
Nitroprusside Combined with Leg Raise at the Time of Right Heart Catheterization to Differentiate Precapillary from Other Hemodynamic Forms of Pulmonary Hypertension: A Single-Center Pilot Study

Abstract
1. Introduction
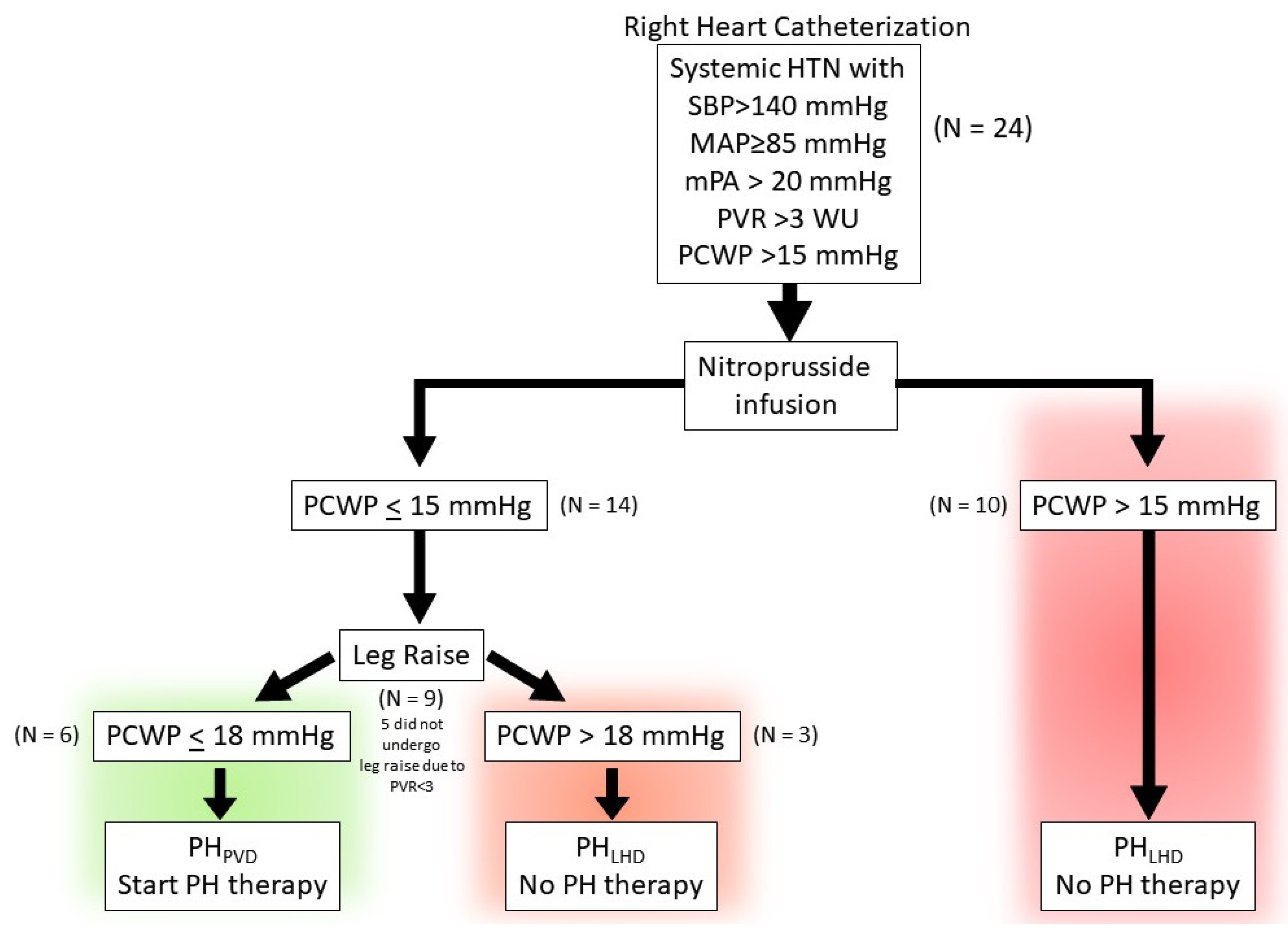
- (1)
- the PCWP decreases to ≤15 mmHg and PVR remains ≥3 with nitroprusside infusion, suggestive of predominant precapillary PH.
