
Improvement of Quantification of Myocardial Synthetic ECV with Second-Generation Deep Learning Reconstruction

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cardiac CT Imaging Protocol
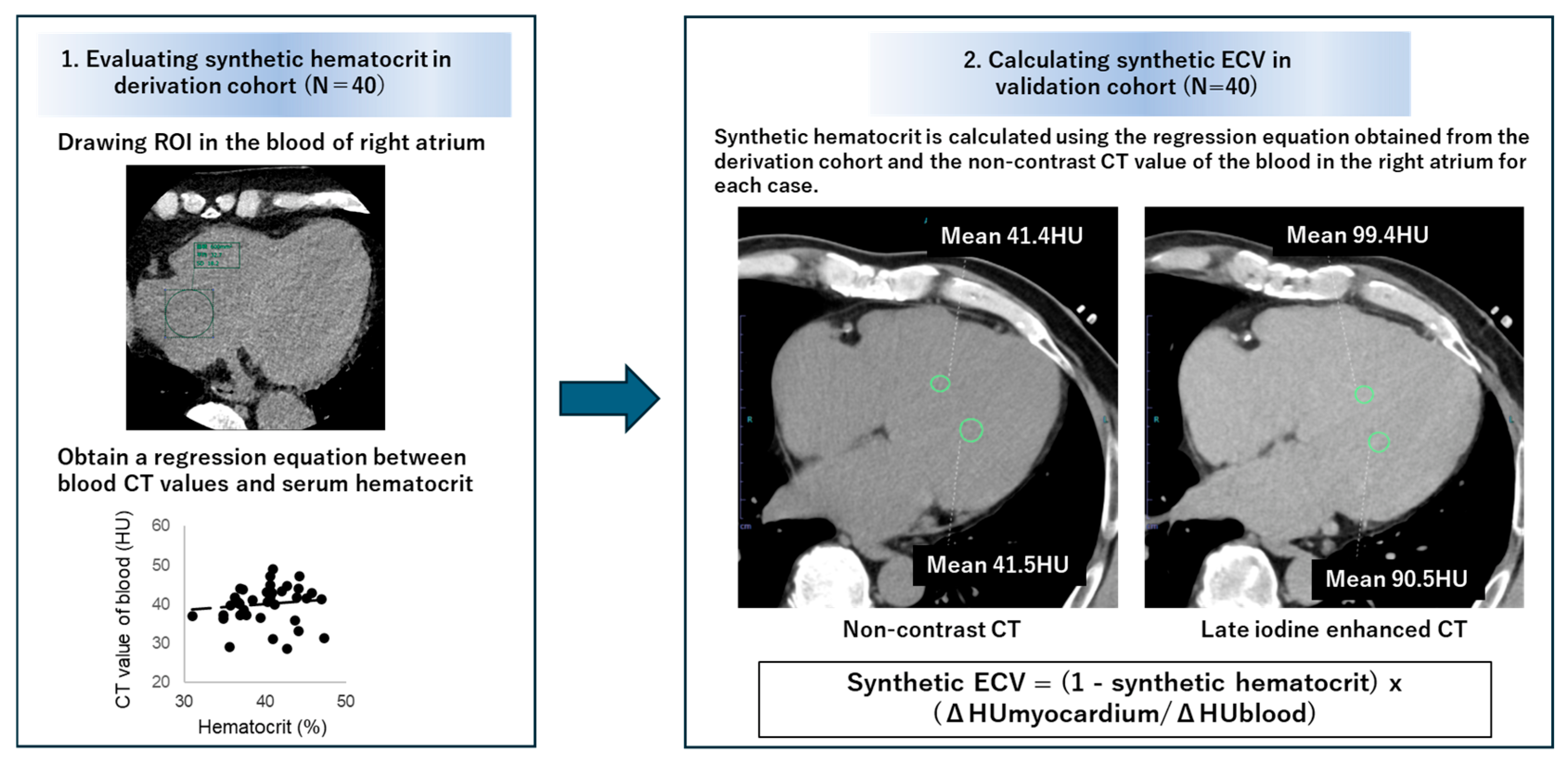
2.2. Calculation of Synthetic Hematocrit
2.3. Calculation of Synthetic ECV
2.4. Statistical Analysis
3. Result
3.1. Patients’ Characteristics
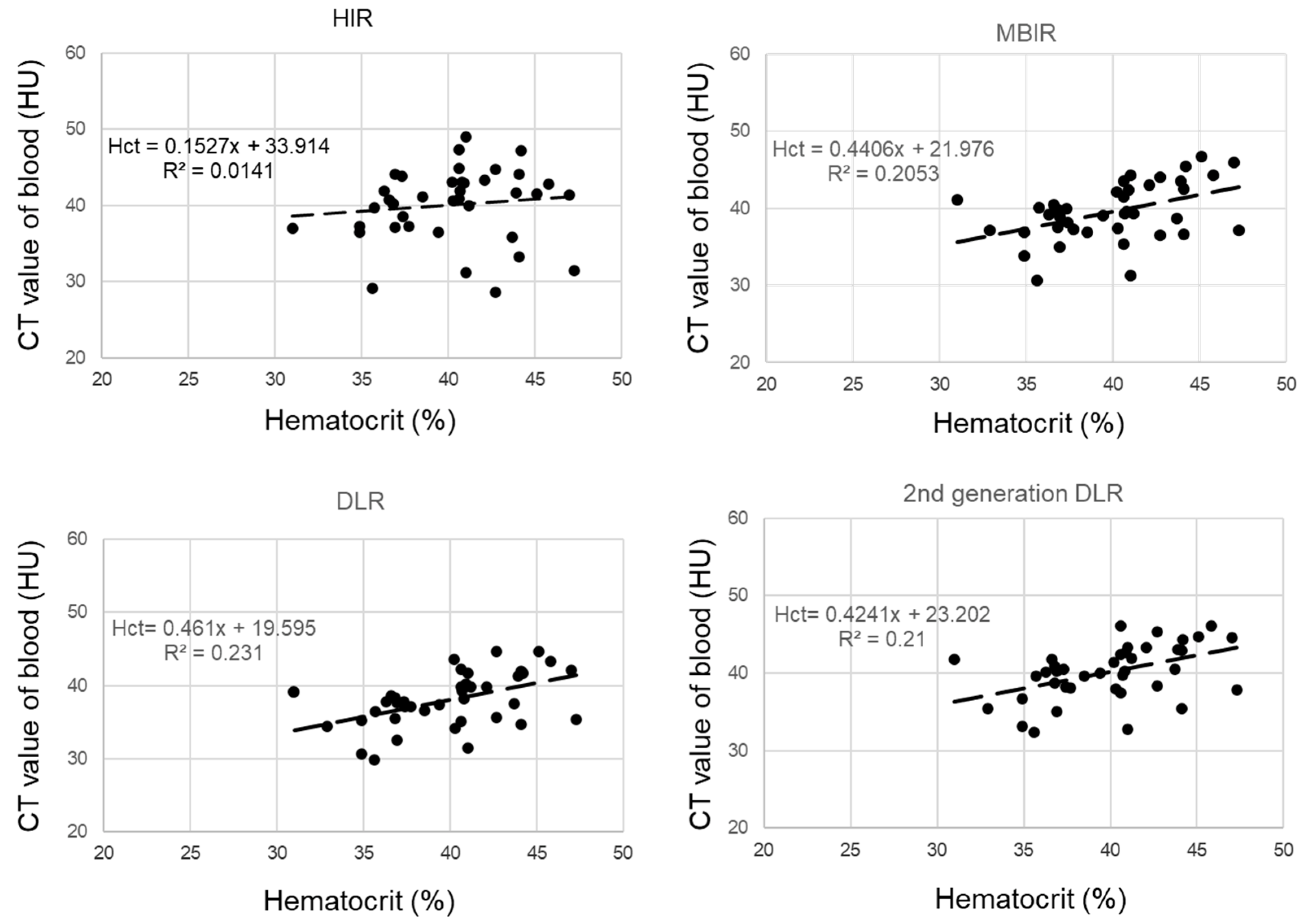
3.2. Creation of the Regression Equations for Synthetic Hematocrit Calculation in the Derivation Cohort
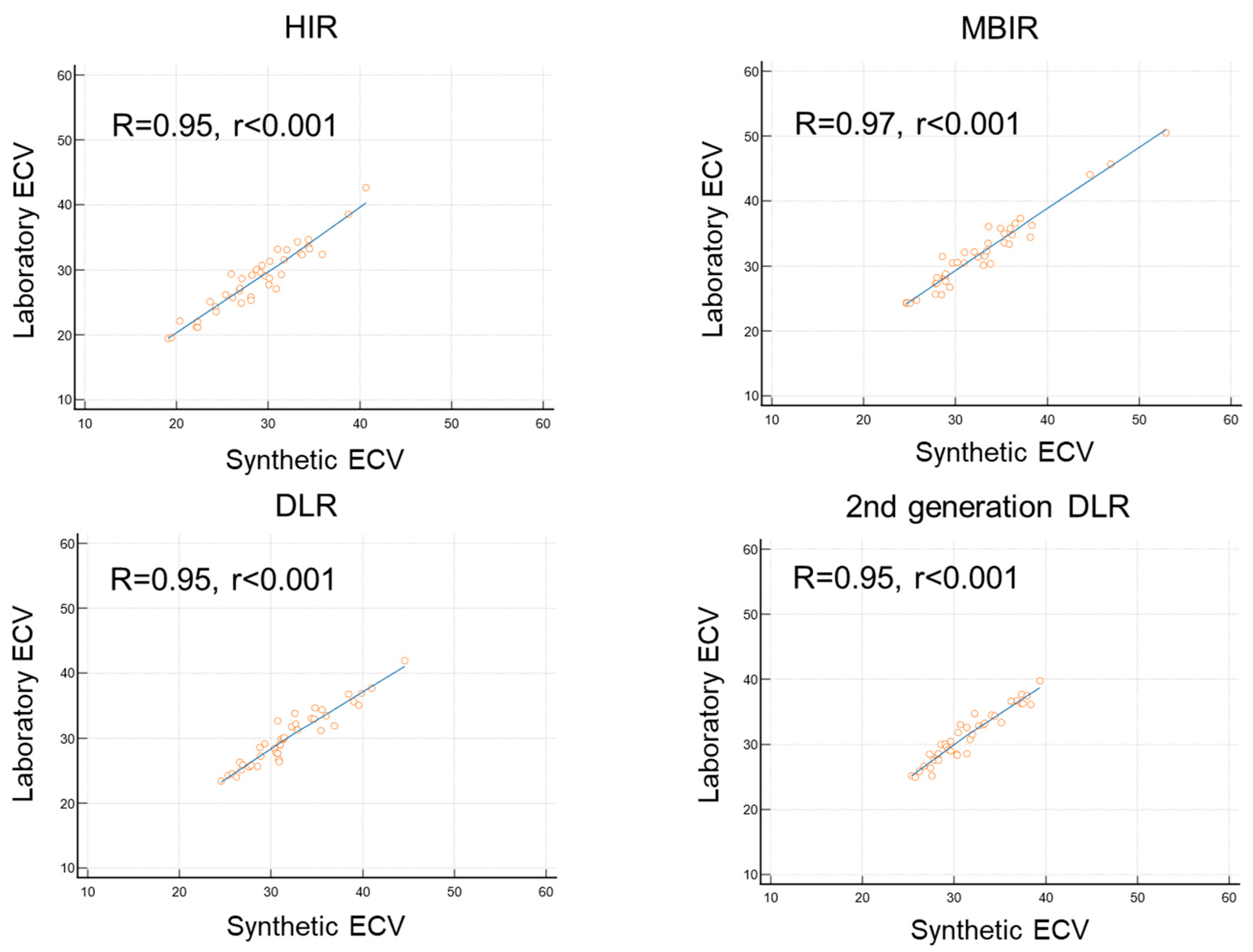
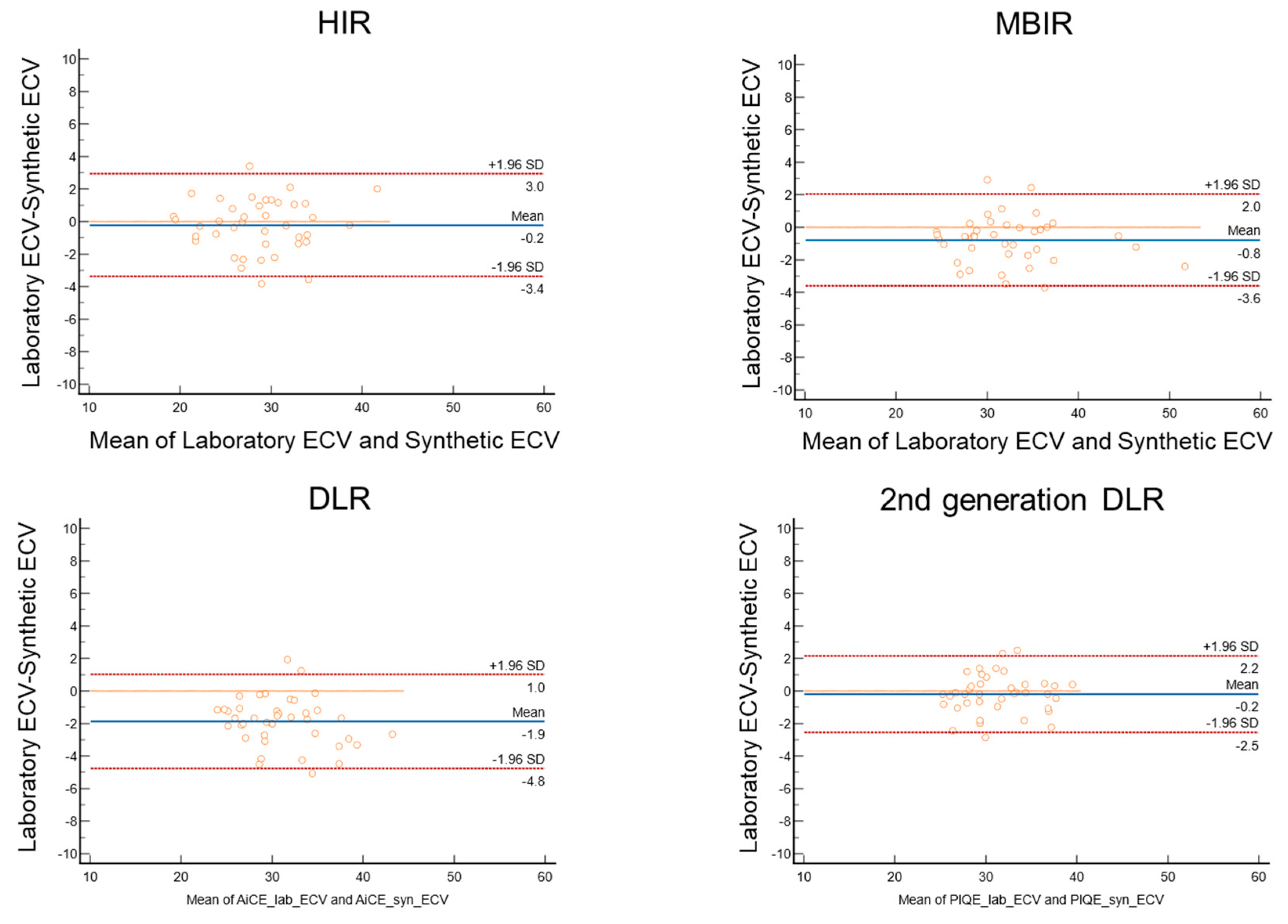
3.3. Comparison of Synthetic ECV and Laboratory ECV across Four Reconstruction Methods in the Validation Cohort
4. Discussion
5. Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mewton, N.; Liu, C.Y.; Croisille, P.; Bluemke, D.; Lima, J.A. Assessment of myocardial fibrosis with cardiovascular magnetic resonance. J. Am. Coll. Cardiol. 2011, 57, 891–903. [Google Scholar] [CrossRef] [PubMed]
- Haaf, P.; Garg, P.; Messroghli, D.R.; Broadbent, D.A.; Greenwood, J.P.; Plein, S. Cardiac T1 Mapping and Extracellular Volume (ECV) in clinical practice: A comprehensive review. J. Cardiovasc. Magn. Reson. 2016, 18, 89. [Google Scholar] [CrossRef]
- Flett, A.S.; Hayward, M.P.; Ashworth, M.T.; Hansen, M.S.; Taylor, A.M.; Elliott, P.M.; McGregor, C.; Moon, J.C. Equilibrium contrast cardiovascular magnetic resonance for the measurement of diffuse myocardial fibrosis: Preliminary validation in humans. Circulation 2010, 122, 138–144. [Google Scholar] [CrossRef]
