Evaluation of the Effectiveness of Acupuncture in the Treatment of Knee Osteoarthritis: A Case Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Characterization
2.2. Materials
2.3. Methodology
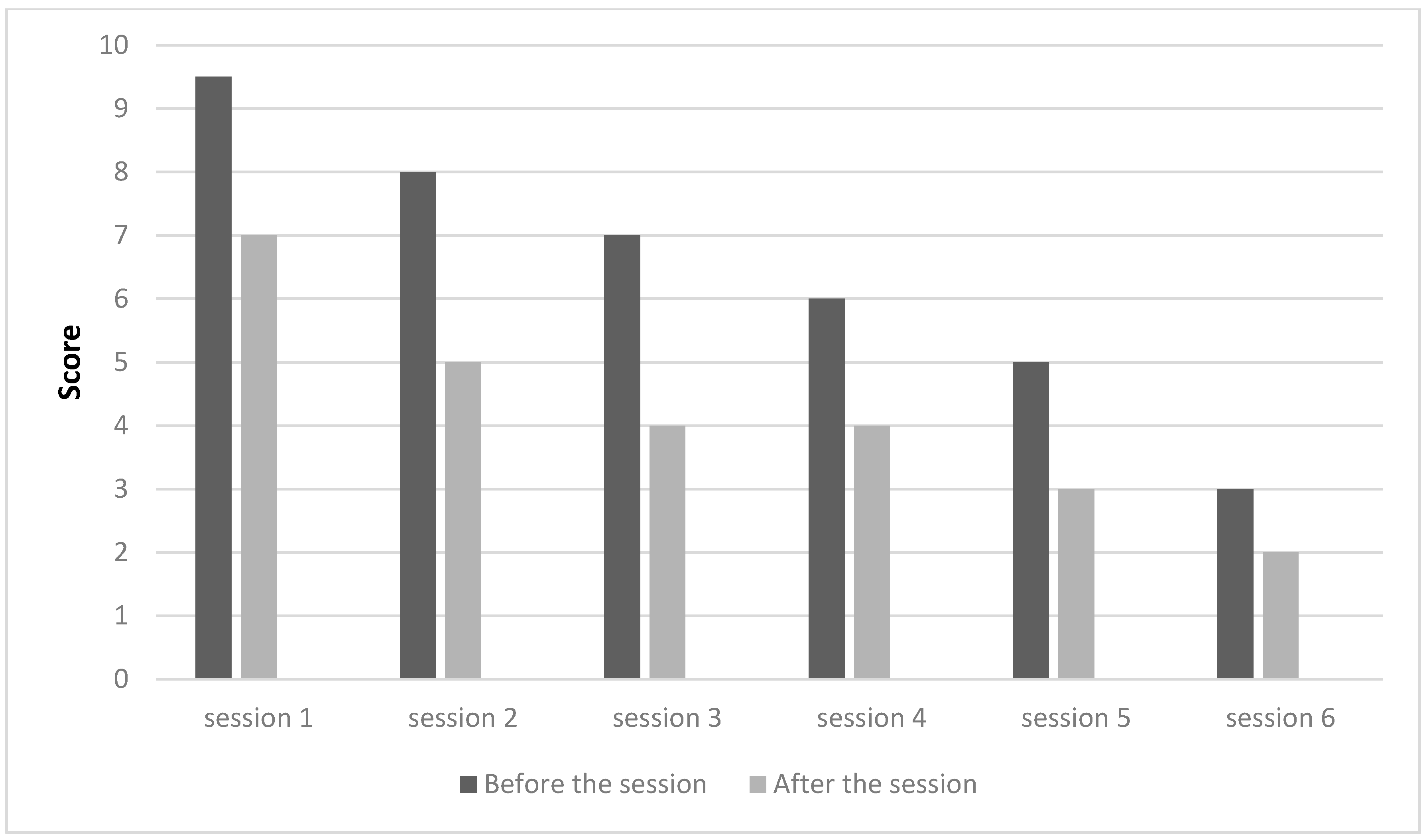
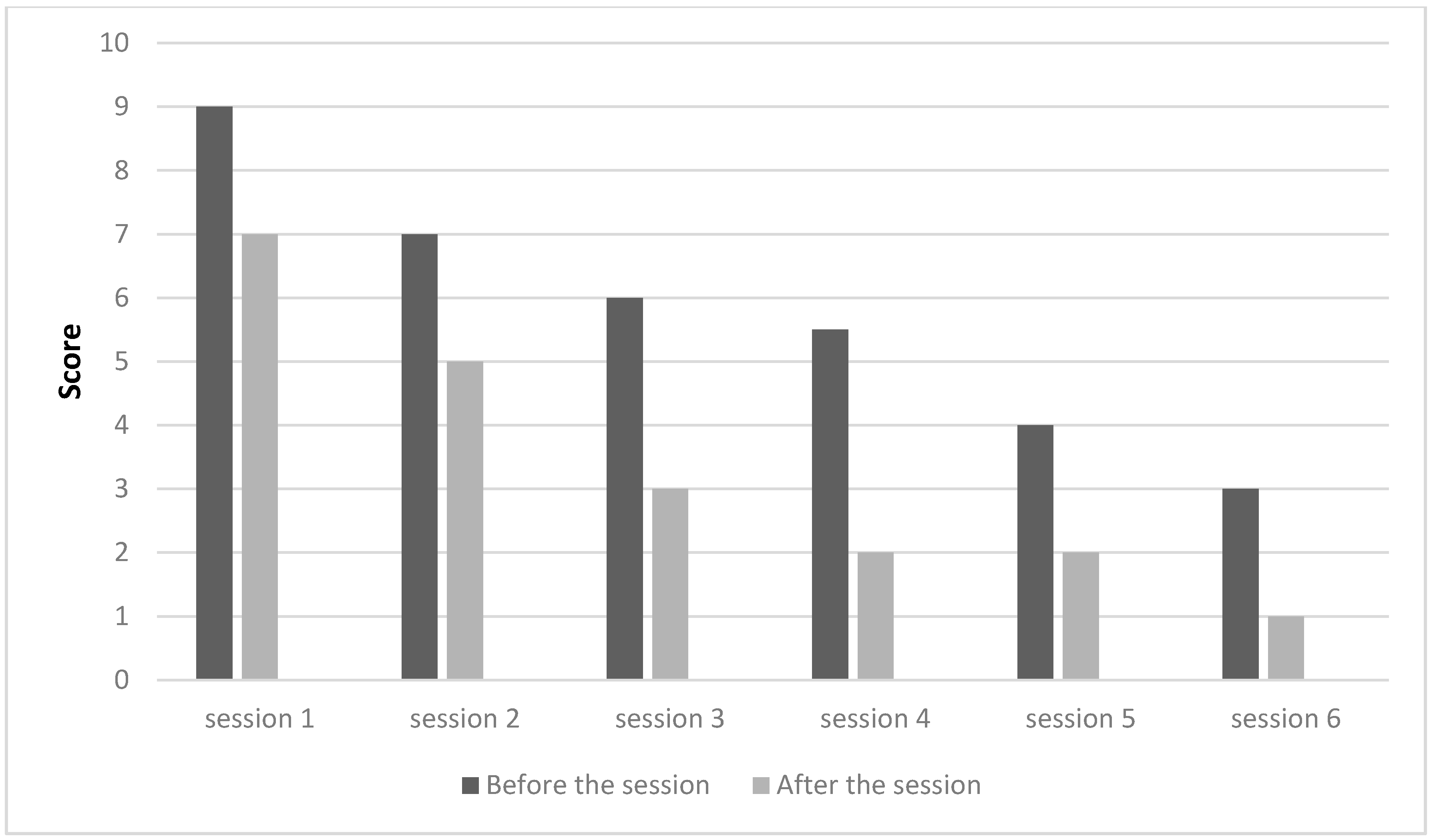
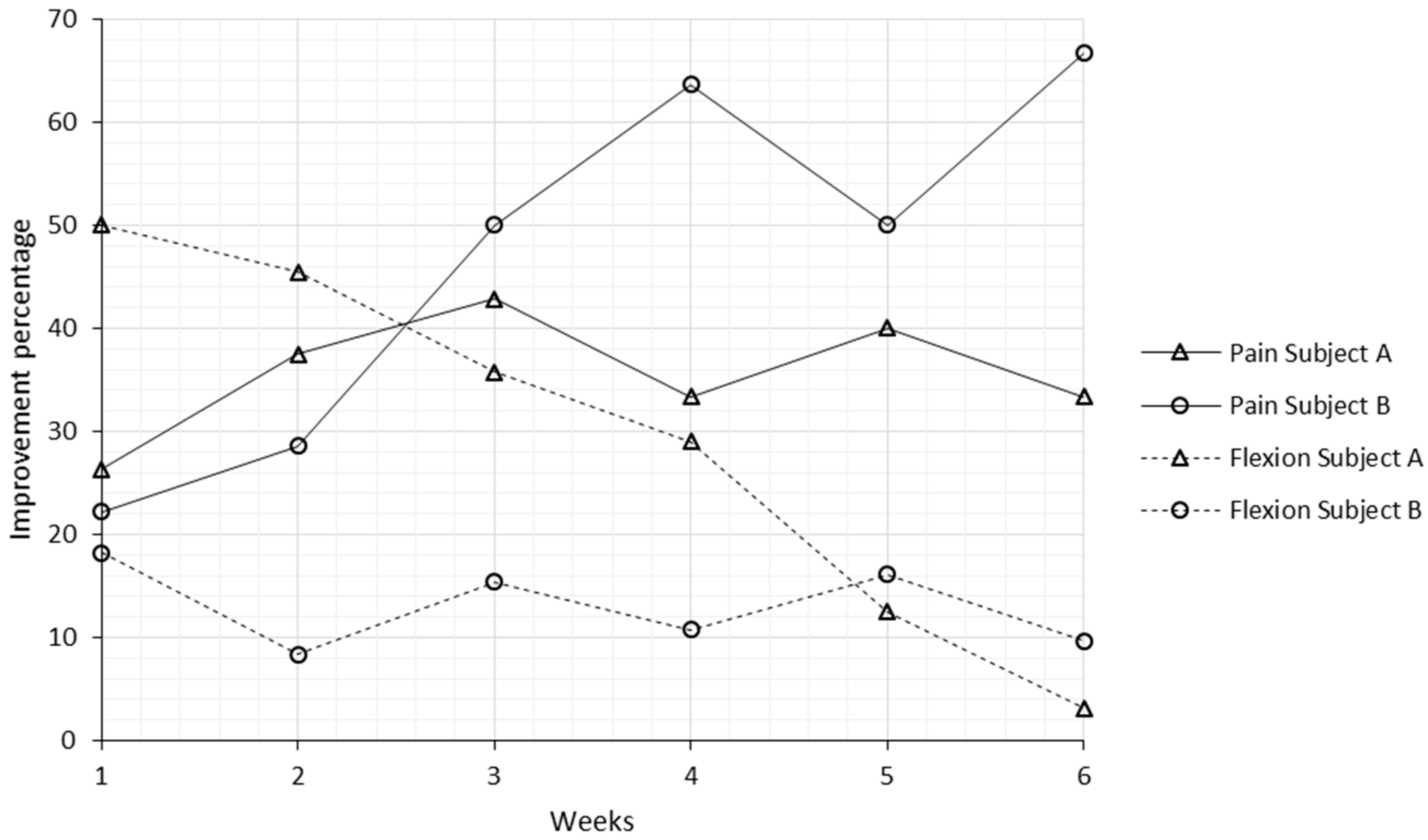
3. Results
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Crawford, D.C.; Miller, L.E.; Block, J.E. Conservative management of symptomatic knee osteoarthritis: A flawed strategy? Orthop. Rev. 2013, 5, e2. [Google Scholar] [CrossRef] [PubMed]
- Langworthy, M.J.; Saad, A.; Langworthy, N.M. Conservative treatment modalities and outcomes for osteoarthritis: The concomitant pyramid of treatment. Phys. Sportsmed. 2010, 38, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Silverwood, V.; Blagojevic-Bucknall, M.; Jinks, C.; Jordan, J.; Protheroe, J.; Jordan, K. Current evidence on risk factors for knee osteoarthritis in older adults: A systematic review and meta-analysis. Osteoarthr. Cartil. 2015, 23, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Boyan, B.D.; Hart, D.A.; Enoka, R.M.; Nicolella, D.P.; Resnick, E.; Berkley, K.J.; Sluka, K.A.; Kwoh, C.K.; Tosi, L.L.; O’Connor, M.I.; et al. Hormonal modulation of connective tissue homeostasis and sex differences in risk for osteoarthritis of the knee. Biol. Sex Differ. 2013, 4, 3. [Google Scholar] [CrossRef] [PubMed]
- Pereira, D.; Peleteiro, B.; Araujo, J.; Branco, J.; Santos, R.; Ramos, E. The effect of osteoarthritis definition on prevalence and incidence estimates: A systematic review. Osteoarthr. Cartil. 2011, 19, 1270–1285. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, M.C.; Altman, R.D.; April, K.T.; Benkhalti, M.; Guyatt, G.; McGowan, J.; Towheed, T.; Welch, V.; Wells, G.; Tugwell, P. American college of rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2012, 64, 465–474. [Google Scholar] [CrossRef]
