
The Role of Multidisciplinary Approaches in the Treatment of Patients with Heart Failure and Coagulopathy of COVID-19

 ,
,  and
and 
Abstract
1. Introduction
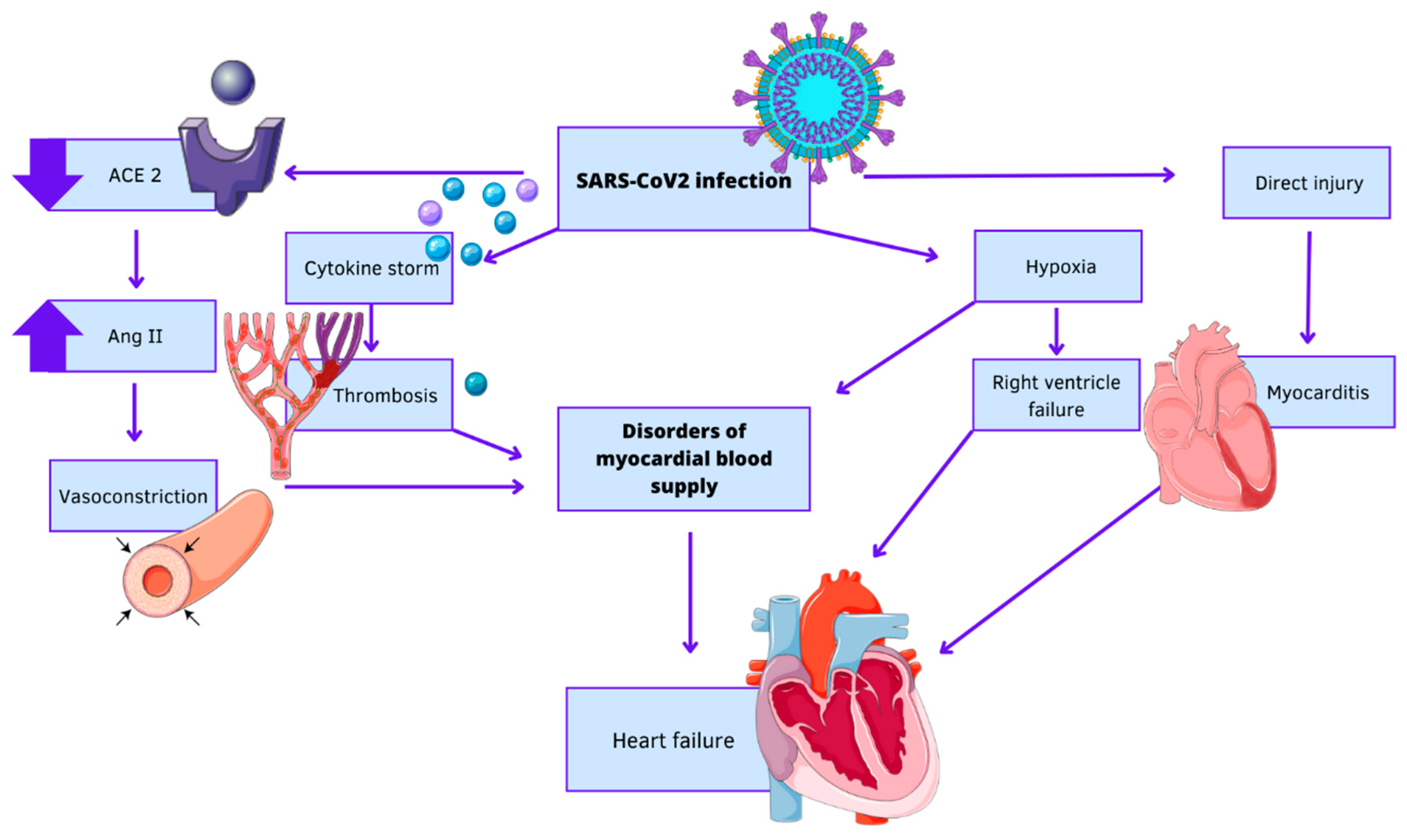
2. COVID-19 and Heart Failure
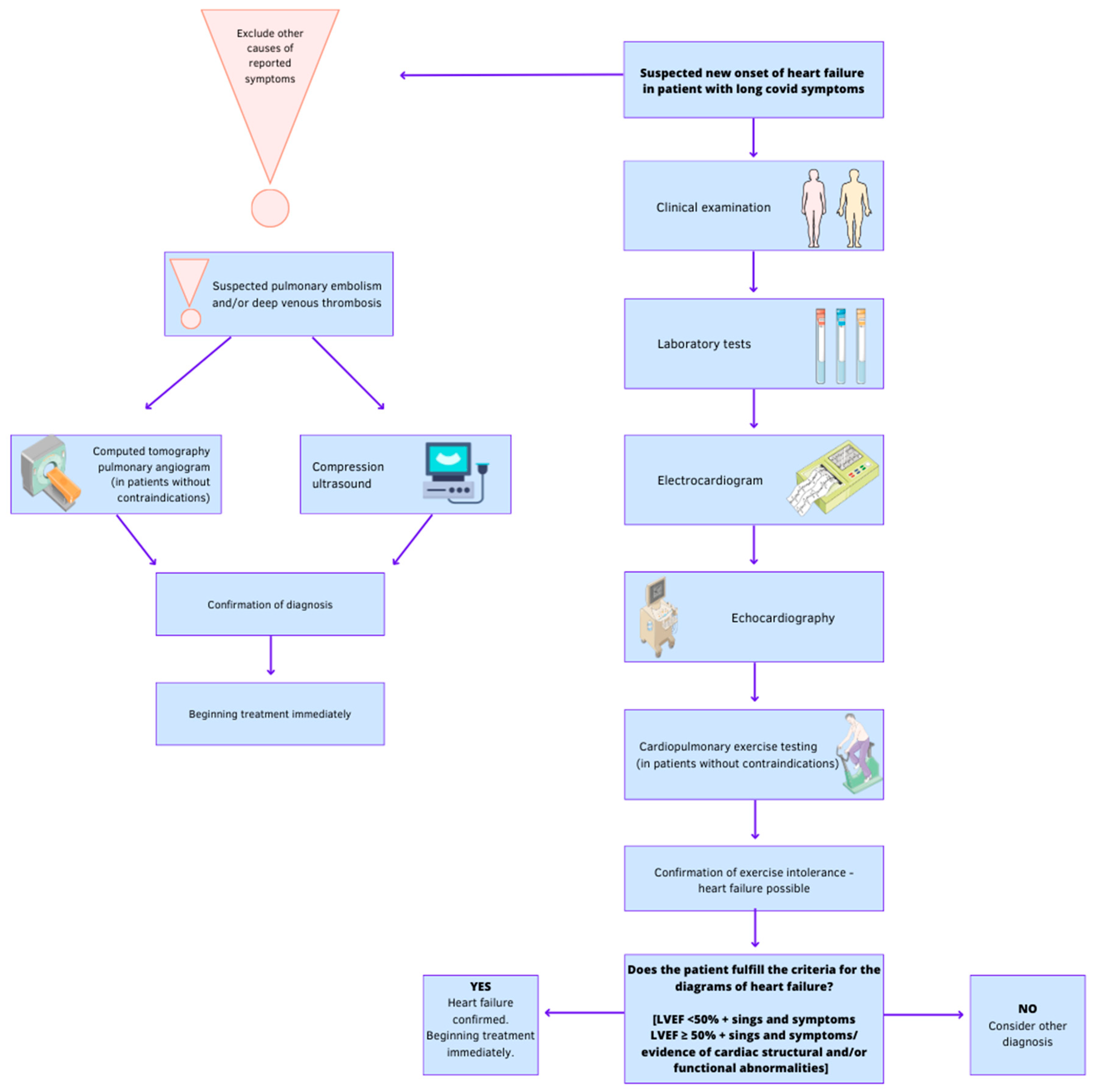
3. Diagnosis of Heart Failure in Patients after COVID-19
3.1. Clinical Examination
3.2. Laboratory Tests
- concentration of natriuretic peptides in plasma—to exclude HF: in a patient without acute worsening of symptoms, HF is unlikely when BNP < 35 pg/mL (<105 pg/mL in atrial fibrillation), NT-proBNP < 125 pg/mL (<365 pg/mL in atrial fibrillation);
- arterial blood gas analysis for detection of respiratory failure;
- serum troponin for detection of acute coronary syndrome (ACS);
- blood urea nitrogen, serum creatinine, electrolytes—for the detection of renal dysfunction;
- full blood count—anemia may exacerbate or cause CHF;
- transferrin, ferritin, signs of iron deficiency, most often of a functional nature—reduced transferrin iron saturation; a decrease in ferritin usually occurs only with absolute iron deficiency (it may not occur in the presence of inflammation);
- inflammatory cytokines (C-reactive protein, procalcitonin)—for the diagnosis of infection;
- increased activity of aminotransferases and lactate dehydrogenase (LDH), increased concentrations of bilirubin in plasma—in patients with venous stasis in the systemic circulation, with hepatomegaly;
- the concentration of thyroid stimulating hormone (TSH), because thyroid disease can mimic or worsen the symptoms of HF;
- D-dimer—when pulmonary embolism (PE) is suspected.
