
An All-in-One Tool for 2D Atherosclerotic Disease Assessment and 3D Coronary Artery Reconstruction
 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
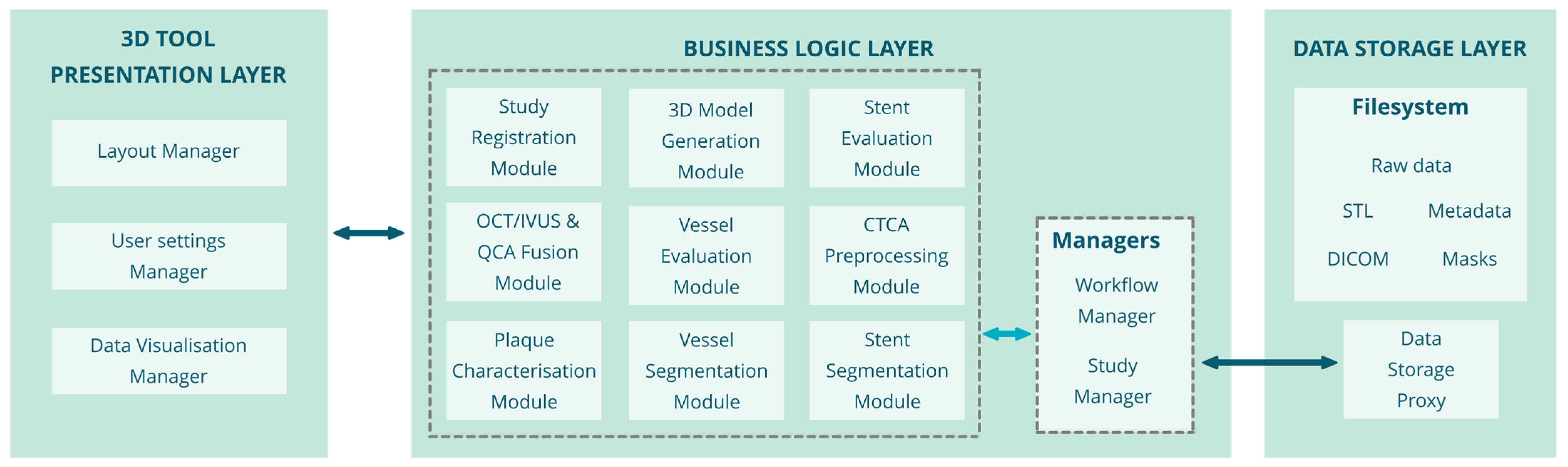
2.1. Architecture
2.2. Modules
- Input: CT DICOM images.
- Output: processed CT DICOM images using the Vesselness filter [2].
- Input: The user inputs depend on the imaging modality (CTCA and CA case: starting and ending points of segment, OCT/IVUS case: lumen and adventitia borders), imaging data in DICOM format.
- Output: OCT, IVUS, CTCA: Vessel lumen and wall, calcified and non-calcified plaque segmentation masks; CA: Lumen and centerline path.
- Input: Segmentation masks of the lumen, adventitia and plaques, 3D centerline path.
- Output: Lumen area and perimeter, outer wall area and perimeter, plaque burden.
- Input: The required input is the masks of the lumen and outer wall borders.
- Output: OCT, IVUS: plaque segmentation masks, 3D point clouds, 3D surfaces of calcified plaques, metrics of plaque area, angle; CTCA: calcified and non-calcified plaques segmentation masks, 3D objects, volumes, areas of the calcified and non-calcified plaques.
- Input: Segmentation masks of the lumen, adventitia and plaques, 3D centerline path, 3D stent transformed point cloud.
- Output: 3D models of the vessel, plaques and stent.
- Input: 3D centerline path, 3D geometries of the vessel, plaques, and stent.
- Output: Co-registered 3D models.
- Input: Imaging data (DICOM series of the OCT/IVUS pullback), user input (manual annotations-corrections of detected stent struts).
