
Physical Activity and Executive Functioning in Children and Adolescents with Congenital Heart Defects: A Scoping Review

 , and
, and
Abstract
:1. Introduction
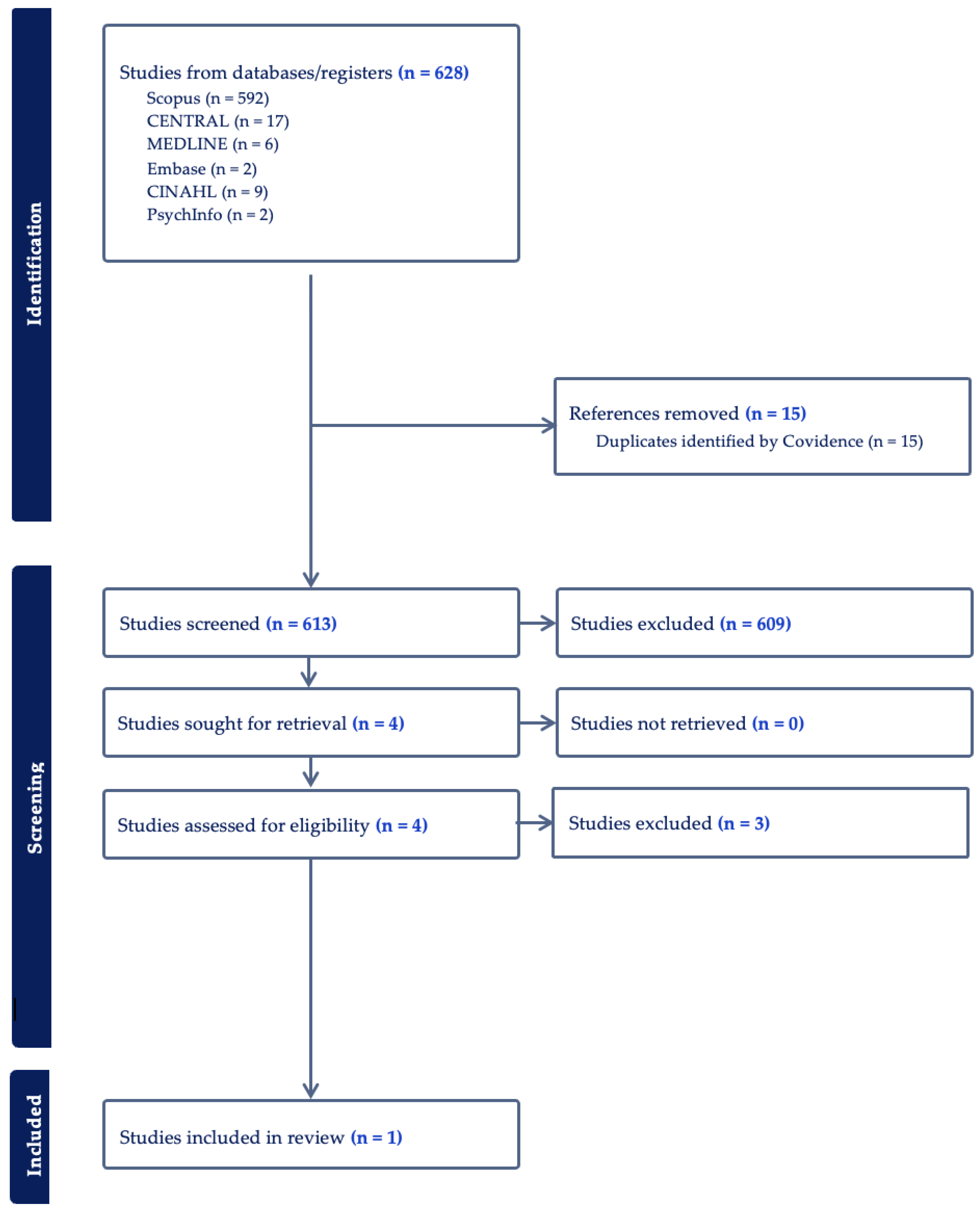
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gauthier, N.; Curran, T.; O’Neill, J.A.; Alexander, M.E.; Rhodes, J. Establishing a comprehensive pediatric cardiac fitness and rehabilitation program for congenital heart disease. Pediatr. Cardiol. 2020, 41, 1569–1579. [Google Scholar] [CrossRef] [PubMed]
- Best, J.R. Effects of physical activity on children’s executive function: Contributions of experimental research on aerobic exercise. Dev. Rev. 2010, 30, 331–351. [Google Scholar] [CrossRef] [PubMed]
- Vassar, R.; Peyvandi, S.; Gano, D.; Cox, S.; Zetino, Y.; Miller, S.; McQuillen, P. Critical congenital heart disease beyond HLHS and TGA: Neonatal brain injury and early neurodevelopment. Pediatr. Res. 2023, 94, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.; Al-Omary, M.; Baker, D.; Spratt, N.; Boyle, A.; Baker, N.; Howe, P.; Collins, N. Cognitive dysfunction is associated with abnormal responses in cerebral blood flow in patients with single ventricular physiology: Novel insights from transcranial Doppler ultrasound. Congenit. Heart Dis. 2019, 14, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Spillmann, R.; Polentarutti, S.; Ehrler, M.; Kretschmar, O.; Wehrle, F.M.; Latal, B. Congenital heart disease in school-aged children: Cognition, education, and participation in leisure activities. Pediatr. Res. 2023, 94, 1523–1529. [Google Scholar] [CrossRef]
- Calderon, J.; Bellinger, D.C. Executive function deficits in congenital heart disease: Why is intervention important? Cardiol. Young 2014, 25, 1238–1246. [Google Scholar] [CrossRef]