3.3. Electrocardiogram (ECG)
3.4. Chest Radiograph
3.5. Echocardiography
- Left ventricular systolic function—by analysing segmental and global left ventricular contractility and left ventricular ejection fraction (LVEF) measurement (Simpson method; <40% indicates significant left ventricular systolic dysfunction; values 41–49% are considered the so-called grey zone and one of the diagnostic criteria HFmrEF—a complete differential diagnosis of noncardiac causes of symptoms is necessary, as in HFpEF) [12].
- Left ventricular diastolic function—transmitral E/A ratio and E velocity deceleration time (DT), e’ velocity (average and absolute value of septal and lateral side) of the mitral annulus by pulsed tissue Doppler, E/e’ ratio, and the estimate of systolic pulmonary artery pressure (sPAP) derived from tricuspid regurgitation (TR) velocity [69].
- Anatomical abnormalities, hypertrophy, dilation of the heart chambers, valvular defects, congenital defects. Additional evaluation of many parameters of cardiac structure and function is of particular importance in differential diagnosis, especially with LVEF <40%. In some cases (e.g., poor imaging conditions on transthoracic examination, suspected prosthetic valve dysfunction, detection of a thrombus in the left ear in patients with atrial fibrillation, diagnosis of bacterial endocarditis or congenital defects), transoesophageal echocardiography is indicated [70].
- Signs of PE—dilation of the right ventricle (RV), pulmonary ejection acceleration time <60 ms with a peak systolic tricuspid valve gradient < 60 mmHg [63]. Echocardiographic examination is not mandatory as part of the routine diagnostic workup in haemodynamically stable patients with suspected PE. In case of suspected high-risk PE, the absence of echocardiographic signs of RV overload or dysfunction practically excludes PE as the cause of hemodynamic instability [71].
3.6. Computed Tomographic Pulmonary Angiography (CTPA)
3.7. Compression Ultrasonography (CUS)
3.8. Cardiopulmonary Exercise Testing (CPET)
4. Treatment of Heart Failure after COVID-19
5. COVID-19 and Coagulopathy
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Da Rosa Mesquita, R.; Francelino Silva, L.C., Jr.; Santos Santana, F.M.; Farias de Oliveira, T.; Campos Alcântara, R.; Monteiro Arnozo, G.; Rodrigues da Silva Filho, E.; Galdino Dos Santos, A.G.; Oliveira da Cunha, E.J.; Salgueiro de Aquino, S.H.; et al. Clinical manifestations of COVID-19 in the general population: Systematic review. Wien. Klin. Wochenschr. 2021, 133, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Bielecka-Dabrowa, A.; Cichocka-Radwan, A.; Lewek, J.; Pawliczak, F.; Maciejewski, M.; Banach, M. Cardiac manifestations of COVID-19. Rev. Cardiovasc. Med. 2021, 22, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062, Erratum in Lancet 2020, 395, 1038. [Google Scholar] [CrossRef] [PubMed]
- Brojakowska, A.; Narula, J.; Shimony, R.; Bander, J. Clinical implications of SARS-CoV-2 interaction with renin angiotensin system: JACC review topic of the week. J. Am. Coll. Cardiol. 2020, 75, 3085–3095. [Google Scholar] [CrossRef] [PubMed]
- Beyerstedt, S.; Casaro, E.B.; Rangel, É.B. COVID-19: Angiotensin-converting enzyme 2 (ACE2) expression and tissue susceptibility to SARS-CoV-2 infection. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 905–919. [Google Scholar] [CrossRef] [PubMed]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef]
- Chudzik, M.; Lewek, J.; Kapusta, J.; Banach, M.; Jankowski, P.; Bielecka-Dabrowa, A. Predictors of Long COVID in Patients without Comorbidities: Data from the Polish Long-COVID Cardiovascular (PoLoCOV-CVD) Study. J. Clin. Med. 2022, 11, 4980. [Google Scholar] [CrossRef]
- Braunwald, E. Cardiovascular Medicine at the Turn of the Millennium: Triumphs, Concerns, and Opportunities. N. Engl. J. Med. 1997, 337, 1360–1369. [Google Scholar] [CrossRef]
- GBD 2017 Collaborators on the Incidence and Prevalence of Disease and Injuries. Global, regional and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Bozkurt, B.; Coats, A.J.S.; Tsutsui, H.; Abdelhamid, C.M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Bohm, M.; Butler, J.; et al. Universal definition and classification of heart failure: A report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur. J. Heart Fail. 2021, 23, 352–380. [Google Scholar] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Owan, T.E.; Hodge, D.O.; Herges, R.M.; Jacobsen, S.J.; Roger, V.L.; Redfield, M.M. Trends in Prevalence and Outcome of Heart Failure with Preserved Ejection Fraction. N. Engl. J. Med. 2006, 355, 251–259. [Google Scholar] [CrossRef]
- Tanai, E.; Frantz, S. Pathophysiology of Heart Failure. Compr. Physiol. 2015, 6, 187–214. [Google Scholar] [CrossRef] [PubMed]
- Xiao, H.; Li, H.; Wang, J.-J.; Zhang, J.-S.; Shen, J.; An, X.-B.; Zhang, C.-C.; Wu, J.-M.; Song, Y.; Wang, X.-Y.; et al. IL-18 cleavage triggers cardiac inflammation and fibrosis upon β-adrenergic insult. Eur. Heart J. 2018, 39, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Adamo, L.; Staloch, L.J.; Rocha-Resende, C.; Matkovich, S.J.; Jiang, W.; Bajpai, G.; Weinheimer, C.J.; Kovacs, A.; Schilling, J.D.; Barger, P.M.; et al. Modulation of subsets of cardiac B lymphocytes improves cardiac function after acute injury. J. Clin. Investig. 2018, 3, e120137. [Google Scholar] [CrossRef] [PubMed]
- Reina-Couto, M.; Pereira-Terra, P.; Quelhas-Santos, J.; Silva-Pereira, C.; Albino-Teixeira, A.; Sousa, T. Inflammation in Human Heart Failure: Major Mediators and Therapeutic Targets. Front. Physiol. 2021, 12, 746494. [Google Scholar] [CrossRef]
- Tromp, J.; Khan, M.A.; Klip, I.T.; Meyer, S.; de Boer, R.A.; Jaarsma, T.; Hillege, H.; van Veldhuisen, D.J.; van der Meer, P.; Voors, A.A. Biomarker profiles in heart failure patients with preserved and reduced ejection fraction. J. Am. Heart Assoc. 2017, 6, e003989. [Google Scholar] [CrossRef]