- Output: Strut point cloud, metrics of struts (number of struts, malapposed struts, in-stent restenosis).
- Input: 3D centerline points, segmented borders of the lumen and wall, strut point cloud.
- Output: Vessel lumen, wall, plaque lesions and strut point cloud in 3D space.
- Input: Strut point cloud, reconstructed 3D stent model.
- Output: Stent evaluation metrics (Stent CSA, minimum/maximum stent diameter, strut malapposition distance, % of unapposed struts, restenosis burden, fracture detection)
- Input: DICOM images, 3D models of the vessel, plaques and stent Vessel/plaque/stent evaluation metrics.
- Output: 3D rendering, 2D plots, visualization of the data.
2.3. User Interfaces
2.4. Algorithms
OCT Analysis
2.5. IVUS Analysis
2.6. QCA Analysis
2.7. CTCA Analysis
3. Results
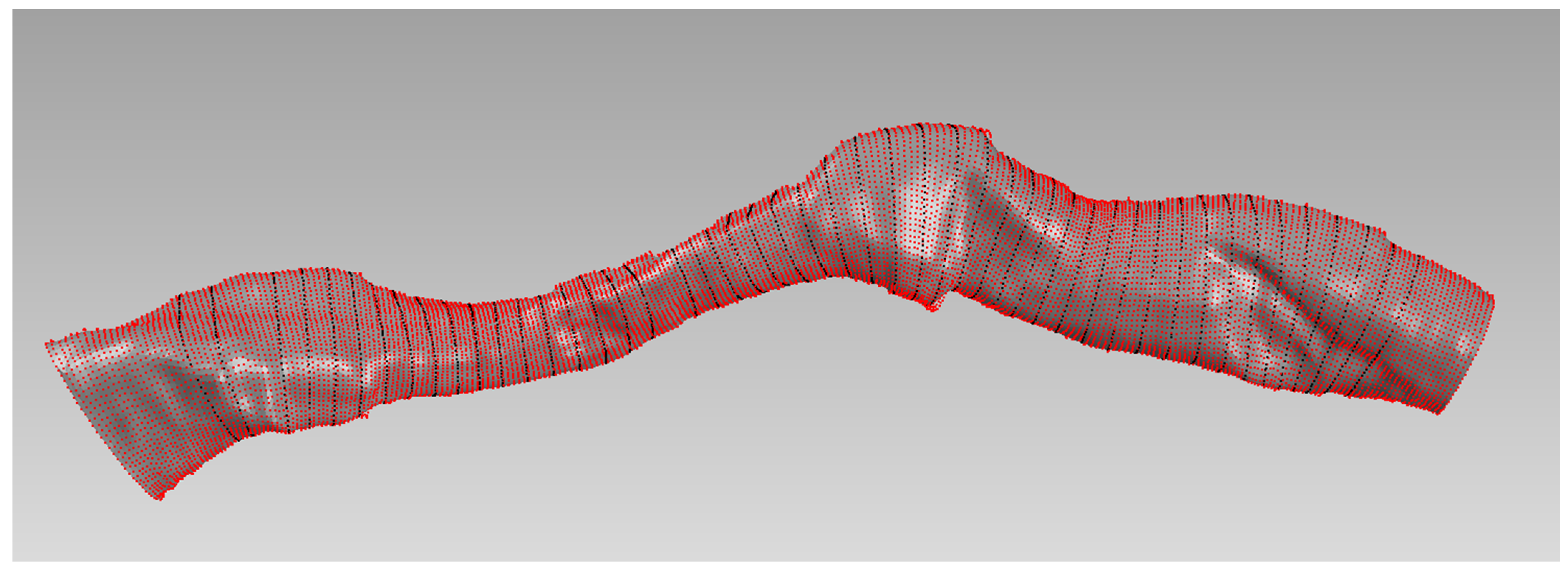
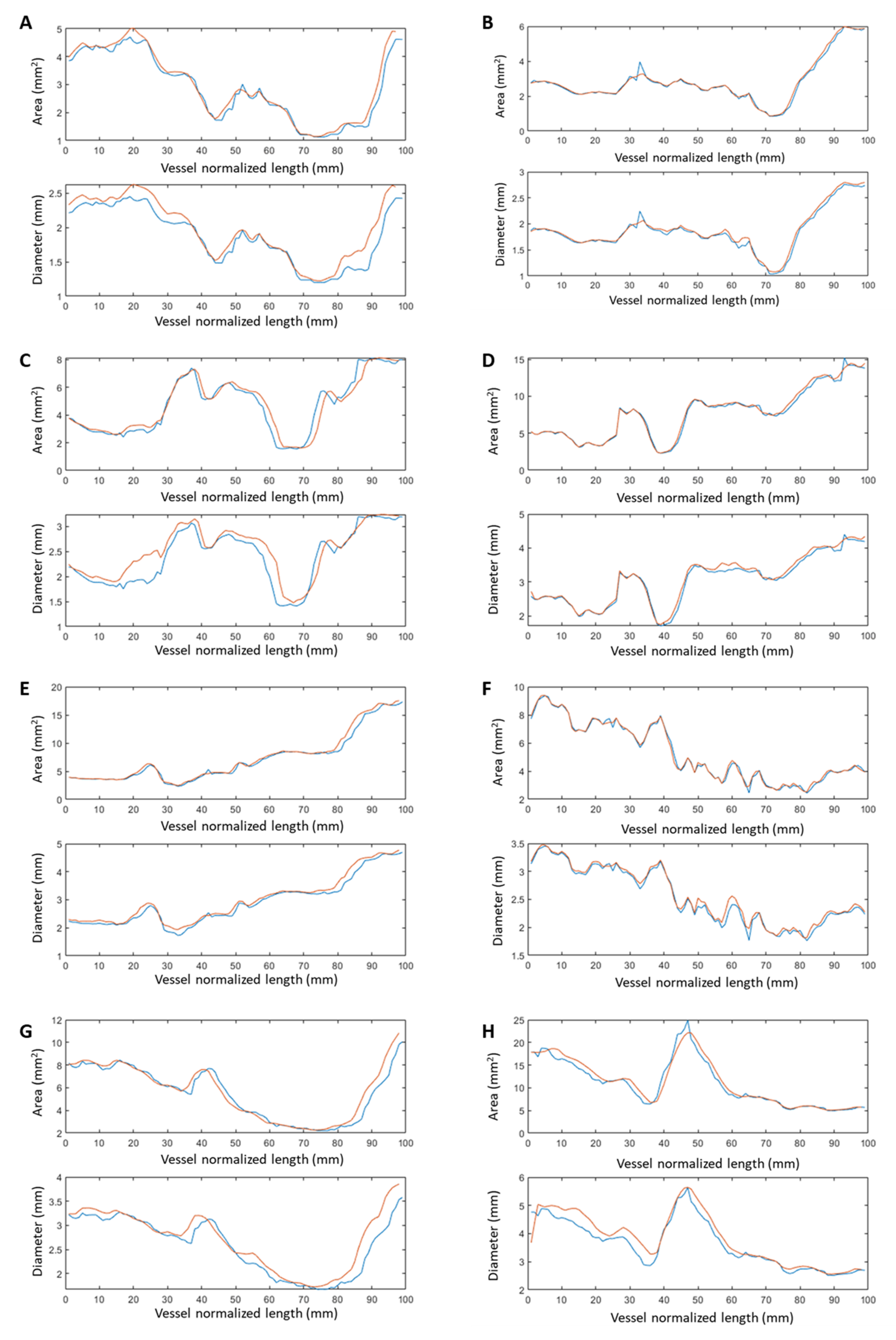
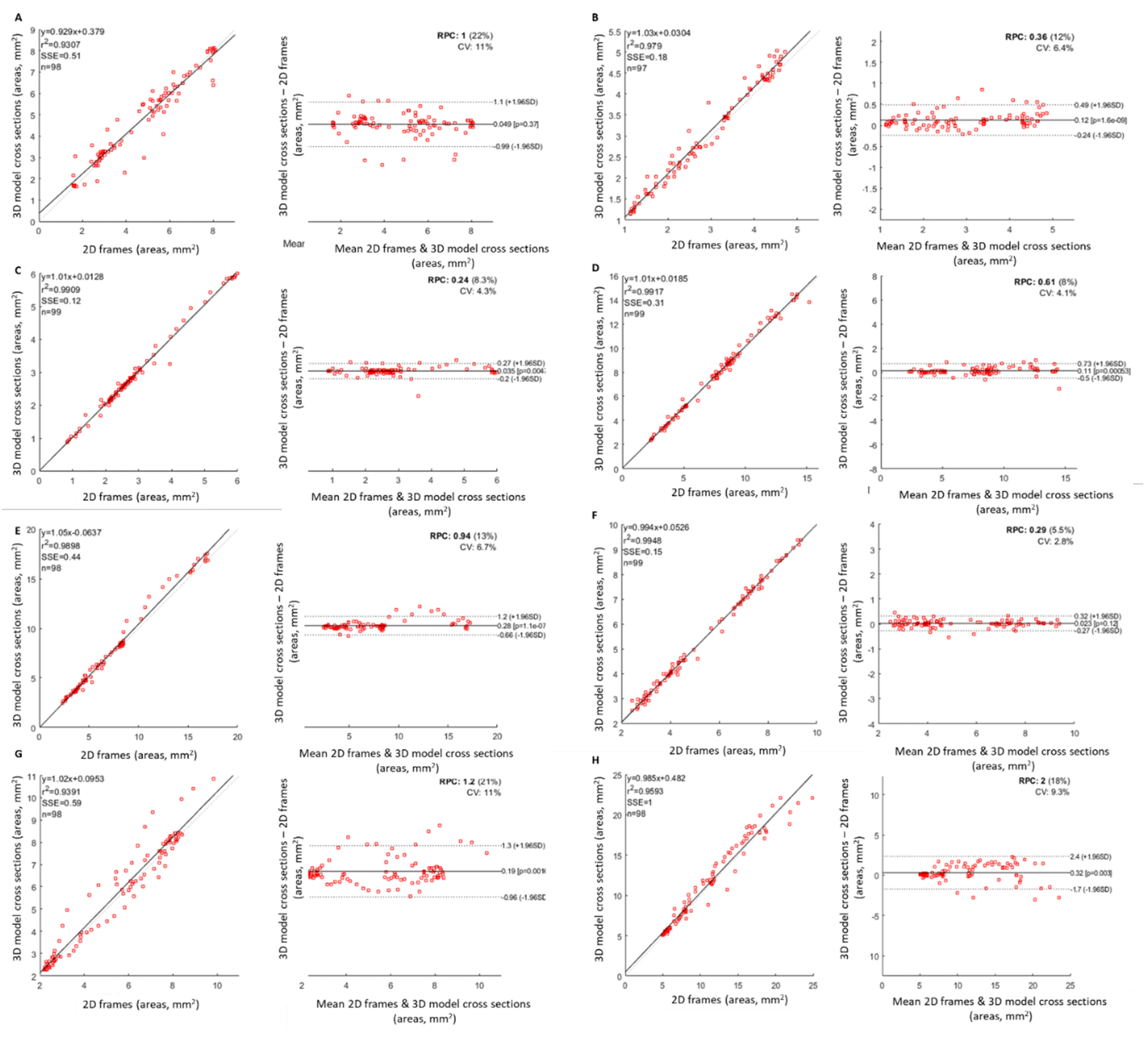
