
Adverse Events Requiring Hospitalization Following Catheter Ablation for Atrial Fibrillation in Heart Failure with versus without Systolic Dysfunction



Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Baseline Characteristics and Classification Based on Left Ventricular EF
2.3. Ablation Procedures
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Catheter Ablation for AF
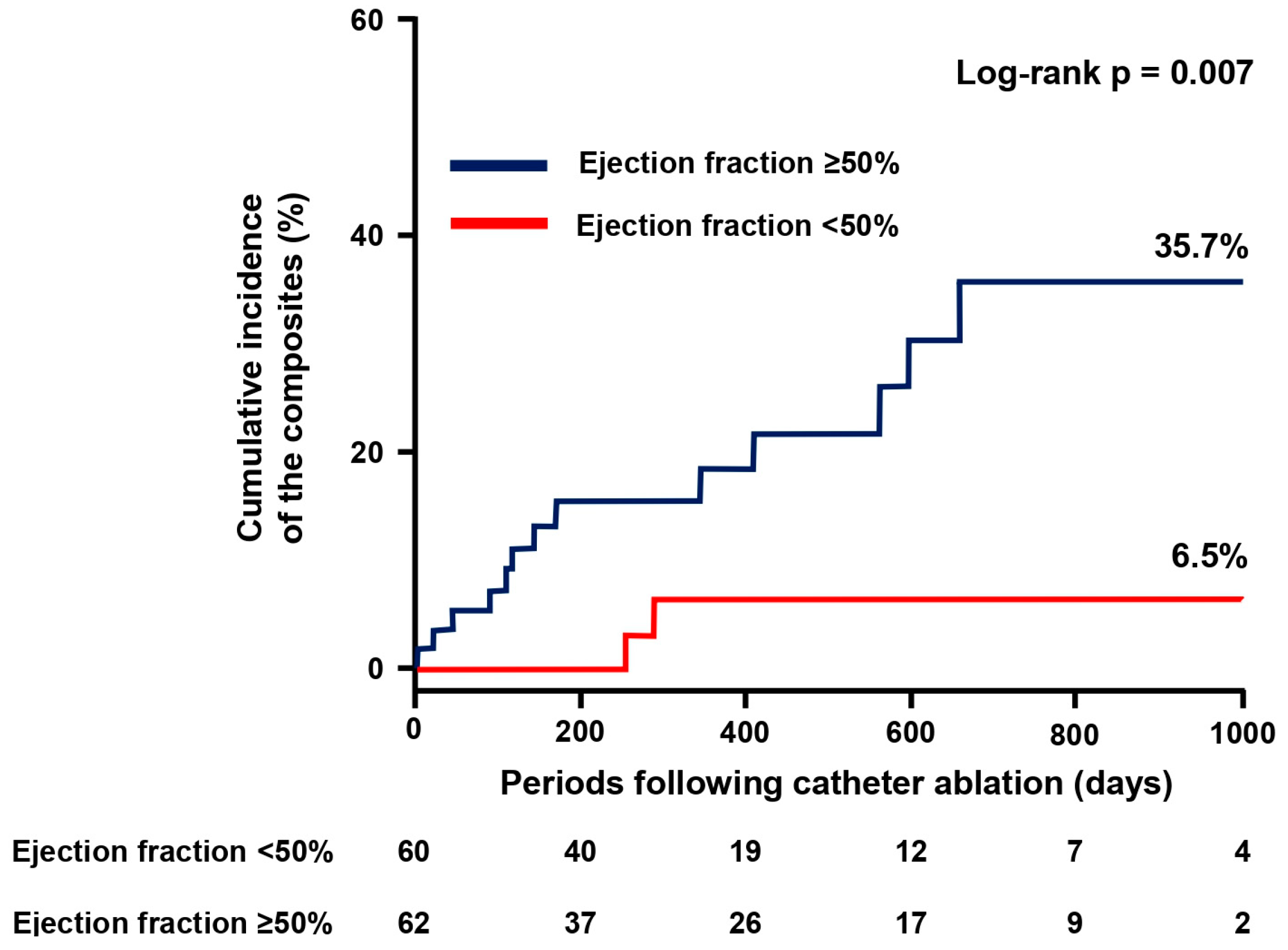
3.3. Primary Endpoint
3.4. Secondary Endpoint
4. Discussion
4.1. Impacts of AF Ablation on Improving EF
4.2. Maintenance of Sinus Rhythm Following AF Ablation
4.3. How to Assess the Impact of AF Ablation on HF and Preserved EF
4.4. Clinical Outcomes Following Catheter Ablation
4.5. Post-Ablation Gastrointestinal Bleeding
4.6. Clinical Perspective
4.7. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lubitz, S.A.; Moser, C.; Sullivan, L.; Rienstra, M.; Fontes, J.D.; Villalon, M.L.; Pai, M.; McManus, D.D.; Schnabel, R.B.; Magnani, J.W.; et al. Atrial Fibrillation Patterns and Risks of Subsequent Stroke, Heart Failure, or Death in the Community. J. Am. Heart Assoc. 2013, 2, e000126. [Google Scholar] [CrossRef]
- Wang, T.J.; Larson, M.G.; Levy, D.; Vasan, R.S.; Leip, E.P.; Wolf, P.A.; D’Agostino, R.B.; Murabito, J.M.; Kannel, W.B.; Benjamin, E.J. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: The Framingham Heart Study. Circulation 2003, 107, 2920–2925. [Google Scholar] [CrossRef] [PubMed]
- Carlisle, M.A.; Fudim, M.; DeVore, A.D.; Piccini, J.P. Heart Failure and Atrial Fibrillation, Like Fire and Fury. JACC Heart Fail. 2019, 7, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Zafrir, B.; Lund, L.H.; Laroche, C.; Ruschitzka, F.; Crespo-Leiro, M.G.; Coats, A.J.S.; Anker, S.D.; Filippatos, G.; Seferovic, P.M.; Maggioni, A.P.; et al. Prognostic implications of atrial fibrillation in heart failure with reduced, mid-range, and preserved ejection fraction: A report from 14,964 patients in the European Society of Cardiology Heart Failure Long-Term Registry. Eur. Heart J. 2018, 39, 4277–4284. [Google Scholar] [CrossRef] [PubMed]
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Zylla, M.M.; Leiner, J.; Rahm, A.-K.; Hoffmann, T.; Lugenbiel, P.; Schweizer, P.; Scholz, E.; Mereles, D.; Kronsteiner, D.; Kieser, M.; et al. Catheter Ablation of Atrial Fibrillation in Patients with Heart Failure and Preserved Ejection Fraction. Circ. Heart Fail. 2022, 15, e009281. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthy, A.; Goyal, P.; Markowitz, S.M.; Liu, C.F.; Thomas, G.; Ip, J.E.; Horn, E.M.; Lerman, B.B.; Kim, L.K.; Cheung, J.W. Outcomes of patients with heart failure with preserved ejection fraction undergoing catheter ablation of atrial fibrillation. Heart Rhythm. O2 2022, 3, 501–508. [Google Scholar] [CrossRef]
