
Impella Versus VA-ECMO for Patients with Cardiogenic Shock: Comprehensive Systematic Literature Review and Meta-Analyses
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Review Profile
3.2. Characteristics of Included Studies
3.3. Evidence from Meta-Analyses
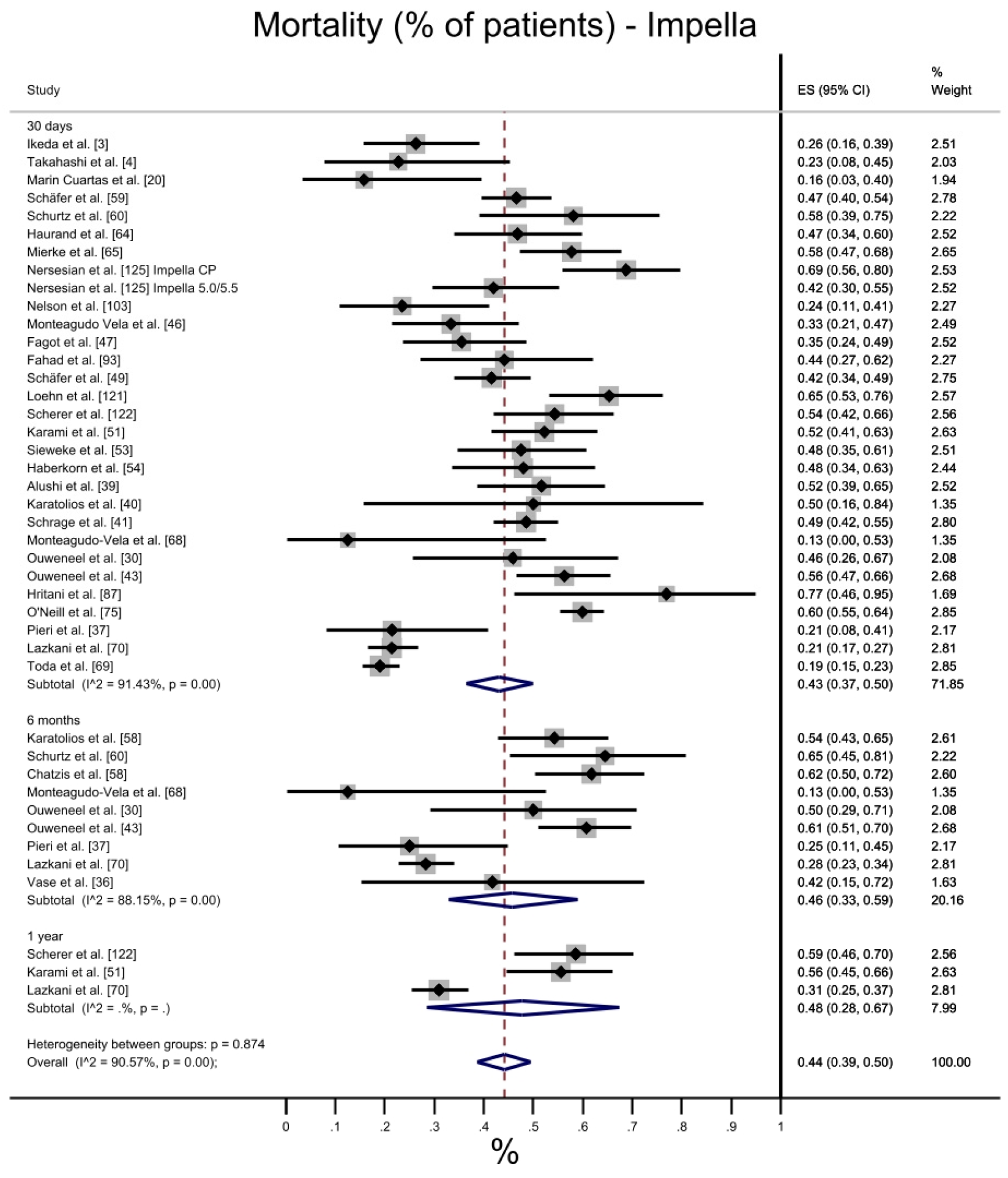
3.3.1. Mortality
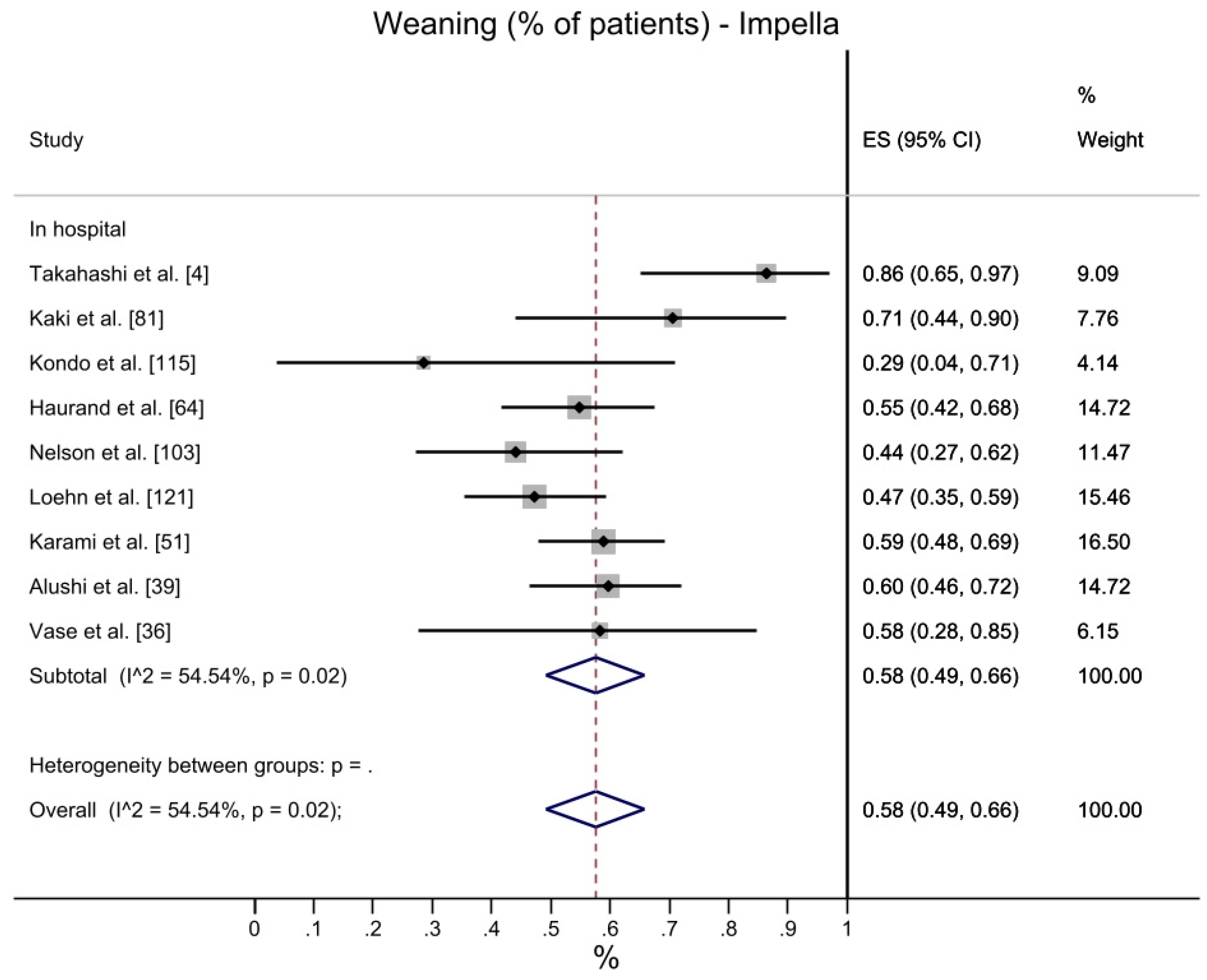
3.3.2. Weaning
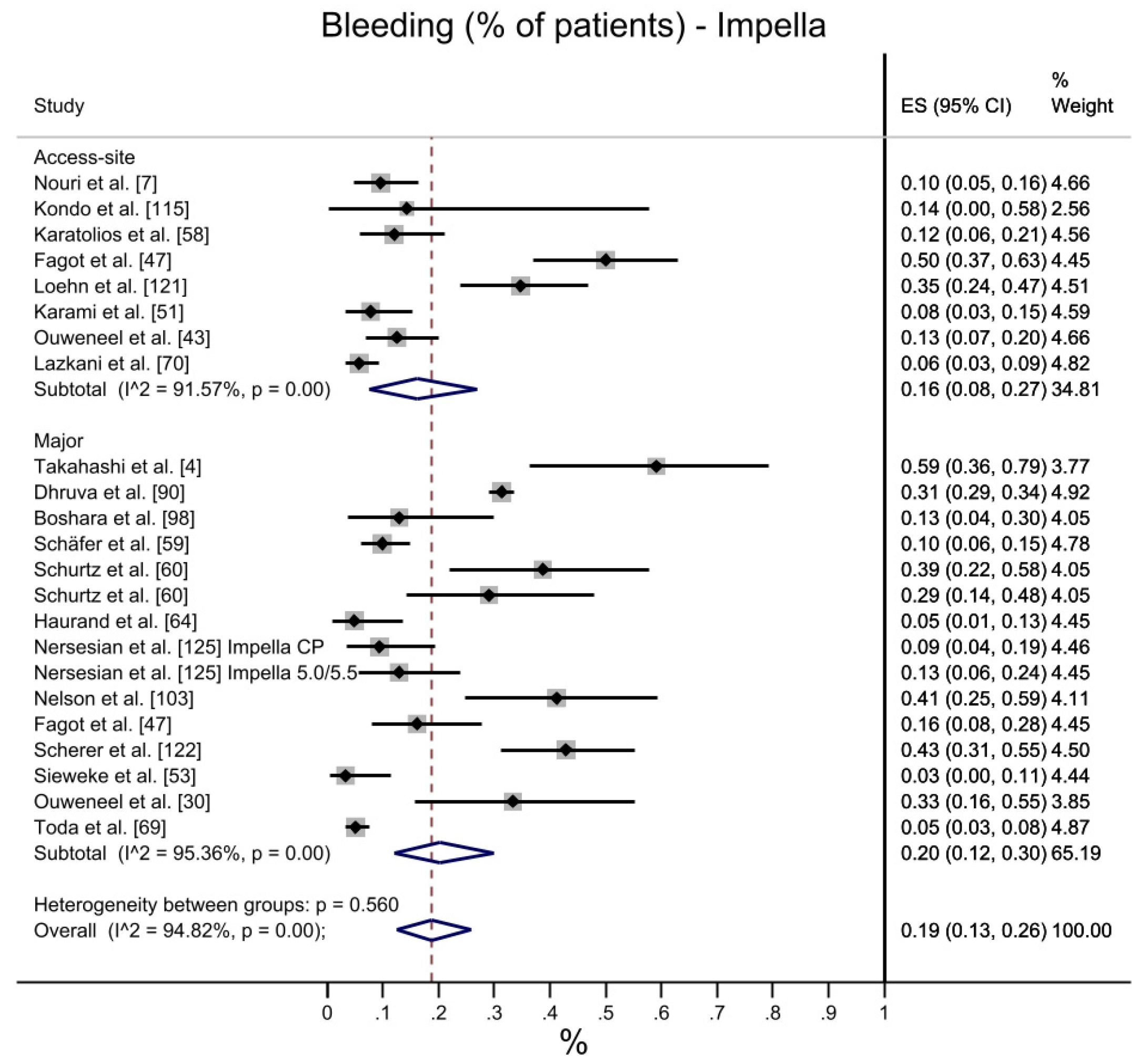
3.3.3. Bleeding
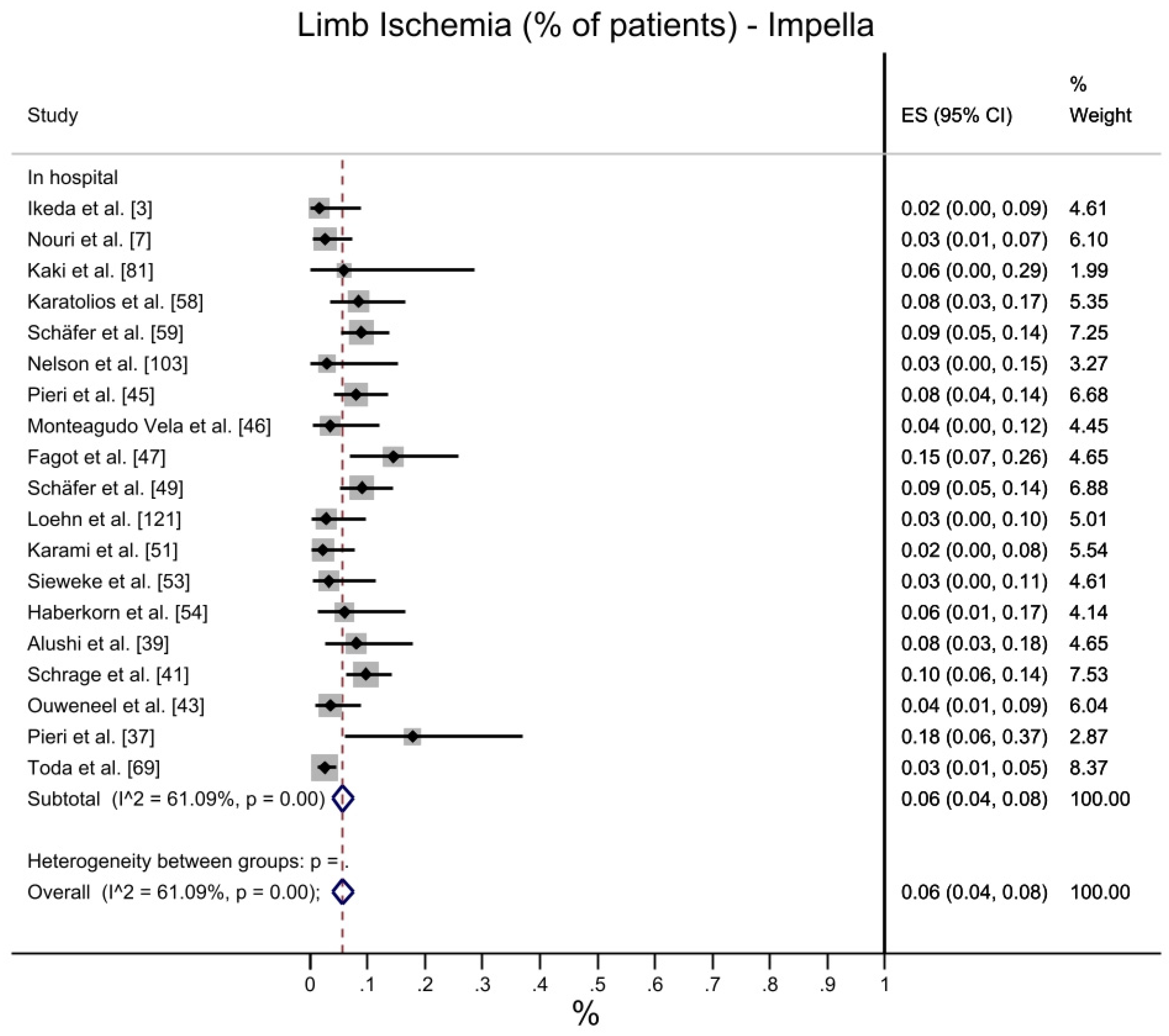
3.3.4. Limb Ischemia
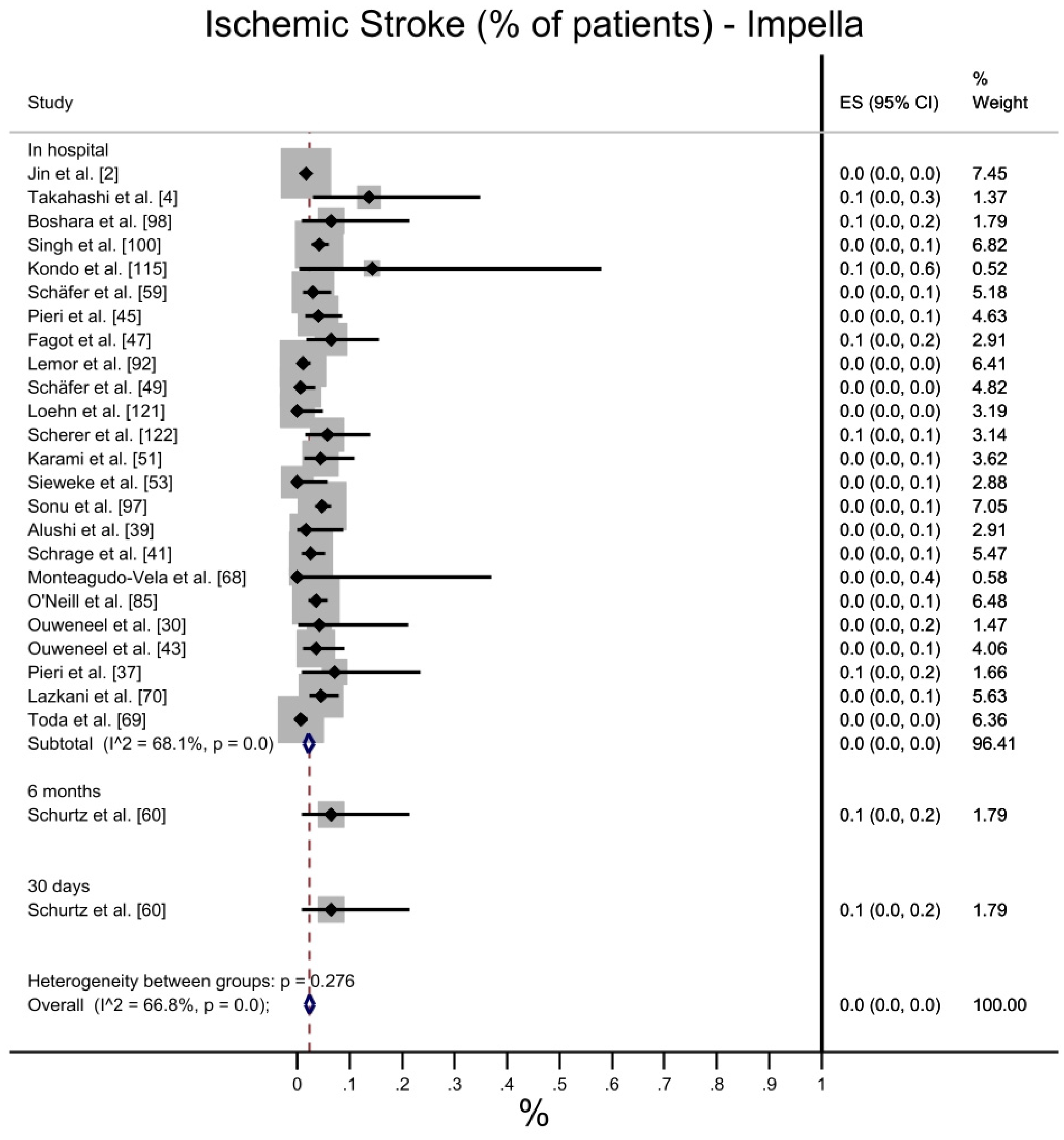
3.3.5. Ischemic Stroke
3.3.6. Bridge to LVAD
3.3.7. Bridge to Transplant
3.3.8. Renal Failure
3.3.9. Days on Support
3.4. Risk of Bias Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shah, R.U.; de Lemos, J.A.; Wang, T.Y.; Chen, A.Y.; Thomas, L.; Sutton, N.R.; Fang, J.C.; Scirica, B.M.; Henry, T.D.; Granger, C.B. Post-Hospital Outcomes of Patients with Acute Myocardial Infarction with Cardiogenic Shock. J. Am. Coll. Cardiol. 2016, 67, 739–747. [Google Scholar] [CrossRef]
- Jin, C.; Yandrapalli, S.; Yang, Y.; Liu, B.; Aronow, W.S.; Naidu, S.S. A Comparison of In-Hospital Outcomes Between the Use of Impella and IABP in Acute Myocardial Infarction Cardiogenic Shock Undergoing Percutaneous Coronary Intervention. J. Invasive Cardiol. 2022, 34, E98–E103. [Google Scholar] [PubMed]
- Ikeda, Y.; Ishii, S.; Maemura, K.; Oki, T.; Yazaki, M.; Fujita, T.; Iida, Y.; Kinoshita, D.; Sato, N.; Ako, J. Hemodynamic assessment and risk classification for successful weaning of Impella in patients with cardiogenic shock. Artif. Organs 2022, 46, 1358–1368. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Kubo, S.; Ikuta, A.; Osakada, K.; Takamatsu, M.; Taguchi, Y.; Ohya, M.; Shimada, T.; Miura, K.; Tada, T.; et al. Incidence, predictors, and clinical outcomes of mechanical circulatory support-related complications in patients with cardiogenic shock. J. Cardiol. 2021, 79, 163–169. [Google Scholar] [CrossRef]
- Burzotta, F.; Russo, G.; Basile, E.; Aurigemma, C.; Leone, A.M.; Niccoli, G.; Porto, I.; Bruno, P.; Massetti, M.; Crea, F.; et al. Come orientarsi tra contropulsatore, Impella e ossigenazione a membrana extracorporea. G. Ital. Cardiol. 2018, 19 (Suppl. 1), 5S–13S. [Google Scholar] [CrossRef]
- Thiele, H.; Zeymer, U.; Thelemann, N.; Neumann, F.J.; Hausleiter, J.; Abdel-Wahab, M.; Fuernau, G.; Eitel, I.; Hambrecht, R.; Böhm, M.; et al. Intraaortic Balloon Pump in Cardiogenic Shock Complicating Acute Myocardial Infarction: Long-Term 6-Year Outcome of the Randomized IABP-SHOCK II Trial. Circulation 2019, 139, 395–403. [Google Scholar] [CrossRef]