- (2)
- the PCWP remains ≤18 mmHg with nitroprusside infusion and passive leg raise.
2. Study Design
2.1. Right Heart Catheterization and Nitroprusside Protocol
2.2. Statistical Analysis
3. Results
3.1. Baseline Demographic Data and Clinical Characteristics Are Summarized in Table 1
3.2. Baseline Hemodynamics
3.3. Hemodynamic Response with Nitroprusside
3.4. Hemodynamic Response to Nitroprusside and Leg Raise
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2022, 43, 3618–3731. [Google Scholar] [CrossRef] [PubMed]
- Naeije, R.; Gerges, M.; Vachiery, J.L.; Caravita, S.; Gerges, C.; Lang, I.M. Hemodynamic Phenotyping of Pulmonary Hypertension in Left Heart Failure. Circ. Heart Fail. 2017, 10, e004082. [Google Scholar] [CrossRef] [PubMed]
- Thenappan, T.; Ormiston, M.L.; Ryan, J.J.; Archer, S.L. Pulmonary arterial hypertension: Pathogenesis and clinical management. BMJ 2018, 360, j5492. [Google Scholar] [CrossRef] [PubMed]
- Naeije, R.; D’Alto, M. The Diagnostic Challenge of Group 2 Pulmonary Hypertension. Prog. Cardiovasc. Dis. 2016, 59, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Guazzi, M.; Borlaug, B.A. Pulmonary hypertension due to left heart disease. Circulation 2012, 126, 975–990. [Google Scholar] [CrossRef] [PubMed]
- Guazzi, M.; Galie, N. Pulmonary hypertension in left heart disease. Eur. Respir. Rev. 2012, 21, 338–346. [Google Scholar] [CrossRef]
- Andersen, M.J.; Olson, T.P.; Melenovsky, V.; Kane, G.C.; Borlaug, B.A. Differential hemodynamic effects of exercise and volume expansion in people with and without heart failure. Circ. Heart Fail. 2015, 8, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Borlaug, B.A. Invasive assessment of pulmonary hypertension: Time for a more fluid approach? Circ. Heart Fail. 2014, 7, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Borlaug, B.A.; Nishimura, R.A.; Sorajja, P.; Lam, C.S.; Redfield, M.M. Exercise hemodynamics enhance diagnosis of early heart failure with preserved ejection fraction. Circ. Heart Fail. 2010, 3, 588–595. [Google Scholar] [CrossRef]
- D’Alto, M.; Romeo, E.; Argiento, P.; Motoji, Y.; Correra, A.; Di Marco, G.M.; Iacono, A.M.; Barracano, R.; D’Andrea, A.; Rea, G.; et al. Clinical Relevance of Fluid Challenge in Patients Evaluated for Pulmonary Hypertension. Chest 2017, 151, 119–126. [Google Scholar] [CrossRef]
- Fujimoto, N.; Borlaug, B.A.; Lewis, G.D.; Hastings, J.L.; Shafer, K.M.; Bhella, P.S.; Carrick-Ranson, G.; Levine, B.D. Hemodynamic responses to rapid saline loading: The impact of age, sex, and heart failure. Circulation 2013, 127, 55–62. [Google Scholar] [CrossRef]
- Herve, P.; Lau, E.M.; Sitbon, O.; Savale, L.; Montani, D.; Godinas, L.; Lador, F.; Jais, X.; Parent, F.; Gunther, S.; et al. Criteria for diagnosis of exercise pulmonary hypertension. Eur. Respir. J. 2015, 46, 728–737. [Google Scholar] [CrossRef]