- Machino-Ohtsuka, T.; Seo, Y.; Ishizu, T.; Yamamoto, M.; Hamada-Harimura, Y.; Machino, T.; Yamasaki, H.; Sekiguchi, Y.; Nogami, N.; Aonuma, K.; et al. Relationships between maintenance of sinus rhythm and clinical outcomes in pa-tients with heart failure with preserved ejection fraction and atrial fibrillation. J. Cardiol. 2019, 74, 235–244. [Google Scholar] [CrossRef]
- Rattka, M.; Kühberger, A.; Pott, A.; Stephan, T.; Weinmann, K.; Baumhardt, M.; Aktolga, D.; Teumer, Y.; Bothner, C.; Scharnbeck, D.; et al. Catheter ablation for atrial fibrillation in HFpEF patients-A propensity-score-matched analysis. J. Cardiovasc. Electrophysiol. 2021, 32, 2357–2367. [Google Scholar] [CrossRef]
- Fujimoto, H.; Doi, N.; Okayama, S.; Naito, M.; Kobori, A.; Kaitani, K.; Inoue, K.; Kurotobi, T.; Morishima, I.; Yamaji, H.; et al. Long-term prognosis of patients undergoing radiofrequency catheter ablation for atrial fibrillation: Comparison between heart failure subtypes based on left ventricular ejection fraction. Europace 2022, 24, 576–586. [Google Scholar] [CrossRef]
- Arora, S.; Lahewala, S.; Tripathi, B.; Mehta, V.; Kumar, V.; Chandramohan, D.; Lemor, A.; Dave, M.; Patel, N.; Patel, N.V.; et al. Causes and Predictors of Readmission in Patients with Atrial Fibrillation Undergoing Catheter Ablation: A National Population-Based Cohort Study. J. Am. Heart Assoc. 2018, 7, e009294. [Google Scholar] [CrossRef] [PubMed]
- Kotecha, D.; Lam, C.S.; Van Veldhuisen, D.J.; Van Gelder, I.C.; Voors, A.A.; Rienstra, M. Heart Failure with Preserved Ejection Fraction and Atrial Fibrillation: Vicious Twins. J. Am. Coll. Cardiol. 2016, 68, 2217–2228. [Google Scholar] [CrossRef] [PubMed]
- Hatori, Y.; Sakai, H.; Hatori, N.; Kunishima, T.; Namiki, A.; Shimizu, M.; Toyosaki, N.; Kuwajima, M.; Sato, N. Long-term outcome and risk factors associated with events in patients with atrial fibrillation treated with oral anticoagulants: The ASSAF-K registry. J. Cardiol. 2022, 81, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation devel-oped in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.-H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e263–e421. [Google Scholar] [CrossRef] [PubMed]
- Mulder, B.A.; Rienstra, M.; Van Gelder, I.C.; Blaauw, Y. Update on management of atrial fibrillation in heart failure: A focus on ablation. Heart 2022, 108, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Angaran, P.; Dorian, P.; Ha, A.C.; Thavendiranathan, P.; Tsang, W.; Leong-Poi, H.; Woo, A.; Dias, B.; Wang, X.; Austin, P.C.; et al. Association of Left Ventricular Ejection Fraction with Mortality and Hospitalizations. J. Am. Soc. Echocardiogr. 2020, 33, 802–811.e6. [Google Scholar] [CrossRef]
