
Sex-Based Difference in Aortic Dissection Outcomes: A Multicenter Study
 ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Oversight, Patient Population, Definitions, and Outcomes
2.2. Patients and Outcomes
2.3. Surgical Technique
2.4. Statistical Analysis
3. Results
3.1. Baseline
3.2. Postoperative Results
3.3. Subgroup Analysis: Predictors of Operative Mortality in Female Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pape, L.A.; Awais, M.; Woznicki, E.M.; Suzuki, T.; Trimarchi, S.; Evangelista, A.; Myrmel, T.; Larsen, M.; Harris, K.M.; Greason, K.; et al. Presentation, diagnosis, and outcomes of acute aortic dissection: 17-year trends from the international registry of acute aortic dissection. J. Am. Coll. Cardiol. 2015, 66, 350–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geirsson, A.; Shioda, K.; Olsson, C.; Ahlsson, A.; Gunn, J.; Hansson, E.C.; Hjortdal, V.; Jeppsson, A.; Mennander, A.; Wickbom, A.; et al. Differential outcomes of open and clamp-on distal anastomosis techniques in acute type A aortic dissection. J. Thorac. Cardiovasc. Surg. 2019, 157, 1750. [Google Scholar] [CrossRef] [PubMed]
- Czerny, M.; Schoenhoff, F.; Etz, C.; Englberger, L.; Khaladj, N.; Zierer, A.; Weigang, E.; Hoffmann, I.; Blettner, M.; Carrel, T.P. The impact of pre-operative malperfusion on outcome in acute type A aortic dissection: Results from the GERAADA Registry. J. Am. Coll. Cardiol. 2015, 65, 2628–2635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evangelista, A.; Isselbacher, E.M.; Bossone, E.; Gleason, T.G.; Di Eusanio, M.; Sechtem, U.; Ehrlich, M.P.; Trimarchi, S.; Braverman, A.C.; Myrmel, T.; et al. Insights from the International Registry of Acute Aortic Dissection: A 20-year experience of collaborative clinical research. Circulation 2018, 137, 1846–1860. [Google Scholar] [CrossRef]
- Fukui, T.; Tabata, M.; Morita, S.; Takanashi, S. Gender Differences in Patients Undergoing Surgery for Acute Type A Aortic Dissection. J. Thorac. Cardiovasc. Surg. 2015, 150, 581–587.e1. [Google Scholar] [CrossRef]
- Conway, B.D.; Stamou, S.C.; Kouchoukos, N.T.; Lobdell, K.W.; Hagberg, R.C. Effects of Gender on Outcomes and Survival Following Repair of Acute Type a Aortic Dissection. Int. J. Angiol. 2015, 24, 93–98. [Google Scholar] [CrossRef] [Green Version]
- Rylski, B.; Georgieva, N.; Beyersdorf, F.; Busch, C.; Boening, A.; Haunschild, J.; Etz, C.D.; Luehr, M.; Kallenbach, K. German Registry for Acute Aortic Dissection Type a Working Group of the German Society of Thoracic, Cardiac, and Vascular Surgery. Gender-Related Differences in Patients with Acute Aortic Dissection Type A. J. Thorac. Cardiovasc. Surg. 2021, 162, 528–535.e1. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Asai, T.; Kinoshita, T. Clinical Differences between Men and Women Undergoing Surgery for Acute Type A Aortic Dissection. Interact. Cardiovasc. Thorac. Surg. 2018, 26, 944–950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nienaber, C.A.; Fattori, R.; Mehta, R.H.; Richartz, B.M.; Evangelista, A.; Petzsch, M.; Cooper, J.V.; Januzzi, J.L.; Ince, H.; Sechtem, U.; et al. Gender-Related Differences in Acute Aortic Dissection. Circulation 2004, 109, 3014–3021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, T.C.; Kon, Z.; Cheema, F.H.; Grau-Sepulveda, M.V.; Englum, B.; Kim, S.; Chaudhuri, P.S.; Thourani, V.H.; Ailawadi, G.; Hughes, G.C.; et al. Contemporary management and outcomes of acute type A aortic dissection: An analysis of the STS adult cardiac surgery database. J. Card. Surg. 2018, 33, 7–18. [Google Scholar] [CrossRef] [Green Version]
- Gasser, S.; Stastny, L.; Kofler, M.; Krapf, C.; Bonaros, N.; Grimm, M.; Dumfarth, J. Type A aortic dissection is more aggressive in women. Eur. J. Cardiothorac. Surg. 2022, 62, ezac040. [Google Scholar] [CrossRef] [PubMed]
- Chemtob, R.A.; Hjortdal, V.; Ahlsson, A.; Gunn, J.; Mennander, A.; Zindovic, I.; Olsson, C.; Pivodic, A.; Hansson, E.C.; Jeppsson, A.; et al. Effects of Sex on Early Outcome Following Repair of Acute Type A Aortic Dissection: Results from The Nordic Consortium for Acute Type A Aortic Dissection (NORCAAD). Aorta 2019, 7, 7–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huckaby, L.V.; Sultan, I.; Trimarchi, S.; Leshnower, B.; Chen, E.P.; Brinster, D.R.; Myrmel, T.; Estrera, A.L.; Montgomery, D.G.; Korach, A.; et al. Sex-Based Aortic Dissection Outcomes from the International Registry of Acute Aortic Dissection. Ann. Thorac. Surg. 2022, 113, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, K.W.; Yin, K.; Connelly, H.L.; Datar, Y.; Brydges, H.; Balasubramaniyan, R.; Karlson, K.J.; Edwards, N.M.; Dobrilovic, N. Sex-based outcomes in surgical repair of acute type A aortic dissection: A meta-analysis and meta-regression. J. Thorac. Cardiovasc. Surg. 2022. [Google Scholar] [CrossRef] [PubMed]
- Funk, M.J.; Westreich, D.; Wiesen, C.; Stürmer, T.; Brookhart, M.A.; Davidian, M. Doubly robust estimation of causal effects. Am. J. Epidemiol. 2011, 173, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Ratkovic, M. Covariate balancing propensity score. J. R. Stat. Soc. B 2014, 76, 243–263. [Google Scholar] [CrossRef]