- Newberry, S.J.; FitzGerald, J.; SooHoo, N.F.; Booth, M.; Marks, J.; Motala, A.; Apaydin, E.; Chen, C.; Raaen, L.; Shanman, R. Treatment of Osteoarthritis of the Knee: An Update Review; Report No. 17-EHC011-EF; AHRQ (US Agency for Healthcare Research and Quality): Rockville, MD, USA, 2017.
- Alshami, A.M. Knee osteoarthritis related pain: A narrative review of diagnosis and treatment. Int. J. Health Sci. 2014, 8, 85–104. [Google Scholar] [CrossRef]
- Hussain, S.; Neilly, D.; Baliga, S.; Patil, S.; Meek, R. Knee osteoarthritis: A review of management options. Scott. Med. J. 2016, 61, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Yue, J. Treatment of 78 patients with knee osteoarthritis by acupuncture, moxibustion, and tuina. World J. Acupunct. Moxibustion 2015, 25, 53–56. [Google Scholar] [CrossRef]
- Mavrommatis, C.I.; Argyra, E.; Vadalouka, A.; Vasilakos, D.G. Acupuncture as an adjunctive therapy to pharmacological treatment in patients with chronic pain due to osteoarthritis of the knee: A 3-armed, randomized, placebo-controlled trial. Pain 2012, 153, 1720–1726. [Google Scholar] [CrossRef] [PubMed]
- Fu, M.; Zhang, Z. Knee osteoarthritis treated with acupuncture based on syndrome differentiation: A randomized controlled trial. World J. Acupunct. Moxibustion 2012, 22, 11–17. [Google Scholar] [CrossRef]
- Corbett, M.S.; Rice, S.J.C.; Madurasinghe, V.; Slack, R.; Fayter, D.A.; Harden, M.; Sutton, A.J.; MacPherson, H.; Woolacott, N.F. Acupuncture and other physical treatments for the relief of pain due to osteoarthritis of the knee: Network meta-analysis. Osteoarthr. Cartil. 2013, 21, 1290–1298. [Google Scholar] [CrossRef] [PubMed]