- Zhang, X.; Sun, Y.; Zhang, Y.; Chen, F.; Dai, M.; Si, J.; Yang, J.; Li, X.; Li, J.; Xia, Y.; et al. Characteristics and outcomes of heart failure with recovered left ventricular ejection fraction. ESC Heart Fail. 2021, 8, 5383–5391. [Google Scholar] [CrossRef]
- Verma, A.; Jiang, C.-Y.; Betts, T.R.; Chen, J.; Deisenhofer, I.; Mantovan, R.; Macle, L.; Morillo, C.A.; Haverkamp, W.; Weerasooriya, R.; et al. Approaches to Catheter Ablation for Persistent Atrial Fibrillation. N. Engl. J. Med. 2015, 372, 1812–1822. [Google Scholar] [CrossRef]
- Cohen, J.B.; Schrauben, S.J.; Zhao, L.; Basso, M.D.; Cvijic, M.E.; Li, Z.; Yarde, M.; Wang, Z.; Bhattacharya, P.T.; Chirinos, D.A.; et al. Clinical Phenogroups in Heart Failure with Preserved Ejection Fraction. JACC Heart Fail. 2020, 8, 172–184. [Google Scholar] [CrossRef]
- Nogami, A.; Kurita, T.; Abe, H.; Ando, K.; Ishikawa, T.; Imai, K.; Usui, A.; Okishige, K.; Kusano, K.; Kumagai, K.; et al. JCS/JHRS 2019 guideline on non-pharmacotherapy of cardiac arrhythmias. J. Arrhythm. 2021, 37, 709–870. [Google Scholar] [CrossRef] [PubMed]
- Mentias, A.; Briasoulis, A.; Shantha, G.; Alvarez, P.; Vaughan-Sarrazin, M. Impact of Heart Failure Type on Thromboembolic and Bleeding Risk in Patients with Atrial Fibrillation on Oral Anticoagulation. Am. J. Cardiol. 2019, 123, 1649–1653. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Keshishian, A.V.; Zhang, Y.; Kang, A.; Dhamane, A.D.; Luo, X.; Klem, C.; Ferri, M.; Jiang, J.; Yuce, H.; et al. Oral An-ticoagulants for Nonvalvular Atrial Fibrillation in Patients with High Risk of Gastrointestinal Bleeding. JAMA Netw Open. 2021, 4, e2120064. [Google Scholar] [CrossRef] [PubMed]
- Schrutka, L.; Seirer, B.; Duca, F.; Binder, C.; Dalos, D.; Kammerlander, A.; Aschauer, S.; Koller, L.; Benazzo, A.; Agibetov, A.; et al. Patients with Heart Failure and Preserved Ejection Fraction Are at Risk of Gastrointestinal Bleeding. J. Clin. Med. 2019, 8, 1240. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Cai, X.; Yang, Y.; Zhou, Y.; Zhu, W. Diagnostic Accuracy of the HAS-BLED Bleeding Score in VKA- or DOAC-Treated Patients with Atrial Fibrillation: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2021, 8, 757087. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Patel, R.B.; Michel, A.; Shah, S.J.; Senni, M.; Gheorghiade, M.; Butler, J. Mode of Death in Heart Failure with Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2017, 69, 556–569. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, T.; Lin, Y.; Ibrahim, A. Chronic low-grade inflammation in heart failure with preserved ejection fraction. Aging Cell 2021, 20, e13453. [Google Scholar] [CrossRef]
- Frangogiannis, N.G. The Extracellular Matrix in Ischemic and Nonischemic Heart Failure. Circ. Res. 2019, 125, 117–146. [Google Scholar] [CrossRef]