- Cole, S.R.; Hernán, M.A. Constructing inverse probability weights for marginal structural models. Am. J. Epidemiol. 2008, 168, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Aban, I. Application of inverse probability weights in survival analysis. J. Nucl. Cardiol. 2015, 22, 611–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rylski, B.; Beyersdorf, F.; Kari, F.A.; Schlosser, J.; Blanke, P.; Siepe, M. Acute type A aortic dissection extending beyond ascending aorta: Limited or extensive distal repair. J. Thorac. Cardiovasc. Surg. 2014, 148, 949–954; discussion: 954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Eusanio, M.; Berretta, P.; Cefarelli, M.; Jacopo, A.; Murana, G.; Castrovinci, S.; di Bartolomeo, R. Total arch replacement versus more conservative management in type A acute aortic dissection. Ann. Thorac. Surg. 2015, 100, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Lang, X.; Lu, F.; Song, Z.; Wang, J.; Han, L.; Xu, Z. Acute type A dissection without intimal tear in arch: Proximal or extensive repair? J. Thorac. Cardiovasc. Surg. 2014, 147, 1251–1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, C.; Robinson, N.B.; Farrington, W.J.; Rahouma, M.; Gambardella, I.; Gaudino, M.; Girardi, L.N. A tailored strategy for repair of acute type A aortic dissection. J. Thorac. Cardiovasc. Surg. 2022, 164, 1698–1707.e3. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Norton, E.L.; Hobbs, R.; Farhat, L.; Wu, X.; Hornsby, W.E.; Kim, K.M.; Patel, H.J.; Deeb, G.M. Short- and long-term outcomes of aortic root repair and replacement in patients undergoing acute type A aortic dissection repair: Twenty-year experience. J. Thorac. Cardiovasc. Surg. 2019, 157, 2125–2136. [Google Scholar] [CrossRef] [Green Version]
- Omura, A.; Miyahara, S.; Yamanaka, K.; Sakamoto, T.; Matsumori, M.; Okada, K.; Okita, Y. Early and late outcomes of repaired acute DeBakey type I aortic dissection after graft replacement. J. Thorac. Cardiovasc. Surg. 2016, 151, 341–348. [Google Scholar] [CrossRef] [Green Version]
- Sun, L.; Qi, R.; Zhu, J.; Liu, Y.; Zheng, J. Total arch replacement combined with stented elephant trunk implantation: A new “standard” therapy for type a dissection involving repair of the aortic arch? Circulation 2011, 123, 971–978. [Google Scholar] [CrossRef] [Green Version]
- Rylski, B.; Milewski, R.K.; Bavaria, J.E.; Vallabhajosyula, P.; Moser, W.; Szeto, W.Y.; Desai, N.D. Long-term results of aggressive hemiarch replacement in 534 patients with type A aortic dissection. J. Thorac. Cardiovasc. Surg. 2014, 148, 2981–2985. [Google Scholar] [CrossRef] [Green Version]
- Sievers, H.-H.; Richardt, D.; Diwoky, M.; Auer, C.; Bucsky, B.; Nasseri, B.; Klotz, S. Survival and reoperation after valve-sparing root replacement and root repair in acute type A dissection. J. Thorac. Cardiovasc. Surg. 2018, 156, 2076–2082.e2. [Google Scholar] [CrossRef]
