
BioMimics 3D Stent in Femoropopliteal Lesions: 3-Year Outcomes with Propensity Matching for Drug-Coated Balloons

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
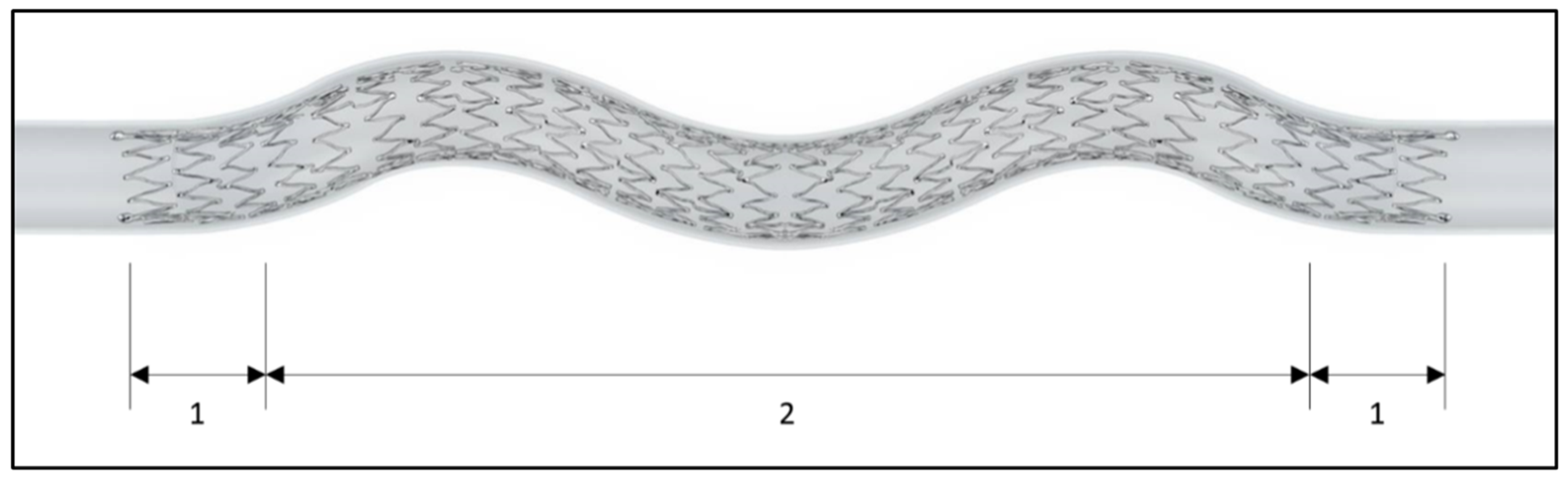
2.2. Study Device and Procedure
2.3. Endpoints and Definitions
2.4. Statistical Analysis
3. Results
Propensity-Matched Cohorts
4. Discussion
4.1. 3-Year Outcomes in the Overall Cohort
4.2. BioMimics 3D in Combination with DCB
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aboyans, V.; Ricco, J.B.; Bartelink, M.L.; Björck, M.; Brodmann, M.; Cohner, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [PubMed]
- Lichtenberg, M.; Zeller, T.; Gaines, P.; Piorkowski, M. BioMimics 3D vascular stent system for femoropopliteal interventions. Vasa 2022, 51, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, T.M.; Zeller, T.; Nakamura, M.; Gaines, P.A. Treatment of Femoropopliteal Lesions With the BioMimics 3D Vascular Stent System: Two-Year Results From the MIMICS-2 Trial. J. Endovasc. Ther. 2021, 28, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Zeller, T.; Gaines, P.A.; Ansel, G.M.; Caro, C.G. Helical Centerline Stent Improves Patency: Two-Year Results From the Randomized Mimics Trial. Circ. Cardiovasc. Interv. 2016, 9, e002930. [Google Scholar] [CrossRef] [PubMed]
- Caro, C.G.; Seneviratne, A.; Heraty, K.B.; Monaco, C.; Burke, M.G.; Krams, R.; Chang, C.C.; Coppola, G.; Gilson, P. Intimal hyperplasia following implantation of helical-centreline and straight-centreline stents in common carotid arteries in healthy pigs: Influence of intraluminal flow. J. R. Soc. Interface 2013, 10, 20130578. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, T.M.; Zeller, T.; Nakamura, M.; Caro, C.G.; Lichtenberg, M. Swirling Flow and Wall Shear: Evaluating the BioMimics 3D Helical Centerline Stent for the Femoropopliteal Segment. Int. J. Vasc. Med. 2018, 2018, 9795174. [Google Scholar] [CrossRef] [PubMed]