- Alfano, F.; Cesari, F.; Gori, A.M.; Berteotti, M.; Salvadori, E.; Giusti, B.; Bertelli, A.; Kura, A.; Barbato, C.; Formelli, B.; et al. The Role of Extracellular Matrix and Inflammation in the Stratification of Bleeding and Thrombotic Risk of Atrial Fibrillation on Oral Anticoagulant Therapy: Insights from Strat-Af Study. J. Clin. Med. 2023, 12, 6866. [Google Scholar] [CrossRef]
- Benali, K.; Khairy, P.; Hammache, N.; Petzl, A.; Da Costa, A.; Verma, A.; Andrade, J.G.; Macle, L. Procedure-Related Complications of Catheter Ablation for Atrial Fibrillation. J. Am. Coll. Cardiol. 2023, 81, 2089–2099. [Google Scholar] [CrossRef]
- Yamagata, K.; Wichterle, D.; Roubíček, T.; Jarkovský, P.; Sato, Y.; Kogure, T.; Peichl, P.; Konečný, P.; Jansová, H.; Kučera, P.; et al. Ultrasound-guided versus conventional femoral venipuncture for catheter ablation of atrial fibrillation: A multicentre randomized efficacy and safety trial (ULTRA-FAST trial). Europace 2017, 20, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Kupó, P.; Pap, R.; Sághy, L.; Tényi, D.; Bálint, A.; Debreceni, D.; Basu-Ray, I.; Komócsi, A. Ultrasound guidance for femoral venous access in electrophysiology procedures—Systematic review and meta-analysis. J. Interv. Card. Electrophysiol. 2020, 59, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Kupo, P.; Riesz, T.J.; Saghy, L.; Vamos, M.; Bencsik, G.; Makai, A.; Kohari, M.; Benak, A.; Miklos, M.; Pap, R. Ultrasound guidance for femoral venous access in patients undergoing pulmonary vein isolation: A quasi-randomized study. J. Cardiovasc. Electrophysiol. 2023, 34, 1177–1182. [Google Scholar] [CrossRef] [PubMed]
- Boersma, L.V.; Ince, H.; Kische, S.; Pokushalov, E.; Schmitz, T.; Schmidt, B.; Gori, T.; Meincke, F.; Protopopov, A.V.; EWOLUTION Investigators; et al. Evaluating Real-World Clinical Outcomes in Atrial Fibrillation Patients Receiving the WATCHMAN Left Atrial Appendage Closure Technology: Final 2-Year Outcome Data of the EWOLUTION Trial Focusing on History of Stroke and Hemorrhage. Circ. Arrhythm. Electrophysiol. 2019, 12, e006841. [Google Scholar] [CrossRef]
- Harrington, J.; Piccini, J.P.; Alexander, J.H.; Granger, C.B.; Patel, M.R. Clinical Evaluation of Factor Xia Inhibitor Drugs: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2023, 81, 71–779. [Google Scholar] [CrossRef]
- Kishima, H.; Mine, T.; Fukuhara, E.; Kitagaki, R.; Asakura, M.; Ishihara, M. Efficacy of Sodium-Glucose Cotransporter 2 Inhib-itors on Outcomes After Catheter Ablation for Atrial Fibrillation. JACC Clin. Electrophysiol. 2022, 8, 1393–1404. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall | EF < 50% | EF ≥ 50% | p Value |