- Andersen, N.D.; Ganapathi, A.M.; Hanna, J.M.; Williams, J.B.; Gaca, J.G.; Hughes, G.C. Outcomes of acute type a dissection repair before and after implementation of a multidisciplinary thoracic aortic surgery program. J. Am. Coll. Cardiol. 2014, 63, 1796–1803. [Google Scholar] [CrossRef] [Green Version]
- Conzelmann, L.O.; Weigang, E.; Mehlhorn, U.; Abugameh, A.; Hoffmann, I.; Blettner, M.; Etz, C.D.; Czerny, M.; Vahl, C.F. Mortality in patients with acute aortic dissection type A: Analysis of pre- and intraoperative risk factors from the German Registry for Acute Aortic Dissection Type A (GERAADA). Eur. J. Cardiothorac. Surg. 2016, 49, e44–e52. [Google Scholar] [CrossRef] [Green Version]
- Benedetto, U.; Dimagli, A.; Kaura, A.; Sinha, S.; Mariscalco, G.; Krasopoulos, G.; Moorjani, N.; Field, M.; Uday, T.; Kendal, S.; et al. Determinants of outcomes following surgery for type A acute aortic dissection: The UK National Adult Cardiac Surgical Audit. Eur. Heart J. 2021, 43, 44–52. [Google Scholar] [CrossRef]
- Geirsson, A.; Bavaria, J.E.; Swarr, D.; Keane, M.G.; Woo, Y.J.; Szeto, W.Y.; Pochettino, A. Fate of the residual distal and proximal aorta after acute type A dissection repair using a contemporary surgical reconstruction algorithm. Ann. Thorac. Surg. 2007, 84, 1955–1964. [Google Scholar] [CrossRef] [PubMed]
- Berretta, P.; Patel, H.J.; Gleason, T.G.; Sundt, T.M.; Myrmel, T.; Desai, N.; Korach, A.; Panza, A.; Bavaria, J.; Khoynezhad, A.; et al. IRAD experience on surgical type A acute dissection patients: Results and predictors of mortality. Ann. Cardiothorac. Surg. 2016, 5, 346–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikeno, Y.; Yokawa, K.; Matsueda, T.; Yamanaka, K.; Inoue, T.; Tanaka, H.; Okita, Y. Longterm outcomes of total arch replacement using a 4-branched graft. J. Thorac. Cardiovasc. Surg. 2019, 157, 75–85.e3. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.B.; Chung, C.H.; Moon, D.H.; Ha, G.J.; Lee, T.Y.; Jung, S.H.; Choo, S.J.; Lee, J.W. Total arch repair versus hemiarch repair in the management of acute DeBakey type I aortic dissection. Eur. J. Cardiothorac. Surg. 2011, 40, 881–887. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, D.; McLarty, A.; Sun, E.; Itagaki, S.; Tannous, H.; Chu, D.; Egorova, N.; Chikwe, J. Type-A aortic dissection and cerebral perfusion: The Society of Thoracic Surgeons Database Analysis. Ann. Thorac. Surg. 2020, 110, 1461–1467. [Google Scholar] [CrossRef]
- Preventza, O.; Simpson, K.H.; Cooley, D.A.; Cornwell, L.; Bakaeen, F.G.; Omer, S.; Rodriguez, V.; de la Cruz, K.I.; Rosengart, T.; Coselli, J.S. Unilateral versus bilateral cerebral perfusion for acute type A aortic dissection. Ann. Thorac. Surg. 2015, 99, 80–87. [Google Scholar] [CrossRef]