- Nouri, S.N.; Malick, W.; Masoumi, A.; Fried, J.A.; Topkara, V.K.; Brener, M.I.; Ahmad, Y.; Prasad, M.; Rabbani, L.E.; Takeda, K.; et al. Impella percutaneous left ventricular assist device as mechanical circulatory support for cardiogenic shock: A retrospective analysis from a tertiary academic medical center. Catheter. Cardiovasc. Interv. 2020, 99, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.H.; Kim, H.C.; Ahn, C.M.; Lee, S.J.; Hong, S.J.; Yang, J.H.; Kim, J.-S.; Kim, B.K.; KO, Y.-G.; Choi, D.; et al. Association Between Timing of Extracorporeal Membrane Oxy-genation and Clinical Outcomes in Refractory Cardiogenic Shock. JACC Cardiovasc. Interv. 2021, 14, 1109–1119. [Google Scholar] [CrossRef]
- Russo, J.J.; Aleksova, N.; Pitcher, I.; Couture, E.; Parlow, S.; Faraz, M.; Visintini, S.; Simard, T.; Di Santo, P.; Mathew, R.; et al. Left Ventricular Unloading During Extracorporeal Membrane Oxygenation in Patients with Cardiogenic Shock. J. Am. Coll. Cardiol. 2019, 73, 654–662. [Google Scholar] [CrossRef]
- Iannaccone, M.; Albani, S.; Giannini, F.; Colangelo, S.; Boccuzzi, G.G.; Garbo, R.; Brilakis, E.S.; D’Ascenzo, F.; de Ferrari, G.M.; Colombo, A. Short term outcomes of Impella in cardiogenic shock: A review and meta-analysis of observational studies. Int. J. Cardiol. 2020, 324, 44–51. [Google Scholar] [CrossRef]
- Kowalewski, M.; Raffa, G.; Zieliński, K.; Meani, P.; Alanazi, M.; Gilbers, M.; Heuts, S.; Natour, E.; Bidar, E.; Schreurs, R.; et al. Baseline surgical status and short-term mortality after extracorporeal membrane oxygenation for post-cardiotomy shock: A meta-analysis. Perfusion 2019, 35, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Raffa, G.M.; Kowalewski, M.; Brodie, D.; Ogino, M.; Whitman, G.; Meani, P.; Pilato, M.; Arcadipane, A.; Delnoij, T.; Natour, E.; et al. Meta-Analysis of Peripheral or Central Extracor-poreal Membrane Oxygenation in Postcardiotomy and Non-Postcardiotomy Shock. Ann. Thorac. Surg. 2019, 107, 311–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowalewski, M.; Raffa, G.M.; Zieliński, K.; Alanazi, M.; Gilbers, M.; Heuts, S.; Natour, E.; Bidar, E.; Schreurs, R.; Delnoij, T.; et al. The impact of Centre’s heart transplant status and volume on in-hospital outcomes following extracorporeal membrane oxygenation for refractory post-cardiotomy cardiogenic shock: A meta-analysis. BMC Cardiovasc. Disord. 2020, 20, 10–11. [Google Scholar] [CrossRef]