3.1. D Fusion Evaluation
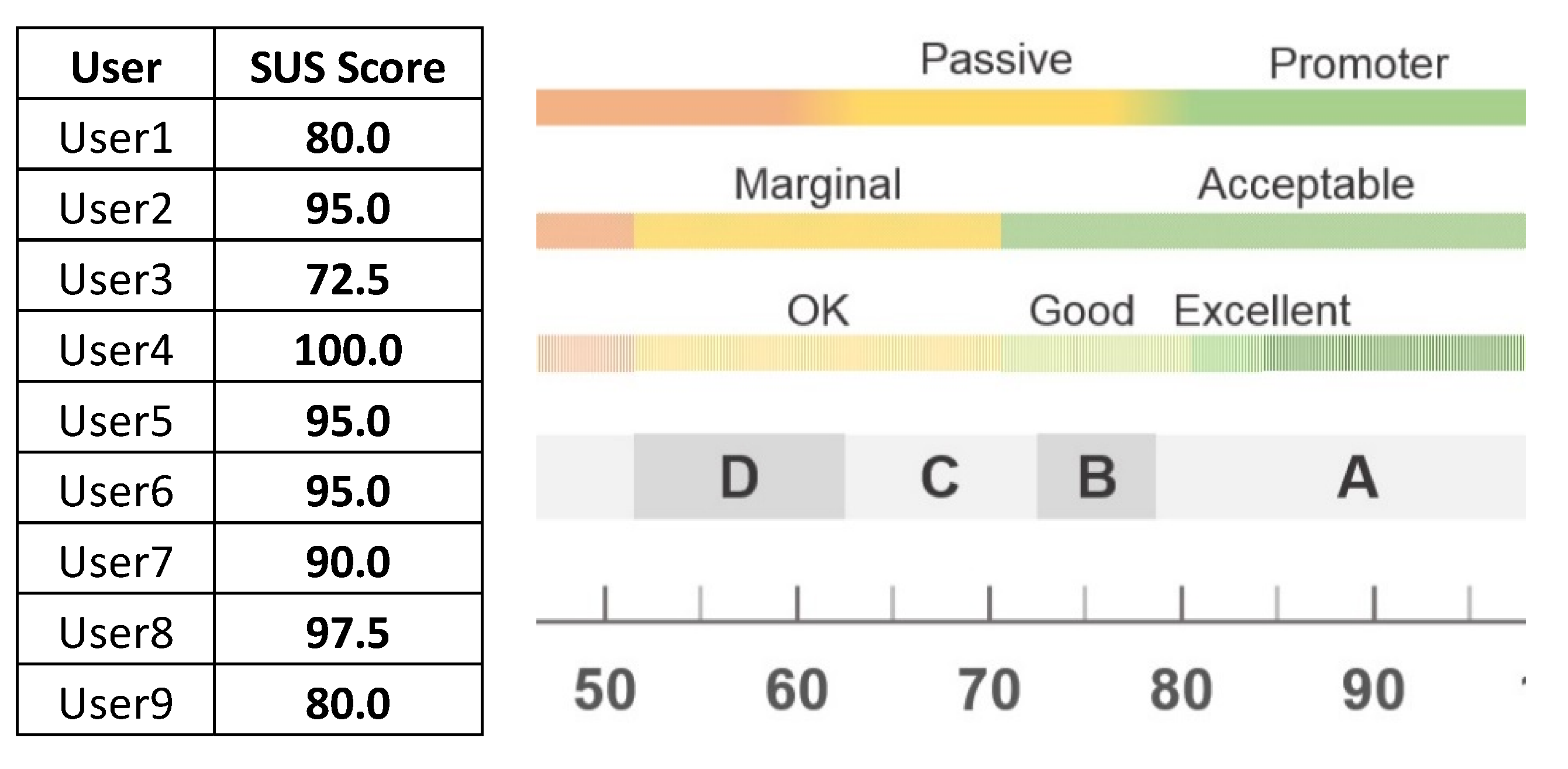
3.2. Usability Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sakellarios, A.I.; Rigas, G.; Kigka, V.; Siogkas, P.; Tsompou, P.; Karanasiou, G.; Exarchos, T.; Andrikos, I.; Tachos, N.; Pelosi, G.; et al. SMARTool: A Tool for Clinical Decision Support for the Management of Patients with Coronary Artery Disease Based on Modeling of Atherosclerotic Plaque Process. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, South Korea, 11–15 July 2017; pp. 96–99. [Google Scholar]
- Frangi, A.F.; Niessen, W.J.; Vincken, K.L.; Viergever, M.A. Multiscale Vessel Enhancement Filtering; Springer: Berlin/Heidelberg, Germany, 1998; Volume 1496, pp. 130–137. [Google Scholar] [CrossRef] [Green Version]
- Dicom.Offis.de-DICOM Software Made by OFFIS-DCMTK-DICOM Toolkit. OFFIS: Oldenburg, Germany. Available online: https://dicom.offis.de/dcmtk.php.en (accessed on 18 May 2021).