- Krüger, T.; Weigang, E.; Hoffmann, I.; Blettner, M.; Aebert, H. Cerebral protection during surgery for acute aortic dissection type A: Results of the German registry for acute aortic dissection type a (GERAADA). Circulation 2011, 124, 434–443. [Google Scholar] [CrossRef] [Green Version]
- Benedetto, U.; Dimagli, A.; Cooper, G.; Uppal, R.; Mariscalco, G.; Krasopoulos, G.; Goodwin, A.; Trivedi, U.; Kendall, S.; Sinha, S.; et al. Neuroprotective strategies in acute aortic dissection: An analysis of the UK National Adult Cardiac Surgical Audit. Eur. J. Cardiothorac. Surg. 2021, 60, 1437–1444. [Google Scholar] [CrossRef]
- Bashir, M.; Harky, A.; Fok, M.; Shaw, M.; Hickey, G.L.; Grant, S.W.; Uppal, R.; Oo, A. Acute type A aortic dissection in the United Kingdom: Surgeon volume-outcome relation. J. Thorac. Cardiovasc. Surg. 2017, 154, 398–406.e1. [Google Scholar] [CrossRef]
- Bhatt, N.; Chung, J.C. Gender differences in acute aortic syndromes. Curr. Opin. Cardiol. 2023, 38, 75–81. [Google Scholar] [CrossRef]
- Furukawa, H.; Yamane, N.; Honda, T.; Yamasawa, T.; Kanaoka, Y.; Tanemoto, K. Initial clinical evaluation of preoperative frailty in surgical patients with Stanford type A acute aortic dissection. Gen. Thorac. Cardiovasc. Surg. 2019, 67, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Kabbani, L.S.; Wasilenko, S.; Nypaver, T.J.; Weaver, M.R.; Taylor, A.R.; Abdul-Nour, K.; Borgi, J.; Shepard, A.D. Socioeconomic disparities affect survival after aortic dissection. J. Vasc. Surg. 2016, 64, 1239–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variables | Woman (N = 192) | Man (N = 441) | p Value | SMD |
|---|---|---|---|---|
| Age (median [IQR]) | 72.00 [61.00, 78.00] | 62.00 [54.00, 72.00] | <0.001 | 0.555 |
| Weight, kg (median [IQR]) | 65.00 [59.00, 75.00] | 81.00 [74.00, 90.00] | <0.001 | 0.981 |
| Height, cm (median [IQR]) | 163.00 [160.00, 168.00] | 175.00 [170.00, 180.00] | <0.001 | 1.589 |
| Obesity (%) | 25 (13.0) | 77 (17.5) | 0.201 | 0.124 |
| eGFR, mL/min/1.73 m2 (median [IQR]) | 61.00 [49.00, 77.00] | 77.00 [57.00, 89.00] | <0.001 | 0.508 |
| Haemoglobin, g/L (median [IQR]) | 115.00 [104.00, 125.00] | 128.00 [110.00, 140.00] | <0.001 | 0.543 |
| Arterial lactate, mmol/L (median [IQR]) | 1.30 [0.90, 2.30] | 1.40 [1.00, 2.60] | 0.262 | 0.007 |
| Family history of aortic dissection or aneurysm (%) | 15 (7.8) | 22 (5.0) | 0.227 | 0.116 |
| Prior cardiac surgery (%) | 10 (5.2) | 11 (2.5) | 0.131 | 0.141 |
| Hypertension (%) | 151 (78.6) | 347 (78.7) | 1.000 | 0.001 |
| Diabetes (%) | 15 (7.8) | 24 (5.4) | 0.337 | 0.095 |
| Stroke (%) | 4 (2.1) | 10 (2.3) | 1.000 | 0.013 |
| Pulmonary disease (%) | 15 (7.8) | 18 (4.1) | 0.081 | 0.158 |