- Vargas, K.G.; Jäger, B.; Kaufmann, C.C.; Biagioli, A.; Watremez, S.; Gatto, F.; Özbek, C.; Razouk, A.; Geppert, A.; Huber, K. Impella in cardiogenic shock following acute my-ocardial infarction: A systematic review and meta-analysis. Wien. Klin. Wochenschr. 2020, 132, 716–725. [Google Scholar] [CrossRef]
- Batsides, G.; Massaro, J.; Cheung, A.; Soltesz, E.; Ramzy, D.; Anderson, M.B. Outcomes of Impella 5.0 in Cardiogenic Shock: A Sys-tematic Review and Meta-analysis. Innovations (Phila) 2018, 13, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wang, H.; Hou, X. Clinical Outcomes of Adult Patients Who Receive Extracorporeal Membrane Oxygenation for Postcardiotomy Cardiogenic Shock: A Systematic Review and Meta-Analysis. J. Cardiothorac. Vasc. Anesthesia 2018, 32, 2087–2093. [Google Scholar] [CrossRef] [PubMed]
- Zavalichi, M.A.; Nistor, I.; Nedelcu, A.-E.; Zavalichi, S.D.; Georgescu, C.M.A.; Stătescu, C.; Covic, A. Extracorporeal Membrane Oxygenation in Cardiogenic Shock due to Acute Myocardial Infarction: A Systematic Review. BioMed Res. Int. 2020, 2020, 6126534. [Google Scholar] [CrossRef] [PubMed]
- Wernly, B.; Seelmaier, C.; Leistner, D.; Stähli, B.E.; Pretsch, I.; Lichtenauer, M.; Jung, C.; Hoppe, U.C.; Landmesser, U.; Thiele, H.; et al. Mechanical circulatory support with Impella versus intra-aortic balloon pump or medical treatment in cardiogenic shock—A critical appraisal of current data. Clin. Res. Cardiol. 2019, 108, 1249–1257. [Google Scholar] [CrossRef]
- Affas, Z.R.; Touza, G.G.; Affas, S. A Meta-Analysis Comparing Venoarterial (VA) Extracorporeal Membrane Oxygenation (ECMO) to Impella for Acute Right Ventricle Failure. Cureus [Internet]. Available online: https://www.cureus.com/articles/75581-a-meta-analysis-comparing-venoarterial-va-extracorporeal-membrane-oxygenation-ecmo-to-impella-for-acute-right-ventricle-failure (accessed on 30 May 2022).
- Marin Cuartas, M.; Wehrmann, K.; Hoebartner, M.; Lehmann, S.; Etz, C.D.; Saeed, D.; Borger, M. Perioperative temporary mechanical circulatory support with Impella in cardiac surgery patients. J. Cardiovasc. Surg. (Torino) 2022, 63, 229–236. [Google Scholar] [CrossRef]
- HTA Regulation. Available online: https://ec.europa.eu/health/health-technology-assessment/regulation-health-technology-assessment_en#:~:text=The%20new%20framework%20covers%20joint,applies%20as%20of%20January%202025 (accessed on 30 May 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Israel, H.; Richter, R.R. A Guide to Understanding Meta-analysis. J. Orthop. Sports Phys. Ther. 2011, 41, 496–504. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis [Internet]; JBI, 2020; Available online: https://synthesismanual.jbi.global (accessed on 30 May 2022).