- Arbelo, E.; Protonotarios, A.; Gimeno, J.R.; Arbustini, E.; Barriales-Villa, R.; Basso, C.; Bezzina, C.R.; Biagini, E.; Blom, N.A.; de Boer, R.A.; et al. 2023 ESC Guidelines for the management of cardiomyopathies. Eur. Heart J. 2023, 44, 3503–3626. [Google Scholar] [CrossRef]
- Kato, S.; Misumi, Y.; Horita, N.; Yamamoto, K.; Utsunomiya, D. Clinical Utility of Computed Tomography-Derived Myocardial Extracellular Volume Fraction: A Systematic Review and Meta-Analysis. JACC Cardiovasc. Imaging 2024, 17, 516–528. [Google Scholar] [CrossRef]
- Scully, P.R.; Patel, K.P.; Saberwal, B.; Klotz, E.; Augusto, J.B.; Thornton, G.D.; Hughes, R.K.; Manisty, C.; Lloyd, G.; Newton, J.D.; et al. Identifying Cardiac Amyloid in Aortic Stenosis: ECV Quantification by CT in TAVR Patients. JACC Cardiovasc. Imaging 2020, 13, 2177–2189. [Google Scholar] [CrossRef]
- Treibel, T.A.; Fontana, M.; Steeden, J.A.; Nasis, A.; Yeung, J.; White, S.K.; Sivarajan, S.; Punwani, S.; Pugliese, F.; Taylor, S.A.; et al. Automatic quantification of the myocardial extracellular volume by cardiac computed tomography: Synthetic ECV by CCT. J. Cardiovasc. Comput. Tomogr. 2017, 11, 221–226. [Google Scholar] [CrossRef]