- Tromp, J.; Westenbrink, B.D.; Ouwerkerk, W.; van Veldhuisen, D.J.; Samani, N.J.; Ponikowski, P.; Metra, M.; Anker, S.D.; Cleland, J.G.; Dickstein, K.; et al. Identifying Pathophysiological Mechanisms in Heart Failure with Reduced Versus Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2018, 72, 1081–1090. [Google Scholar] [CrossRef]
- Dubrock, H.M.; AbouEzzeddine, O.F.; Redfield, M.M. High-sensitivity C-reactive protein in heart failure with preserved ejection fraction. PLoS ONE 2018, 13, e0201836. [Google Scholar] [CrossRef]
- Paulus, W.J.; Zile, M.R. From Systemic Inflammation to Myocardial Fibrosis: The heart failure with preserved ejection fraction paradigm revisited. Circ. Res. 2021, 128, 1451–1467. [Google Scholar] [CrossRef] [PubMed]
- Santhanakrishnan, R.; Chong, J.P.; Ng, T.P.; Ling, L.H.; Sim, D.; Leong, K.T.; Yeo, P.S.; Ong, H.Y.; Jaufeerally, F.; Wong, R.; et al. Growth differentiation factor 15, ST2, high-sensitivity troponin T, and N-terminal pro brain natriuretic peptide in heart failure with preserved vs. reduced ejection fraction. Eur. J. Heart Fail. 2012, 14, 1338–1347. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, J.; Sugiyama, S.; Nozaki, T.; Sugamura, K.; Konishi, M.; Ohba, K.; Matsuzawa, Y.; Akiyama, E.; Yamamoto, E.; Sakamoto, K.; et al. Pentraxin 3 Is a New Inflammatory Marker Correlated with Left Ventricular Diastolic Dysfunction and Heart Failure With Normal Ejection Fraction. J. Am. Coll. Cardiol. 2011, 57, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Chuda-Wietczak, A.; Sakowicz, A.; Tycinska, A.; Bytyci, I.; Bielecka-Dabrowa, A. The GLVC scoring system: A single-center model for predicting survival and hospitalization in patients with heart failure. Ir. J. Med. Sci. 2023, 1–14. [Google Scholar] [CrossRef]
- Ferro, M.D.; Bussani, R.; Paldino, A.; Nuzzi, V.; Collesi, C.; Zentilin, L.; Schneider, E.; Correa, R.; Silvestri, F.; Zacchigna, S.; et al. SARS-CoV-2, myocardial injury and inflammation: Insights from a large clinical and autopsy study. Clin. Res. Cardiol. 2021, 110, 1822–1831. [Google Scholar] [CrossRef]
- Halushka, M.K.; Vander Heide, R.S. Myocarditis is rare in COVID-19 autopsies: Cardiovascular findings across 277 post-mortem examinations. Cardiovasc. Pathol. 2020, 50, 107300. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; the Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef]
- Wei, J.-F.; Huang, F.-Y.; Xiong, T.-Y.; Liu, Q.; Chen, H.; Wang, H.; Huang, H.; Luo, Y.-C.; Zhou, X.; Liu, Z.-Y.; et al. Acute myocardial injury is common in patients with COVID-19 and impairs their prognosis. Heart 2020, 106, 1154–1159. [Google Scholar] [CrossRef] [PubMed]
- Bergami, M.; Manfrini, O.; Cenko, E.; Dorobantu, M.; Demiri, I.; Fronea, O.; Kedev, S.; Mjehovic, P.; Pasalic, M.; Poposka, L.; et al. Prognostic value of brain natriuretic peptide in COVID-19 with or without acute heart failure. Eur. Heart J. 2022, 43, ehac544.922. [Google Scholar] [CrossRef]
- Falsey, A.R.; Walsh, E.; Esser, M.T.; Shoemaker, K.; Yu, L.; Griffin, M.P. Respiratory syncytial virus–associated illness in adults with advanced chronic obstructive pulmonary disease and/or congestive heart failure. J. Med. Virol. 2019, 91, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Madjid, M.; Aboshady, I.; Awan, I.; Litovsky, S.; Casscells, S.W. Influenza and cardiovascular disease: Is there a causal relationship? Tex. Heart Inst. J. 2004, 31, 4–13. [Google Scholar]
- Panhwar, M.S.; Kalra, A.; Gupta, T.; Kolte, D.; Khera, S.; Bhatt, D.L.; Ginwalla, M. Effect of Influenza on Outcomes in Patients with Heart Failure. JACC Heart Fail. 2019, 7, 112–117. [Google Scholar] [CrossRef]
- Kytömaa, S.; Hegde, S.; Claggett, B.; Udell, J.A.; Rosamond, W.; Temte, J.; Nichol, K.; Wright, J.D.; Solomon, S.D.; Vardeny, O. Association of influenza-like illness activity with hospitalizations for heart failure: The atherosclerosis risk in communities study. JAMA Cardiol. 2019, 4, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.E.; Vaduganathan, M.; Khan, M.S.; Papadimitriou, L.; Long, R.C.; Hernandez, G.A.; Moore, C.K.; Lennep, B.W.; Mcmullan, M.R.; Butler, J. Reductions in Heart Failure Hospitalizations During the COVID-19 Pandemic. J. Card. Fail. 2020, 26, 462–463. [Google Scholar] [CrossRef]
- Bhatt, A.S.; Moscone, A.; McElrath, E.E.; Varshney, A.S.; Claggett, B.L.; Bhatt, D.L.; Januzzi, J.L.; Butler, J.; Adler, D.S.; Solomon, S.D.; et al. Declines in hospitalizations for acute cardiovascular conditions during the COVID-19 pandemic: A multicenter tertiary care experience. J. Am. Coll. Cardiol. 2020, 76, 280–288. [Google Scholar] [CrossRef]
- Woolf, S.H.; Chapman, D.A.; Sabo, R.T.; Weinberger, D.M.; Hill, L. Excess Deaths From COVID-19 and Other Causes, March-April 2020. JAMA 2020, 324, 510–513. [Google Scholar] [CrossRef]
- Giustino, G.; Croft, L.B.; Stefanini, G.G.; Bragato, R.; Silbiger, J.J.; Vicenzi, M.; Danilov, T.; Kukar, N.; Shaban, N.; Kini, A.; et al. Characterization of Myocardial Injury in Patients With COVID-19. J. Am. Coll. Cardiol. 2020, 76, 2043–2055. [Google Scholar] [CrossRef]
- Inciardi, R.M.; Adamo, M.; Lupi, L.; Cani, D.S.; Di Pasquale, M.; Tomasoni, D.; Italia, L.; Zaccone, G.; Tedino, C.; Fabbricatore, D.; et al. Characteristics and outcomes of patients hospitalized for COVID-19 and cardiac disease in Northern Italy. Eur. Heart J. 2020, 41, 1821–1829, Erratum in Eur. Heart J. 2020, 41, 4591. [Google Scholar] [CrossRef]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef]
- Tomasoni, D.; Inciardi, R.M.; Lombardi, C.M.; Tedino, C.; Agostoni, P.; Ameri, P.; Barbieri, L.; Bellasi, A.; Camporotondo, R.; Canale, C.; et al. Impact of heart failure on the clinical course and outcomes of patients hospitalized for COVID-19. Results of the Cardio-COVID-Italy multicentre study. Eur. J. Heart Fail. 2020, 22, 2238–2247. [Google Scholar] [CrossRef]