- Lewis, G.D.; Bossone, E.; Naeije, R.; Grunig, E.; Saggar, R.; Lancellotti, P.; Ghio, S.; Varga, J.; Rajagopalan, S.; Oudiz, R.; et al. Pulmonary vascular hemodynamic response to exercise in cardiopulmonary diseases. Circulation 2013, 128, 1470–1479. [Google Scholar] [CrossRef]
- Naeije, R.; Vanderpool, R.; Dhakal, B.P.; Saggar, R.; Saggar, R.; Vachiery, J.L.; Lewis, G.D. Exercise-induced pulmonary hypertension: Physiological basis and methodological concerns. Am. J. Respir. Crit. Care Med. 2013, 187, 576–583. [Google Scholar] [CrossRef]
- Lim, H.S.; Zaphiriou, A. Sodium Nitroprusside in Patients With Mixed Pulmonary Hypertension and Left Heart Disease: Hemodynamic Predictors of Response and Prognostic Implications. J. Card. Fail. 2016, 22, 117–124. [Google Scholar] [CrossRef]
- Pagano, D.; Townend, J.N.; Horton, R.; Smith, C.; Clutton-Brock, T.; Bonser, R.S. A comparison of inhaled nitric oxide with intravenous vasodilators in the assessment of pulmonary haemodynamics prior to cardiac transplantation. Eur. J. Cardiothorac. Surg. 1996, 10, 1120–1126. [Google Scholar] [CrossRef][Green Version]
- Guglin, M.; Mehra, S.; Mason, T.J. Comparison of drugs for pulmonary hypertension reversibility testing: A meta-analysis. Pulm. Circ. 2013, 3, 406–413. [Google Scholar] [CrossRef]
- Cockrill, B.A.; Kacmarek, R.M.; Fifer, M.A.; Bigatello, L.M.; Ginns, L.C.; Zapol, W.M.; Semigran, M.J. Comparison of the effects of nitric oxide, nitroprusside, and nifedipine on hemodynamics and right ventricular contractility in patients with chronic pulmonary hypertension. Chest 2001, 119, 128–136. [Google Scholar] [CrossRef]
- Schwartzenberg, S.; Redfield, M.M.; From, A.M.; Sorajja, P.; Nishimura, R.A.; Borlaug, B.A. Effects of vasodilation in heart failure with preserved or reduced ejection fraction implications of distinct pathophysiologies on response to therapy. J. Am. Coll. Cardiol. 2012, 59, 442–451. [Google Scholar] [CrossRef] [PubMed]
- Kozitza, C.J.; Dharmavaram, N.; Tao, R.; Tabima, D.M.; Chesler, N.C.; Raza, F. Pulmonary vascular distensibility with passive leg raise is comparable to exercise and predictive of clinical outcomes in pulmonary hypertension. Pulm. Circ. 2022, 12, e12029. [Google Scholar] [CrossRef] [PubMed]
- van de Bovenkamp, A.A.; Wijkstra, N.; Oosterveer, F.P.T.; Vonk Noordegraaf, A.; Bogaard, H.J.; van Rossum, A.C.; de Man, F.S.; Borlaug, B.A.; Handoko, M.L. The Value of Passive Leg Raise During Right Heart Catheterization in Diagnosing Heart Failure with Preserved Ejection Fraction. Circ. Heart Fail. 2022, 15, e008935. [Google Scholar] [CrossRef] [PubMed]