- Tufanaru, C.; Munn, Z.; Aromataris, E.; Campbell, J.; Hopp, L. Chapter 3: Systematic reviews of effectiveness. In JBI Manual for Evidence Synthesis [Internet]; JBI, 2020; Available online: https://synthesismanual.jbi.global (accessed on 30 May 2022).
- Refworks; ProQuest LLC: Ann Arbor, MI, USA, 2022.
- Zotero Software. Available online: http://www.zotero.org (accessed on 2 November 2020).
- Ouweneel, D.M.; Eriksen, E.; Sjauw, K.D.; van Dongen, I.M.; Hirsch, A.; Packer, E.J.; Vis, M.M.; Wykrzykowska, J.J.; Koch, K.T.; Baan, J.; et al. Percutaneous Mechanical Circulatory Support Versus Intra-Aortic Balloon Pump in Cardiogenic Shock After Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2016, 69, 278–287. [Google Scholar] [CrossRef] [PubMed]
- Pappalardo, F.; Schulte, C.; Pieri, M.; Schrage, B.; Contri, R.; Soeffker, G.; Greco, T.; Lembo, R.; Müllerleile, K.; Colombo, A.; et al. Concomitant implantation of Impella® on top of veno-arterial extracorporeal membrane oxygenation may improve survival of patients with cardiogenic shock. Eur. J. Heart Fail. 2016, 19, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Le Pennec-Prigent, S.; Flecher, E.; Auffret, V.; Leurent, G.; Daubert, J.C.; Leclercq, C.; Mabo, P.; Verhoye, J.P.; Martins, R.P. Effectiveness of Extracorporeal Life Support for Patients with Cardiogenic Shock Due To Intractable Arrhythmic Storm. Crit. Care Med. 2017, 45, e281–e289. [Google Scholar] [CrossRef] [PubMed]
- Schmack, B.; Seppelt, P.; Weymann, A.; Alt, C.; Farag, M.; Arif, R.; Philippe, M.; Jean-Philippe, V.; Raphael, P.M. Extracorporeal life support with left ventricular decompres-sion-improved survival in severe cardiogenic shock: Results from a retrospective study. PeerJ 2017, 5, e3813. [Google Scholar] [CrossRef] [Green Version]
- Dangers, L.; Bréchot, N.; Schmidt, M.; Lebreton, G.; Hékimian, G.; Nieszkowska, A.; Besset, S.; Trouillet, J.-L.; Chastre, J.; Leprince, P.; et al. Extracorporeal Membrane Oxygenation for Acute Decompensated Heart Failure. Crit. Care Med. 2017, 45, 1359–1366. [Google Scholar] [CrossRef]
- de Waha, S.; Graf, T.; Desch, S.; Fuernau, G.; Eitel, I.; Pöss, J.; Jobs, A.; Stiermaier, T.; Ledwoch, J.; Wiedau, A.; et al. Outcome of elderly undergoing extracorporeal life support in refractory cardiogenic shock. Clin. Res. Cardiol. 2017, 106, 379–385. [Google Scholar] [CrossRef]
- Vase, H.; Christensen, S.; Christiansen, A.; Therkelsen, C.J.; Christiansen, E.H.; Eiskjaer, H.; Poulsen, S.H. The Impella CP device for acute mechanical circulatory support in refractory cardiac arrest. Resuscitation 2017, 112, 70–74. [Google Scholar] [CrossRef]
- Pieri, M.; Sorrentino, T.; Oppizzi, M.; Melisurgo, G.; Lembo, R.; Colombo, A.; Zangrillo, A.; Pappalardo, F. The role of different mechanical circulatory support devices and their timing of implantation on myocardial damage and mid-term recovery in acute myocardial infarction related cardiogenic shock. J. Interv. Cardiol. 2018, 31, 717–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunner, S.; Guenther, S.P.W.; Lackermair, K.; Peterss, S.; Orban, M.; Boulesteix, A.L.; Michel, S.; Hausleiter, J.; Massberg, S.; Hagl, C. Extracorporeal Life Support in Cardiogenic Shock Complicating Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2019, 73, 2355–2357. [Google Scholar] [CrossRef]
- Alushi, B.; Douedari, A.; Froehlig, G.; Knie, W.; Wurster, T.H.; Leistner, D.M.; Staehli, B.-E.; Mochmann, H.-C.; Pieske, B.; Landmesser, U.; et al. Impella versus IABP in acute myocardial infarction complicated by cardiogenic shock. Open Heart 2019, 6, e000987. [Google Scholar] [CrossRef] [Green Version]
- Karatolios, K.; Chatzis, G.; Luesebrink, U.; Markus, B.; Ahrens, H.; Tousoulis, D.; Michel, S.; Hausleiter, J.; Massberg, S.; Hagl, C. Impella support following emergency percu-taneous balloon aortic valvuloplasty in patients with severe aortic valve stenosis and cardiogenic shock. Hell. J. Cardiol. 2019, 60, 178–181. [Google Scholar] [CrossRef]
- Schrage, B.; Ibrahim, K.; Loehn, T.; Werner, N.; Sinning, J.-M.; Pappalardo, F.; Pieri, M.; Skurk, C.; Lauten, A.; Landmesser, U.; et al. Impella Support for Acute Myocardial Infarction Complicated by Cardiogenic Shock. Circulation 2019, 139, 1249–1258. [Google Scholar] [CrossRef] [PubMed]
- Morshuis, M.; Bruenger, F.; Becker, T.; Kempa-Haupt, A.; Kizner, L.; Al-Khalil, R.; Gummert, J.F.; Schramm, R. Inter-hospital transfer of extracorporeal membrane oxygenation-assisted patients: The hub and spoke network. Ann. Cardiothorac. Surg. 2019, 8, 62–65. [Google Scholar] [CrossRef] [Green Version]
- Ouweneel, D.M.; De Brabander, J.; Karami, M.; Sjauw, K.D.; E Engström, A.; Vis, M.M.; Wykrzykowska, J.J.; A Beijk, M.; Koch, K.T.; Baan, J.; et al. Real-life use of left ventricular circulatory support with Impella in cardiogenic shock after acute myocardial infarction: 12 years AMC experience. Eur. Heart J. Acute Cardiovasc. Care 2018, 8, 338–349. [Google Scholar] [CrossRef] [Green Version]
- Fux, T.; Holm, M.; Corbascio, M.; Lund, L.H.; van der Linden, J. VA-ECMO Support in Nonsurgical Patients with Refractory Car-diogenic Shock: Pre-Implant Outcome Predictors. Artif. Organs 2019, 43, 132–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieri, M.; Pappalardo, F. Bedside insertion of impella percutaneous ventricular assist device in patients with cardiogenic shock. Int. J. Cardiol. 2020, 316, 26–30. [Google Scholar] [CrossRef]
- Monteagudo Vela, M.; Simon, A.; Riesgo Gil, F.; Rosenberg, A.; Dalby, M.; Kabir, T.; Saez, D.G.; Panoulas, V. Clinical Indications of IMPELLA Short-Term Mechanical Circulatory Support in a Tertiary Centre. Cardiovasc. Revasc Med. 2020, 21, 629–637. [Google Scholar] [CrossRef]
- Fagot, J.; Bouisset, F.; Bonello, L.; Biendel, C.; Lhermusier, T.; Porterie, J.; Roncalli, J.; Galinier, M.; Elbaz, M.; Lairez, O.; et al. Early Evaluation of Patients on Axial Flow Pump Support for Refractory Cardiogenic Shock is Associated with Left Ventricular Recovery. J. Clin. Med. 2020, 9, 4130. [Google Scholar] [CrossRef]
- Pozzi, M.; Flagiello, M.; Armoiry, X.; Generali, T.; Adamou Nouhou, K.; Koffel, C.; Saez, D.G.; Panoulas, V. Extracorporeal life support in the multidis-ciplinary management of cardiogenic shock complicating acute myocardial infarction. Catheter. Cardiovasc. Interv. 2020, 95, E71–E77. [Google Scholar] [CrossRef]
- Schäfer, A.; Werner, N.; Burkhoff, D.; Sieweke, J.-T.; Zietzer, A.; Masyuk, M.; Udesen, N.L.J.; Westenfeld, R.; Møller, J.E. Influence of Timing and Predicted Risk on Mortality in Impella-Treated Infarct-Related Cardiogenic Shock Patients. Front. Cardiovasc. Med. 2020, 7, 74. [Google Scholar] [CrossRef] [PubMed]
- Schrage, B.; Becher, P.M.; Bernhardt, A.; Bezerra, H.; Blankenberg, S.; Brunner, S.; Colson, P.; Deseda, G.C.; Dabboura, S.; Eckner, D.; et al. Left Ventricular Unloading Is Associated with Lower Mortality in Patients with Cardiogenic Shock Treated with Venoarterial Extracorporeal Membrane Oxygenation: Re-sults from an International, Multicenter Cohort Study. Circulation 2020, 142, 2095–2106. [Google Scholar] [CrossRef]
- Karami, M.; den Uil, C.A.; Ouweneel, D.M.; Scholte, N.T.; Engström, A.E.; Akin, S.; Lagrand, W.K.; Vlaar, A.P.; Jewbali, L.S.; Henriques, J.P. Mechanical circulatory support in cardiogenic shock from acute myocardial infarction: Impella CP/5.0 versus ECMO. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 164–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chommeloux, J.; Montero, S.; Franchineau, G.; Bréchot, N.; Hékimian, G.; Lebreton, G.; Le Guennec, L.; Bourcier, S.; Nieszkowska, A.; Leprince, P.; et al. Microcirculation Evolution in Patients on Venoarterial Extracorporeal Membrane Oxygenation for Refractory Cardiogenic Shock. Crit. Care Med. 2020, 48, e9–e17. [Google Scholar] [CrossRef]