| Extracardiac arteriopathy (%) | 8 (4.2) | 14 (3.2) | 0.696 | 0.053 |
| Poor mobility (%) | 13 (6.8) | 36 (8.2) | 0.659 | 0.053 |
| Recent myocardial infarction (%) | 5 (2.6) | 14 (3.2) | 0.894 | 0.034 |
| Systolic pulmonary artery pressure (%) | 0.477 | 0.162 | ||
| <30 mmHg | 117 (60.9) | 239 (54.2) | ||
| <31 mmHg | 1 (0.5) | 1 (0.2) | ||
| >55 mmHg | 3 (1.6) | 5 (1.1) | ||
| 30–55 mmHg | 21 (10.9) | 54 (12.2) | ||
| Bicuspid aortic valve (%) | 0 (0.0) | 12 (2.7) | 0.047 | 0.237 |
| Cardiogenic shock requiring inotropes (%) | 16 (8.3) | 52 (11.8) | 0.249 | 0.115 |
| Cardiac tamponade (%) | 38 (19.8) | 69 (15.6) | 0.244 | 0.109 |
| Preoperative intubation (%) | 61 (31.8) | 122 (27.7) | 0.341 | 0.090 |
| Any malperfusion excluding myocardial malperfusion (%) | 41 (21.4) | 109 (24.7) | 0.416 | 0.080 |
| Tear in the aortic root (%) | 45 (23.4) | 136 (30.8) | 0.072 | 0.167 |
| Tear in the ascending aorta (%) | 116 (60.4) | 229 (51.9) | 0.059 | 0.172 |
| Tear in the aortic arch (%) | 20 (10.4) | 70 (15.9) | 0.092 | 0.162 |
| CABG (%) | 16 (8.3) | 40 (9.1) | 0.882 | 0.026 |
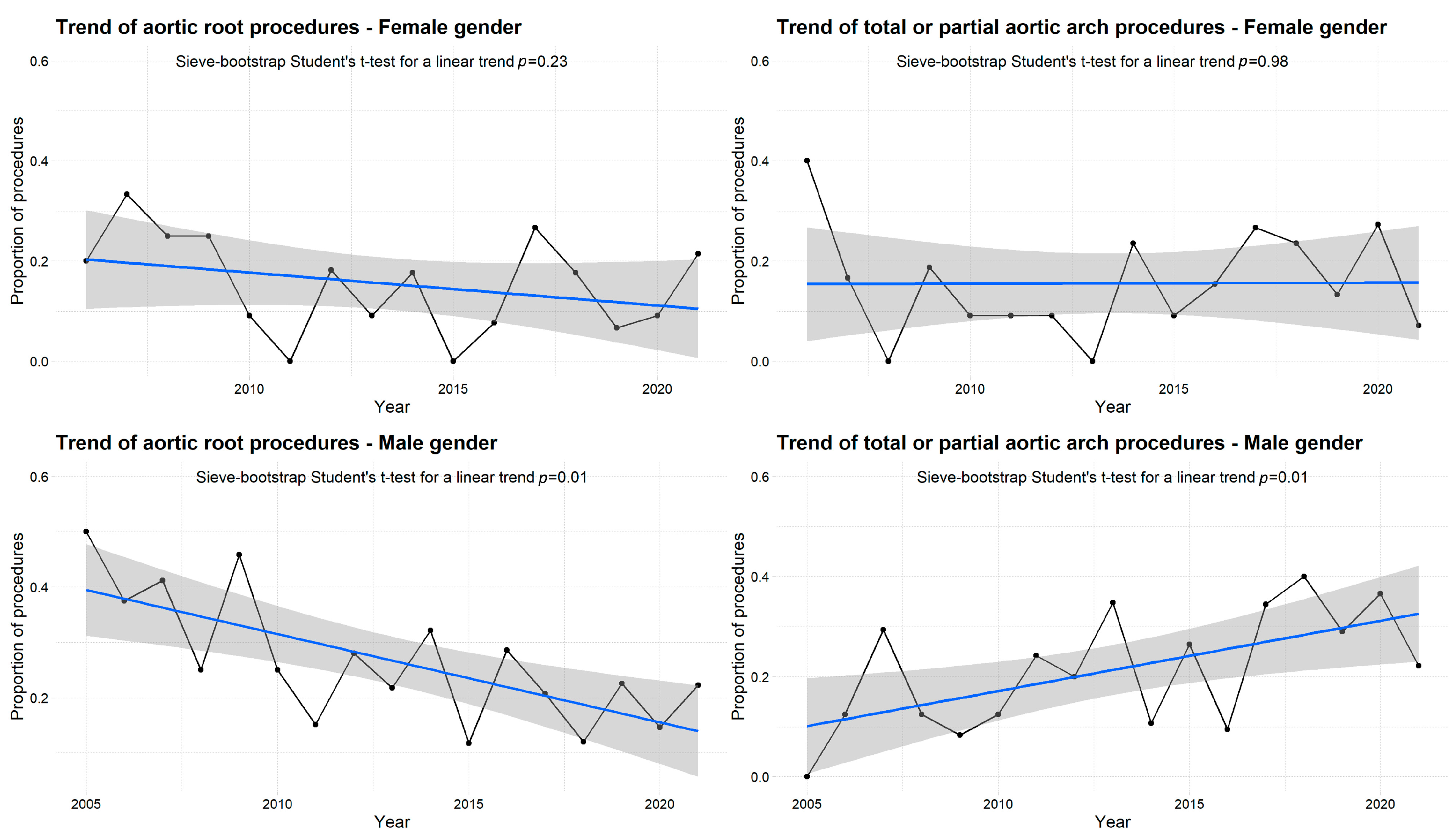
| Aortic root replacement (%) | 29 (15.1) | 106 (24.0) | 0.016 | 0.227 |
| Total or partial aortic arch repair (%) | 30 (15.6) | 103 (23.4) | 0.037 | 0.196 |
| Antegrade cerebral perfusion (%) | 80 (41.7) | 200 (45.4) | 0.441 | 0.074 |
| Retrograde cerebral perfusion (%) | 34 (17.7) | 83 (18.8) | 0.826 | 0.029 |
| Myocardial ischemic time, min (median [IQR]) | 91.00 [64.50, 133.50] | 108.00 [77.00, 152.00] | 0.005 | 0.179 |
| Cardiopulmonary bypass time, min (median [IQR]) | 164.00 [119.00, 222.00] | 186.00 [128.00, 260.00] | 0.012 | 0.163 |
| Hypothermic circulatory arrest duration, min (median [IQR]) | 28.00 [15.50, 41.50] | 30.00 [5.00, 48.00] | 0.529 | 0.143 |
| Variables | Overall Series | Doubly Robust Adjustment § | ||||
|---|---|---|---|---|---|---|
| Female Gender N = 192 | Male Gender N = 441 | p Value | Odds Ratio | 95% CI | p Value | |
| Stroke (%) | 25 (13.0) | 57 (12.9) | 0.481 | 0.928 | 0.521–1.653 | 0.800 |
| Paraplegia (%) | 9 (4.7) | 14 (3.2) | 0.987 | 1.379 | 0.563–3.380 | 0.483 |
| Tetraplegia or tetraparesis (%) | 1 (0.5) | 4 (0.9) | 0.337 | 0.492 | 0.054–4.452 | 0.529 |
| Laryngeal nerve palsy (%) | 3 (1.6) | 2 (0.5) | 0.569 | 4.997 | 0.822–30.393 | 0.081 |
| Mesenteric ischemia (%) | 11 (5.7) | 19 (4.3) | 0.861 | 0.936 | 0.423–2.071 | 0.871 |
| Sepsis (%) | 33 (17.2) | 80 (18.1) | 0.168 | 0.866 | 0.511–1.470 | 0.595 |
| Dialysis (%) | 16 (8.3) | 55 (12.5) | 0.241 | 0.504 | 0.271–0.939 | 0.031 |
| Atrial fibrillation (%) | 47 (24.5) | 88 (20.0) | 0.583 | 1.098 | 0.712–1.693 | 0.673 |
| Reoperation for intrathoracic bleeding (%) | 17 (8.9) | 47 (10.7) | 1.000 | 0.683 | 0.367–1.270 | 0.229 |