- Arunachalam, A.; Chaisson, N.F.; Tonelli, A.R. Methods to improve the yield of right heart catheterization in pulmonary hypertension. Respir. Med. X 2020, 2, 100015. [Google Scholar] [CrossRef]
- Benza, R.L.; Kanwar, M.K.; Raina, A.; Scott, J.V.; Zhao, C.L.; Selej, M.; Elliott, C.G.; Farber, H.W. Development and Validation of an Abridged Version of the REVEAL 2.0 Risk Score Calculator, REVEAL Lite 2, for Use in Patients With Pulmonary Arterial Hypertension. Chest 2021, 159, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Carroll, J.D.; Lang, R.M.; Neumann, A.L.; Borow, K.M.; Rajfer, S.I. The differential effects of positive inotropic and vasodilator therapy on diastolic properties in patients with congestive cardiomyopathy. Circulation 1986, 74, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Cohn, J.N.; Franciosa, J.A. Vasodilator therapy of cardiac failure: (first of two parts). N. Engl. J. Med. 1977, 297, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Penicka, M.; Bartunek, J.; Trakalova, H.; Hrabakova, H.; Maruskova, M.; Karasek, J.; Kocka, V. Heart failure with preserved ejection fraction in outpatients with unexplained dyspnea: A pressure-volume loop analysis. J. Am. Coll. Cardiol. 2010, 55, 1701–1710. [Google Scholar] [CrossRef] [PubMed]
- Borlaug, B.A.; Reddy, Y.N.V. The Role of the Pericardium in Heart Failure: Implications for Pathophysiology and Treatment. JACC Heart Fail. 2019, 7, 574–585. [Google Scholar] [CrossRef] [PubMed]
- Tyberg, J.V.; Taichman, G.C.; Smith, E.R.; Douglas, N.W.; Smiseth, O.A.; Keon, W.J. The relationship between pericardial pressure and right atrial pressure: An intraoperative study. Circulation 1986, 73, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Tedford, R.J.; Hassoun, P.M.; Mathai, S.C.; Girgis, R.E.; Russell, S.D.; Thiemann, D.R.; Cingolani, O.H.; Mudd, J.O.; Borlaug, B.A.; Redfield, M.M.; et al. Pulmonary capillary wedge pressure augments right ventricular pulsatile loading. Circulation 2012, 125, 289–297. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | PHPVD | PHLHD | p Value |
|---|---|---|---|
| Total Number of Patients | n = 14 | n = 10 | |
| Female | 10 (73.00%) | 5 (50.00%) | 0.2038 |
| Age (Years) | 75 (56–89) | 74 (51–88) | 0.8739 |
| Nitroprusside Dose (mcg/kg/min) | 0.84 ± 0.42 | 1.22 ± 0.40 | 0.0126 |
| Comorbidities | |||
| HFpEF | 9 (64.20%) | 9 (90.00%) | 0.3408 |
| BMI (kg/m2) | 29 (17.77–45.21) | 33 (21.45–60.45) | 0.4031 |
| CAD | 7 (50.00%) | 4 (40.00%) | 0.6968 |
| HTN | 11 (78.60%) | 10 (100.00%) | 0.2391 |
| DM II | 7 (50.00%) | 4 (40.00%) | 0.6968 |
| Atrial fibrillation/Flutter | 6 (42.90%) | 7 (70.00%) | 0.2397 |
| Lung Disease (COPD/ILD) | 8 (57.10%) | 4 (40.00%) | 0.6802 |
| OSA | 6 (42.90%) | 5 (50.00%) | 0.9999 |