- Kim, N.Y.; Im, D.J.; Youn, J.C.; Hong, Y.J.; Choi, B.W.; Kang, S.M.; Lee, H.J. Synthetic Extracellular Volume Fraction Derived Using Virtual Unenhanced Attenuation of Blood on Contrast-Enhanced Cardiac Dual-Energy CT in Nonischemic Cardiomyopathy. AJR Am. J. Roentgenol. 2022, 218, 454–461. [Google Scholar] [CrossRef]
- Greffier, J.; Pastor, M.; Si-Mohamed, S.; Goutain-Majorel, C.; Peudon-Balas, A.; Bensalah, M.Z.; Frandon, J.; Beregi, J.P.; Dabli, D. Comparison of two deep-learning image reconstruction algorithms on cardiac CT images: A phantom study. Diagn. Interv. Imaging 2024, 105, 110–117. [Google Scholar] [CrossRef]
- Kawai, H.; Motoyama, S.; Sarai, M.; Sato, Y.; Matsuyama, T.; Matsumoto, R.; Takahashi, H.; Katagata, A.; Kataoka, Y.; Ida, Y.; et al. Coronary computed tomography angiographic detection of in-stent restenosis via deep learning reconstruction: A feasibility study. Eur. Radiol. 2024, 34, 2647–2657. [Google Scholar] [CrossRef]
- Sawamura, S.; Kato, S.; Funama, Y.; Oda, S.; Mochizuki, H.; Inagaki, S.; Takeuchi, Y.; Morioka, T.; Izumi, T.; Ota, Y.; et al. Evaluation of four computed tomography reconstruction algorithms using a coronary artery phantom. Quant. Imaging Med. Surg. 2024, 14, 2870–2883. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.C.; Piehler, K.; Meier, C.G.; Testa, S.M.; Klock, A.M.; Aneizi, A.A.; Shakesprere, J.; Kellman, P.; Shroff, S.G.; Schwartzman, D.S.; et al. Association between extracellular matrix expansion quantified by cardiovascular magnetic resonance and short-term mortality. Circulation 2012, 126, 1206–1216. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Guo, H.; Liu, G.; Wu, C.; Ma, Y.; Li, S.; Zheng, Y.; Zhang, J. CT for the evaluation of myocardial extracellular volume with MRI as reference: A systematic review and meta-analysis. Eur. Radiol. 2023, 33, 8464–8476. [Google Scholar] [CrossRef]
- Muthalaly, R.G.; Tan, S.; Nelson, A.J.; Abrahams, T.; Han, D.; Tamarappoo, B.K.; Dey, D.; Nicholls, S.J.; Lin, A.; Nerlekar, N. Variation of computed tomography-derived extracellular volume fraction and the impact of protocol parameters: A systematic review and meta-analysis. J. Cardiovasc. Comput. Tomogr. 2024, 18, 457–464. [Google Scholar] [CrossRef]
- Mergen, V.; Ehrbar, N.; Moser, L.J.; Harmes, J.C.; Manka, R.; Alkadhi, H.; Eberhard, M. Synthetic hematocrit from virtual non-contrast images for myocardial extracellular volume evaluation with photon-counting detector CT. Eur. Radiol. 2024. [Google Scholar] [CrossRef]
- Takagi, H.; Tanaka, R.; Nagata, K.; Ninomiya, R.; Arakita, K.; Schuijf, J.D.; Yoshioka, K. Diagnostic performance of coronary CT angiography with ultra-high-resolution CT: Comparison with invasive coronary angiography. Eur. J. Radiol. 2018, 101, 30–37. [Google Scholar] [CrossRef]