- Rits, J.; van Herwaarden, J.A.; Jahrome, A.K.; Krievins, D.; Moll, F.L. The incidence of arterial stent fractures with exclusion of coronary, aortic, and non-arterial settings. Eur. J. Vasc. Endovasc. Surg. 2008, 36, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Dake, M.D.; Ansel, G.M.; Jaff, M.R.; Ohki, T.; Saxon, R.R.; Smouse, H.B.; Machan, L.S.; Snyder, S.A.; O’leary, E.E.; Ragheb, A.O.; et al. Durable Clinical Effectiveness With Paclitaxel-Eluting Stents in the Femoropopliteal Artery: 5-Year Results of the Zilver PTX Randomized Trial. Circulation 2016, 133, 1472–1483. [Google Scholar] [CrossRef] [PubMed]
- Müller-Hülsbeck, S.; Keirse, K.; Zeller, T.; Schroë, H.; Diaz-Cartelle, J. Long-Term Results from the MAJESTIC Trial of the Eluvia Paclitaxel-Eluting Stent for Femoropopliteal Treatment: 3-Year Follow-up. Cardiovasc. Interv. Radiol. 2017, 40, 1832–1838. [Google Scholar] [CrossRef] [PubMed]
- Bausback, Y.; Wittig, T.; Schmidt, A.; Zeller, T.; Bosiers, M.; Peeters, P.; Brucks, S.; Lottes, A.E.; Scheinert, D.; Steiner, S. Drug-Eluting Stent Versus Drug-Coated Balloon Revascularization in Patients With Femoropopliteal Arterial Disease. J. Am. Coll. Cardiol. 2019, 73, 667–679. [Google Scholar] [CrossRef] [PubMed]
- Torsello, G.; Stavroulakis, K.; Brodmann, M.; Micari, A.; Tepe, G.; Veroux, P.; Benko, A.; Choi, D.; Vermassen, F.E.G.; Jaff, M.R.; et al. Three-Year Sustained Clinical Efficacy of Drug-Coated Balloon Angioplasty in a Real-World Femoropopliteal Cohort. J. Endovasc. Ther. 2020, 27, 693–705. [Google Scholar] [CrossRef] [PubMed]
- Shishehbor, M.H.; Schneider, P.A.; Zeller, T.; Razavi, M.K.; Laird, J.R.; Wang, H.; Tieché, C.; Parikh, S.A.; Iida, O.; Jaff, M.R. Total IN.PACT drug-coated balloon initiative reporting pooled imaging and propensity-matched cohorts. J. Vasc. Surg. 2019, 70, 1177–1191.e9. [Google Scholar] [CrossRef] [PubMed]
- Brodmann, M.; Lansink, W.; Guetl, K.; Micari, A.; Menk, J.; Zeller, T. Long-Term Outcomes of the 150 mm Drug-Coated Balloon Cohort from the IN.PACT Global Study. Cardiovasc. Interv. Radiol. 2022, 45, 1276–1287. [Google Scholar] [CrossRef] [PubMed]