- Alvarez-Garcia, J.; Lee, S.; Gupta, A.; Cagliostro, M.; Joshi, A.A.; Rivas-Lasarte, M.; Contreras, J.; Mitter, S.S.; LaRocca, G.; Tlachi, P.; et al. Prognostic Impact of Prior Heart Failure in Patients Hospitalized With COVID-19. J. Am. Coll. Cardiol. 2020, 76, 2334–2348. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Coats, A.J.; Zheng, Z.; Adamo, M.; Ambrosio, G.; Anker, S.D.; Butler, J.; Xu, D.; Mao, J.; Khan, M.S.; et al. Management of heart failure patients withCOVID-19: A joint position paper of the Chinese Heart Failure Association & National Heart Failure Committee and the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 941–956. [Google Scholar] [CrossRef] [PubMed]
- Salah, H.M.; Fudim, M.; O’neil, S.T.; Manna, A.; Chute, C.G.; Caughey, M.C. Post-recovery COVID-19 and incident heart failure in the National COVID Cohort Collaborative (N3C) study. Nat. Commun. 2022, 13, 4117. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, A.S.; Jering, K.S.; Vaduganathan, M.; Claggett, B.L.; Cunningham, J.W.; Rosenthal, N.; Signorovitch, J.; Thune, J.J.; Vardeny, O.; Solomon, S.D. Clinical Outcomes in Patients with Heart Failure Hospitalized with COVID-19. JACC Heart Fail. 2021, 9, 65–73. [Google Scholar] [CrossRef]
- Sokolski, M.; Trenson, S.; Sokolska, J.M.; D’Amario, D.; Meyer, P.; Poku, N.K.; Biering-Sørensen, T.; Lassen, M.C.H.; Skaarup, K.G.; Barge-Caballero, E.; et al. Heart failure in COVID-19: The multicentre, multinational PCHF-COVICAV registry. ESC Heart Fail. 2021, 8, 4955–4967. [Google Scholar] [CrossRef]
- Greene, S.J.; Lautsch, D.; Yang, L.; Tan, X.; Brady, J.E. Prognostic Interplay Between COVID-19 and Heart Failure with Reduced Ejection Fraction. J. Card. Fail. 2022, 28, 1287–1297. [Google Scholar] [CrossRef]
- Kim, H.J.; Park, M.; Shin, J.I.; Park, J.; Kim, D.; Jeon, J.; Kim, J.; Song, T. Associations of heart failure with susceptibility and severe complications of COVID-19: A nationwide cohort study. J. Med. Virol. 2022, 94, 1138–1145. [Google Scholar] [CrossRef]
- Sisti, N.; Valente, S.; Mandoli, G.E.; Santoro, C.; Sciaccaluga, C.; Franchi, F.; Cameli, P.; Mondillo, S.; Cameli, M. COVID-19 in patients with heart failure: The new and the old epidemic. Heart 2021, 97, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Yonas, E.; Alwi, I.; Pranata, R.; Huang, I.; Lim, M.A.; Gutierrez, E.J.; Yamin, M.; Siswanto, B.B.; Virani, S.S. Effect of heart failure on the outcome of COVID-19—A meta analysis and systematic review. Am. J. Emerg. Med. 2021, 46, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Rey, J.R.; Caro-Codón, J.; Rosillo, S.O.; Iniesta, Á.M.; Castrejón-Castrejón, S.; Marco-Clement, I.; Martín-Polo, L.; Merino-Argos, C.; Rodríguez-Sotelo, L.; García-Veas, J.M.; et al. Heart failure in COVID-19 patients: Prevalence, incidence and prognostic implications. Eur. J. Heart Fail. 2020, 22, 2205–2215. [Google Scholar] [CrossRef] [PubMed]
- Zaccone, G.; Tomasoni, D.; Italia, L.; Lombardi, C.M.; Metra, M. Myocardial Involvement in COVID-19: An Interaction Between Comorbidities and Heart Failure with Preserved Ejection Fraction. A Further Indication of the Role of Inflammation. Curr. Heart Fail. Rep. 2021, 18, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Zuin, M.; Rigatelli, G.; Roncon, L.; Pasquetto, G.; Bilato, C. Risk of incident heart failure after COVID-19 recovery: A systematic review and meta-analysis. Heart Fail. Rev. 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Gryglewska-Wawrzak, K.; Sakowicz, A.; Banach, M.; Maciejewski, M.; Bielecka-Dabrowa, A. Factors of Persistent Limited Exercise Tolerance in Patients after COVID-19 with Normal Left Ventricular Ejection Fraction. Biomedicines 2022, 10, 3257. [Google Scholar] [CrossRef] [PubMed]
- Lassen, M.C.H.; Skaarup, K.G.; Lind, J.N.; Alhakak, A.S.; Sengeløv, M.; Nielsen, A.B.; Espersen, C.; Ravnkilde, K.; Hauser, R.; Schöps, L.B.; et al. Echocardiographic abnormalities and predictors of mortality in hospitalized COVID-19 patients: The ECHOVID-19 study. ESC Heart Fail. 2020, 7, 4189–4197. [Google Scholar] [CrossRef]
- Szekely, Y.; Lichter, Y.; Taieb, P.; Banai, A.; Hochstadt, A.; Merdler, I.; Oz, A.G.; Rothschild, E.; Baruch, G.; Peri, Y.; et al. Spectrum of Cardiac Manifestations in COVID-19: A Systematic Echocardiographic Study. Circulation 2020, 142, 342–353. [Google Scholar] [CrossRef]
- Tudoran, C.; Tudoran, M.; Cut, T.G.; Lazureanu, V.E.; Oancea, C.; Marinescu, A.R.; Pescariu, S.A.; Pop, G.N.; Bende, F. Evolution of Echocardiographic Abnormalities Identified in Previously Healthy Individuals Recovering from COVID-19. J. Pers. Med. 2022, 12, 46. [Google Scholar] [CrossRef]
- Tudoran, M.; Tudoran, C.; Lazureanu, V.E.; Marinescu, A.R.; Pop, G.N.; Pescariu, A.S.; Enache, A.; Cut, T.G. Alterations of Left Ventricular Function Persisting during Post-Acute COVID-19 in Subjects without Previously Diagnosed Cardiovascular Pathology. J. Pers. Med. 2021, 11, 225. [Google Scholar] [CrossRef]
- Harada, R.; Mantha, Y.; Hieda, M. Back to Basics: Key Physical Examinations and Theories in Patients with Heart Failure. Heart Fail. Clin. 2020, 16, 139–151. [Google Scholar] [CrossRef] [PubMed]
- Thibodeau, J.T.; Drazner, M.H. The Role of the Clinical Examination in Patients with Heart Failure. JACC Heart Fail. 2018, 6, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.-J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jimenez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur. Respir. J. 2019, 54, 1901647. [Google Scholar] [PubMed]
- Carrier, M.; Righini, M.; Djurabi, R.K.; Huisman, M.V.; Perrier, A.; Wells, P.S.; Rodger, M.; Wuillemin, W.A.; Le Gal, G. VIDAS D-dimer in combination with clinical pre-test probability to rule out pulmonary embolism. A systematic review of management outcome studies. Thromb. Haemost. 2009, 101, 886–892. [Google Scholar] [CrossRef] [PubMed]
- Righini, M.; Van Es, J.; Exter, P.D. Age-Adjusted D-Dimer Cutoff Levels to Rule Out Pulmonary Embolism: The ADJUST-PE Study. JAMA 2014, 311, 1117. [Google Scholar] [CrossRef] [PubMed]
- Varikasuvu, S.R.; Varshney, S.; Dutt, N.; Munikumar, M.; Asfahan, S.; Kulkarni, P.P.; Gupta, P. D-dimer, disease severity, and deaths (3D-study) in patients with COVID-19: A systematic review and meta-analysis of 100 studies. Sci. Rep. 2021, 11, 21888. [Google Scholar] [CrossRef]