- Hou, P.-W.; Fu, P.-K.; Hsu, H.-C.; Hsieh, C.-L. Traditional chinese medicine in patients with osteoarthritis of the knee. J. Tradit. Complement. Med. 2015, 5, 182–196. [Google Scholar] [CrossRef] [PubMed]
- Selfe, T.K.; Taylor, A.G. Acupuncture and osteoarthritis of the knee: A review of randomized, controlled trials. Fam. Community Health 2008, 31, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Ezzo, J.; Hadhazy, V.; Birch, S.; Lao, L.; Kaplan, G.; Hochberg, M.; Berman, B. Acupuncture for osteoarthritis of the knee: A systematic review. Arthritis Rheumatol. 2001, 44, 819–825. [Google Scholar] [CrossRef]
- Mc Neill, S.; Fullen, B.M. Acupuncture for osteoarthritis of the knee: Common points and treatment parameters used. Physiotherapy 2015, 101, e968–e969. [Google Scholar] [CrossRef]
- Witt, C.M.; Jena, S.; Brinkhaus, B.; Liecker, B.; Wegscheider, K.; Willich, S.N. Acupuncture in patients with osteoarthritis of the knee or hip: A randomized, controlled trial with an additional nonrandomized arm. Arthritis Rheumatol. 2006, 54, 3485–3493. [Google Scholar] [CrossRef] [PubMed]
- Manyanga, T.; Froese, M.; Zarychanski, R.; Abou-Setta, A.; Friesen, C.; Tennenhouse, M.; Shay, B.L. Pain management with acupuncture in osteoarthritis: A systematic review and meta-analysis. BMC Complement. Altern. Med. 2014, 14, 312. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Acupuncture: Review and Analysis of Reports on Controlled Clinical Trials; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Soh, K.-S. Bonghan circulatory system as an extension of acupuncture meridians. J. Acupunct. Meridian Stud. 2009, 2, 93–106. [Google Scholar] [CrossRef]