- Thieme, M.; Von Bilderling, P.; Paetzel, C.; Karnabatidis, D.; Perez Delgado, J.; Lichtenberg, M.; Lutonix Global SFA Registry Investigators. The 24-Month Results of the Lutonix Global SFA Registry: Worldwide Experience with Lutonix Drug-Coated Balloon. JACC Cardiovasc. Interv. 2017, 10, 1682–1690. [Google Scholar] [CrossRef] [PubMed]
- Widder, J.D.; Cortese, B.; Levesque, S.; Berliner, D.; Eccleshall, S.; Graf, K.; Doutrelant, L.; Ahmed, J.; Bressollette, E.; Zavalloni, D.; et al. Coronary artery treatment with a urea-based paclitaxel-coated balloon: The European-wide FALCON all-comers DCB Registry (FALCON Registry). EuroIntervention 2019, 15, e382–e388. [Google Scholar] [CrossRef] [PubMed]
- Deloose, K.; Bosiers, M.; Peeters, P.; Verbist, J.; Maene, L.; Beelen, R.; Keirse, K.; Hendriks, J.; Lauwers, P.; Wauters, J.; et al. Combining the Passeo-18 Lux Drug-Coated Balloon and the Pulsar-18 Bare Metal Stent: 12- and 24-Month Outcomes of the BIOLUX 4EVER Investigator-Initiated Trial. J. Endovasc. Ther. 2020, 27, 936–945. [Google Scholar] [CrossRef]
- Lichtenberg, M.; Breuckmann, F.; Kramer, V.; Betge, S.; Sixt, S.; Hailer, B.; Nikol, S.; Arjumand, J.; Wittenberg, G.; Teßarek, J.; et al. Effectiveness of the Pulsar-18 self-expanding stent with optional drug-coated balloon angioplasty in the treatment of femoropopliteal lesions—The BIOFLEX PEACE All-Comers Registry. Vasa 2019, 48, 425–432. [Google Scholar] [CrossRef]
- Schmidt, A.; Piorkowski, M.; Görner, H.; Steiner, S.; Bausback, Y.; Scheinert, S.; Banning-Eichenseer, U.; Staab, H.; Branzan, D.; Varcoe, R.L.; et al. Drug-Coated Balloons for Complex Femoropopliteal Lesions: 2-Year Results of a Real-World Registry. JACC Cardiovasc. Interv. 2016, 9, 715–724. [Google Scholar] [CrossRef]
- Ansari, F.; Pack, L.K.; Brooks, S.S.; Morrison, T.M. Design considerations for studies of the biomechanical environment of the femoropopliteal arteries. J. Vasc. Surg. 2013, 58, 804–813. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Full Cohort | Propensity-Matched Cohort | |||
|---|---|---|---|---|
| Any DCB | No DCB | p-Value | ||
| N = 507 | N = 195 | N = 195 | ||
| Age (years) | 70.1 ± 10.0 | 70.4 ± 9.6 | 69.7 ± 10.0 | 0.419 |