|---|---|---|---|---|
| Number of patients | 122 | 60 | 62 | |
| Age (years) | 75 [70–79] | 74 [64–79] | 77 [72–80] | 0.020 |
| Female, n (%) | 54 (44) | 25 (42) | 29 (47) | 0.570 |
| Body mass index (kg/m2) | 22.2 [19.6–25.4] | 21.3 [19.1–24.2] | 23.7 [20.2–25.8] | 0.050 |
| Paroxysmal AF, n (%) | 48 (39) | 19 (32) | 29 (47) | 0.088 |
| CHADS2 | 3 [2–3] | 3 [2–3] | 3 [2–3] | 0.674 |
| CHA2DS2-VASc | 4 [3–5] | 4 [3–5] | 4 [3–5] | 0.089 |
| HAS-BLED | 1 [1–2] | 1 [1–2] | 1 [1–2] | 0.521 |
| Daily drinking, n (%) | 38 (31) | 18 (30) | 20 (32) | 0.788 |
| Daily smoking, n (%) | 20 (16) | 10 (17) | 10 (16) | 0.936 |
| Comorbidities | ||||
| Hypertension, n (%) | 69 (57) | 26 (43) | 43 (69) | 0.004 |
| Diabetes mellitus, n (%) | 36 (30) | 18 (30) | 18 (29) | 0.907 |
| Dyslipidemia, n (%) | 39 (32) | 18 (30) | 21 (34) | 0.647 |
| Ischemic etiology, n (%) | 22 (18) | 11 (18) | 11 (18) | 0.932 |
| Primary cardiomyopathies, n (%) | 32 (26) | 27 (45) | 5 (8) | <0.001 |
| Valvular heart diseases, n (%) | 14 (11) | 4 (7) | 10 (16) | 0.101 |
| CIEDs, n (%) | 19 (16) | 15 (25) | 4 (6) | 0.005 |
| Pacemaker, n (%) | 7 (6) | 5 (8) | 2 (3) | 0.225 |
| Implantable cardioverter defibrillator, n (%) | 10 (8) | 8 (13) | 2 (3) | 0.042 |
| Cardiac resynchronization therapy, n (%) | 10 (8) | 10 (17) | 0 (0) | 0.001 |
| Left atrial appendage closure devices, n (%) | 14 (11) | 7 (12) | 7 (11) | 0.948 |
| Medications | ||||
| ACEi or ARB, n (%) | 63 (52) | 30 (50) | 33 (53) | 0.722 |
| ARNI, n (%) | 28 (23) | 20 (33) | 8 (13) | 0.007 |
| β-blockers, n (%) | 103 (84) | 57 (95) | 46 (74) | 0.002 |
| MRA, n (%) | 59 (48) | 38 (63) | 21 (34) | 0.001 |
| SGLT2 inhibitor, n (%) | 52 (43) | 34 (57) | 18 (29) | 0.002 |
| Loop diuretics, n (%) | 76 (62) | 38 (63) | 38 (62) | 0.906 |
| Anti-arrhythmic drugs | ||||
| Amiodarone, n (%) | 36 (30) | 22 (37) | 14 (23) | 0.088 |
| Bepridil, n (%) | 5 (4) | 1 (2) | 4 (6) | 0.183 |
| Sodium channel blockers, n (%) | 2 (2) | 0 (0) | 2 (3) | 0.161 |
| Anticoagulant | ||||
| Dabigatran, n (%) | 32 (26) | 15 (25) | 17 (27) | 0.761 |
| Apixaban, n (%) | 43 (35) | 23 (38) | 20 (32) | 0.483 |
| Edoxaban, n (%) | 30 (25) | 15 (25) | 15 (24) | 0.918 |
| Rivaroxaban, n (%) | 5 (4) | 1 (2) | 4 (6) | 0.183 |
| Warfarin, n (%) | 12 (10) | 6 (10) | 6 (10) | 0.952 |
| Antiplatelet, n (%) | 25 (20) | 12 (20) | 13 (21) | 0.895 |
| Echocardiographic parameters | ||||
| LVEF (%) | 50 [37–64] | 37 [29–44] | 64 [55–68] | <0.001 |
| LV end diastolic diameter (mm) | 49 [45–54] | 53 [49–60] | 46 [42–49] | <0.001 |
| LV end systolic diameter (mm) | 36 [29–43] | 42 [37–50] | 29 [26–33] | <0.001 |
| Left atrial diameter (mm) | 45 [40–50] | 45 [39–50] | 45 [40–50] | 0.852 |
| Laboratory data | ||||