- Cassidy, A.R.; White, M.T.; DeMaso, D.R.; Newburger, J.W.; Bellinger, D.C. Executive function in children and adolescents with critical cyanotic congenital heart disease. J. Int. Neuropsychol. Soc. 2015, 21, 34–49. [Google Scholar] [CrossRef]
- Bolduc, M.E.; Lambert, H.; Ganeshamoorthy, S.; Brossard-Racine, M. Structural brain abnormalities in adolescents and young adults with congenital heart defect: A systematic review. Dev. Med. Child. Neurol. 2018, 60, 1209–1224. [Google Scholar] [CrossRef]
- Sanz, J.H.; Wang, J.; Berl, M.M.; Armour, A.C.; Cheng, Y.I.; Donofrio, M.T. Executive function and psychosocial quality of life in school age children with congenital heart disease. J. Pediatr. 2018, 202, 63–69. [Google Scholar] [CrossRef]
- Dishman, R.K.; Berthoud, H.R.; Booth, F.W.; Cotman, C.W.; Edgerton, V.R.; Fleshner, M.R.; Gandevia, S.C.; Gomez-Pinilla, F.; Greenwood, B.N.; Hillman, C.H.; et al. Neurobiology of exercise. Obesity 2006, 14, 345–356. [Google Scholar] [CrossRef]
- Byun, K.; Hyodo, K.; Suwabe, K.; Ochi, G.; Sakairi, Y.; Kato, M.; Dan, I.; Soya, H. Positive effect of acute mild exercise on executive function via arousal-related prefrontal activations: An fNIRS study. Neuroimage 2014, 98, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Lambrick, D.; Stoner, L.; Grigg, R.; Faulkner, J. Effects of continuous and intermittent exercise on executive function in children aged 8–10 years. Psychophysiology 2016, 53, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, S.S.; Chueh, T.Y.; Huang, C.J.; Kao, S.C.; Hillman, C.H.; Chang, Y.K.; Hung, T.M. Systematic review of the acute and chronic effects of high-intensity interval training on executive function across the lifespan. J. Sports Sci. 2021, 39, 10–22. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- Aromataris, E.; Lockwood, C.; Porritt, K.; Pilla, B.; Jordan, Z. (Eds.) JBI Manual for Evidence Synthesis. 2024. Available online: https://synthesismanual.jbi.global (accessed on 5 May 2024).