- Gouda, P.; Brown, P.; Rowe, B.H.; McAlister, F.A.; Ezekowitz, J.A. Insights into the importance of the electrocardiogram in patients with acute heart failure. Eur. J. Heart Fail. 2016, 18, 1032–1040. [Google Scholar] [CrossRef] [PubMed]
- Pan, D.; Pellicori, P.; Dobbs, K.; Bulemfu, J.; Sokoreli, I.; Urbinati, A.; Brown, O.; Sze, S.; Rigby, A.S.; Kazmi, S.; et al. Prognostic value of the chest X-ray in patients hospitalised for heart failure. Clin. Res. Cardiol. 2021, 110, 1743–1756. [Google Scholar] [CrossRef]
- Galderisi, M.; Cosyns, B.; Edvardsen, T.; Cardim, N.; Delgado, V.; Di Salvo, G.; Donal, E.; Sade, L.E.; Ernande, L.; Garbi, M.; et al. Standardization of adult transthoracic echocardiography reporting in agreement with recent chamber quantification, diastolic function, and heart valve disease recommendations: An expert consensus document of the European association of cardiovascular imaging. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1301–1310. [Google Scholar] [CrossRef] [PubMed]
- Szyszka, A.; Płońska-Gościniak, E. Transesophageal echocardiography. J. Ultrason. 2019, 19, 62–65. [Google Scholar] [CrossRef]
- Roy, P.-M.; Colombet, I.; Durieux, P.; Chatellier, G.; Sors, H.; Meyer, G. Systematic review and meta-analysis of strategies for the diagnosis of suspected pulmonary embolism. BMJ 2005, 331, 259. [Google Scholar] [CrossRef] [PubMed]
- Kearon, C. Natural History of Venous Thromboembolism. Circulation 2003, 107, I22–I30. [Google Scholar] [CrossRef] [PubMed]
- Glaab, T.; Taube, C. Practical guide to cardiopulmonary exercise testing in adults. Respir. Res. 2022, 23, 9. [Google Scholar] [CrossRef]
- Durstenfeld, M.S.; Sun, K.; Tahir, P.; Peluso, M.J.; Deeks, S.G.; Aras, M.A.; Grandis, D.J.; Long, C.S.; Beatty, A.; Hsue, P.Y. Use of Cardiopulmonary Exercise Testing to Evaluate Long COVID-19 Symptoms in Adults: A Systematic Review and Meta-analysis. JAMA Netw. Open 2022, 5, e2236057. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Nikravesh, M.; Chukwuemeka, U.; Randazzo, M.; Flores, P.; Choday, P.; Raja, A.; Aseri, M.; Shivang, S.; Chaudhuri, S.; et al. Safety of ACEi and ARB in COVID-19 management: A retrospective analysis. Clin. Cardiol. 2022, 45, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Cannata, F.; Chiarito, M.; Reimers, B.; Azzolini, E.; Ferrante, G.; My, I.; Viggiani, G.; Panico, C.; Regazzoli, D.; Ciccarelli, M.; et al. Continuation versus discontinuation of ACE inhibitors or angiotensin II receptor blockers in COVID-19: Effects on blood pressure control and mortality. Eur. Heart J. 2020, 6, 412–414. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.D.; Macedo, A.V.S.; de Barros ESilva, P.G.M.; Moll-Bernardes, R.J.; dos Santos, T.M.; Mazza, L.; Feldman, A.; D’Andréa Saba Arruda, G.; de Albuquerque, D.C.; Camiletti, A.S.; et al. Effect of discontinuing vs continuing angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on days alive and out of the hospital in patients admitted with COVID-19: A randomized clinical trial. JAMA 2021, 325, 254–264. [Google Scholar] [CrossRef]
- Palazzuoli, A.; Mancone, M.; De Ferrari, G.M.; Forleo, G.; Secco, G.G.; Ruocco, G.M.; D’Ascenzo, F.; Monticone, S.; Paggi, A.; Vicenzi, M.; et al. Antecedent Administration of Angiotensin-Converting Enzyme Inhibitors or Angiotensin II Receptor Antagonists and Survival After Hospitalization for COVID-19 Syndrome. J. Am. Heart Assoc. 2020, 9, e017364. [Google Scholar] [CrossRef]
- Zhu, Z.; Zeng, Q.; Liu, Q.; Wen, J.; Chen, G. Association of Glucose-Lowering Drugs with Outcomes in Patients with Diabetes Before Hospitalization for COVID-19: A Systematic Review and Network Meta-analysis. JAMA Netw. Open 2022, 5, e2244652. [Google Scholar] [CrossRef]
- Pauschinger, M.; Rutschow, S.; Chandrasekharan, K.; Westermann, D.; Weitz, A.; Peter Schwimmbeck, L.; Zeichhardt, H.; Poller, W.; Noutsias, M.; Li, J.; et al. Carvedilol improves left ventricular function in murine coxsackievirus-induced acute myocarditis. Association with reduced myocardial interleukin-1beta and MMP-8 expression and a modulated immune response. Eur. J. Heart Fail. 2005, 7, 444–452. [Google Scholar] [CrossRef]
- Vicenzi, M.; Ruscica, M.; Iodice, S.; Rota, I.; Ratti, A.; Di Cosola, R.; Corsini, A.; Bollati, V.; Aliberti, S.; Blasi, F. The Efficacy of the Mineralcorticoid Receptor Antagonist Canrenone in COVID-19 Patients. J. Clin. Med. 2020, 9, 2943. [Google Scholar] [CrossRef]
- Kumar, N.; Zuo, Y.; Yalavarthi, S.; Hunker, K.L.; Knight, J.S.; Kanthi, Y.; Obi, A.T.; Ganesh, S.K. SARS-CoV-2 Spike Protein S1-Mediated Endothelial Injury and Pro-Inflammatory State Is Amplified by Dihydrotestosterone and Prevented by Mineralocorticoid Antagonism. Viruses 2021, 13, 2209. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Miyazaki, K.; Shah, P.; Kozai, L.; Kewcharoen, J. Association between Mineralocorticoid Receptor Antagonist and Mortality in SARS-CoV-2 Patients: A Systematic Review and Meta-Analysis. Healthcare 2022, 10, 645. [Google Scholar] [CrossRef] [PubMed]
- Spyropoulos, A.C.; Weitz, J.I. Hospitalized COVID-19 patients and venous thromboembolism: A perfect storm. Circulation 2020, 142, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal Coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Yan, X.; Fan, Q.; Liu, H.; Liu, X.; Liu, Z.; Zhang, Z. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19. J. Thromb. Haemost. 2020, 18, 1324–1329. [Google Scholar] [CrossRef] [PubMed]
- Giamarellos-Bourboulis, E.J.; Netea, M.G.; Rovina, N.; Akinosoglou, K.; Antoniadou, A.; Antonakos, N.; Damoraki, G.; Gkavogianni, T.; Adami, M.-E.; Katsaounou, P.; et al. Complex Immune Dysregulation in COVID-19 Patients with Severe Respiratory Failure. Cell Host Microbe 2020, 27, 992–1000.e3. [Google Scholar] [CrossRef]
- Lachant, D.J.; Lachant, N.A.; Kouides, P.; Rappaport, S.; Prasad, P.; White, R.J. Chronic therapeutic anticoagulation is associated with decreased thrombotic complications in SARS-CoV-2 infection. J. Thromb. Haemost. 2020, 18, 2640–2645. [Google Scholar] [CrossRef]