- McCormick, M.; Liu, X.; Jomier, J.; Marion, C.; Ibanez, L. ITK: Enabling Reproducible Research and Open Science. Front. Neuroinformatics 2014, 8, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emgu CV: OpenCV in. NET (C#, VB, C++ and More). Available online: https://www.emgu.com/wiki/index.php/Main_Page (accessed on 18 May 2021).
- Home. Available online: https://opencv.org/ (accessed on 18 May 2021).
- Schroeder, W.; Martin, K.; Lorensen, B. The Visualization Toolkit, 4th ed.; VTK-The Visualization Toolkit; Kitware Inc.: New York, NY, USA, 2006; ISBN 978-1-930934-19-1. [Google Scholar]
- Vmtk-the Vascular Modelling Toolkit. Available online: http://www.vmtk.org/index.html (accessed on 16 March 2023).
- Keras-Team/Keras 2021. Available online: https://github.com/tensorflow/tensorflow/releases/tag/v2.12.0-rc0 (accessed on 16 March 2023).
- Wang, A.; Tang, X. Automatic Segmentation of Vessel Lumen in Intravascular Optical Coherence Tomography Images. In Proceedings of the 2016 IEEE International Conference on Mechatronics and Automation, Harbin, China, 7–10 August 2016; pp. 948–953. [Google Scholar]
- Ester, M.; Kriegel, H.-P.; Sander, J.; Xu, X. A Density-Based Algorithm for Discovering Clusters in Large Spatial Databases with Noise. In Proceedings of the KDD, Portland, ON, USA, 2–4 August 1996; AAAI Press: Portland, ON, USA, 1996. [Google Scholar]
- Amrute, J.M.; Athanasiou, L.S.; Rikhtegar, F.; de la Torre Hernández, J.M.; Camarero, T.G.; Edelman, E.R. Polymeric Endovascular Strut and Lumen Detection Algorithm for Intracoronary Optical Coherence Tomography Images. J. Biomed. Opt. 2018, 23, 1. [Google Scholar] [CrossRef] [PubMed]
- Siogkas, P.K.; Stefanou, K.A.; Athanasiou, L.S.; Papafaklis, M.I.; Michalis, L.K.; Fotiadis, D.I. Art Care: A Multi-Modality Coronary 3D Reconstruction and Hemodynamic Status Assessment Software. Technol. Health Care 2018, 26, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Andrikos, I.O.; Sakellarios, A.I.; Siogkas, P.K.; Tsompou, P.I.; Kigka, V.I.; Michalis, L.K.; Fotiadis, D.I. A Novel Method for 3D Reconstruction of Coronary Bifurcation Using Quantitative Coronary Angiography. In Proceedings of the World Congress on Medical Physics and Biomedical Engineering 2018, Prague, Czech Republic, 3–8 June 2018; Lhotska, L., Sukupova, L., Lacković, I., Ibbott, G.S., Eds.; Springer: Singapore, 2019; pp. 191–195. [Google Scholar]