| Deep sternal wound infection/mediastinitis (%) | 6 (3.1) | 13 (2.9) | 0.746 | 1.062 | 0.368–3.071 | 0.911 |
| IABP (%) | 4 (2.1) | 6 (1.4) | 0.971 | 1.773 | 0.478–6.572 | 0.392 |
| VA ECMO (%) | 7 (3.6) | 18 (4.1) | 0.705 | 0.560 | 0.224–1.402 | 0.216 |
| ICU stay, days (median [IQR]) | 10.00 [4.00, 19.00] | 9.00 [3.00, 20.25] | 0.483 | −0.954 § | 1.393 § | 0.494 § |
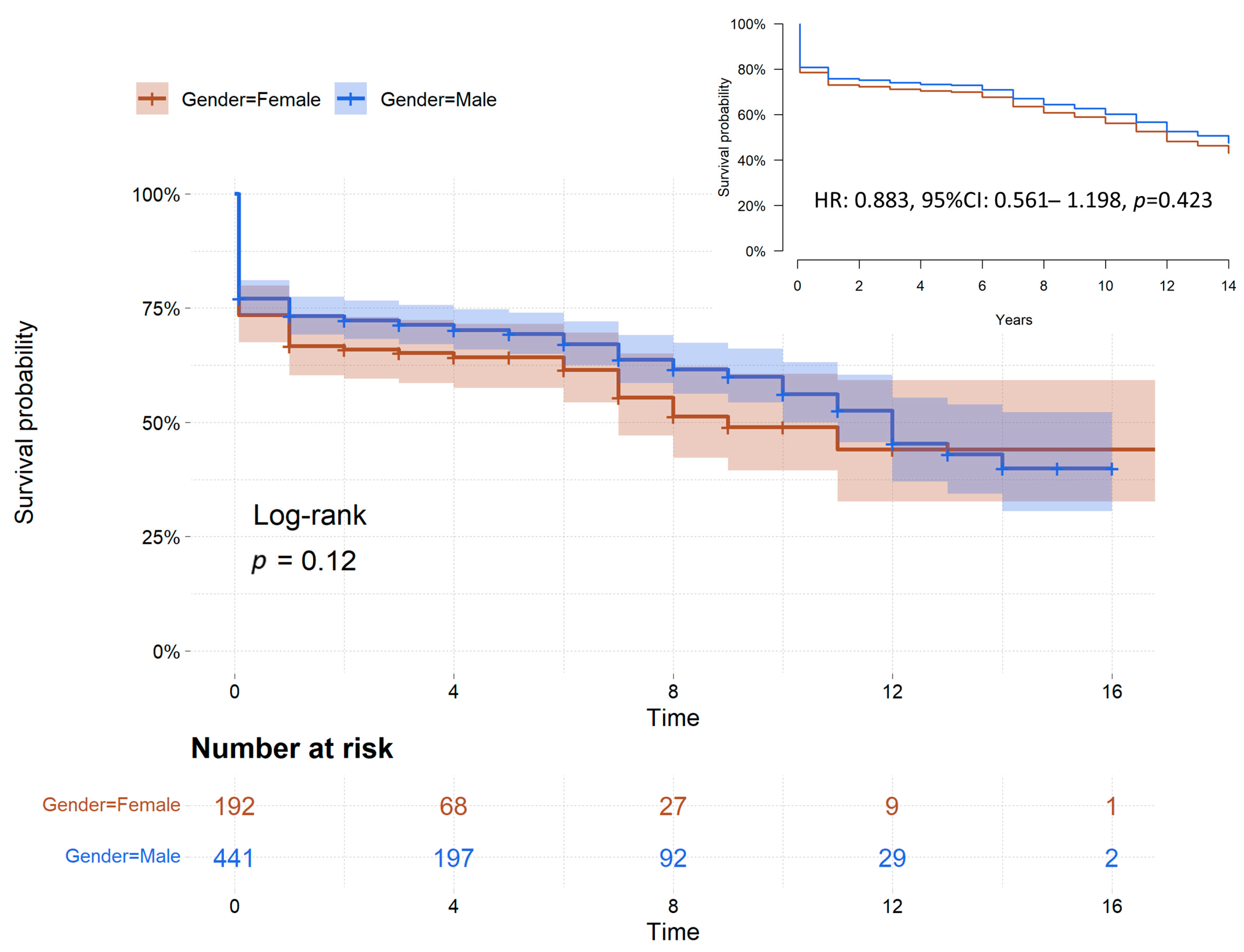
| In-hospital mortality (%) | 51 (26.6) | 104 (23.6) | 1.000 | 0.745 | 0.491–1.130 | 0.166 |
| Variables | Univariate Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|---|
| No Event (N = 141) | Operative Mortality (N = 51) * | p Value | Beta-Coefficient | OR | 95% CI | p Value | |
| Baseline and operative characteristics | |||||||
| Age (median [IQR]) | 69.00 [59.00, 78.00] | 76.00 [72.00, 80.00] | <0.001 | ||||
| Weight, kg (median [IQR]) | 65.00 [59.75, 75.25] | 63.50 [58.00, 72.25] | 0.431 | ||||
| Height, cm (median [IQR]) | 163.00 [159.75, 169.00] | 161.00 [160.00, 167.00] | 0.349 | ||||
| Obesity (%) | 20 (14.2) | 5 (9.8) | 0.580 | ||||
| eGFR, mL/min/1.73 m2 (median [IQR]) | 65.00 [58.00, 82.00] | 50.00 [37.00, 61.00] | <0.001 | −0.049 | 0.952 | 0.929–0.976 | <0.001 |
| Hemoglobin, g/L (median [IQR]) | 117.50 [106.75, 125.00] | 109.00 [100.75, 123.50] | 0.112 | ||||
| Arterial lactate, mmol/L (median [IQR]) | 1.10 [0.90, 2.00] | 2.10 [1.20, 4.50] | <0.001 | 0.384 | 1.468 | 1.133–1.901 | 0.004 |
| Family history of aortic dissection or aneurysm (%) | 12 (8.5) | 3 (5.9) | 0.768 | ||||
| Prior cardiac surgery (%) | 8 (5.7) | 2 (3.9) | 0.909 | ||||
| Hypertension (%) | 108 (76.6) | 43 (84.3) | 0.340 | ||||
| Diabetes (%) | 10 (7.1) | 5 (9.8) | 0.754 | ||||
| Stroke (%) | 2 (1.4) | 2 (3.9) | 0.617 | ||||
| Pulmonary disease (%) | 6 (4.3) | 9 (17.6) | 0.006 | ||||
| Extracardiac arteriopathy (%) | 5 (3.5) | 3 (5.9) | 0.759 | ||||
| Poor mobility (%) | 9 (6.4) | 4 (7.8) | 0.976 | ||||
| Recent myocardial infarction (%) | 1 (0.7) | 4 (7.8) | 0.026 | ||||
| Systolic pulmonary artery pressure (%) | 0.455 | ||||||
| <30 mmHg | 81 (57.4) | 36 (70.6) | |||||
| <31 mmHg | 1 (0.7) | 0 (0.0) | |||||
| >55 mmHg | 2 (1.4) | 1 (2.0) | |||||
| 30–55 mmHg | 18 (12.8) | 3 (5.9) | |||||
| Bicuspid aortic valve (%) | 0 (0) | 0 (0) | NA | ||||
| Cardiogenic shock requiring inotropes (%) | 7 (5.0) | 9 (17.6) | 0.012 | ||||
| Cardiac tamponade (%) | 19 (13.5) | 19 (37.3) | 0.001 | ||||
| Preoperative intubation (%) | 38 (27.0) | 23 (45.1) | 0.027 | ||||
| Any malperfusion excluding myocardial malperfusion (%) | 21 (14.9) | 20 (39.2) | 0.001 | ||||
| Tear in the aortic root (%) | 33 (23.4) | 12 (23.5) | 1.000 | ||||
