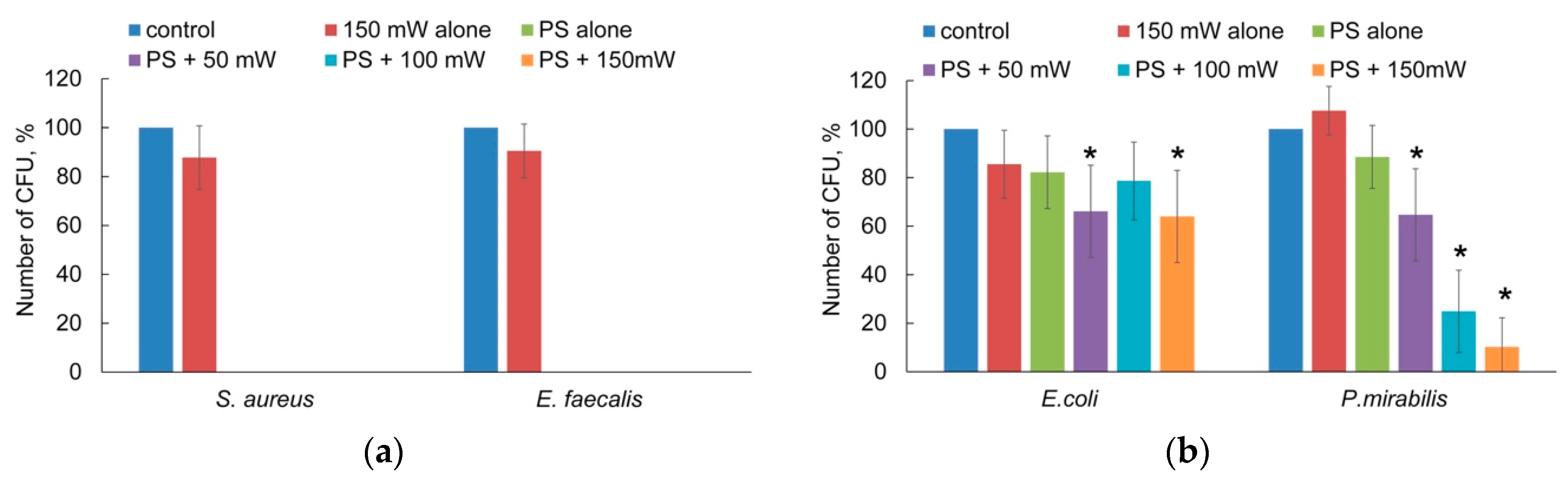
3.4. Photodynamic Inactivation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mahato, S.; Mandal, P.; Mahato, A. Biofilm producon by uropathogens like Klebsiella spp. and Pseudomonas spp. and their antibiotic susceptibility. BJHS 2020, 5, 902–906. [Google Scholar]
- Rice, L.B. Federal funding for the study of antimicrobial resistance in nosocomial pathogens: No ESKAPE. J. Infect. Dis. 2008, 15, 1079–1081. [Google Scholar] [CrossRef] [PubMed]
- Türk, C.; Knoll, T.; Petrik, A.; Sarica, K.; Skolarikos, A.; Straub, M.; Seitz, C. Guidelines on Urolithiasis. Eur. Urol. 2014, 20, 308–341. [Google Scholar]
- Sánchez-Martín, F.M.; Rodríguez, M.F.; Fernández, E.S.; Tomás, S.J.; Rousaud Barón, F.; Martínez-Rodríguez, R.; Villavicencio Mavrich, H. Incidencia y prevalencia de la urolitiasis en España: Revisión de los datos originales disponibles hasta la actualidad (Incidence and prevalence of published studies about urolithiasis in Spain. A review). Actas Urológicas Españolas 2007, 31, 511–520. [Google Scholar] [CrossRef] [Green Version]
- Bazin, D.; André, G.; Weil, R.; Matzen, G.; Emmanuel, V.; Carpentier, X.; Daudon, M. Absence of bacterial imprints on struvite-containing kidney stones: A structural investigation at the mesoscopic and atomic scale. Urology 2012, 79, 786–790. [Google Scholar] [CrossRef]
- Shah, P.; Baral, R.; Agrawal, C.S.; Lamsal, M.; Baral, D.; Khanal, B. Urinary Calculi: A Microbiological and Biochemical Analysis at a Tertiary Care Hospital in Eastern Nepal. Int. J. Microbiol. 2020, 2020, 8880403. [Google Scholar] [CrossRef] [PubMed]
- Flannigan, R.; Choy, W.H.; Chew, B.; Lange, D. Renal struvite stones—Pathogenesis, microbiology, and management strategies. Nat. Rev. Urol. 2014, 11, 333–341. [Google Scholar] [CrossRef]
- Strohmaier, W. Epidemiologie und Pathogenese der Urolithiasis. In Die Urologie; Part of the series Springer Reference Medizin; Springer: Berlin/Heidelberg, Germany, 2016; pp. 473–478. [Google Scholar] [CrossRef]
- Surawicz, C.M.; McFarland, L.V. Pseudomembranous colitis: Causes and cures. Digestion 1999, 60, 91–100. [Google Scholar] [CrossRef]
- Cohen, S.H.; Gerding, D.N.; Johnson, S.; Kelly, C.P.; Loo, V.G.; McDonald, L.C.; Pepin, J.; Wilcox, M.H.; Society for Healthcare Epidemiology of America; Infectious Diseases Society of America. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the infectious diseases society of America (IDSA). Infect. Control Hosp. Epidemiol. 2010, 31, 431–455. [Google Scholar] [CrossRef]
- Sperandio, F.F.; Huang, Y.Y.; Hamblin, M.R. Antimicrobial photodynamic therapy to kill gram-negative bacteria. Recent Pat. Anti-Infect. Drug Discov. 2013, 8, 108–120. [Google Scholar] [CrossRef] [Green Version]
- Cieplik, F.; Deng, D.; Crielaard, W.; Buchalla, W.; Hellwig, E.; Al-Ahmad, A.; Maisch, T. Antimicrobial photodynamic therapy—What we know and what we don’t. Crit. Rev. Microbiol. 2018, 44, 571–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rkein, A.M.; Ozog, D.M. Photodynamic therapy. Dermatol. Clin. 2014, 32, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Kashef, N.; Hamblin, M.R. Can microbial cells develop resistance to oxidative stress in antimicrobial photodynamic inactivation? Drug Resist. Updates 2017, 31, 31–42. [Google Scholar] [CrossRef]