- Motoyama, S.; Ito, H.; Sarai, M.; Nagahara, Y.; Miyajima, K.; Matsumoto, R.; Doi, Y.; Kataoka, Y.; Takahashi, H.; Ozaki, Y.; et al. Ultra-High-Resolution Computed Tomography Angiography for Assessment of Coronary Artery Stenosis. Circ. J. 2018, 82, 1844–1851. [Google Scholar] [CrossRef]
- Iwasawa, T.; Sato, M.; Yamaya, T.; Sato, Y.; Uchida, Y.; Kitamura, H.; Hagiwara, E.; Komatsu, S.; Utsunomiya, D.; Ogura, T. Ultra-high-resolution computed tomography can demonstrate alveolar collapse in novel coronavirus (COVID-19) pneumonia. Jpn. J. Radiol. 2020, 38, 394–398. [Google Scholar] [CrossRef]
- Orii, M.; Sone, M.; Osaki, T.; Ueyama, Y.; Chiba, T.; Sasaki, T.; Yoshioka, K. Super-resolution deep learning reconstruction at coronary computed tomography angiography to evaluate the coronary arteries and in-stent lumen: An initial experience. BMC Med. Imaging 2023, 23, 171. [Google Scholar] [CrossRef]
- Censi, S.; Cimaglia, P.; Barbieri, A.; Naldi, M.; Ruggerini, S.; Brogneri, S.; Tonet, E.; Rapezzi, C.; Squeri, A. Performance of Synthetic Extracellular Volume Fraction in Different Cardiac Phenotypes From a Prospective Cohort of Patients Referred for Cardiac Magnetic Resonance. J. Magn. Reson. Imaging 2021, 54, 429–439. [Google Scholar] [CrossRef]
- Kammerlander, A.A.; Duca, F.; Binder, C.; Aschauer, S.; Zotter-Tufaro, C.; Koschutnik, M.; Marzluf, B.A.; Bonderman, D.; Mascherbauer, J. Extracellular volume quantification by cardiac magnetic resonance imaging without hematocrit sampling: Ready for prime time? Wien. Klin. Wochenschr. 