- Ramacciotti, E.; Agati, L.B.; Calderaro, D.; Aguiar, V.C.R.; Spyropoulos, A.C.; de Oliveira, C.C.C.; dos Santos, J.L.; Volpiani, G.G.; Sobreira, M.L.; Joviliano, E.E.; et al. Rivaroxaban versus no anticoagulation for post-discharge thromboprophylaxis after hospitalisation for COVID-19 (MICHELLE): An open-label, multicentre, randomised, controlled trial. Lancet 2022, 399, 50–59. [Google Scholar] [CrossRef]
- Won, T.; Wood, M.K.; Hughes, D.M.; Talor, M.V.; Ma, Z.; Schneider, J.; Skinner, J.T.; Asady, B.; Goerlich, E.; Halushka, M.K.; et al. Endothelial thrombomodulin downregulation caused by hypoxia contributes to severe infiltration and coagulopathy in COVID-19 patient lungs. Ebiomedicine 2022, 75, 103812. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Wichmann, D.; Sperhake, J.P.; Lütgehetmann, M.; Steurer, S.; Edler, C.; Heinemann, A.; Heinrich, F.; Mushumba, H.; Kniep, I.; Schröder, A.S.; et al. Autopsy Findings and Venous Thromboembolism in Patients with COVID-19: A Prospective Cohort Study. Ann. Intern. Med. 2020, 173, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Bansal, A.; Kumar, A.; Patel, D.; Puri, R.; Kalra, A.; Kapadia, S.R.; Reed, G.W. Meta-analysis Comparing Outcomes in Patients with and without Cardiac Injury and Coronavirus Disease 2019 (COVID-19). Am. J. Cardiol. 2021, 141, 140–146. [Google Scholar] [CrossRef]
- Jin, S.; Jin, Y.; Xu, B.; Hong, J.; Yang, X. Prevalence and Impact of Coagulation Dysfunction in COVID-19 in China: A Meta-Analysis. Thromb. Haemost. 2020, 120, 1524–1535. [Google Scholar] [CrossRef]
- Polimeni, A.; Leo, I.; Spaccarotella, C.; Mongiardo, A.; Sorrentino, S.; Sabatino, J.; De Rosa, S.; Indolfi, C. Differences in coagulopathy indices in patients with severe versus non-severe COVID-19: A meta-analysis of 35 studies and 6427 patients. Sci. Rep. 2021, 11, 10464. [Google Scholar] [CrossRef]
- Zhu, J.; Pang, J.; Ji, P.; Zhong, Z.; Li, H.; Li, B.; Zhang, J.; Lu, J. Coagulation dysfunction is associated with severity of COVID-19: A meta-analysis. J. Med. Virol. 2021, 93, 962–972. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Leng, Y.; Zhang, Y.; Wu, K.; Ji, Y.; Lei, S.; Xia, Z. Meta-analysis of coagulation parameters associated with disease severity and poor prognosis of COVID-19. Int. J. Infect. Dis. 2020, 100, 441–448. [Google Scholar] [CrossRef]
- Zhang, X.; Yang, X.; Jiao, H.; Liu, X. Coagulopathy in patients with COVID-19: A systematic review and meta-analysis. Aging 2020, 12, 24535–24551. [Google Scholar] [CrossRef]
- Agarwal, G.; Hajra, A.; Chakraborty, S.; Patel, N.; Biswas, S.; Adler, M.K.; Lavie, C.J. Predictors and mortality risk of venous thromboembolism in patients with COVID-19: Systematic review and meta-analysis of observational studies. Ther. Adv. Cardiovasc. Dis. 2022, 16, 17539447221105013. [Google Scholar] [CrossRef]
- Alharbi, M.G.; Alanazi, N.; Yousef, A.; Alanazi, N.; Alotaibi, B.; Aljurf, M.; El Fakih, R. COVID-19 associated with immune thrombocytopenia: A systematic review and meta-analysis. Expert Rev. Hematol. 2022, 15, 157–166. [Google Scholar] [CrossRef]
- Cui, S.; Chen, S.; Li, X.; Liu, S.; Wang, F. Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 1421–1424. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Gandet, F.F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Roncon, L.; Zuin, M.; Barco, S.; Valerio, L.; Zuliani, G.; Zonzin, P.; Konstantinides, S.V. Incidence of acute pulmonary embolism in COVID-19 patients: Systematic review and meta-analysis. Eur. J. Intern. Med. 2020, 82, 29–37. [Google Scholar] [CrossRef]
- Ng, J.J.; Liang, Z.C.; Choong, A.M.T.L. The incidence of pulmonary thromboembolism in COVID-19 patients admitted to the intensive care unit: A meta-analysis and meta-regression of observational studies. J. Intensiv. Care 2021, 9, 20. [Google Scholar] [CrossRef] [PubMed]
- Gong, X.; Yuan, B.; Yuan, Y. Incidence and prognostic value of pulmonary embolism in COVID-19: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0263580. [Google Scholar] [CrossRef] [PubMed]
- Whyte, M.B.; Barker, R.; Kelly, P.A.; Gonzalez, E.; Czuprynska, J.; Patel, R.K.; Rea, C.; Perrin, F.; Waller, M.; Jolley, C.; et al. Three-month follow-up of pulmonary embolism in patients with COVID-19. Thromb. Res. 2021, 201, 113–115. [Google Scholar] [CrossRef]
- Ritchie, C.A.; Johnson, M.M.; Stowell, J.T.; Idrees, H.; Toskich, B.; Paz-Fumagalli, R.; Montazeri, S.; Fortich, S.; Franco-Mesa, C.; Gloviczki, P.; et al. Resolution of acute pulmonary embolism using anticoagulation therapy alone in coronavirus disease 2019. J. Vasc. Surg. Venous Lymphat. Disord. 2022, 10, 578–584.e2. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study (Year) | Number of Patients | Design | Findings | |
|---|---|---|---|---|
| [41] | Inciardi R.M. et al. (2020) | 99 | Single-centre | Out of 99 patients, 53 had cardiac disease, and 40% of them had a history of heart failure. Patients with cardiac disease had a higher mortality rate compared to those without cardiac disease (36% vs. 15%). Furthermore, patients with cardiac disease had a higher prevalence of thromboembolic incidents and septic shock compared to those without cardiac disease (23% vs. 6% and 11% vs. 0%, respectively). |
| [42] | Chen T et al. (2020) | 274 | Retrospective case series | Patients who died from COVID-19 had higher levels of troponin I, NT-proBNP, and D-dimer than those who recovered. Additionally, parameters such as alanine aminotransferase, aspartate aminotransferase, creatinine, creatine kinase, and lactate dehydrogenase were higher in deceased patients. Patients who died from COVID-19 were more likely to develop complications such as heart failure (41/83; 49%) or acute cardiac injury (72/94; 77%), and had a higher incidence of acute respiratory distress syndrome (113; 100%), type I respiratory failure (18/35; 51%), sepsis (113; 100%), alkalosis (14/35; 40%), hyperkalemia (42; 37%), acute kidney injury (28; 25%) and hypoxic encephalopathy (23; 20%). Cardiovascular complications were more common in patients with cardiovascular comorbidity. Acute cardiac injury and heart failure were more common in patients who died of COVID-19. These were independent of a history of cardiovascular disease. |
