Power Output of Two Semiconductor Lasers: An Observational Study

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Power Delivered in Continuous-Wave Mode
2.2. Power Delivered in Pulsed Mode
3. Results
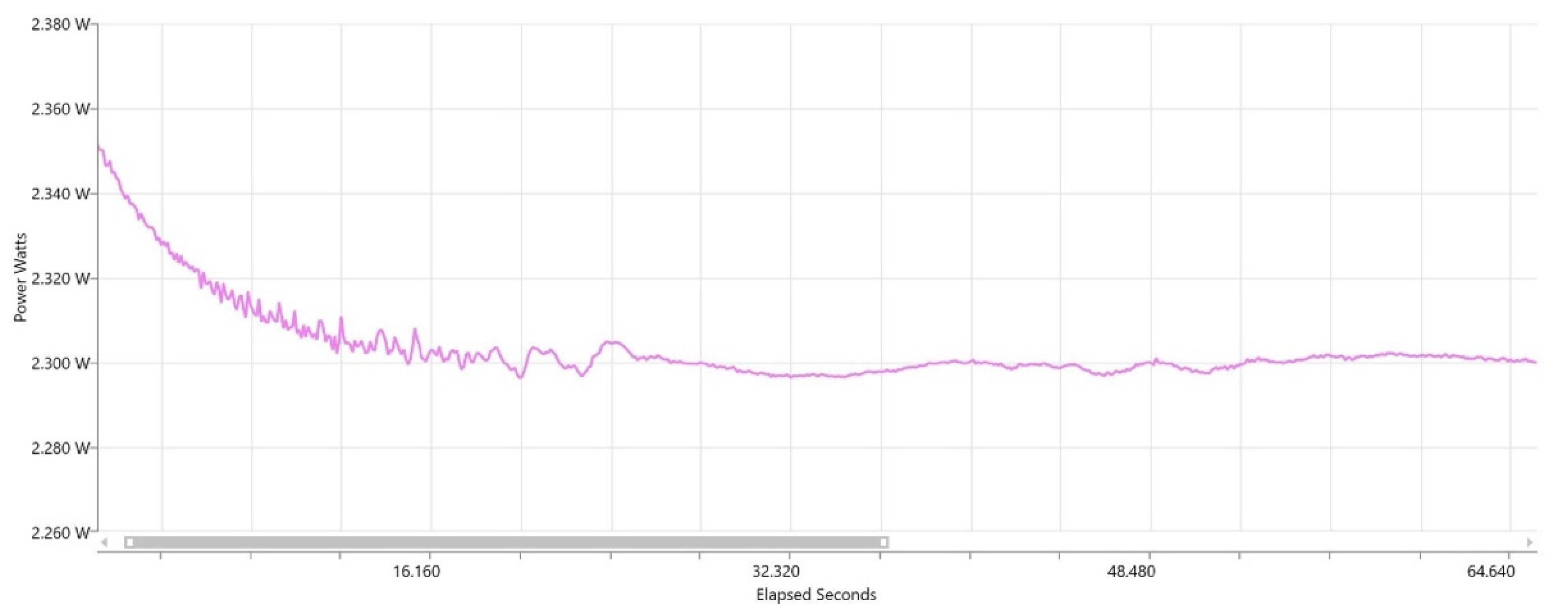
3.1. Test in Continuous-Wave Mode
3.2. Test in Pulsed Mode
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Verma, S.K.; Maheshwari, S.; Singh, R.K.; Chaudhari, P.K. Laser in dentistry: An innovative tool in modern dental practice. Natl. J. Maxillofac. Surg. 2012, 3, 124–132. [Google Scholar] [CrossRef] [Green Version]
- Karic, V.; Melman, G.; Mulder, R. Introduction to Dental Lasers. S. Afr. Dent. J. 2016, 71, 178. [Google Scholar]
- Rios, F.G.; Viana, E.R.; Ribeiro, G.M.; González, J.C.; Abelenda, A.; Peruzzo, D.C. Temperature evaluation of dental implant surface irradiated with high-power diode laser. Lasers Med. Sci. 2016, 31, 1309–1316. [Google Scholar] [CrossRef] [PubMed]
- Derikvand, N.; Chinipardaz, Z.; Ghasemi, S.; Chiniforush, N. The versatility of 980 nm diode laser in dentistry: A case series. J. Lasers Med. Sci. 2016, 7, 205. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Concepción, D.; Cano-Durán, J.A.; Peña-Cardelles, J.F.; Paredes-Rodríguez, V.M.; González-Serrano, J.; López-Quiles, J. The application of diode laser in the treatment of oral soft tissues lesions. A literature review. J. Clin. Exp. Dent. 2017, 9, e925–e928. [Google Scholar] [CrossRef] [Green Version]
- Kumar, R.; Jain, G.; Dhodapkar, S.V.; Kumathalli, K.I.; Jaiswal, G. The Comparative Evaluation of Patient’s Satisfaction and Comfort Level by Diode Laser and Scalpel in the Management of Mucogingival Anomalies. J. Clin. Diagn Res. 2015, 9, ZC56–ZC58. [Google Scholar] [CrossRef] [PubMed]
- Michalik, M.; Szymańczyk, J.; Stajnke, M.; Ochrymiuk, T.; Cenian, A. Medical Applications of Diode Lasers: Pulsed versus Continuous Wave (cw) Regime. Micromachines 2021, 12, 710. [Google Scholar] [CrossRef] [PubMed]
- Azma, E.; Safavi, N. Diode laser application in soft tissue oral surgery. J. Lasers Med. Sci. 2013, 4, 206–211. [Google Scholar] [PubMed]
- Bago, I.; Plečko, V.; Gabrić Pandurić, D.; Schauperl, Z.; Baraba, A.; Anić, I. Antimicrobial efficacy of a high-power diode laser, photo-activated disinfection, conventional and sonic activated irrigation during root canal treatment. Int. Endod. J. 2013, 46, 339–347. [Google Scholar] [CrossRef] [Green Version]