| CKD | 7 (50.00%) | 1(10.00%) | 0.0791 |
| Autoimmune diseases | 3 (21.40%) | 0 (0%) | 0.2391 |
| PH Etiology | |||
| Non-PAH † | 2 | ||
| PAH | |||
| Idiopathic-PAH | 2 | ||
| ILD-PAH | 2 | ||
| CTD-PAH | 2 | ||
| Toxin-PAH | 1 | ||
| Medications | |||
| ARNi/ACEi/ARB | 9 (64.20%) | 8 (80.00%) | 0.6529 |
| MRA | 10 (71.40%) | 9 (90.00%) | 0.3577 |
| SGLT2i | 2 (14.20%) | 7 (70.00%) | 0.0104 |
| PDE5 inhibitor only | 2 (14.20%) | 1 (10.00%) | >0.9999 |
| Echocardiographic Parameters | |||
| Mean ± STDev | Mean ± STDev | p Value | |
| LVEF | 63.46 ± 8.02 | 59.4 ± 5.91 | 0.1902 |
| LAVi | 37.04 ± 11.12 | 48.88 ± 31.86 | 0.4833 |
| Diastolic Dysfunction (Grade I–III) | 9 (64.20%) | 8 (80.00%) | 0.66 |
| IVS Systolic Septal flattening | 9 (69.23%) | 7 (70.00%) | >0.9999 |
| RVEDd (cm)—basal width | 4.03 ± 0.52 | 4.7 ± 0.70 | 0.0341 |
| RVOT PW doppler notch | 9 (69.23%) | 10 (100%) | 0.1045 |
| RA size (RAVi) | 30.60 ± 10.74 | 50.91 ± 21.56 | 0.0147 |
| PASP | 57.41 ± 16.52 | 62.77 ±17.18 | 0.354 |
| TAPSE | 1.98 ± 0.62 | 1.33 ± 0.51 | 0.031 |
| RV S′ | 12.28 ± 2.89 | 8.97 ± 2.30 | 0.0054 |
| Resting | PHPVD | PHLHD | p-Value a |
|---|---|---|---|
| Mean ± STDev | Mean ± STDev | ||
| RAP (mmHg) | 9.35 † ± 3.56 | 17.6 ‡ ± 5.02 | 0.0002 |
| PASP (mmHg) | 64.00 † ± 16.71 | 84.9 ‡ ± 16.00 | 0.0044 |
| PADP (mmHg) | 25.00 † ± 5.87 | 38.3 ‡ ± 13.90 | 0.0006 |
| mPAP (mmHg) | 38.00 † ± 8.50 | 53.83 ‡± 13.70 | 0.0004 |
| PCWP (mmHg) | 17.92 † ± 4.57 | 25.6 ‡ ± 5.27 | 0.0009 |
| DPG (mmHg) | 7.07 ± 4.50 | 12.7 ± 13.22 | 0.5345 |
| TPG (mmHg) | 20.07 ± 7.96 | 28.23 ‡ ± 12.32 | 0.0865 |
| PVR (WU) | 5.33 † ± 2.62 | 7.71 ‡ ± 5.03 | 0.3784 |
| SVR (mmHg⋅min⋅mL−1) | 1990.61 † ± 332.13 | 1633.62 ‡ ± 647.98 | 0.4279 |
| CO (L/min) | 4.02 ± 1.04 | 4.24 ‡ ± 1.35 | 0.5938 |
| CI (L/min/m2) | 2.08 ± 0.56 | 2.11 ‡ ± 0.56 | 0.8894 |
| SV (mL) | 59.39 ± 12.29 | 59.66 ‡ ± 21.65 | 0.7638 |
| SVi (mL/m2) | 30.93 ± 7.55 | 30.18 ‡ ± 11.44 | 0.5458 |
| HR (bpm) | 67.71 † ± 9.11 | 72.6 ± 12.05 | 0.5159 |
| MAP (mmHg) | 106.35 † ± 12.72 | 104.10 ‡ ± 12.30 | 0.6555 |
| PAPi | 4.65 ± 1.94 | 2.78 ± 0.79 | 0.0093 |
| RAP:PCWP | 0.54 ± 0.27 | 0.69 ‡ ± 0.18 | 0.0356 |
| LVTMFP | 8.57 † ± 5.40 | 8.00 ± 5.10 | 0.6548 |
| Parameter Δ | PHPVD | PHLHD | p-Value a |
|---|---|---|---|
| Mean ± STDev | Mean ± STDev | ||
| ΔRAP (mmHg) | −2.77 ± 1.36 | −5.80 ± 2.86 | 0.0092 |
| ΔPASP (mmHg) | −16.14 ± 10.68 | −21.90 ± 11.29 | 0.1847 |
| ΔPADP (mmHg) | −5.86 ± 4.45 | −11.70 ± 12.82 | 0.2387 |
| ΔmPAP (mmHg) | −9.29 ± 5.96 | −15.10 ± 11.19 | 0.2407 |
| ΔPCWP (mmHg) | −6.29 ± 4.25 | −5.10 ± 2.42 | 0.4254 |
| ΔDPG (mmHg) | 0.43 ± 4.78 | −6.60 ± 11.47 | 0.0614 |
| ΔTPG (mmHg) | −3.00 ± 5.67 | −10.00 ± 9.68 | 0.0433 |
| ΔPVR (WU) | −1.08 ± 1.61 | −3.57 ± 3.52 | 0.0417 |