| Male | 332/507 (65.5%) | 129/195 (66.2%) | 131/195 (67.2%) | 0.915 |
| CVA or TIA | 57/507 (11.2%) | 20/195 (10.3%) | 22/195 (11.3%) | 0.870 |
| Hypertension | 434/507 (85.6%) | 172/195 (88.2%) | 158/195 (81.0%) | 0.067 |
| Hypercholesterolemia/dyslipidemia | 324/507 (63.9%) | 131/195 (67.2%) | 129/195 (66.2%) | 0.915 |
| Coronary artery disease | 51/507 (10.1%) | 19/195 (9.7%) | 23/195 (11.8%) | 0.625 |
| Smoking | 345/507 (68.0%) | 130/195 (66.7%) | 136/195 (69.7%) | 0.587 |
| Current | 191/507 (37.7%) | 71/195 (36.4%) | 76/195 (39.0%) | 0.676 |
| Diabetes mellitus | 187/507 (36.9%) | 76/195 (39.0%) | 73/195 (37.4%) | 0.835 |
| Insulin | 82/507 (16.2%) | 24/195 (12.3%) | 34/195 (17.4%) | 0.200 |
| Renal insufficiency | 42/507 (8.3%) | 13/195 (6.7%) | 17/195 (8.7%) | 0.569 |
| Dialysis | 10/507 (2.0%) | 3/195 (1.5%) | 5/195 (2.6%) | 0.724 |
| Non-healing wound on the target limb | 73/507 (14.4%) | 22/195 (11.3%) | 30/195 (15.4%) | 0.297 |
| Full Cohort | Propensity-Matched Cohort | |||
|---|---|---|---|---|
| Any DCB | No DCB | p-Value | ||
| N = 518 Lesions | N = 202 Lesions | N = 198 Lesions | ||
| Target Lesion Type | ||||
| De novo | 467/518 (90.2%) | 183/202 (90.6%) | 177/198 (89.4%) | 0.741 |
| Restenotic | 51/518 (9.8%) | 19/202 (9.4%) | 21/198 (10.6%) | 0.741 |
| Maximal RVD (mm) | 5.5 ± 0.7 | 5.4 ± 0.6 (202) | 5.4 ± 0.7 (198) | 0.760 |
| Lesion length (mm) | 125.9 ± 91.0 | 123.6 ± 93.7 (202) | 124.7 ± 86.6 (198) | 0.402 |
| Diameter stenosis (%) | 94.6 ± 8.0 | 95.2 ± 7.2 (202) | 94.2 ± 8.1 (198) | 0.318 |
| Occlusion | 294/518 (56.8%) | 119/202 (58.9%) | 110/198 (55.6%) | 0.545 |
| Calcification | ||||
| Grade 0 (no visible calcium) | 91/516 (17.6%) | 41/202 (20.3%) | 29/197 (14.7%) | 0.150 |
| Grade 1 (unilateral, <5 cm) | 152/516 (29.5%) | 68/202 (33.7%) | 53/197 (26.9%) | 0.157 |
| Grade 2 (unilateral, ≥5 cm) | 125/516 (24.4%) | 48/202 (23.8%) | 48/197 (24.4%) | 0.907 |
| Grade 3 (bilateral, <5 cm) | 76/516 (14.7%) | 29/202 (14.4%) | 29/197 (14.7%) | 1.0000 |
| Grade 4 (bilateral, ≥5 cm) | 71/516 (13.8%) | 16/202 (7.9%) | 38/197 (19.3%) | 0.001 |