| Aspartate aminotransferase, mg/dL | 24 [20–30] | 23 [18–33] | 24 [20–28] | 0.743 |
| Alanine aminotransferase, mg/dl | 18 [12–23] | 19 [13–26] | 17 [12–23] | 0.192 |
| γ-Glutamyl transpeptidase, mg/dL | 30 [22–56] | 32 [23–55] | 29 [19–58] | 0.313 |
| Creatinine, mg/dL | 1.0 [0.8–1.3] | 1.0 [0.9–1.4] | 0.9 [0.8–1.3] | 0.055 |
| Estimated GFR, mL/min/1.73 m2 | 51 [38–63] | 48 [36–63] | 52 [42–63] | 0.281 |
| Sodium, mEq/L | 140 [138–142] | 139 [137–142] | 141 [140–142] | 0.004 |
| Potassium, mEq/L | 4.4 [4.1–4.6] | 4.4 [4.1–4.6] | 4.4 [4.1–4.6] | 0.655 |
| Hemoglobin, g/dL | 13.1 [11.6–14.3] | 13.5 [11.8–14.7] | 12.7 [11.1–14.0] | 0.059 |
| N-terminal pro-B-type natriuretic peptide, pg/mL | 1403 [570–3060] | 2242 [651–3887] | 1188 [469–1896] | 0.011 |
| B-type natriuretic peptide, pg/mL | 184 [85–413] | 223 [86–476] | 169 [85–348] | 0.215 |
| Troponin I, pg/mL | 10.0 [0–26.8] | 11 [0–26] | 10 [0–28] | 0.763 |
| Uric acid, mg/dL | 6.1 [4.8–7.2] | 5.8 [4.7–6.9] | 6.2 [4.9–7.5] | 0.253 |
| C-reactive protein, mg/dL | 0.10 [0.05–0.29] | 0.09 [0.06–0.64] | 0.11 [0.04–0.23] | 0.191 |
| Overall | EF < 50% | EF ≥ 50% | p Value | |
|---|---|---|---|---|
| Cryoballoon ablation, n (%) | 78 (64) | 38 (63) | 40 (65) | 0.892 |
| Pulmonary vein isolation, n (%) | 122 (100) | 60 (100) | 62 (100) | |
| Additional linear ablation, n (%) | 68 (56) | 42 (70) | 26 (42) | 0.002 |
| Roofline with cryoballoon, n (%) | 28 (23) | 20 (33) | 8 (13) | 0.007 |
| Posterior wall isolation, n (%) | 28 (23) | 15 (25) | 13 (21) | 0.597 |
| Mitral isthmus block line, n (%) | 1 (0) | 1 (2) | 0 | 0.307 |
| Superior vena cava isolation, n (%) | 1 (0) | 1 (2) | 0 | 0.307 |
| Cavotricuspid isthmus block line, n (%) | 15 (12) | 8 (13) | 7 (11) | 0.731 |
| Hazard Ratio | 95% CI | p Value | |
|---|---|---|---|
| Model 1 | |||
| HF with EF ≥ 50% | 6.18 | 1.36–28.04 | 0.018 |
| CHA2SD2-VASc Score (1 point increase) | 0.91 | 0.63–1.32 | 0.622 |
| Model 2 | |||
| HF with EF ≥ 50% | 6.53 | 1.45–29.28 | 0.014 |
| HAS-BELD Score (1 point increase) | 1.63 | 0.91–2.70 | 0.073 |
| Model 3 | |||
| HF with EF ≥ 50% | 9.27 | 1.82–47.18 | 0.007 |
| Primary cardiomyopathies | 2.41 | 0.69–8.40 | 0.169 |
| Model 4 | |||
| HF with EF ≥ 50% | 7.23 | 1.40–37.30 | 0.018 |
| CIEDs | 1.59 | 0.30–8.23 | 0.580 |
| Model 5 | |||
| HF with EF ≥ 50% | 6.79 | 1.50–30.68 | 0.013 |
| Creatinine (1 mg/dL increase) | 1.24 | 0.950–01.47 | 0.092 |
| Model 6 | |||
| HF with EF ≥ 50% | 7.36 | 1.51–35.83 | 0.013 |
| Sodium (1 mEq/L increase) | 0.93 | 0.79–1.12 | 0.404 |
| Model 7 | |||
| HF with EF ≥ 50% | 5.31 | 1.18–23.87 | 0.030 |
| Recurrence of any atrial tachyarrhythmias | 2.15 | 0.72–6.40 | 0.170 |
| Model 8 | |||
| HF with EF ≥ 50% | 6.27 | 1.37–28.81 | 0.018 |
| Additional liner ablation | 1.11 | 0.39–3.15 | 0.841 |