- Zhou, W.; Benharash, P. Effects and mechanisms of acupuncture based on the principle of meridians. J. Acupunct. Meridian Stud. 2014, 7, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Cheng, K.J. Neurobiological mechanisms of acupuncture for some common illnesses: A clinician's perspective. J. Acupunct. Meridian Stud. 2014, 7, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Frank Brazkiewicz, H.J.G. Conduit-(Channel) System, Acupuncture Points, Basic; Heidelberg School of Chinese Medicine: Heidelberg, Germany, 2009. [Google Scholar]
- Greten, H. Understanding Tcm—Scientific Chinese Medicine—The Heidelberg Model; Heidelberg School of Chinese Medicine: Heidelberg, Germany, 2008. [Google Scholar]
- Greten, H.J. Clinical Subjects, Scientific Chinese Medicine, the Heidelberg Model; Heidelberg School of Chinese Medicine: Heidelberg, Germany, 2008. [Google Scholar]
- Sousa, C.; Gonçalves, M.; Machado, J.; Greten, H. Treating musculoskeletal pain with traditional chinese medicine techniques—A short review. Exp. Pathol. Health Sci. 2016, 8, 25–28. [Google Scholar]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual analog scale for pain (vas pain), numeric rating scale for pain (nrs pain), mcgill pain questionnaire (mpq), short-form mcgill pain questionnaire (sf-mpq), chronic pain grade scale (cpgs), short form-36 bodily pain scale (sf-36 bps), and measure of intermittent and constant osteoarthritis pain (icoap). Arthritis Care Res. 2011, 63, S240–S252. [Google Scholar]
- Audette, J.F.; Bailey, A. Integrative Pain Medicine: The Science and Practice of Complementary and Alternative Medicine in Pain Management; Springer: Berlin/Heidelberg, Germany, 2008. [Google Scholar]