- Sieweke, J.-T.; Berliner, D.; Tongers, J.; Napp, L.C.; Flierl, U.; Zauner, F.; Bauersachs, J.; Schäfer, A. Mortality in patients with cardiogenic shock treated with the Impella CP microaxial pump for isolated left ventricular failure. Eur. Heart J. Acute Cardiovasc. Care 2018, 9, 138–148. [Google Scholar] [CrossRef]
- Haberkorn, S.; Uwarow, A.; Haurand, J.; Jung, C.; Kelm, M.; Westenfeld, R.; Horn, P. Percutaneous left ventricular assist support is associated with less pulmonary congestion and lower rate of pneumonia in patients with cardiogenic shock. Open Heart 2020, 7, e001385. [Google Scholar] [CrossRef] [PubMed]
- Becher, P.M.; Twerenbold, R.; Schrage, B.; Schmack, B.; Sinning, C.R.; Fluschnik, N.; Schwarzl, M.; Waldeyer, C.; Seiffert, M.; Clemmensen, P.; et al. Risk prediction of in-hospital mortality in patients with venoarterial extracorporeal membrane oxygenation for cardiopulmonary support: The ECMO-ACCEPTS score. J. Crit. Care 2019, 56, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Ali, J.M.; Vuylsteke, A.; Fowles, J.-A.; Pettit, S.; Salaunkey, K.; Bhagra, S.; Lewis, C.; Parameshwar, J.; Kydd, A.; Patvardhan, C.; et al. Transfer of Patients with Cardiogenic Shock Using Veno-Arterial Extracorporeal Membrane Oxygenation. J. Cardiothorac. Vasc. Anesthesia 2020, 34, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Lang, C.N.; Kaier, K.; Zotzmann, V.; Stachon, P.; Pottgiesser, T.; von Zur Muehlen, C.; Zehender, M.; Duerschmied, D.; Schmid, B.; Bode, C.; et al. Cardiogenic shock: Incidence, survival and mechanical circulatory support usage 2007-2017-insights from a national registry. Clin. Res. Cardiol. 2021, 110, 1421–1430. [Google Scholar] [CrossRef]
- Karatolios, K.; Chatzis, G.; Markus, B.; Luesebrink, U.; Ahrens, H.; Divchev, D.; Syntila, S.; Jerrentrup, A.; Schieffer, B. Comparison of mechanical circulatory support with venoarterial extracorporeal membrane oxygenation or Impella for patients with cardiogenic shock: A propensity-matched analysis. Clin. Res. Cardiol. 2020, 110, 1404–1411. [Google Scholar] [CrossRef]
- Schäfer, A.; Westenfeld, R.; Sieweke, J.-T.; Zietzer, A.; Wiora, J.; Masiero, G.; Martinez, C.S.; Tarantini, G.; Werner, N. Complete Revascularisation in Impella-Supported Infarct-Related Cardiogenic Shock Patients Is Associated with Improved Mortality. Front. Cardiovasc. Med. 2021, 8, 678748. [Google Scholar] [CrossRef] [PubMed]
- Schurtz, G.; Rousse, N.; Saura, O.; Balmette, V.; Vincent, F.; Lamblin, N.; Porouchani, S.; Verdier, B.; Puymirat, E.; Robin, E.; et al. IMPELLA® or Extracorporeal Membrane Oxygenation for Left Ventricular Dominant Refractory Cardiogenic Shock. J. Clin. Med. 2021, 10, 759. [Google Scholar] [CrossRef]
- Hernández-Pérez, F.J.; Álvarez-Avelló, J.M.; Forteza, A.; Gómez-Bueno, M.; González, A.; López-Ibor, J.V.; Silva-Melchor, L.; Goicolea, J.; Martín, C.E.; Iranzo, R.; et al. Initial outcomes of a multidisciplinary network for the care of patients with cardiogenic shock. Rev. Esp. Cardiol. 2020, 74, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Karami, M.; Eriksen, E.; Ouweneel, D.M.; Claessen, B.E.; Vis, M.M.; Baan, J.; Beijk, M.; Packer, E.J.S.; Sjauw, K.D.; Engstrom, A. Long-term 5-year outcome of the randomized IM-PRESS in severe shock trial: Percutaneous mechanical circulatory support vs. intra-aortic balloon pump in cardiogenic shock after acute myocardial infarction. Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Lackermair, K.; Brunner, S.; Orban, M.; Peterss, S.; Orban, M.; Theiss, H.D.; Huber, B.C.; Juchem, G.; Born, F.; Boulesteix, A.-L.; et al. Outcome of patients treated with extracorporeal life support in cardiogenic shock complicating acute myocardial infarction: 1-year result from the ECLS-Shock study. Clin. Res. Cardiol. 2020, 110, 1412–1420. [Google Scholar] [CrossRef]
- Haurand, J.M.; Haberkorn, S.; Haschemi, J.; Oehler, D.; Aubin, H.; Akhyari, P.; Boeken, U.; Kelm, M.; Westenfeld, R.; Horn, P.; et al. Outcome of patients with non-ischaemic car-diogenic shock supported by percutaneous left ventricular assist device. ESC Heart Fail. 2021, 8, 3594–3602. [Google Scholar] [CrossRef]
- Mierke, J.; Loehn, T.; Ende, G.; Jahn, S.; Quick, S.; Speiser, U.; Jellinghaus, S.; Pfluecke, C.; Linke, A.; Ibrahim, K. Percutaneous Left Ventricular Assist Device Leads to Heart Rhythm Stabilisation in Cardiogenic Shock: Results from the Dresden Impella Registry. Heart Lung Circ. 2020, 30, 577–584. [Google Scholar] [CrossRef]
- Szczanowicz, L.; Majunke, N.; de Waha-Thiele, S.; Tietz, F.; Schürer, S.; Kirsch, K.; Desch, S.; Thiele, H.; Sandri, M. Predictors of Clinical Outcome After Early Veno-Arterial Extracorporeal Membrane Oxygenation in Cardiogenic Shock Complicating ST-Elevation Myocardial Infarction. J. Am. Coll. Cardiol. 2021, 33, E329–E335. [Google Scholar]
- Nersesian, G.; Potapov, E.V.; Nelki, V.; Stein, J.; Starck, C.; Falk, V.; Schoenrath, F.; Krackhardt, F.; Tschöpe, C.; Spillmann, F. Propensity score-based analysis of 30-day survival in car-diogenic shock patients supported with different microaxial left ventricular assist devices. J. Card. Surg. 2021, 36, 4141–4152. [Google Scholar] [CrossRef]
- Monteagudo-Vela, M.; Panoulas, V.; García-Saez, D.; de Robertis, F.; Stock, U.; Simon, A.R. Outcomes of heart transplantation in patients bridged with Impella 5.0: Comparison with native chest transplanted patients without preoperative mechanical cir-culatory support. Artif. Organs. 2021, 45, 254–262. [Google Scholar] [CrossRef]
- Toda, K.; Ako, J.; Hirayama, A.; Kinugawa, K.; Kobayashi, Y.; Ono, M.; Nishimura, T.; Sato, N.; Shindo, T.; Takayama, M.; et al. Three-year experience of catheter-based micro-axial left ventricular assist device, Impella, in Japanese patients: The first interim analysis of Japan registry for percutaneous ventricular assist device (J-PVAD). J. Artif. Organs 2022, 1–7. [Google Scholar] [CrossRef]
- Lazkani, M.; Murarka, S.; Kobayashi, A.; Seibolt, L.; Yang, T.; Pershad, A. A retrospective analysis of Impella use in all-comers: 1-year outcomes. J. Interv. Cardiol. 2017, 30, 577–583. [Google Scholar] [CrossRef]
- Basir, M.B.; Schreiber, T.L.; Grines, C.L.; Dixon, S.R.; Moses, J.W.; Maini, B.S.; Khandelwal, A.K.; Ohman, E.M.; O’Neill, W.W. Effect of Early Initiation of Mechanical Circulatory Support on Survival in Cardiogenic Shock. Am. J. Cardiol. 2017, 119, 845–851. [Google Scholar] [CrossRef]
- Meraj, P.M.; Doshi, R.; Schreiber, T.; Maini, B.; O’Neill, W.W. Impella 2.5 initiated prior to unprotected left main PCI in acute myo-cardial infarction complicated by cardiogenic shock improves early survival. J. Interv. Cardiol. 2017, 30, 256–263. [Google Scholar] [CrossRef]
- Alhussein, M.; Osten, M.; Horlick, E.; Ross, H.; Fan, E.; Rao, V.; Billia, F. Percutaneous left atrial decompression in adults with refractory cardiogenic shock supported with veno-arterial extracorporeal membrane oxygenation. J. Card. Surg. 2017, 32, 396–401. [Google Scholar] [CrossRef]
- Lorusso, R.; Gelsomino, S.; Parise, O.; Mendiratta, P.; Prodhan, P.; Rycus, P.; MacLaren, G.; Brogan, T.V.; Chen, Y.-S.; Maessen, J.; et al. Venoarterial Extracorporeal Membrane Oxygenation for Refractory Cardiogenic Shock in Elderly Patients: Trends in Application and Outcome from the Extracorporeal Life Support Organization (ELSO) Registry. Ann. Thorac. Surg. 2017, 104, 62–69. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, W.W.; Grines, C.; Schreiber, T.; Moses, J.; Maini, B.; Dixon, S.R.; Ohman, E.M. Analysis of outcomes for 15,259 US patients with acute myocardial infarction cardiogenic shock (AMICS) supported with the Impella device. Am. Heart J. 2018, 202, 33–38. [Google Scholar] [CrossRef]
- El Sibai, R.; Bachir, R.; El Sayed, M. ECMO use and mortality in adult patients with cardiogenic shock: A retrospective observational study in U.S. hospitals. BMC Emerg. Med. 2018, 18, 20. [Google Scholar] [CrossRef] [Green Version]