- Beer, F.; Farmakis, E.T.; Kopic, J.; Kurzmann, C.; Moritz, A. Temperature Development on the External Root Surface During Laser-Assisted Endodontic Treatment Applying a Microchopped Mode of a 980 nm Diode Laser. Photomed. Laser Surg. 2017, 35, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, H.G.; Kurtulmus-Yilmaz, S.; Cengiz, E. Long-term effect of diode laser irradiation compared to sodium fluoride varnish in the treatment of dentine hypersensitivity in periodontal maintenance patients: A randomized controlled clinical study. Photomed. Laser Surg. 2011, 29, 721–725. [Google Scholar] [CrossRef] [PubMed]
- De Moor, R.J.; Verheyen, J.; Verheyen, P.; Diachuk, A.; Meire, M.A.; De Coster, P.J.; De Bruyne, M.; Keulemans, F. Laser teeth bleaching: Evaluation of eventual side effects on enamel and the pulp and the efficiency in vitro and in vivo. Sci. World J. 2015, 2015, 835405. [Google Scholar] [CrossRef]
- Al-Maliky, M.A.; Frentzen, M.; Meister, J. Artificial Caries Resistance in Enamel after Topical Fluoride Treatment and 445 nm Laser Irradiation. Biomed. Res. Int. 2019, 2019, 9101642. [Google Scholar] [CrossRef] [PubMed]
- Lagdive, S.; Doshi, Y.; Marawar, P. Management of Gingival Hyperpigmentation Using Surgical Blade and Diode Laser Therapy: A Comparative Study. J. Oral Laser Appl. 2009, 9, 208–210. [Google Scholar]
- Pogrel, M.; Muff, D.; Marshall, G. Structural changes in dental enamel induced by high energy continuous wave carbon dioxide laser. Lasers Surg. Med. 1993, 13, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Miglani, S.; Patro, S. Lasers in Implant Dentistry. In Advances in Dental Implantology using Nanomaterials and Allied Technology Applications; Chaughule, R.S., Dashaputra, R., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 225–245. [Google Scholar] [CrossRef]
- George, R. Laser in dentistry-Review. Int. J. Dent. Clin. 2009, 1, 13–19. [Google Scholar]
- Coluzzi, D.; Parker, S. Lasers in Dentistry—Current Concepts; Springer International Publishing: Berlin/Heidelberg, Germany, 2017. [Google Scholar] [CrossRef]
- Belikov, A.V.; Skrypnik, A.V.; Shatilova, K.V. Comparison of diode laser in soft tissue surgery using continuous wave and pulsed modes in vitro. Front. Optoelectron. 2015, 8, 212–219. [Google Scholar] [CrossRef]
- Coluzzi, D.J.; Robert, A. Laser fundamentals. In Principles and Practice of Laser Dentistry; Elsevier: Amsterdam, The Netherlands, 2015; pp. 12–26. [Google Scholar]
- Parker, S. Verifiable CPD paper: Introduction, history of lasers and laser light production. Br. Dent. J. 2007, 202, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Epperlein, P.W. Semiconductor Laser Engineering, Reliability and Diagnostics: A Practical Approach to High Power and Single Mode Devices; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Jiménez, J. Laser diode reliability: Crystal defects and degradation modes. Comptes Rendus Phys. 2003, 4, 663–673. [Google Scholar] [CrossRef]