- Karner, M.; Brazkiewicz, F.; Remppis, A.; Fischer, J.; Gerlach, O.; Stremmel, W.; Subramanian, S.V.; Greten, H.J. Objectifying specific and nonspecific effects of acupuncture: A double-blinded randomised trial in osteoarthritis of the knee. Evid. Based Complement. Altern. Med. eCAM 2013, 2013, 427265. [Google Scholar] [CrossRef] [PubMed]
- Berman, B.M.; Lao, L.; Langenberg, P.; Lee, W.L.; Gilpin, A.M.; Hochberg, M.C. Effectiveness of acupuncture as adjunctive therapy in osteoarthritis of the kneea randomized, controlled trial. Ann. Intern. Med. 2004, 141, 901–910. [Google Scholar] [CrossRef] [PubMed]
- Tukmachi, E.; Jubb, R.; Dempsey, E.; Jones, P. The effect of acupuncture on the symptoms of knee osteoarthritis-an open randomised controlled study. Acupunct. Med. 2004, 22, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Vas, J.; Méndez, C.; Perea-Milla, E.; Vega, E.; Panadero, M.D.; León, J.M.; Borge, M.Á.; Gaspar, O.; Sánchez-Rodríguez, F.; Aguilar, I. Acupuncture as a complementary therapy to the pharmacological treatment of osteoarthritis of the knee: Randomised controlled trial. BMJ 2004, 329, 1216. [Google Scholar] [CrossRef] [PubMed]
- Witt, C.; Brinkhaus, B.; Jena, S.; Linde, K.; Streng, A.; Wagenpfeil, S.; Hummelsberger, J.; Walther, H.; Melchart, D.; Willich, S. Acupuncture in patients with osteoarthritis of the knee: A randomised trial. Lancet 2005, 366, 136–143. [Google Scholar] [CrossRef]
- White, A.; Tough, L.; Eyre, V.; Vickery, J.; Asprey, A.; Quinn, C.; Warren, F.; Pritchard, C.; Foster, N.E.; Taylor, R.S.; et al. Western medical acupuncture in a group setting for knee osteoarthritis: Results of a pilot randomised controlled trial. Pilot Feasibility Stud. 2016, 2, 10. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, R.; Lumini-Oliveira, J.; Santos, M.J.; Ramos, B.; Machado, J.; Greten, H. Effect of acupuncture on delayed onset muscle soreness: Series of case studies. Exp. Pathol. Health Sci. 2016, 8, 85–92. [Google Scholar]