- Dulfer, K.; Duppen, N.; Kuipers, I.M.; Schokking, M.; van Domburg, R.T.; Verhulst, F.C.; Helbing, W.A.; Utens, E. Aerobic exercise influences quality of life of children and youngsters with congenital heart disease: A randomized controlled trial. J. Adolesc. Health 2014, 55, 65–72. [Google Scholar] [CrossRef]
- Cooney, S.J.; Campbell, K.; Wolfe, K.; DiMaria, M.V.; Rausch, C.M. Is neurodevelopment related to exercise capacity in single ventricle patients who have undergone Fontan palliation? Pediatr. Cardiol. 2021, 42, 408–416. [Google Scholar] [CrossRef]
- Verrall, C.E.; Tran, D.L.; Yang, J.Y.M.; Lubans, D.R.; Winlaw, D.S.; Ayer, J.; Celermajer, D.; Cordina, R. Exercise as therapy for neurodevelopmental and cognitive dysfunction in people with a Fontan circulation: A narrative review. Front. Pediatr. 2023, 11, 1111785. [Google Scholar] [CrossRef]
- Fox, K.R.; Vannatta, K.; Jackson, J.L. Difficulties with Executive Function are associated with risky health behaviors among young adult congenital heart defect survivors. J. Cardiovasc. Nurs. 2023, 38, 60–69. [Google Scholar] [CrossRef]
- Kobayashi, K.; Liu, C.; Jonas, R.A.; Ishibashi, N. The current status of neuroprotection in congenital heart disease. Children 2021, 8, 1116. [Google Scholar] [CrossRef]
- van der Mheen, M.; Meentken, M.G.; van Beynum, I.M.; van der Ende, J.; van Galen, E.; Zirar, A.; Aendekerk, E.W.; Adel, T.P.v.D.; Bogers, A.J.; McCusker, C.G.; et al. CHIP-Family intervention to improve the psychosocial well-being of young children with congenital heart disease and their families: Results of a randomised controlled trial. Cardiol. Young 2019, 29, 1172–1182. [Google Scholar] [CrossRef] [PubMed]
- Marino, B.S.; Lipkin, P.H.; Newburger, J.W.; Peacock, G.; Gerdes, M.; Gaynor, J.W.; Mussatto, K.A.; Uzark, K.; Goldberg, C.S.; Johnson, W.H.; et al. Neurodevelopmental outcomes in children with congenital heart disease: Evaluation and management: A scientific statement from the American Heart Association. Circulation 2012, 126, 1143–1172. [Google Scholar] [CrossRef] [PubMed]
- Bellinger, D.C.; Rappaport, L.A.; Wypij, D.; Wernovsky, G.; Newburger, J.W. Patterns of developmental dysfunction after surgery during infancy to correct transposition of the great arteries. J. Dev. Behav. Pediatr. 1997, 18, 75–83. [Google Scholar] [CrossRef]
- Bellinger, D.C.; Wypij, D.; Kuban, K.C.; Rappaport, L.A.; Hickey, P.R.; Wernovsky, G.; Jonas, R.A.; Newburger, J.W. Developmental and neurological status of children at 4 years of age after heart surgery with hypothermic circulatory arrest or low-flow cardiopulmonary bypass. Circulation 1999, 100, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Bellinger, D.C.; Wypij, D.; duPlessis, A.J.; Rappaport, L.A.; Jonas, R.A.; Wernovsky, G.; Newburger, J.W. Neurodevelopmental status at eight years in children with dextro-transposition of the great arteries: The Boston Circulatory Arrest Trial. J. Thorac. Cardiovasc. Surg. 2003, 126, 1385–1396. [Google Scholar] [CrossRef]
- Bellinger, D.C.; Wypij, D.; Rivkin, M.J.; DeMaso, D.R.; Robertson, R.L., Jr.; Dunbar-Masterson, C.; Rappaport, L.A.; Wernovsky, G.; Jonas, R.A.; Newburger, J.W. Adolescents with d-transposition of the great arteries corrected with the arterial switch procedure: Neuropsychological assessment and structural brain imaging. Circulation 2011, 124, 1361–1369. [Google Scholar] [CrossRef]
- Bellinger, D.C.; Watson, C.G.; Rivkin, M.J.; Robertson, R.L.; Roberts, A.E.; Stopp, C.; Dunbar-Masterson, C.; Bernson, D.; DeMaso, D.R.; Wypij, D.; et al. Neuropsychological status and structural brain imaging in adolescents with single ventricle who underwent the Fontan procedure. J. Am. Heart Assoc. 2015, 4, e002302. [Google Scholar] [CrossRef]
- Sananes, R.; Goldberg, C.S.; Newburger, J.W.; Hu, C.; Trachtenberg, F.; Gaynor, J.W.; Mahle, W.T.; Miller, T.; Uzark, K.; Mussatto, K.A.; et al. Six-year neurodevelopmental outcomes for children with single-ventricle physiology. Pediatrics 2021, 147, e2020014589. [Google Scholar] [CrossRef]