| [43] | Tomasoni D. et al. (2020) | 692 | Prospective multicentre cohort study | Patients diagnosed with heart failure were more likely to have complications such as acute heart failure (33.3% vs. 5.1%), acute renal failure (28.1% vs. 12.9%), multiorgan failure (15.9% vs. 5.8%) or sepsis (18.4% vs. 8.9%). A history of heart failure indicates a higher risk of death from COVID-19 infection (41% vs. 21%). |
| [44] | Alvarez-Garcia J. et al. (2020) | 6439 | Retrospective analysis | Patients with diagnosed heart failure were more likely to require mechanical ventilation (22.8% vs. 11.9%) and had a higher mortality rate (40.0% vs. 24.9%). Patients with previous heart failure had comparable results, regardless of the ejection fraction of left ventricle or the use of renin–angiotensin–aldosterone inhibitor. |
| [46] | Salah H.M. et al. (2022) | 257,075 | Cohort study, multicentre | Hospitalization for COVID-19 was related to increased risk of heart failure by 45%. Heart failure occurred more often in patients under 65 years of age, white, or who had been diagnosed with cardiovascular disease. |
| [47] | Bhatt A.S. et al. (2021) | 132,312 | Cohort study | Patients who were previously diagnosed with heart failure and were hospitalized due to COVID-19 had a significantly higher mortality rate (24.2%) compared to those who were hospitalized for acute heart failure (2.6%). Additionally, male gender, advanced age, morbid obesity, and diabetes were identified as risk factors associated with poorer outcomes and higher mortality during hospitalization. |
| [48] | Sokolski M. et al. (2021) | 1282 | Cohort study, multicentre, retrospective | Patients with a history of heart failure had a mortality rate of 36%, which was higher than the mortality rate of patients without a history of heart failure (23%). During hospitalization, 15% of patients experienced an acute heart failure incident, and 40% of these incidents were new cases. Patients who experienced acute heart failure during hospitalization had a higher mortality rate of 48% compared to non-heart failure patients (23%). |
| [49] | Greene S.J. et al. (2022) | 99,052 | Retrospective, cohort study | Patients with worsening heart failure with reduced ejection fraction (HFrEF) and those without HFrEF exacerbation had a higher 30-day mortality compared to patients without concomitant heart failure. Among patients diagnosed with HFrEF who tested positive for COVID-19, there was a higher risk of death within 30 days and an increased likelihood that their heart failure worsened. Additionally, patients who presented to healthcare facilities as outpatients had a higher mortality rate. |
| [50] | Kim H.J. et al. (2022) | 212,678 | Retrospective, cohort study | COVID-19 infection increases the risk of developing new-onset heart failure and exacerbating pre-existing heart failure. Patients with a history of heart failure had a poorer prognosis, a higher mortality rate (17.71% vs. 9.28%), and greater risk of developing severe complications compared to patients without heart failure. However, mechanical ventilation or admission to the intensive care unit was not required more often in patients with a history of HF. In contrast, COVID-19 infection was not found to be more frequent in patients with heart failure. |
| [52] | Yonas E. et al. (2021) | 21,640 | Analysis | Patients who have been diagnosed with heart failure and develop COVID-19 are more likely to require hospitalisation (odds ratio [OR] 2.37), experience poor outcomes (OR 2.86), and have an increased risk of death (OR 3.46). |
| [53] | Rey J.R. et al. (2020) | 3080 | Prospective cohort study | Patients diagnosed with chronic heart failure (CHF) have a higher frequency of acute heart failure (AHF) episodes (11.2%) than patients without CHF (2.1%), and N-terminal pro brain natriuretic peptide levels are elevated. Additionally, CHF is associated with higher mortality rates (48.7%) than non-HF patients (19%). Arrhythmias during hospital admission and CHF were found to be the main factors contributing to the development of AHF. Patients who develop AHF have a higher mortality rate (46.8% vs. 19.7%). Discontinuation of guideline-directed medical therapy, including beta-blockers, mineralocorticoid receptor antagonists, and angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, was also associated with increased mortality rates. |
| [54] | Zaccone G. et al. (2021) | Analysis | In patients hospitalised for COVID-19 infection, the incidence of HF comorbidity is (4–16%), this may be due to a shared cardiometabolic risk profile and comorbidities such as hypertension, diabetes, obesity and chronic kidney disease, which increase the risk of severe course of COVID-19 and are also risk factors of HFpEF. COVID-19 infection can induce acute decompensation of HF in patients with pre-existing HFpEF and in those with subclinical diastolic dysfunction. In the acute and subacute phases of COVID-19, impaired diastole (rather than systole), pulmonary hypertension, and right ventricular dysfunction can be observed. In 78% of patients in the chronic phase of COVID-19, inflammation and myocardial fibrosis are observed. | |
| [55] | Zuin M. et al. (2022) | 1,628,424 | Retrospective | Cardiovascular disease and structural heart changes are more common in patients after recovery from COVID-19. Additionally, patients who underwent COVID-19 were more likely to experience an episode of HF. The overall incidence of HF after COVID-19 infection was 0.4–2%. After 9.2 months, the frequency was 1.8–2.04. Moreover, an increased risk of HF was caused by older age and hypertension. |
| [56] | Gryglewska-Wawrzak K. et al. (2022) | 120 | Single-centre | The group of study participants with %VO2pred < 80% had a significantly higher proportion of men and a higher total body water (TBW%) compared to the control group (53% vs. 29% and 52.67% (±6.41) vs. 49.89% (±4.59), respectively). Individuals who presented with limited exercise capacity after COVID-19 infection demonstrated lower tricuspid annular plane systolic excursion (TAPSE), global peak systolic strain (GLPS), and late diastolic filling (A) velocity [21.86 mm (±4.53) vs. 24.08 mm (±3.20); 19.34% (±1.72) vs. 20.10% (±1.35)%; a median of 59.5 cm/s vs. 70.5 cm/s) compared to the control group. |