- Liu, Y.-H.; Wei, I.-P.; Wang, T.-M.; Lu, T.-W.; Lin, J.-G. Immediate effects of acupuncture treatment on intra-and inter-limb contributions to body support during gait in patients with bilateral medial knee osteoarthritis. Am. J. Chin. Med. 2017, 45, 23–35. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Session | Subject A | Subject B | ||
|---|---|---|---|---|
| Before | After | Before | After | |
| 1st | 45° | 90° | 90° | 110° |
| 2nd | 60° | 110° | 110° | 120° |
| 3rd | 90° | 140° | 110° | 130° |
| 4th | 110° | 155° | 125° | 140° |
| 5th | 140° | 160° | 130° | 155° |
| 6th | 155° | 160° | 140° | 155° |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teixeira, J.; Santos, M.J.; Matos, L.C.; Machado, J.P. Evaluation of the Effectiveness of Acupuncture in the Treatment of Knee Osteoarthritis: A Case Study. Medicines 2018, 5, 18. https://doi.org/10.3390/medicines5010018
Teixeira J, Santos MJ, Matos LC, Machado JP. Evaluation of the Effectiveness of Acupuncture in the Treatment of Knee Osteoarthritis: A Case Study. Medicines. 2018; 5(1):18. https://doi.org/10.3390/medicines5010018
Chicago/Turabian StyleTeixeira, Joana, Maria João Santos, Luís Carlos Matos, and Jorge Pereira Machado. 2018. "Evaluation of the Effectiveness of Acupuncture in the Treatment of Knee Osteoarthritis: A Case Study" Medicines 5, no. 1: 18. https://doi.org/10.3390/medicines5010018
APA StyleTeixeira, J., Santos, M. J., Matos, L. C., & Machado, J. P. (2018). Evaluation of the Effectiveness of Acupuncture in the Treatment of Knee Osteoarthritis: A Case Study. Medicines, 5(1), 18. https://doi.org/10.3390/medicines5010018