| Tear in the ascending aorta (%) | 84 (59.6) | 32 (62.7) | 0.818 | ||||
| Tear in the aortic arch (%) | 14 (9.9) | 6 (11.8) | 0.920 | ||||
| CABG (%) | 12 (8.5) | 4 (7.8) | 1.000 | ||||
| Aortic root replacement (%) | 23 (16.3) | 6 (11.8) | 0.583 | ||||
| Total or partial aortic arch repair (%) | 23 (16.3) | 7 (13.7) | 0.833 | ||||
| Antegrade cerebral perfusion (%) | 57 (40.4) | 23 (45.1) | 0.679 | ||||
| Retrograde cerebral perfusion (%) | 25 (17.7) | 9 (17.6) | 1.000 | ||||
| Myocardial ischemic time, min (median [IQR]) | 91.50 [66.75, 126.50] | 91.00 [60.00, 158.50] | 0.912 | ||||
| Cardiopulmonary bypass time, min (median [IQR]) | 156.50 [119.00, 218.25] | 182.00 [122.50, 252.50] | 0.255 | ||||
| Hypothermic circulatory arrest duration, min (median [IQR]) | 29.00 [17.00, 42.00] | 26.00 [10.00, 41.25] | 0.596 | ||||
| Postoperative events | |||||||
| Stroke (%) | 13 (9.2) | 12 (23.5) | 0.018 | ||||
| Paraplegia (%) | 5 (3.5) | 4 (7.8) | 0.391 | ||||
| Tetraplegia or tetraparesis (%) | 0 (0.0) | 1 (2.0) | 0.595 | ||||
| Laryngeal nerve palsy (%) | 3 (2.1) | 0 (0.0) | 0.696 | ||||
| Mesenteric ischemia (%) | 1 (0.7) | 10 (19.6) | <0.001 | 3.489 | 32.742 | 3.361–319.017 | 0.003 |
| Sepsis (%) | 23 (16.3) | 10 (19.6) | 0.750 | ||||
| Dialysis (%) | 8 (5.7) | 8 (15.7) | 0.055 | ||||
| Atrial fibrillation (%) | 40 (28.4) | 7 (13.7) | 0.058 | ||||
| Reoperation for intrathoracic bleeding (%) | 14 (9.9) | 3 (5.9) | 0.559 | ||||
| Deep sternal wound infection/mediastinitis (%) | 3 (2.1) | 3 (5.9) | 0.395 | ||||
| IABP (%) | 2 (1.4) | 2 (3.9) | 0.617 | ||||
| VA ECMO (%) | 2 (1.4) | 5 (9.8) | 0.021 | ||||
| Constant | 0.884 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nappi, F.; Petiot, S.; Salsano, A.; Avtaar Singh, S.S.; Berger, J.; Kostantinou, M.; Bonnet, S.; Gambardella, I.; Biancari, F.; Almazil, A.; et al. Sex-Based Difference in Aortic Dissection Outcomes: A Multicenter Study. J. Cardiovasc. Dev. Dis. 2023, 10, 147. https://doi.org/10.3390/jcdd10040147
Nappi F, Petiot S, Salsano A, Avtaar Singh SS, Berger J, Kostantinou M, Bonnet S, Gambardella I, Biancari F, Almazil A, et al. Sex-Based Difference in Aortic Dissection Outcomes: A Multicenter Study. Journal of Cardiovascular Development and Disease. 2023; 10(4):147. https://doi.org/10.3390/jcdd10040147
Chicago/Turabian StyleNappi, Francesco, Sandra Petiot, Antonio Salsano, Sanjeet Singh Avtaar Singh, Joelle Berger, Marisa Kostantinou, Severine Bonnet, Ivancarmine Gambardella, Fausto Biancari, Almothana Almazil, and et al. 2023. "Sex-Based Difference in Aortic Dissection Outcomes: A Multicenter Study" Journal of Cardiovascular Development and Disease 10, no. 4: 147. https://doi.org/10.3390/jcdd10040147