- Temov, K.; Sun, Z. Coronary Computed Tomography Angiography Investigation of the Association between Left Main Coronary Artery Bifurcation Angle and Risk Factors of Coronary Artery Disease. Int. J. Cardiovasc. Imaging 2016, 32 (Suppl. 1), 129–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panetta, D.; Pelosi, G.; Viglione, F.; Kusmic, C.; Terreni, M.; Belcari, N.; Guerra, A.D.; Athanasiou, L.; Exarchos, T.; Fotiadis, D.I.; et al. Quantitative Micro-CT Based Coronary Artery Profiling Using Interactive Local Thresholding and Cylindrical Coordinates. Technol. Health Care Off. J. Eur. Soc. Eng. Med. 2015, 23, 557–570. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Wingert, A.; Wang, J.; Zhang, J.; Wang, X.; Sun, J.; Chen, F.; Khalid, S.G.; Jiang, J.; Zheng, D. Extraction of Coronary Atherosclerotic Plaques from Computed Tomography Imaging: A Review of Recent Methods. Front. Cardiovasc. Med. 2021, 8, 597568. [Google Scholar] [CrossRef] [PubMed]
- Kigka, V.I.; Sakellarios, A.; Rigas, G.; Tsobou, P.; Andrikos, I.O.; Michalis, L.K.; Fotiadis, D.I. A Three-Dimensional Quantification of Calcified and Non-Calcified Plaque Based on Computed Tomography Coronary Angiography Images: Comparison with Virtual Histology Intravascular Ultrasound. In Proceedings of the World Congress on Medical Physics and Biomedical Engineering, Prague, Czech Republic, 3–8 June 2018; Lhotska, L., Sukupova, L., Lacković, I., Ibbott, G.S., Eds.; Springer: Singapore, 2019; pp. 207–211. [Google Scholar]
- Kigka, V.I.; Rigas, G.; Sakellarios, A.; Siogkas, P.; Andrikos, I.O.; Exarchos, T.P.; Loggitsi, D.; Anagnostopoulos, C.D.; Michalis, L.K.; Neglia, D.; et al. 3D Reconstruction of Coronary Arteries and Atherosclerotic Plaques Based on Computed Tomography Angiography Images. Biomed. Signal Process. Control 2018, 40, 286–294. [Google Scholar] [CrossRef] [Green Version]
- Kigka, V.I.; Sakellarios, A.; Kyriakidis, S.; Rigas, G.; Athanasiou, L.; Siogkas, P.; Tsompou, P.; Loggitsi, D.; Benz, D.C.; Buechel, R.; et al. A Three-Dimensional Quantification of Calcified and Non-Calcified Plaques in Coronary Arteries Based on Computed Tomography Coronary Angiography Images: Comparison with Expert’s Annotations and Virtual Histology Intravascular Ultrasound. Comput. Biol. Med. 2019, 113, 103409. [Google Scholar] [CrossRef] [PubMed]
- Kyriakidis, S.; Sakellarios, A.; Karanasiou, G.; Fotiadis, D.I. A Novel Methodology for Detection of Lumen, Outer Wall, Plaques and Stent Struts in Coronary Arteries Using Optical Coherence Tomography. In Proceedings of the 2019 IEEE 19th International Conference on Bioinformatics and Bioengineering (BIBE), Athens, Greece, 28–30 October 2019; pp. 697–701. [Google Scholar]
- Karanasiou, G.S.; Rigas, G.A.; Kyriakidis, S.K.; Tachos, N.S.; Sakellarios, A.I.; Fotiadis, D.I. InSilc: 3D Reconstruction and Plaque Characterization Tool. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. IEEE Eng. Med. Biol. Soc. Annu. Int. Conf. 2018, 2018, 4528–4531. [Google Scholar] [CrossRef] [Green Version]
- Affairs, A.S. For P. System Usability Scale (SUS). Available online: System-usability-scale.html (accessed on 12 April 2021).