- Basir, M.B.; Schreiber, T.; Dixon, S.; Alaswad, K.; Patel, K.; Almany, S.; Khandelwal, A.; Hanson, I.; George, A.; Ashbrook, M. Feasibility of early mechanical circulatory support in acute myocardial infarction complicated by cardiogenic shock: The Detroit cardiogenic shock initiative. Catheter. Cardiovasc. Interv. 2018, 91, 454–461. [Google Scholar] [CrossRef]
- Esposito, M.L.; Jablonski, J.; Kras, A.; Krasney, S.; Kapur, N.K. Maximum level of mobility with axillary deployment of the Impella 5.0 is associated with improved survival. Int. J. Artif. Organs 2018, 41, 236–239. [Google Scholar] [CrossRef]
- Guenther, S.P.; Shudo, Y.; Hiesinger, W.; Banerjee, D. Prolonged veno-arterial extracorporeal life support for cardiac failure. Int. J. Artif. Organs 2018, 41, 437–444. [Google Scholar] [CrossRef]
- Sun, T.; Guy, A.; Sidhu, A.; Finlayson, G.; Grunau, B.; Ding, L.; Harle, S.; Dewar, L.; Cook, R.; Kanji, H.D. Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) for emergency cardiac support. J. Crit. Care 2018, 44, 31–38. [Google Scholar] [CrossRef]
- Kaki, A.; Blank, N.; Alraies, M.C.; Jani, A.; Shemesh, A.; Kajy, M.; Laktineh, A.; Hasan, R.; Gade, C.L.F.; Mohamad, T.; et al. Axillary Artery Access for Mechanical Circulatory Support Devices in Patients with Prohibitive Peripheral Arterial Disease Presenting with Cardiogenic Shock. Am. J. Cardiol. 2019, 123, 1715–1721. [Google Scholar] [CrossRef]
- Ba, M.R.F.; Kapur, N.K.; Patel, K.; Salam, M.A.; Schreiber, T.; Kaki, A.; Hanson, I.; Almany, S.; Timmis, S.; Dixon, S.; et al. Improved Outcomes Associated with the use of Shock Protocols: Updates from the National Cardiogenic Shock Initiative. Catheter. Cardiovasc. Interv. 2019, 93, 1173–1183. [Google Scholar] [CrossRef]
- Esposito, M.L.; Morine, K.J.; Annamalai, S.K.; O’Kelly, R.; Aghili, N.; Pedicini, R.; Breton, C.; Mullin, A.; Hamadeh, A.; Kiernan, M.S.; et al. Increased Plasma-Free Hemoglobin Levels Identify Hemolysis in Patients with Cardiogenic Shock and a Trans valvular Micro-Axial Flow Pump. Artif. Organs 2018, 43, 125–131. [Google Scholar] [CrossRef]
- Yourshaw, J.P.; Mishra, P.; Armstrong, M.C.; Ramu, B.; Craig, M.L.; Van Bakel, A.B.; Steinberg, D.H.; DiSalvo, T.G.; Tedford, R.J.; Houston, B.A. Effects of Percutaneous LVAD Support on Right Ventricular Load and Adaptation. J. Cardiovasc. Transl. Res. 2019, 12, 142–149. [Google Scholar] [CrossRef]
- O’Neill, B.P.; Cohen, M.G.; Basir, M.B.; Schreiber, T.; Kapur, N.K.; Dixon, S.; Khandelwal, A.K.; Grines, C.; Ohman, E.M.; O’Neill, W.W. Outcomes Among Patients Transferred for Revas-cularization with Impella for Acute Myocardial Infarction with Cardiogenic Shock from the cVAD Registry. Am. J. Cardiol. 2019, 123, 1214–1219. [Google Scholar] [CrossRef]
- Garan, A.R.; Takeda, K.; Salna, M.; Vandenberge, J.; Doshi, D.; Karmpaliotis, D.; Kirtane, A.J.; Takayama, H.; Kurlansky, P. Prospective Comparison of a Percutaneous Ventricular Assist Device and Venoarterial Extracorporeal Membrane Oxygenation for Patients with Cardiogenic Shock Fol-lowing Acute Myocardial Infarction. J. Am. Heart Assoc. 2019, 8, e012171. [Google Scholar] [CrossRef] [Green Version]
- Hritani, A.W.; Wani, A.S.; Olet, S.; Lauterbach, C.J.; Allaqaband, S.Q.; Bajwa, T.; Jan, M.F. Secular Trend in the Use and Implementation of Impella in High-Risk Percutaneous Coronary Intervention and Cardiogenic Shock: A Real-World Experience. J. Am. Coll. Cardiol. 2019, 31, E265–E270. [Google Scholar]
- Rohm, C.L.; Gadidov, B.; Leitson, M.; Ray, H.E.; Prasad, R. Predictors of Mortality and Outcomes of Acute Severe Cardiogenic Shock Treated with the Impella Device. Am. J. Cardiol. 2019, 124, 499–504. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.M.; Lipinski, J.; Al-Kindi, S.G.; Patel, T.; Saric, P.; Li, J.; Nadeem, F.; Ladas, T.; Alaiti, A.; Phillips, A.; et al. Simultaneous Venoarterial Extracorporeal Membrane Oxygenation and Percutaneous Left Ventricular Decompression Therapy with Impella Is Associated with Improved Outcomes in Refractory Cardiogenic Shock. ASAIO J. 2019, 65, 21–28. [Google Scholar] [CrossRef]
- Dhruva, S.S.; Ross, J.; Mortazavi, B.J.; Hurley, N.C.; Krumholz, H.M.; Curtis, J.P.; Berkowitz, A.; Masoudi, F.A.; Messenger, J.C.; Parzynski, C.S.; et al. Association of Use of an Intravascular Microaxial Left Ventricular Assist Device vs Intra-aortic Balloon Pump with In-Hospital Mortality and Major Bleeding Among Patients with Acute Myocardial Infarction Complicated by Cardiogenic Shock. JAMA 2020, 323, 734. [Google Scholar] [CrossRef]
- Kajy, M.; Laktineh, A.; Blank, N.; Tayal, R.; Tanveer, S.; Mohamad, T.; Elder, M.; Schreiber, T.; Kaki, A. Deploying Mechanical Circulatory Support Via the Ax-illary Artery in Cardiogenic Shock and High-Risk Percutaneous Coronary Intervention. Am. J. Cardiol. 2020, 128, 127–133. [Google Scholar] [CrossRef]
- Lemor, A.; Dehkordi, S.H.H.; Basir, M.B.; Villablanca, P.A.; Jain, T.; Koenig, G.C.; Alaswad, K.; Moses, J.W.; Kapur, N.K.; O’Neill, W. Impella Versus Extracorporeal Membrane Oxygenation for Acute Myocardial Infarction Cardiogenic Shock. Cardiovasc. Revascularization Med. 2020, 21, 1465–1471. [Google Scholar] [CrossRef]
- Fahad, F.; Shaukat, M.H.S.; Yager, N. Incidence and Outcomes of Acute Kidney Injury Requiring Renal Replacement Therapy in Patients on Percutaneous Mechanical Circulatory Support with Impella-CP for Cardiogenic Shock. Cureus 2020, 12, e6591. [Google Scholar] [CrossRef] [Green Version]
- Hassett, C.E.; Cho, S.-M.; Hasan, S.; Rice, C.J.; Migdady, I.; Starling, R.C.; Soltesz, E.; Uchino, K. Ischemic Stroke and Intracranial Hemorrhages During Impella Cardiac Support. ASAIO J. 2020, 66, e105–e109. [Google Scholar] [CrossRef]
- Trpkov, C.; Gibson, J.D.; Miller, R.J.H.; Grant, A.D.M.; Schnell, G.; Har, B.J.; Clarke, K. Percutaneous Left Ventricular Assist Device in Car-diogenic Shock: A Five-Year Single Canadian Center Initial Experience. CJC Open 2020, 2, 370–378. [Google Scholar] [CrossRef]
- Vallabhajosyula, S.; Dunlay, S.M.; Barsness, G.W.; Miller, P.E.; Cheungpasitporn, W.; Stulak, J.M.; Rihal, C.S.; Holmes, D.R.; Bell, M.R.; Miller, V.M. Sex Disparities in the Use and Outcomes of Temporary Mechanical Circulatory Support for Acute Myocardial Infarction-Cardiogenic Shock. CJC Open 2020, 2, 462–472. [Google Scholar] [CrossRef]
- Sonu, G.; Rupak, D.; Bishoy, H.; Abhishek, D.; Gautam, K.; Rajesh, S.; Adam, E.B. The Impact of Atrial Fibrillation on In-Hospital Outcomes in Patients with Acute Myocardial Infarction Complicated by Cardiogenic Shock Undergoing Coronary Revascularization with Percutaneous Ventricular Assist Device Support. J. Atr. Fibrillation 2020, 12, 2179. [Google Scholar]
- Boshara, A.; Patel, A.; Alasaad, M.; Dutcheshen, K.J.N.; LaLonde, T.A.; Schreiber, T.L.; Mehta, R.H.M.; Kaki, A.; Rosman, H.S. Cardiogenic Shock Complicating Acute Myocardial Infarction Treated with Percutaneous Coronary Intervention Supported by Impella: Implications of Advanced Age and Refractory Shock on Outcomes. Crit. Care Explor. 2021, 3, e0447. [Google Scholar] [CrossRef]
- Char, S.; Fried, J.; Melehy, A.; Mehta, S.; Ning, Y.; Kurlansky, P.; Takeda, K. Clinical efficacy of direct or indirect left ventricular unloading during venoarterial extracorporeal membrane oxygenation for primary cardiogenic shock. J. Thorac. Cardiovasc. Surg. 2021, 165, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.; Mehta, R.H.; O’Neill, W.; Kapur, N.K.; Lalonde, T.; Ohman, M.; Ghiu, I.; Chen-Hsing, Y.; Dutcheshen, K.; Schreiber, T.; et al. Clinical features and outcomes in patients with car-diogenic shock complicating acute myocardial infarction: Early vs recent experience with impella. Am. Heart J. 2021, 238, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Montfort, J.; Sinha, S.S.; Thayer, K.L.; Whitehead, E.H.; Pahuja, M.; Garan, A.R.; Mahr, C.; Haywood, J.L.; Harwani, N.M.; Schaeffer, A.; et al. Clinical Outcomes Associated with Acute Mechanical Circulatory Support Utilization in Heart Failure Related Cardiogenic Shock. Circ. Heart Fail. 2021, 14, e007924. [Google Scholar] [CrossRef]