- Staerck, C.; Gastebois, A.; Vandeputte, P.; Calenda, A.; Larcher, G.; Gillmann, L.; Papon, N.; Bouchara, J.P.; Fleury, M.J.J. Microbial antioxidant defense enzymes. Microb. Pathog. 2017, 110, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Sarda, R.A.; Shetty, R.M.; Tamrakar, A.; Shetty, S.Y. Antimicrobial efficacy of photodynamic therapy, diode laser, and sodium hypochlorite and their combinations on endodontic pathogens. Photodiagnosis Photodyn. Ther. 2019, 28, 265–272. [Google Scholar] [CrossRef]
- Schreiner, M.; Baumler, W.; Eckl, D.B.; Spath, A.; Konig, B.; Eichner, A. Photodynamic inactivation of bacteria to decolonize meticillin-resistant Staphylococcus aureus from human skin. Brit. J. Dermatol. 2018, 179, 1358–1367. [Google Scholar] [CrossRef]
- Otieno, W.; Liu, C.; Deng, H.; Li, J.; Zeng, X.; Ji, Y. Hypocrellin B-Mediated photodynamic inactivation of gram-positive antibiotic-resistant bacteria: An in vitro study. Photobiomodul. Photomed. Laser Surg. 2019, 38, 36–42. [Google Scholar] [CrossRef]
- Wayne, P.A. Performance Standards for Antimicrobial Disk Susceptibility Tests, 12th ed.; CLSI document M02-A12; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2015. [Google Scholar]
- Gonzales, M.F.; Brooks, T.; Pukatzki, S.U.; Provenzano, D. Rapid protocol for preparation of electrocompetent Escherichia coli and Vibrio cholerae. J. Vis. Exp. 2013, 8, 50684. [Google Scholar] [CrossRef] [Green Version]
- Abou-Elela, A. Epidemiology, pathophysiology, and management of uric acid urolithiasis: A narrative review. J. Adv. Res. 2017, 8, 513–527. [Google Scholar] [CrossRef]
- Thass, N.; Kumar, M.; Kaur, R. Phenotypic methods to detect virulence factors of uropathogenic e.coli isolates and their antimicrobial susceptibility pattern. Int. J. Cur. Adv. Res. 2020, 9, 22345–22348. [Google Scholar]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Cortes-Penfield, N.W.; Trautner, B.W.; Jump, R.L.P. Urinary tract infection and asymptomac bacteriuria in older adults. Infect. Dis. Clin. N. Am. 2017, 31, 673–688. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.N.; Armbruster, C.E. Indwelling urinary catheter model of Proteus mirabilis infection. Methods Mol. Biol. 2019, 2021, 187–200. [Google Scholar] [CrossRef]
- Morris, N.S.; Stickler, D.J.; McLean, R.J. The development of bacterial biofilms on indwelling urethral catheters. World J. Urol. 1999, 17, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Qin, R.; Zaat, S.A.J.; Breukink, E.; Heger, M. Antibacterial photodynamic therapy: Overview of a promising approach to fight antibiotic-resistant bacterial infections. J. Clin. Transl. Res. 2015, 1, 140–167. [Google Scholar] [PubMed]
- Rapacka-Zdończyk, A.; Woźniak, A.; Michalska, K.; Pierański, M.; Ogonowska, P.; Grinholc, M.; Nakonieczna, J. Factors determining the susceptibility of bacteria to antibacterial photodynamic inactivation. Front. Med. (Lausanne) 2021, 8, 642609. [Google Scholar] [CrossRef]
- Delcour, A.H. Outer membrane permeability and antibiotic resistance. Biochim. Et Biophys. Acta 2009, 1794, 808–816. [Google Scholar] [CrossRef] [Green Version]
- Buzalewicz, I.; Ulatowska-Jarża, A.; Kaczorowska, A.; Gąsior-Głogowska, M.; Podbielska, H.; Karwańska, M.; Wieliczko, A.; Matczuk, A.K.; Kowal, K.; Kopaczyńska, M. Bacteria single-cell and photosensitizer interaction revealed by quantitative phase imaging. Int. J. Mol. Sci. 2021, 22, 5068. [Google Scholar] [CrossRef]
- George, S.; Hamblin, M.R.; Kishen, A. Uptake pathways of anionic and cationic photosensitizers into bacteria. Photochem. Photobiol. Sci. 2009, 8, 788–795. [Google Scholar] [CrossRef] [Green Version]