- Sakellarios, A.I.; Tsompou, P.; Kigka, V.; Siogkas, P.; Kyriakidis, S.; Tachos, N.; Karanasiou, G.; Scholte, A.; Clemente, A.; Neglia, D.; et al. Non-Invasive Prediction of Site-Specific Coronary Atherosclerotic Plaque Progression Using Lipidomics, Blood Flow, and LDL Transport Modeling. Appl. Sci. 2021, 11, 1976. [Google Scholar] [CrossRef]
- Pleouras, D.S.; Sakellarios, A.I.; Tsompou, P.; Kigka, V.; Kyriakidis, S.; Rocchiccioli, S.; Neglia, D.; Knuuti, J.; Pelosi, G.; Michalis, L.K.; et al. Simulation of Atherosclerotic Plaque Growth Using Computational Biomechanics and Patient-Specific Data. Sci. Rep. 2020, 10, 17409. [Google Scholar] [CrossRef] [PubMed]
- Siogkas, P.K.; Anagnostopoulos, C.D.; Liga, R.; Exarchos, T.P.; Sakellarios, A.I.; Rigas, G.; Scholte, A.; Papafaklis, M.I.; Loggitsi, D.; Pelosi, G.; et al. Noninvasive CT-Based Hemodynamic Assessment of Coronary Lesions Derived from Fast Computational Analysis: A Comparison against Fractional Flow Reserve. Eur. Radiol. 2018, 29, 2117–2126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siogkas, P.K.; Lakkas, L.; Sakellarios, A.I.; Rigas, G.; Kyriakidis, S.; Stefanou, K.A.; Anagnostopoulos, C.D.; Clemente, A.; Rocchiccioli, S.; Pelosi, G.; et al. SmartFFR, a New Functional Index of Coronary Stenosis: Comparison with Invasive FFR Data. Front. Cardiovasc. Med. 2021, 8, 714471. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | 30% under 30 years old, 56% 30–39 years old, 11% over 40 years old |
| Experience | 37% less than 2 years, 37% 2 to 5 years, 13% 6–10 years, 13% 11 to 15 years |
| Profession | 44% Cardiologists/radiologists, 56% stent industry, researchers, CROs |
| Computer use | 75% everyday, 25% all the time |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kyriakidis, S.; Rigas, G.; Kigka, V.; Zaridis, D.; Karanasiou, G.; Tsompou, P.; Karanasiou, G.; Lakkas, L.; Nikopoulos, S.; Naka, K.K.; et al. An All-in-One Tool for 2D Atherosclerotic Disease Assessment and 3D Coronary Artery Reconstruction. J. Cardiovasc. Dev. Dis. 2023, 10, 130. https://doi.org/10.3390/jcdd10030130
Kyriakidis S, Rigas G, Kigka V, Zaridis D, Karanasiou G, Tsompou P, Karanasiou G, Lakkas L, Nikopoulos S, Naka KK, et al. An All-in-One Tool for 2D Atherosclerotic Disease Assessment and 3D Coronary Artery Reconstruction. Journal of Cardiovascular Development and Disease. 2023; 10(3):130. https://doi.org/10.3390/jcdd10030130
Chicago/Turabian StyleKyriakidis, Savvas, George Rigas, Vassiliki Kigka, Dimitris Zaridis, Georgia Karanasiou, Panagiota Tsompou, Gianna Karanasiou, Lampros Lakkas, Sotirios Nikopoulos, Katerina K. Naka, and et al. 2023. "An All-in-One Tool for 2D Atherosclerotic Disease Assessment and 3D Coronary Artery Reconstruction" Journal of Cardiovascular Development and Disease 10, no. 3: 130. https://doi.org/10.3390/jcdd10030130
APA StyleKyriakidis, S., Rigas, G., Kigka, V., Zaridis, D., Karanasiou, G., Tsompou, P., Karanasiou, G., Lakkas, L., Nikopoulos, S., Naka, K. K., Michalis, L. K., Fotiadis, D. I., & Sakellarios, A. I. (2023). An All-in-One Tool for 2D Atherosclerotic Disease Assessment and 3D Coronary Artery Reconstruction. Journal of Cardiovascular Development and Disease, 10(3), 130. https://doi.org/10.3390/jcdd10030130