- Pahuja, M.; Ranka, S.; Chehab, O.; Mishra, T.; Akintoye, E.; Adegbala, O.; Yassin, A.S.; Ando, A.T.; Thayer, K.L.; Shah, P.; et al. Incidence and clinical outcomes of bleeding compli-cations and acute limb ischemia in STEMI and cardiogenic shock. Catheter. Cardiovasc. Interv. 2021, 97, 1129–1138. [Google Scholar] [CrossRef]
- Nelson, D.W.; Sundararajan, S.; Klein, E.; Joyce, L.D.; Durham, L.A.; Joyce, D.L.; Mohammed, A.A. Sustained Use of the Impella 5.0 Heart Pump Enables Bridge to Clinical Decisions in 34 Patients. Tex. Heart Inst. J. 2021, 48, e207260. [Google Scholar] [CrossRef] [PubMed]
- Diakos, N.A.; Thayer, K.; Swain, L.; Goud, M.; Jain, P.; Kapur, N.K. Systemic Inflammatory Burden Correlates with Severity and Predicts Outcomes in Patients with Cardiogenic Shock Supported by a Percutaneous Mechanical Assist Device. J. Cardiovasc. Transl. Res. 2021, 14, 476–483. [Google Scholar] [CrossRef]
- Carter, K.T.; O’Brien, R.; Larson, S.B.; Creswell, L.L.; Kutcher, M.; Baran, D.A.; Copeland, J.G.; Copeland, H. Venoarterial extracorporeal membrane oxygenation is a viable option as a bridge to heart transplant. J. Thorac. Cardiovasc. Surg. 2020, 163, 140–147. [Google Scholar] [CrossRef]
- Liao, X.-Z.; Zhou, Z.; Cheng, Z.; Yang, X.-Y.; Zhou, X.; Li, B.-F.; Feng, X. The Prognostic Risk Factors of ECMO in Patients with Cardiogenic Shock: A Retrospective Cohort Analysis. Heart Surg. Forum 2017, 20, 170–177. [Google Scholar] [CrossRef] [Green Version]
- Chong, S.-Z.; Fang, C.-Y.; Fang, H.-Y.; Chen, H.-C.; Chen, C.-J.; Yang, C.-H.; Hang, C.-L.; Yip, H.-K.; Wu, C.-J.; Lee, W.-C. Associations with the In-Hospital Survival Following Extracorporeal Membrane Oxygenation in Adult Acute Fulminant Myocarditis. J. Clin. Med. 2018, 7, 452. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, M.; Asaumi, Y.; Nakamura, Y.; Nakatani, T.; Nagai, T.; Kanaya, T.; Kawakami, S.; Honda, S.; Kataoka, Y.; Nakajima, S.; et al. Clinical determinants of successful weaning from extracorporeal membrane oxygenation in patients with fulminant myocarditis. ESC Heart Fail. 2018, 5, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Liao, X.; Li, B.; Cheng, Z. Extracorporeal membrane oxygenation in adult patients with acute fulminant myocarditis: Clinical outcomes and risk factor analysis. Herz 2018, 43, 728–732. [Google Scholar] [CrossRef]
- Huang, C.C.; Hsu, J.C.; Wu, Y.W.; Ke, S.R.; Huang, J.H.; Chiu, K.M.; Liao, P.-C. Implementation of extracorporeal membrane oxygenation before primary percutaneous coronary intervention may improve the survival of patients with ST-segment elevation myo-cardial infarction and refractory cardiogenic shock. Int. J. Cardiol. 2018, 269, 45–50. [Google Scholar] [CrossRef]
- Yeh, Y.-C.; Lee, C.-T.; Wang, C.-H.; Tu, Y.-K.; Lai, C.-H.; Wang, Y.-C.; Chao, A.; Huang, C.-H.; Cheng, Y.-J.; NTUH Center of Microcirculation Medical Research (NCMMR). Investigation of microcirculation in patients with venoarterial extracorporeal membrane oxygenation life support. Crit. Care 2018, 22, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toda, K.; Fujita, T.; Seguchi, O.; Yanase, M.; Nakatani, T. Role of percutaneous veno-arterial extracorporeal membrane oxygenation as bridge to left ventricular assist device. J. Artif. Organs 2017, 21, 39–45. [Google Scholar] [CrossRef]
- Hong, D.; Choi, K.H.; Cho, Y.H.; Cho, S.H.; Park, S.J.; Kim, D.; Park, T.K.; Lee, J.M.; Bin Song, Y.; Choi, J.-O.; et al. Multidisciplinary team approach in acute myocardial infarction patients undergoing veno-arterial extracorporeal membrane oxygenation. Ann. Intensiv. Care 2020, 10, 83. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.H.; Yang, J.H.; Hong, D.; Park, T.K.; Lee, J.M.; Bin Song, Y.; Hahn, J.-Y.; Choi, S.-H.; Choi, J.-H.; Chung, S.R.; et al. Optimal Timing of Venoarterial-Extracorporeal Membrane Oxygenation in Acute Myocardial Infarction Patients Suffering from Refractory Cardiogenic Shock. Circ. J. 2020, 84, 1502–1510. [Google Scholar] [CrossRef]
- Kondo, T.; Morimoto, R.; Mutsuga, M.; Fujimoto, K.; Okumura, T.; Shibata, N.; Kazama, S.; Kimira, Y.; Oishi, H.; Kuwayama, T.; et al. Comparison of Impella 5.0 and extracorporeal left ventricular assist device in patients with cardiogenic shock. Int. J. Artif. Organs 2021, 44, 846–853. [Google Scholar] [CrossRef]
- Tadokoro, N.; Fukushima, S.; Minami, K.; Taguchi, T.; Saito, T.; Kawamoto, N.; Kakuta, T.; Seguchi, O.; Watanabe, T.; Doi, S.N.; et al. Efficacy of central extracorporeal life support for patients with fulminant myocarditis and cardiogenic shock. Eur. J. Cardio-Thoracic. Surg. 2021, 60, 1184–1192. [Google Scholar] [CrossRef]
- Shin, D.G.; Shin, S.D.; Han, D.; Kang, M.K.; Lee, S.H.; Kim, J.; Cho, J.-R.; Kim, K.; Choi, S.; Lee, N. Features of Patients Receiving Extracorporeal Membrane Oxygen-ation Relative to Cardiogenic Shock Onset: A Single-Centre Experience. Medicina (Kaunas) 2021, 57, 886. [Google Scholar] [CrossRef]
- Wang, H.; Chen, C.; Li, B.; Cheng, Z.; Wang, Z.; Huang, X.; Xian, M.; Zhuang, J.; Chen, J.; Zhou, C.; et al. Nomogram to predict survival outcome of patients with veno-arterial extracorporeal membrane oxygenation after refractory cardiogenic shock. Postgrad. Med. 2021, 134, 37–46. [Google Scholar] [CrossRef] [PubMed]
- El Sibai, R.; Bachir, R.; El Sayed, M. Outcomes in Cardiogenic Shock Patients with Extracorporeal Membrane Oxygenation Use: A Matched Cohort Study in Hospitals across the United States. Biomed Res. Int. 2018, 2018, 2428648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abouelwafa, M.; Radwan, W.; Abdelfattah, A.; Abdelbary, A.; Khaled, M.; Samy, W.; Yousry, M.; Saeed, A.; Saad, M. The usefulness of Veno-Arterial Extra-corporeal Membranous Oxygenation in Patients with Cardiogenic Shock. Open Access Maced. J. Med. Sci. 2019, 7, 1768–1773. [Google Scholar] [CrossRef] [Green Version]
- Loehn, T.; O’Neill, W.W.; Lange, B.; Pfluecke, C.; Schweigler, T.; Mierke, J.; Waessnig, N.; Mahlmann, A.; Youssef, A.; Speiser, U.; et al. Long term survival after early unloading with Impella CP® in acute myocardial infarction complicated by cardiogenic shock. Eur. Heart J. Acute Cardiovasc. Care 2018, 9, 149–157. [Google Scholar] [CrossRef]
- Scherer, C.; Lüsebrink, E.; Kupka, D.; Stocker, T.J.; Stark, K.; Stremmel, C.; Orban, M.; Petzold, T.; Germayer, A.; Mauthe, K.; et al. Long-Term Clinical Outcome of Cardiogenic Shock Patients Undergoing Impella CP Treatment vs. Standard of Care. J. Clin. Med. 2020, 9, 3803. [Google Scholar] [CrossRef]
- Lee, S.Y.; Jeon, K.-H.; Lee, H.J.; Kim, J.-B.; Jang, H.-J.; Kim, J.S.; Kim, T.H.; Park, J.-S.; Choi, R.K.; Choi, Y.J. Complications of veno-arterial extracorporeal membrane oxygenation for refractory cardiogenic shock or cardiac arrest. Int. J. Artif. Organs 2019, 43, 37–44. [Google Scholar] [CrossRef]
- Kim, D.; Park, Y.; Choi, K.H.; Park, T.K.; Lee, J.M.; Cho, Y.H.; Choi, J.-O.; Jeon, E.-S.; Yang, J.H. Prognostic Implication of RV Coupling to Pulmonary Circulation for Successful Weaning from Extracorporeal Membrane Oxygenation. JACC Cardiovasc. Imaging 2021, 14, 1523–1531. [Google Scholar] [CrossRef] [PubMed]
- Nersesian, G.; Tschöpe, C.; Spillmann, F.; Gromann, T.; Roehrich, L.; Mueller, M.; Mulzer, J.; Starck, C.; Falk, V.; Schoenrath, F.; et al. Prediction of survival of patients in cardiogenic shock treated by surgically implanted Impella 5+ short-term left ventricular assist device. Interact. Cardiovasc. Thorac. Surg. 2020, 31, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Yang, D. Extracorporeal Membrane Oxygenation in Refractory Cardiogenic Shock. Heart Surg. Forum 2020, 23, E888–E894. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011] [Internet]. 2011. Available online: www.handbook.cochrane.org (accessed on 30 May 2022).