| Study (Year) | Number of Patients | Design | Findings | |
|---|---|---|---|---|
| [93] | Bansal A. et al. (2020) | 3175 | Meta-analysis | Cardiac injury in patients with a COVID-19 was associated with higher risk of mortality (risk ratio [RR]:7.79; 95% confidence interval [CI]: 4.69–13.01; I2 = 58%), admission to the intensive care unit (ICU) (RR: 4.06; 95% CI: 1.50–10.97; I2 = 61%), mechanical ventilation (RR: 5.53; 95% CI: 3.09–9.91; I2 = 0%), and developing coagulopathy (RR: 3.86; 95% CI: 2.81–5.32; I2 = 0%). |
| [94] | Jin S. et al. (2020) | 4889 | Meta-analysis | Severe patients had significantly higher D-dimer levels and prolonged prothrombin time (PT) compared with non-severe patients. Non-survivors had significantly higher D-dimer levels, prolonged PT, and decreased platelet count (PLT) compared to survivors. In total, 6.2% (95% CI: 2.6–9.9%) of COVID-19 patients were complicated by disseminated intravascular coagulation (DIC), in which the log risk ratio in non-survivors was 3.267 (95% CI: 2.191–4.342, Z ¼ 5.95, p < 0.05) compared with that in survivors. |
| [95] | Polimeni A. et al. (2021) | 6439 | Meta-analysis | D-dimer was significantly lower in COVID-19 patients with non-severe disease than in those with severe (standardized mean difference [SMD] −2.15 [−2.73–−1.56], I2 98%, p < 0.0001). D-dimer in survivors was lower compared to non-survivors (SMD −2.91 [−3.87–−1.96], I2 98%, p < 0.0001). Platelet count showed higher levels of mean PLT in non-severe patients than those observed in the severe group (SMD 0.77 [0.32–1.22], I2 96%, p < 0.001). |
| [96] | Zhu J. et al. (2021) | 6492 | Meta-analysis | Patients with severe disease showed a significantly lower platelet count (weighted mean difference [WMD]: −16.29 × 109/L; 95% CI: −25.34–7.23) and shorter activated partial thromboplastin time (WMD: 0.81 s; 95% CI: −1.94–0.33) but higher D dimer levels (WMD: 0.44 μg/mL; 95% CI: 0.29-0.58), higher fibrinogen levels (WMD: 0.51 g/L; 95% CI: 0.33–0.69) and longer prothrombin time (PT; WMD: 0.65 s; 95% CI: 0.44–0.86). The patients who died showed significantly higher D dimer levels (WMD: 6.58 μg/mL; 95% CI: 3.59–9.57), longer PT (WMD: 1.27 s; 95% CI: 0.49–2.06) and lower platelet count (WMD: −39.73 × 109/L; 95% CI: 61.99–−17.45) than patients who survived. |
| [97] | Zhang A. et al. (2020) | 2277 | Meta-analysis | The level in severe cases was lower than in mild cases, while the levels of PT, D-Dimer and fibrinogen were higher than those in mild cases (p < 0.05). The PT of the ICU patients was significantly longer (p < 0.05) than that of the non-ICU patients. PT and D-dimer were higher in non-survivors, PLT was lower than that of survivors (p < 0.05). |
| [98] | Zhang X. et al. (2020) | 3952 | Meta-analysis | Patients with severe symptoms exhibited higher levels of D-dimer, PT and fibrinogen than patients with less severe symptoms (SMD 0.83, 95% CI 0.70–0.97, I2 56.9%; SMD 0.39, 95% CI: 0.14–0.64, I2 79.4%; and SMD 0.35, 95% CI 0.17–0.53, I2 42.4%, respectively). |
| [99] | Agarwal G. et al. (2022) | 6053 | Meta-analysis | Patients with COVID-19 with venous thromboembolic events (VTE) had higher leukocyte counts and higher levels of D-dimer, C-reactive protein, and procalcitonin. |
| [100] | Alharbi M.G. et al. (2022) | 55 | Meta-analysis | Immune thrombocytopenia (ITP) secondary to COVID-19 infection was slightly more common among males (54.8%) than females. |
| [103] | Roncon et al. (2020) | 7178 | Meta-analysis | Among patients with COVID-19 hospitalized in general wards and ICU, the pooled in-hospital incidence of pulmonary embolism (PE) (or lung thrombosis) was 14.7% of cases (95% CI: 9.9–21.3%, I2 = 95.0%, p < 0.0001) and 23.4% (95% CI:16.7–31.8%, I2 = 88.7%, p < 0.0001), respectively. Segmental/sub-segmental pulmonary arteries were more frequently involved compared to main/lobar arteries (6.8% vs. 18.8%, p < 0.001). |
| [104] | Ng J. J. et al. (2020) | 1182 | Meta-analysis | The weighted average incidence of PE in COVID-19 patients admitted to the ICU was 11.1% (95% CI 7.7% to 15.7%, I2 = 78%, Cochran’s Q test p < 0.01). |
| [105] | Gong X et al. (2022) | 10,367 | Meta-analysis | The cumulative incidence of PE in patients with COVID-19 was 21% (95% confidence interval [95% CI]: 18–24%; p < 0.001), and the incidence of pulmonary embolism in ICU and non-ICU patients was 26% (95% CI: 22–31%; p < 0.001) and 17% (95% CI: 14–20%; p < 0.001), respectively. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gryglewska-Wawrzak, K.; Cienkowski, K.; Cienkowska, A.; Banach, M.; Bielecka-Dabrowa, A. The Role of Multidisciplinary Approaches in the Treatment of Patients with Heart Failure and Coagulopathy of COVID-19. J. Cardiovasc. Dev. Dis. 2023, 10, 245. https://doi.org/10.3390/jcdd10060245
Gryglewska-Wawrzak K, Cienkowski K, Cienkowska A, Banach M, Bielecka-Dabrowa A. The Role of Multidisciplinary Approaches in the Treatment of Patients with Heart Failure and Coagulopathy of COVID-19. Journal of Cardiovascular Development and Disease. 2023; 10(6):245. https://doi.org/10.3390/jcdd10060245
Chicago/Turabian StyleGryglewska-Wawrzak, Katarzyna, Krzysztof Cienkowski, Alicja Cienkowska, Maciej Banach, and Agata Bielecka-Dabrowa. 2023. "The Role of Multidisciplinary Approaches in the Treatment of Patients with Heart Failure and Coagulopathy of COVID-19" Journal of Cardiovascular Development and Disease 10, no. 6: 245. https://doi.org/10.3390/jcdd10060245
APA StyleGryglewska-Wawrzak, K., Cienkowski, K., Cienkowska, A., Banach, M., & Bielecka-Dabrowa, A. (2023). The Role of Multidisciplinary Approaches in the Treatment of Patients with Heart Failure and Coagulopathy of COVID-19. Journal of Cardiovascular Development and Disease, 10(6), 245. https://doi.org/10.3390/jcdd10060245