2018, 130, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Raucci, F.J.; Parra, D.A.; Christensen, J.T.; Hernandez, L.E.; Markham, L.W.; Xu, M.; Slaughter, J.C.; Soslow, J.H. Synthetic hematocrit derived from the longitudinal relaxation of blood can lead to clinically significant errors in measurement of extracellular volume fraction in pediatric and young adult patients. J. Cardiovasc. Magn. Reson. 2017, 19, 58. [Google Scholar] [CrossRef] [PubMed]
- Robison, S.; Karur, G.R.; Wald, R.M.; Thavendiranathan, P.; Crean, A.M.; Hanneman, K. Noninvasive hematocrit assessment for cardiovascular magnetic resonance extracellular volume quantification using a point-of-care device and synthetic derivation. J. Cardiovasc. Magn. Reson. 2018, 20, 19. [Google Scholar] [CrossRef]
- Thongsongsang, R.; Songsangjinda, T.; Tanapibunpon, P.; Krittayaphong, R. Native T1 mapping and extracellular volume fraction for differentiation of myocardial diseases from normal CMR controls in routine clinical practice. BMC Cardiovasc. Disord. 2021, 21, 270. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Derivation Cohort (n = 40) | Validation Cohort (n = 40) | |
|---|---|---|
| Male | 60% (24/40) | 63% (25/40) |
| Age, years | 71 ± 12 | 67 ± 11 |
| Interval between CT scan and blood test, days | 3.0 ± 7.9 | 8.0 ± 6.7 |
| Atrial fibrillation | 2% (2/40) | 0% (0/40) |