| Case No. | Age at Enrollment | Gender | Underlying Heart Disease | Type of AF | CHA2DS2-VASc | HAS-BLED | Outcomes |
|---|---|---|---|---|---|---|---|
| HF with impaired EF | |||||||
| 1 | 79 | Female | None | Long-persistent | 4 | 1 | HF with AF recurrence |
| 2 | 70 | Male | Hypertrophic cardiomyopathy | Paroxysmal | 4 | 1 | HF without AF recurrence |
| HF with preserved EF | |||||||
| 1 | 75 | Male | None | Paroxysmal | 4 | 2 | Stroke |
| 2 | 79 | Female | None | Paroxysmal | 5 | 1 | Gastrointestinal bleeding |
| 3 | 64 | Male | Ischemia | Persistent | 2 | 2 | HF with AF recurrence |
| 4 | 67 | Male | Hypertrophic cardiomyopathy | Paroxysmal | 3 | 2 | HF without AF recurrence |
| 5 | 84 | Female | None | Paroxysmal | 4 | 1 | HF due to gastrointestinal bleeding |
| 6 | 86 | Female | None | Paroxysmal | 4 | 1 | HF due to gastrointestinal bleeding |
| 7 | 78 | Male | None | Long and persistent | 3 | 1 | Stroke |
| 8 | 86 | Male | None | Paroxysmal | 5 | 1 | HF with AF recurrence |
| 9 | 76 | Female | Amyloidosis | Paroxysmal | 5 | 3 | HF with AF recurrence |
| 10 | 83 | Male | None | Paroxysmal | 3 | 1 | Sudden cardiac death |
| 11 | 79 | Female | None | Paroxysmal | 5 | 1 | HF with AF recurrence |
| 12 | 68 | Male | None | Paroxysmal | 5 | 4 | Bleeding from the puncture site |
| 13 | 74 | Male | None | Paroxysmal | 6 | 3 | HF with AF recurrence |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kataoka, N.; Imamura, T.; Koi, T.; Uchida, K.; Kinugawa, K. Adverse Events Requiring Hospitalization Following Catheter Ablation for Atrial Fibrillation in Heart Failure with versus without Systolic Dysfunction. J. Cardiovasc. Dev. Dis. 2024, 11, 35. https://doi.org/10.3390/jcdd11020035
Kataoka N, Imamura T, Koi T, Uchida K, Kinugawa K. Adverse Events Requiring Hospitalization Following Catheter Ablation for Atrial Fibrillation in Heart Failure with versus without Systolic Dysfunction. Journal of Cardiovascular Development and Disease. 2024; 11(2):35. https://doi.org/10.3390/jcdd11020035
Chicago/Turabian StyleKataoka, Naoya, Teruhiko Imamura, Takahisa Koi, Keisuke Uchida, and Koichiro Kinugawa. 2024. "Adverse Events Requiring Hospitalization Following Catheter Ablation for Atrial Fibrillation in Heart Failure with versus without Systolic Dysfunction" Journal of Cardiovascular Development and Disease 11, no. 2: 35. https://doi.org/10.3390/jcdd11020035
APA StyleKataoka, N., Imamura, T., Koi, T., Uchida, K., & Kinugawa, K. (2024). Adverse Events Requiring Hospitalization Following Catheter Ablation for Atrial Fibrillation in Heart Failure with versus without Systolic Dysfunction. Journal of Cardiovascular Development and Disease, 11(2), 35. https://doi.org/10.3390/jcdd11020035