- Sanz, J.H.; Berl, M.M.; Armour, A.C.; Wang, J.; Cheng, Y.I.; Donofrio, M.T. Prevalence and pattern of executive dysfunction in school age children with congenital heart disease. Congenit. Heart Dis. 2017, 12, 202–209. [Google Scholar] [CrossRef]
- Rogers, S.; Dixon, B. The new age of cardiac rehab: Do adult protocols meet the needs of children? Arch. Phys. Med. Rehabil. 2021, 102, e114. [Google Scholar] [CrossRef]
- Kwon, S.J.; Choi, E.K.; Lee, K.H.; Im, Y.M. Factors influencing physical activity in adolescents with complex congenital heart disease. Child. Health Nurs. Res. 2019, 25, 262–272. [Google Scholar] [CrossRef] [PubMed]
- Lui, G.K.; Saidi, A.; Bhatt, A.B.; Burchill, L.J.; Deen, J.F.; Earing, M.G.; Gewitz, M.; Ginns, J.; Kay, J.D.; Kim, Y.Y.; et al. Diagnosis and management of noncardiac complications in adults with congenital heart disease: A scientific statement from the American heart association. Circulation 2017, 136, e348–e392. [Google Scholar] [CrossRef] [PubMed]
- Soshi, T.; Andersson, M.; Kawagoe, T.; Nishiguchi, S.; Yamada, M.; Otsuka, Y.; Nakai, R.; Abe, N.; Aslah, A.; Igasaki, T.; et al. Prefrontal plasticity after a 3-month exercise intervention in older adults relates to enhanced cognitive performance. Cereb. Cortex 2021, 31, 4501–4517. [Google Scholar] [CrossRef] [PubMed]
- Wilckens, K.A.; Stillman, C.M.; Waiwood, A.M.; Kang, C.; Leckie, R.L.; Peven, J.C.; Foust, J.E.; Fraundorf, S.H.; Erickson, K.I. Exercise interventions preserve hippocampal volume: A meta-analysis. Hippocampus 2021, 31, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Raichlen, D.A.; Klimentidis, Y.C.; Bharadwaj, P.K.; Alexander, G.E. Differential associations of engagement in physical activity and estimated cardiorespiratory fitness with brain volume in middle-aged to older adults. Brain Imaging Behav. 2020, 14, 1994–2003. [Google Scholar] [CrossRef]
- Chaddock, L.; Erickson, K.I.; Prakash, R.S.; Kim, J.S.; Voss, M.W.; Vanpatter, M.; Pontifex, M.B.; Raine, L.B.; Konkel, A.; Hillman, C.H.; et al. A neuroimaging investigation of the association between aerobic fitness, hippocampal volume, and memory performance in preadolescent children. Brain Res. 2010, 1358, 172–183. [Google Scholar] [CrossRef]
- Riggs, L.; Piscione, J.; Laughlin, S.; Cunningham, T.; Timmons, B.W.; Courneya, K.S.; Bartels, U.; Skocic, J.; de Medeiros, C.; Liu, F.; et al. Exercise training for neural recovery in a restricted sample of pediatric brain tumor survivors: A controlled clinical trial with crossover of training versus no training. Neuro Oncol. 2017, 19, 440–450. [Google Scholar] [CrossRef]

{kind=link}
| Author | Dulfer et al. [17] | Cooney et al. [18] | Verrall et al. [19] |
|---|---|---|---|
| Aims/Purpose | To investigate the effect of an exercise program on HRQoL in children and adolescents with TOF or Fontan circulation. | To characterize the relationship between neurodevelopment and exercise capacity in SVHD post-Fontan by evaluating associations between CPET and clinical NPT. | To discuss current interventions and evidence supporting exercise as a potential intervention for improving cognitive functioning in people with Fontan circulation. |
| Population | Ninety-three participants, ages 10–25 years, had a surgical repair for ToF or with Fontan circulation. | Twenty-three participants, ages 7–17 years old, with Fontan circulation. | Discusses impact from fetus to aging adult. |
| Methodology | Stratified, randomized controlled intervention conducted in five pediatric centers in The Netherlands. Random allocation with a ratio of 2:1 in a 12-week period with an exercise program of three times per week or a control group. | Retrospective, cross-sectional pilot study conducted in the United States. One-time conduction of CPET with gas analysis and one-time conduction of NPT. | Narrative summary and discussion with the following categories: established neurodevelopmental and cognitive interventions; exercise, cognition, and Fontan physiology; neural mechanisms underpinning the exercise–cognition relationship; and psychosocial and behavioral mediators of the exercise–cognition relationship. |