| Full Cohort | Propensity-Matched Cohort | |||
|---|---|---|---|---|
| Any DCB | No DCB | p-Value | ||
| N = 507 Patients | N = 195 Patients | N = 195 Patients | ||
| N = 518 Lesions | N = 202 Lesions | N = 198 Lesions | ||
| Procedure time (min) | 74.6 ± 48.8 | 74.3 ± 51.0 (194) | 74.2 ± 50.3 (194) | 0.621 |
| Total fluoroscopy time (min) | 14.9 ± 11.1 | 15.4 ± 10.8 | 14.6 ± 12.3 | 0.09 |
| Total amount of contrast (mL) | 111.8 ± 60.2 | 135.7 ± 61.2 (194) | 90.9 ± 49.4 (193) | <0.0001 |
| Guide wire size (inch) | ||||
| 0.035 | 269/507 (53.1%) | 92/195 (47.2%) | 122/195 (62.6%) | 0.003 |
| 0.018 | 209/507 (41.2%) | 88/195 (45.1%) | 69/195 (35.4%) | 0.063 |
| 0.014 | 29/507 (5.7%) | 15/195 (7.7%) | 4/195 (2.1%) | 0.017 |
| Number of BioMimics stent deployed | ||||
| 1 | 395/518 (76.3%) | 153/202 (75.7%) | 148/198 (74.7%) | 0.908 |
| 2 | 96/518 (18.5%) | 38/202 (18.8%) | 41/198 (20.7%) | 0.707 |
| 3 | 19/518 (3.7%) | 8/202 (4.0%) | 6/198 (3.0%) | 0.787 |
| 4 | 8/518 (1.5%) | 3/202 (1.5%) | 3/198 (1.5%) | 1.000 |
| Total stented length | 131.2 ± 80.1 | 128.3 ± 80.9 (202) | 132.2 ± 79.2 (198) | 0.262 |
| Spot-stenting (in any lesion) * | 74/507 (14.6%) | 31/195 (15.9%) | 22/195 (11.3%) | 0.237 |
| Total stent length spot-stenting (mm) | 114.0 ± 52.1 | 106.8 ± 56.1 | 117.7 ± 52.4 | |
| No patent infrapopliteal vessel | 22/507 (4.3%) | 7/195 (3.6%) | 11/195 (5.6%) | 0.470 |
| PTA balloon | ||||
| Pre-dilatation | 454/518 (87.6%) | 188/202 (93.1%) | 167/198 (84.3%) | 0.007 |
| Post-dilatation | 353/518 (68.1%) | 77/202 (38.1%) | 185/198 (93.4%) | <0.0001 |
| DCB | ||||
| Pre-BioMimics stent placement | 123/518 (23.7%) | 94/202 (46.5%) | - | - |
| Post-BioMimics stent placement | 137/518 (26.4%) | 113/202 (55.9%) | - | - |
| Full Cohort | Propensity-Matched Cohort | |||
|---|---|---|---|---|
| Any DCB | No DCB | Log-Rank | ||
| p-Value | ||||
| 12-month follow-up (day 365) | - | |||
| Survival | 93.9% [91.8; 96.1] | 94.1% [90.8; 97.5] | 95.6% [92.6; 98.6] | - |
| Freedom from major amputation | 98.5% [97.3; 99.6] | 99.4% [98.3; 100] | 97.2% [94.8; 99.6] | - |