- Tarricone, R.; Callea, G.; Ogorevc, M.; Prevolnik Rupel, V. Improving the Methods for the Economic Evaluation of Medical Devices: Medical devices distinctive features. Health Econ. 2017, 26, 70–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarricone, R.; Torbica, A.; Drummond, M. Challenges in the Assessment of Medical Devices: The MedtecHTA Project: Challenges in the assessment of medical devices. Health Econ. 2017, 26, 5–12. [Google Scholar] [CrossRef] [Green Version]
- Tarricone, R.; Boscolo, P.R.; Armeni, P. What type of clinical evidence is needed to assess medical devices? Eur. Respir Rev. 2016, 25, 259–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarricone, R.; Torbica, A.; Drummond, M.; for the MedtecHTA Project Group. Key Recommendations from the MedtecHTA Project: Improving the conduct and use of HTA for medical devices. Health Econ. 2017, 26, 145–152. [Google Scholar] [CrossRef] [Green Version]
- Batchelor, R.J.; Wheelahan, A.; Zheng, W.C.; Stub, D.; Yang, Y.; Chan, W. Impella versus Venoarterial Extracorporeal Membrane Oxygenation for Acute Myocardial Infarction Cardiogenic Shock: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 3955. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Ahsan, M.J.; Ikram, S.; Lateef, N.; Khan, B.A.; Tabassum, S.; Naeem, A.; Qavi, A.H.; Ardhanari, S.; Goldsweig, A.M. Impella Versus Extracorporeal Membranous Oxygenation (ECMO) for Cardiogenic Shock: A Systematic Review and Meta-analysis. Curr. Probl. Cardiol. 2023, 48, 101427. [Google Scholar] [CrossRef] [PubMed]
- Abusnina, W.; Ismayl, M.; Al-Abdouh, A.; Ganesan, V.; Mostafa, M.R.; Hallak, O.; Peterson, E.; Abdou, M.; Goldsweig, A.M.; Aboeata, A.; et al. Impella versus extracorporeal membrane oxygenation in cardiogenic shock: A systematic review and meta-analysis. Shock 2022, 58, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Drummond, M.; Tarricone, R.; Torbica, A. European union regulation of health technology assessment: What is required for it to succeed? Eur. J. Health Econ. 2022, 23, 913–915. [Google Scholar] [CrossRef]
- Tarricone, R.; Amatucci, F.; Armeni, P.; Banks, H.; Borsoi, L.; Callea, G.; Ciani, O.; Costa, F.; Federici, C.; Torbica, A.; et al. Establishing a national HTA program for medical devices in Italy: Overhauling a fragmented system to ensure value and equal access to new medical technologies. Health Policy 2021, 125, 602–608. [Google Scholar] [CrossRef]
- Harmonization Of Health Technology Assessment Across The European Union: Lessons For The United States [Internet]. 2021. Available online: http://www.healthaffairs.org/do/10.1377/forefront.20211130.24462/full/ (accessed on 30 May 2022).
- Naidu, S.S.; Baran, D.A.; Jentzer, J.C.; Hollenberg, S.M.; van Diepen, S.; Basir, M.B.; Grines, C.L.; Diercks, D.B.; Hall, S.; Kapur, N.K.; et al. SCAI SHOCK Stage Classification Expert Consensus Update: A Review and Incorporation of Validation Studies. J. Am. Coll. Cardiol. 2022, 79, 933–946. [Google Scholar] [CrossRef]
- Dhruva, S.S.; Ross, J.S.; Mortazavi, B.J.; Hurley, N.C.; Krumholz, H.M.; Curtis, J.P.; Berkowitz, A.P.; Masoudi, F.A.; Messenger, J.C.; Parzynski, C.S.; et al. Use of Mechanical Circulatory Support Devices Among Patients with Acute Myocardial Infarction Complicated by Cardiogenic Shock. JAMA Netw. Open 2021, 4, e2037748. [Google Scholar] [CrossRef] [PubMed]
- de Lemos, J.A.; Nallamothu, B.K. The Challenges of Observational Comparative Effectiveness Research. Circulation 2020, 141, 237–239. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcomes | N | % | Included in Meta-Analysis |
|---|---|---|---|
| Mortality | 100 | 98% | Yes |
| Bleeding | 60 | 59% | Yes |
| Duration of support | 60 | 59% | Yes |
| Ischemic stroke | 50 | 49% | Yes |
| Renal failure | 44 | 43% | Yes |
| Limb ischemia | 40 | 39% | Yes |
| Bridge to LVAD | 30 | 29% | Yes |
| Weaning | 27 | 26% | Yes |
| Days in hospital/ICU | 25 | 25% | No |
| Bridge to transplant | 23 | 23% | Yes |
| Hemolysis | 22 | 22% | No |
| Sepsis | 20 | 20% | No |
| Myocardial recovery | 10 | 10% | Yes |
| Major device malfunction | 8 | 8% | No |
| Average Impella pump flow | 6 | 6% | No |
| Device exchange | 5 | 5% | No |
| Resource use | 5 | 5% | No |
| Aortic valve injury | 3 | 3% | No |
| Mitral valve injury | 3 | 3% | No |
| LV perforation | 0 | 0% | No |
| Aortic dissection | 0 | 0% | No |
| Early mobilization and physiotherapy | 0 | 0% | No |
| Average Impella performance level | 0 | 0% | No |
| Quality of life | 0 | 0% | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ardito, V.; Sarucanian, L.; Rognoni, C.; Pieri, M.; Scandroglio, A.M.; Tarricone, R. Impella Versus VA-ECMO for Patients with Cardiogenic Shock: Comprehensive Systematic Literature Review and Meta-Analyses. J. Cardiovasc. Dev. Dis. 2023, 10, 158. https://doi.org/10.3390/jcdd10040158
Ardito V, Sarucanian L, Rognoni C, Pieri M, Scandroglio AM, Tarricone R. Impella Versus VA-ECMO for Patients with Cardiogenic Shock: Comprehensive Systematic Literature Review and Meta-Analyses. Journal of Cardiovascular Development and Disease. 2023; 10(4):158. https://doi.org/10.3390/jcdd10040158
Chicago/Turabian StyleArdito, Vittoria, Lilit Sarucanian, Carla Rognoni, Marina Pieri, Anna Mara Scandroglio, and Rosanna Tarricone. 2023. "Impella Versus VA-ECMO for Patients with Cardiogenic Shock: Comprehensive Systematic Literature Review and Meta-Analyses" Journal of Cardiovascular Development and Disease 10, no. 4: 158. https://doi.org/10.3390/jcdd10040158
APA StyleArdito, V., Sarucanian, L., Rognoni, C., Pieri, M., Scandroglio, A. M., & Tarricone, R. (2023). Impella Versus VA-ECMO for Patients with Cardiogenic Shock: Comprehensive Systematic Literature Review and Meta-Analyses. Journal of Cardiovascular Development and Disease, 10(4), 158. https://doi.org/10.3390/jcdd10040158