| eGFR, mL/min/1.73 m2 | 66.8 ± 15.2 | 61.20 ± 13.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morioka, T.; Kato, S.; Onoma, A.; Izumi, T.; Sakano, T.; Ishikawa, E.; Sawamura, S.; Yasuda, N.; Nagase, H.; Utsunomiya, D. Improvement of Quantification of Myocardial Synthetic ECV with Second-Generation Deep Learning Reconstruction. J. Cardiovasc. Dev. Dis. 2024, 11, 304. https://doi.org/10.3390/jcdd11100304
Morioka T, Kato S, Onoma A, Izumi T, Sakano T, Ishikawa E, Sawamura S, Yasuda N, Nagase H, Utsunomiya D. Improvement of Quantification of Myocardial Synthetic ECV with Second-Generation Deep Learning Reconstruction. Journal of Cardiovascular Development and Disease. 2024; 11(10):304. https://doi.org/10.3390/jcdd11100304
Chicago/Turabian StyleMorioka, Tsubasa, Shingo Kato, Ayano Onoma, Toshiharu Izumi, Tomokazu Sakano, Eiji Ishikawa, Shungo Sawamura, Naofumi Yasuda, Hiroaki Nagase, and Daisuke Utsunomiya. 2024. "Improvement of Quantification of Myocardial Synthetic ECV with Second-Generation Deep Learning Reconstruction" Journal of Cardiovascular Development and Disease 11, no. 10: 304. https://doi.org/10.3390/jcdd11100304
APA StyleMorioka, T., Kato, S., Onoma, A., Izumi, T., Sakano, T., Ishikawa, E., Sawamura, S., Yasuda, N., Nagase, H., & Utsunomiya, D. (2024). Improvement of Quantification of Myocardial Synthetic ECV with Second-Generation Deep Learning Reconstruction. Journal of Cardiovascular Development and Disease, 11(10), 304. https://doi.org/10.3390/jcdd11100304