- Pirnat, S. Versatility of an 810 nm diode laser in dentistry: An overview. J. Laser Health Acad. 2007, 4, 1–9. [Google Scholar]
- Frentzen, M.; Kraus, D.; Reichelt, J.; Engelbach, C.; Dehn, C.; Meister, J. A novel blue light diode laser (445 nm) for dental application Biomedical testing and clinical aspects. Laser Int. Mag. Laser Dent. 2016, 8, 6–13. [Google Scholar]
- Katalinić, I.; Budimir, A.; Bošnjak, Z.; Jakovljević, S.; Anić, I. The photo-activated and photo-thermal effect of the 445/970 nm diode laser on the mixed biofilm inside root canals of human teeth in vitro: A pilot study. Photodiagnosis Photodyn. Ther. 2019, 26, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Klim, J.D.; Fox, D.B.; Coluzzi, D.J.; Neckel, C.P.; Swick, M.D. The diode laser in dentistry. Rev. Wavel. 2000, 8, 13–16. [Google Scholar]
- Dostalova, T.; Jelinkova, H.; Housova, D.; Sulc, J.; Nemec, M.; Miyagi, M.; Junior, A.B.; Zanin, F. Diode laser-activated bleaching. Braz. Dent. J. 2004, 15, SI-3. [Google Scholar]
- Braun, A.; Braun, A.; Kettner, M.; Berthold, M.; Wenzler, J.-S.; Heymann, P.G.B.; Frankenberger, R. Efficiency of soft tissue incision with a novel 445-nm semiconductor laser. Lasers Med. Sci. 2018, 33, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Ibacache, M.C.T.; Arcos, P.; Sanchez, S.; Weinstein, G. Use of diode lasers in dentistry. Clin. Dent. Rev. 2020, 4, 6. [Google Scholar] [CrossRef]
- Ren, C.; McGrath, C.; Jin, L.; Zhang, C.; Yang, Y. The effectiveness of low-level laser therapy as an adjunct to non-surgical periodontal treatment: A meta-analysis. J. Periodontal Res. 2017, 52, 8–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehuys, D.G. Chapter 4-High-Power Semiconductor Lasers. In Semiconductor Lasers II; Kapon, E., Ed.; Academic Press: San Diego, CA, USA, 1999; pp. 259–321. [Google Scholar]
- Hanke, A.; Fimmers, R.; Frentzen, M.; Meister, J. Quantitative determination of cut efficiency during soft tissue surgery using diode lasers in the wavelength range between 400 and 1500 nm. Lasers Med. Sci. 2021, 36, 1633–1647. [Google Scholar] [CrossRef] [PubMed]
- Beer, F.; Körpert, W.; Passow, H.; Steidler, A.; Meinl, A.; Buchmair, A.G.; Moritz, A. Reduction of collateral thermal impact of diode laser irradiation on soft tissue due to modified application parameters. Lasers Med. Sci. 2012, 27, 917–921. [Google Scholar] [CrossRef]