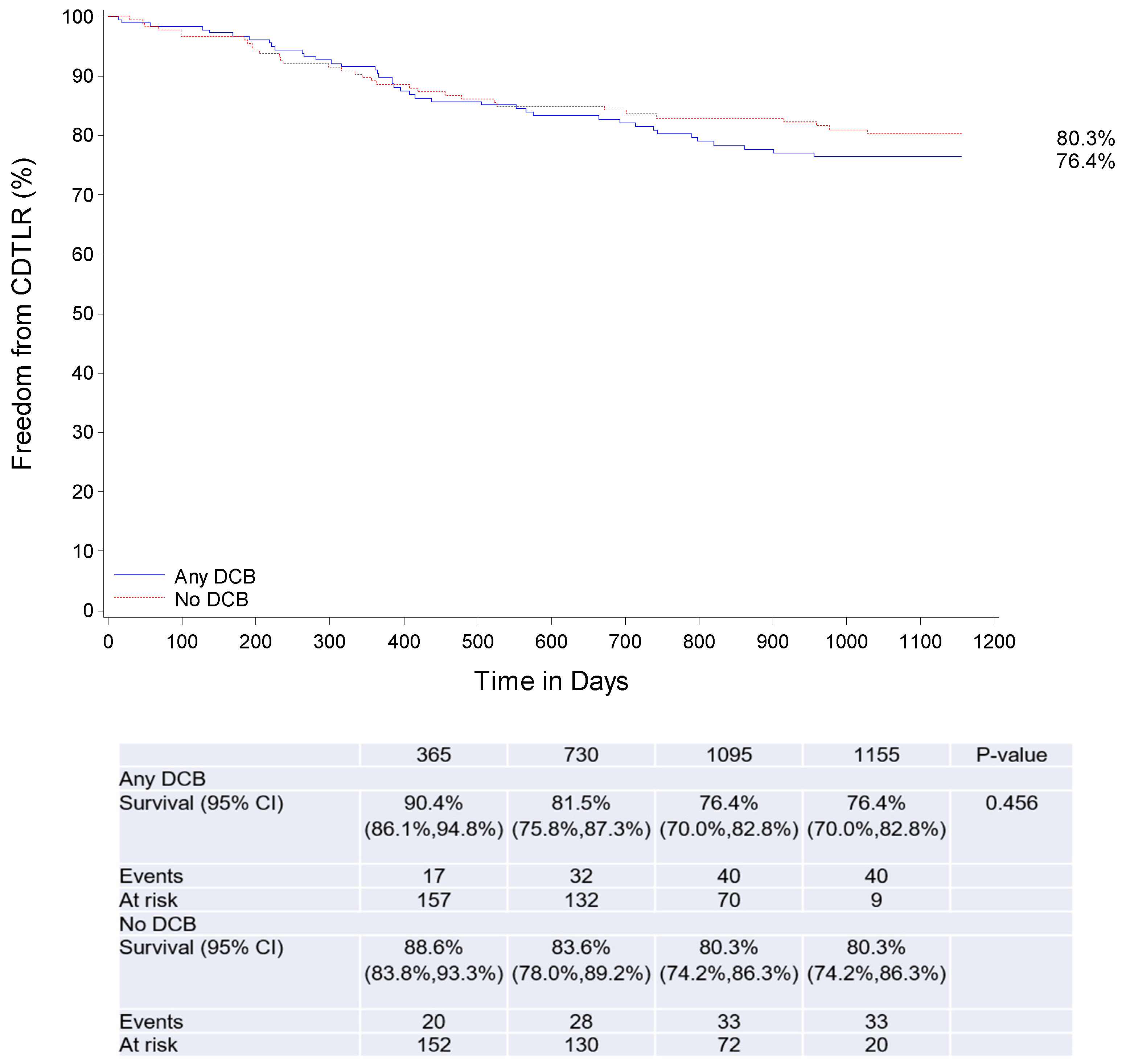
| Freedom from CD-TLR | 90.0% [87.3; 92.8] | 90.4% [86.1; 94.8] | 88.6% [83.8; 93.3] | - |
| Primary patency | 87.2% [84.1; 90.2] | 89.9% [85.4; 94.3] | 86.3% [81.2; 91.4%] | - |
| 36-month follow-up (day 1095) | ||||
| Survival | 85.4% [82.2; 88.7] | 87.9% [83.1; 92.6] | 85.1% [79.7; 90.4] | 0.411 |
| Freedom from major amputation | 98.5% [97.3; 99.6] | 99.4% [98.3; 100] | 97.2% [94.8; 99.6] | 0.097 |
| Freedom from CD-TLR | 78.0% [74.1; 81.9] | 76.4% [70.0; 82.8] | 80.3% [74.2; 86.3] | 0.456 |
| Primary patency | 70.2% [65.8; 74.6] | 68.5% [61.3; 75.7] | 74.4% [67.6; 81.2] | 0.287 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piorkowski, M.; Zeller, T.; Rammos, C.; Deloose, K.; Hertting, K.; Sesselmann, V.; Tepe, G.; Gaines, P.; Lichtenberg, M. BioMimics 3D Stent in Femoropopliteal Lesions: 3-Year Outcomes with Propensity Matching for Drug-Coated Balloons. J. Cardiovasc. Dev. Dis. 2023, 10, 126. https://doi.org/10.3390/jcdd10030126
Piorkowski M, Zeller T, Rammos C, Deloose K, Hertting K, Sesselmann V, Tepe G, Gaines P, Lichtenberg M. BioMimics 3D Stent in Femoropopliteal Lesions: 3-Year Outcomes with Propensity Matching for Drug-Coated Balloons. Journal of Cardiovascular Development and Disease. 2023; 10(3):126. https://doi.org/10.3390/jcdd10030126
Chicago/Turabian StylePiorkowski, Michael, Thomas Zeller, Christos Rammos, Koen Deloose, Klaus Hertting, Volker Sesselmann, Gunnar Tepe, Peter Gaines, and Michael Lichtenberg. 2023. "BioMimics 3D Stent in Femoropopliteal Lesions: 3-Year Outcomes with Propensity Matching for Drug-Coated Balloons" Journal of Cardiovascular Development and Disease 10, no. 3: 126. https://doi.org/10.3390/jcdd10030126
APA StylePiorkowski, M., Zeller, T., Rammos, C., Deloose, K., Hertting, K., Sesselmann, V., Tepe, G., Gaines, P., & Lichtenberg, M. (2023). BioMimics 3D Stent in Femoropopliteal Lesions: 3-Year Outcomes with Propensity Matching for Drug-Coated Balloons. Journal of Cardiovascular Development and Disease, 10(3), 126. https://doi.org/10.3390/jcdd10030126