| ΔSVR (mmHg⋅min⋅mL−1) | −578.43 ± 275.17 | −629.59 ± 333.42 | 0.8315 |
| ΔCO (L/min) | 0.22 ± 0.71 | 0.55 ± 0.35 | 0.0468 |
| ΔCI (L/min/m2) | 0.17 ± 0.32 | 0.28 ± 0.16 | 0.0928 |
| ΔSV (mL) | −1.83 ± 8.79 | 6.77 ± 5.88 | 0.0178 |
| ΔSVi (mL/m2) | −0.33 ± 3.54 | 3.57 ± 2.95 | 0.0084 |
| ΔHR (bpm) | 5.07 ± 4.67 | 0.90 ± 5.24 | 0.0742 |
| ΔMAP (mmHg) | −30.07 ± 12.07 | −28.1 ± 13.26 | 0.8068 |
| ΔPAPi | 0.18 ± 1.24 | 1.04 ± 1.83 | 0.7961 |
| ΔRAP:PCWP | 0.02 ± 0.20 | −0.12 ± 0.15 | 0.7961 |
| ΔLVTMFP | −3.57 ± 4.67 | 0.70 ± 3.74 | 0.0454 |
| PHPVD Patient | Etiology | Medication | Δ6MWD (m) | ΔWHO FC | ΔNT-proBNP (% Change from Baseline) | ΔREVEAL Lite 2.0 Risk Score a | REVEAL Lite 2.0 Risk Status b |
|---|---|---|---|---|---|---|---|
| Patient 1 | ILD | Sildenafil 40 mg PO q8hrs +INH Treprostinil 64 mcg INH QID | +209 | −1 | −72% | −5 | Intermediate |
| Patient 2 | ILD | Sildenafil 60 mg PO q8hrs c | +145 | −1 | −68% | −5 | Intermediate |
| Patient 3 | Toxin | Sildenafil 20 mg PO q8hrs c | +130 | −1 | −45% | −4 | High |
| Patient 4 | Idiopathic | Sildenafil 60 mg q8hr | +244 | −1 | −36% | −5 | Low |
| Patient 5 | Idiopathic | Sildenafil 20 mg PO q8hrs | +85 | −1 | −84% | −5 | Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naguib, M.; Aljwaid, A.; Marella, D.; Flores, R.J.; Singh, A. Nitroprusside Combined with Leg Raise at the Time of Right Heart Catheterization to Differentiate Precapillary from Other Hemodynamic Forms of Pulmonary Hypertension: A Single-Center Pilot Study. J. Cardiovasc. Dev. Dis. 2024, 11, 124. https://doi.org/10.3390/jcdd11040124
Naguib M, Aljwaid A, Marella D, Flores RJ, Singh A. Nitroprusside Combined with Leg Raise at the Time of Right Heart Catheterization to Differentiate Precapillary from Other Hemodynamic Forms of Pulmonary Hypertension: A Single-Center Pilot Study. Journal of Cardiovascular Development and Disease. 2024; 11(4):124. https://doi.org/10.3390/jcdd11040124
Chicago/Turabian StyleNaguib, Mostafa, Ahmed Aljwaid, Dean Marella, Raul J. Flores, and Abhishek Singh. 2024. "Nitroprusside Combined with Leg Raise at the Time of Right Heart Catheterization to Differentiate Precapillary from Other Hemodynamic Forms of Pulmonary Hypertension: A Single-Center Pilot Study" Journal of Cardiovascular Development and Disease 11, no. 4: 124. https://doi.org/10.3390/jcdd11040124
APA StyleNaguib, M., Aljwaid, A., Marella, D., Flores, R. J., & Singh, A. (2024). Nitroprusside Combined with Leg Raise at the Time of Right Heart Catheterization to Differentiate Precapillary from Other Hemodynamic Forms of Pulmonary Hypertension: A Single-Center Pilot Study. Journal of Cardiovascular Development and Disease, 11(4), 124. https://doi.org/10.3390/jcdd11040124