- de Alencar Mollo, M.; Frigo, L.; Favero, G.M.; Lopes-Martins, R.Á.B.; Junior, A.B. In vitro analysis of human tooth pulp chamber temperature after low-intensity laser therapy at different power outputs. Lasers Med. Sci. 2011, 26, 143–147. [Google Scholar] [CrossRef] [PubMed]
- da Fonseca Alvarez, A.; Davidowicz, H.; Moura-Netto, C.; Frugoli, A.D.; Fernando, C.; Aranha, A.C.C. Temperature changes on the root surfaces of mandibular incisors after an 810-nm high-intensity intracanal diode laser irradiation. J. Biomed. Opt. 2012, 17, 015006. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dental Device | SIROLaser Blue | Picasso | |
|---|---|---|---|
| Wavelength | 445 nm | 970 nm | 810 nm |
| Spot diameter | 1 mm | 1 mm | 1 mm |
| Spot area | 0.8 mm2 | 0.8 mm2 | 0.8 mm2 |
| Stipulated output power | 3 W | 2 W | 2.5 W |
| Lowest output power measured | 3.5 W | 2.4 W | 2.2 W |
| Highest output power measured | 3.7 W | 2.5 W | 2.6 W |
| Mean output power measured | 3.6 W | 2.5 W | 2.3 W |
| Smallest difference in output power | 0.5 W | 0.4 W | 0.1 W |
| Largest difference in output power | 0.7 W | 0.5 W | −0.3 W |
| Percentage change in mean output power | 21% | 22% | −8% |
| Dental Device | SIROLaser Blue | Picasso | |
|---|---|---|---|
| Wavelength | 445 nm | 970 nm | 810 nm |
| Spot diameter | 1 mm | 1 mm | 1 mm |
| Spot area | 0.8 mm2 | 0.8 mm2 | 0.8 mm2 |
| Pulse duration | 50 ms | 50 ms | 29 ms |
| Duty cycle | 50% | 50% | 50% |
| Frequency | 10 Hz | 10 Hz | 17 Hz |
| Stipulated output power | 3 W | 2 W | 2.5 W |
| Stipulated average power | 1.5 W | 1.0 W | 1.3 W |
| Lowest output power measured | 4.0 W | 2.5 W | 2.4 W |
| Highest output power measured | 4.1 W | 2.5 W | 2.4 W |
| Mean output power measured | 4.1 W | 2.5 W | 2.4 W |
| Mean average power measured | 1.9 W | 1.2 W | 1.2 W |
| Smallest difference in output power | 1.0 W | 0.5 W | −0.1 W |
| Largest difference in output power | 1.1 W | 0.5 W | −0.1 W |
| Percentage change of the mean output power | 37% | 26% | −3% |
| Percentage change in mean average power | 29% | 24% | −5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xue, V.W.; Yin, I.X.; Niu, J.Y.; Luk, K.; Lo, E.C.M.; Chu, C.H. Power Output of Two Semiconductor Lasers: An Observational Study. Photonics 2022, 9, 219. https://doi.org/10.3390/photonics9040219
Xue VW, Yin IX, Niu JY, Luk K, Lo ECM, Chu CH. Power Output of Two Semiconductor Lasers: An Observational Study. Photonics. 2022; 9(4):219. https://doi.org/10.3390/photonics9040219
Chicago/Turabian StyleXue, Vicky Wenqing, Iris Xiaoxue Yin, John Yun Niu, Kenneth Luk, Edward Chin Man Lo, and Chun Hung Chu. 2022. "Power Output of Two Semiconductor Lasers: An Observational Study" Photonics 9, no. 4: 219. https://doi.org/10.3390/photonics9040219