| Interventions | Exercise program consisted of three one-hour long training sessions a week. Patients already active were encouraged to continue to perform activities two times a week. An hour session consisted of 10 min warm up, 40 min aerobic training, and 10 min cooldown. Participants trained within given heart rate ranges. | Exercise testing was performed with a Medgraphics (Saint Paul, MN, USA) metabolic cart. Breath-by-breath data were collected and averaged over 20 s intervals. Patients performed a symptom-limited test using a ramp protocol on a cycle ergometer. Oxygen saturation was monitored, and electrocardiogram and blood pressure were also measured. NPT was conducted in a single session on a day separate from the CPET. Standardized scores were assessed from tests of working memory, processing speed, sustained visual attention, executive function, parent ratings of adaptive function, and internalizing problems. Scores were standardized by age. | Individuals with Fontan physiology have a greater risk of neurodevelopmental and cognitive impairments. Exercise is low-risk and has benefits on physical and cognitive functioning. Future research is needed to provide exercise prescriptions and determine accessible interventions. |
| Outcomes | At baseline and follow-up after 12 weeks, participants and parents, as appropriate, completed the HRQoL measures: for the 10–15 group, TACQOL CF and TACQOL PF; for the 16–25 group, SF-36 and CONHD-TAAQOL; and for the total group 10–25, LAS. | CPET measures: VO2max indexed to body weight, anaerobic threshold, peak heart rate, ventilatory efficiency, pulmonary vasodilator use, and RER. Results were compared to percent predicted values for VO2max and peak heart rate based on gender, height, and weight. NPT measures: executive function (WAIS-IV or WISC-V and TOL), attention (CPT-2,3), adaptive function (ABAS-2,3), and emotional function (BASC-2,3). | |
| Key Findings | Compared with the control group, children aged 10–15 years in the exercise group improved significantly in self-reported cognitive functioning and parent-reported social functioning. Increase was noted in this group with lower baseline HRQoL. Participants aged 16–25 years did not change their HRQoL. | Higher VO2max and anaerobic thresholds were related to better adaptive functioning scores, and higher peak heart rates were related to better scores when measuring sustained visual attention. The relationship appeared strongest in relation to adaptive function, as both higher VO2 max and anaerobic threshold were significantly associated with a higher global adaptive composite score. CPET variables related to working memory, processing speed, executive functioning, or internalizing symptoms were not significant. Ventilatory efficiency was not significantly related to any of the NPT variables. | Interventions for impaired neurodevelopment and cognitive dysfunction in people with Fontan circulation are lacking. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clifton, A.; Kirk-Sanchez, N.; Cipriano, G., Jr.; Moore, J.G.; Cahalin, L.P. Physical Activity and Executive Functioning in Children and Adolescents with Congenital Heart Defects: A Scoping Review. J. Cardiovasc. Dev. Dis. 2024, 11, 309. https://doi.org/10.3390/jcdd11100309
Clifton A, Kirk-Sanchez N, Cipriano G Jr., Moore JG, Cahalin LP. Physical Activity and Executive Functioning in Children and Adolescents with Congenital Heart Defects: A Scoping Review. Journal of Cardiovascular Development and Disease. 2024; 11(10):309. https://doi.org/10.3390/jcdd11100309
Chicago/Turabian StyleClifton, Amanda, Neva Kirk-Sanchez, Gerson Cipriano, Jr., James G. Moore, and Lawrence P. Cahalin. 2024. "Physical Activity and Executive Functioning in Children and Adolescents with Congenital Heart Defects: A Scoping Review" Journal of Cardiovascular Development and Disease 11, no. 10: 309. https://doi.org/10.3390/jcdd11100309