- Sułek, A.; Pucelik, B.; Kobielusz, M.; Barzowska, A.; Dąbrowski, J.M. Photodynamic inactivation of bacteria with porphyrin derivatives: Effect of charge, lipophilicity, ROS generation, and cellular uptake on their biological activity in vitro. Int. J. Mol. Sci. 2020, 21, 8716. [Google Scholar] [CrossRef] [PubMed]
- Schrader, A.M.; Cheng, C.-Y.; Israelachvili, J.N.; Han, S. Communication: Contrasting effects of glycerol and DMSO on lipid membrane surface hydration dynamics and forces. J. Chem. Phys. 2016, 145, 041101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pocivavsek, L.; Gavrilov, K.; Cao, K.D.; Chi, E.Y.; Li, D.; Lin, B.; Meron, M.; Majewski, J.; Lee, K.Y. Glycerol-induced membrane stiffening: The role of viscous fluid adlayers. Biophys. J. 2011, 101, 118–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kourtesi, C.; Ball, A.R.; Huang, Y.Y.; Jachak, S.M.; Vera, D.M.; Khondkar, P.; Gibbons, S.; Hamblin, M.R.; Tegos, G.P. Microbial efflux systems and inhibitors: Approaches to drug discovery and the challenge of clinical implementation. Open Microbiol. J. 2013, 7, 34–52. [Google Scholar] [CrossRef] [Green Version]
- Mueller, E.A.; Levin, P.A. Bacterial cell wall quality control during environmental stress. mBio 2020, 11, e02456-20. [Google Scholar] [CrossRef] [PubMed]
- Zgurskaya, H.I.; Löpez, C.A.; Gnanakaran, S. Permeability barrier of gram-negative cell envelopes and approaches to bypass it. ACS Infect. Dis. 2015, 1, 512–522. [Google Scholar] [CrossRef] [Green Version]
- Skovsen, E.; Snyder, J.W.; Lambert, J.D.; Ogilby, P.R. Lifetime and diffusion of singlet oxygen in a cell. J. Phys. Chem. 2005, 12, 8570–8573. [Google Scholar] [CrossRef]
- Mullineaux, C.W.; Nenninger, A.; Ray, N.; Robinson, C. Diffusion of green fluorescent protein in three cell environments in Escherichia coli. J. Bacteriol. 2006, 188, 3442–3448. [Google Scholar] [CrossRef] [Green Version]
- Fekrazad, R.; Zare, H.; Mohammadi, S.S.; Morsali, P. The effect of antimicrobial photodynamic therapy with radachlorin® on Staphylococcus aureus and Escherichia coli: An in vitro study. J. Lasers Med. Sci. 2014, 5, 82–85. [Google Scholar]
- Luke-Marshall, N.R.; Hansen, L.A.; Shafirstein, G.; Campagnari, A.A. Antimicrobial photodynamic therapy with chlorin e6 is bactericidal against biofilms of the primary human otopathogens. mSphere 2020, 5, e00492-20. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ignatova, N.; Ivanova, T.; Antonyan, A.; Budruev, I.; Streltsova, O.; Elagin, V.; Kamensky, V. Efficacy of Photodynamic Inactivation against the Major Human Antibiotic-Resistant Uropathogens. Photonics 2021, 8, 495. https://doi.org/10.3390/photonics8110495
Ignatova N, Ivanova T, Antonyan A, Budruev I, Streltsova O, Elagin V, Kamensky V. Efficacy of Photodynamic Inactivation against the Major Human Antibiotic-Resistant Uropathogens. Photonics. 2021; 8(11):495. https://doi.org/10.3390/photonics8110495
Chicago/Turabian StyleIgnatova, Nadezhda, Tatiana Ivanova, Artem Antonyan, Ivan Budruev, Olga Streltsova, Vadim Elagin, and Vladislav Kamensky. 2021. "Efficacy of Photodynamic Inactivation against the Major Human Antibiotic-Resistant Uropathogens" Photonics 8, no. 11: 495. https://doi.org/10.3390/photonics8110495
APA StyleIgnatova, N., Ivanova, T., Antonyan, A., Budruev, I., Streltsova, O., Elagin, V., & Kamensky, V. (2021). Efficacy of Photodynamic Inactivation against the Major Human Antibiotic-Resistant Uropathogens. Photonics, 8(11), 495. https://doi.org/10.3390/photonics8110495