
Catheter-Based Fetal Cardiac Interventions

Abstract
:1. Introduction
2. Fetal Aortic Valvuloplasty for Severe Aortic Valve Stenosis (FAV)
2.1. Patient Selection
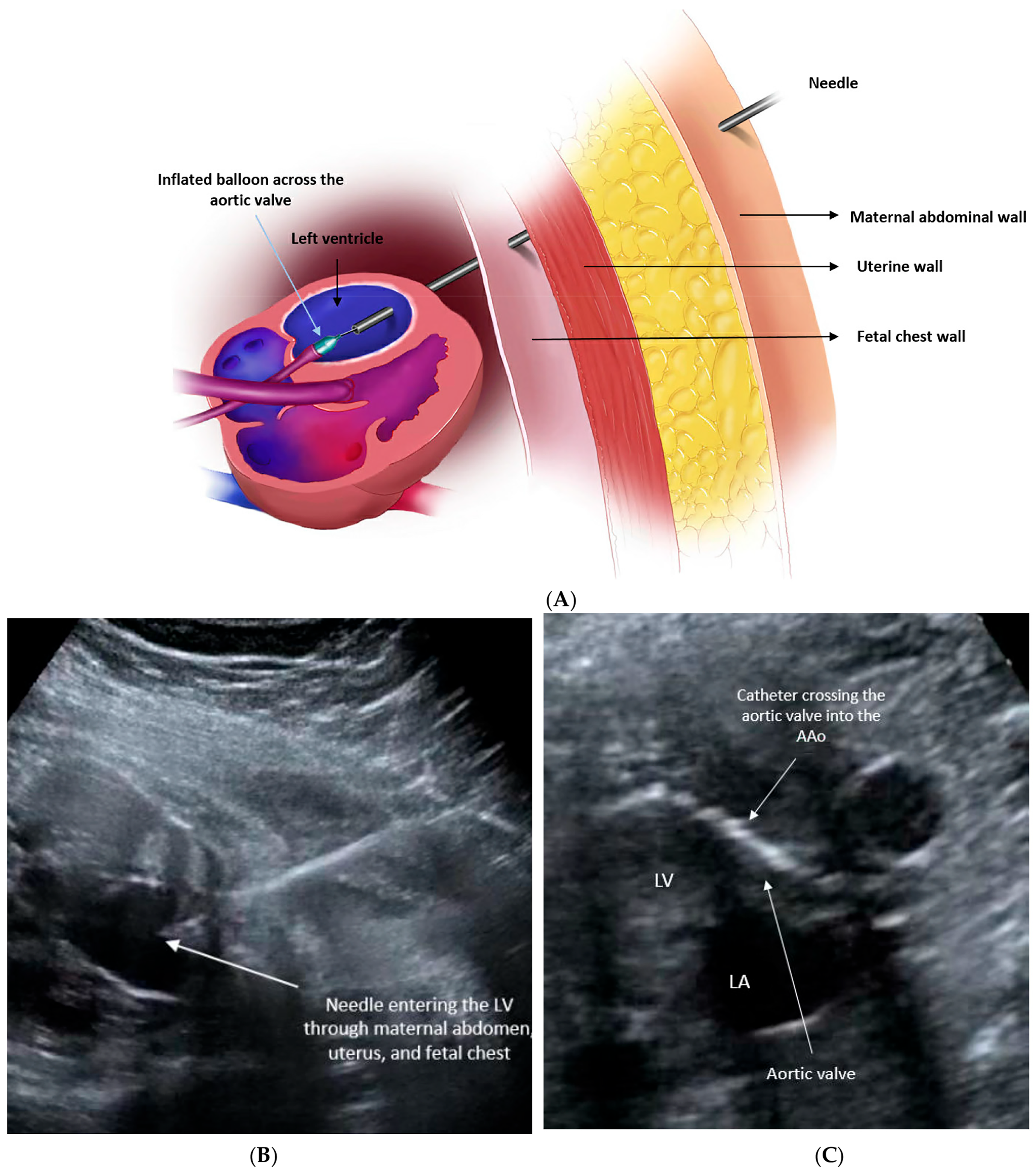
2.2. Procedural Technique
2.3. Procedural Outcomes
2.4. Post-Procedural Outcomes
2.5. Postnatal Outcomes
3. Atrial Septal Intervention for Hypoplastic Left Heart Syndrome (Hlhs) with Highly Restrictive or Intact Atrial Septum (R/Ias)
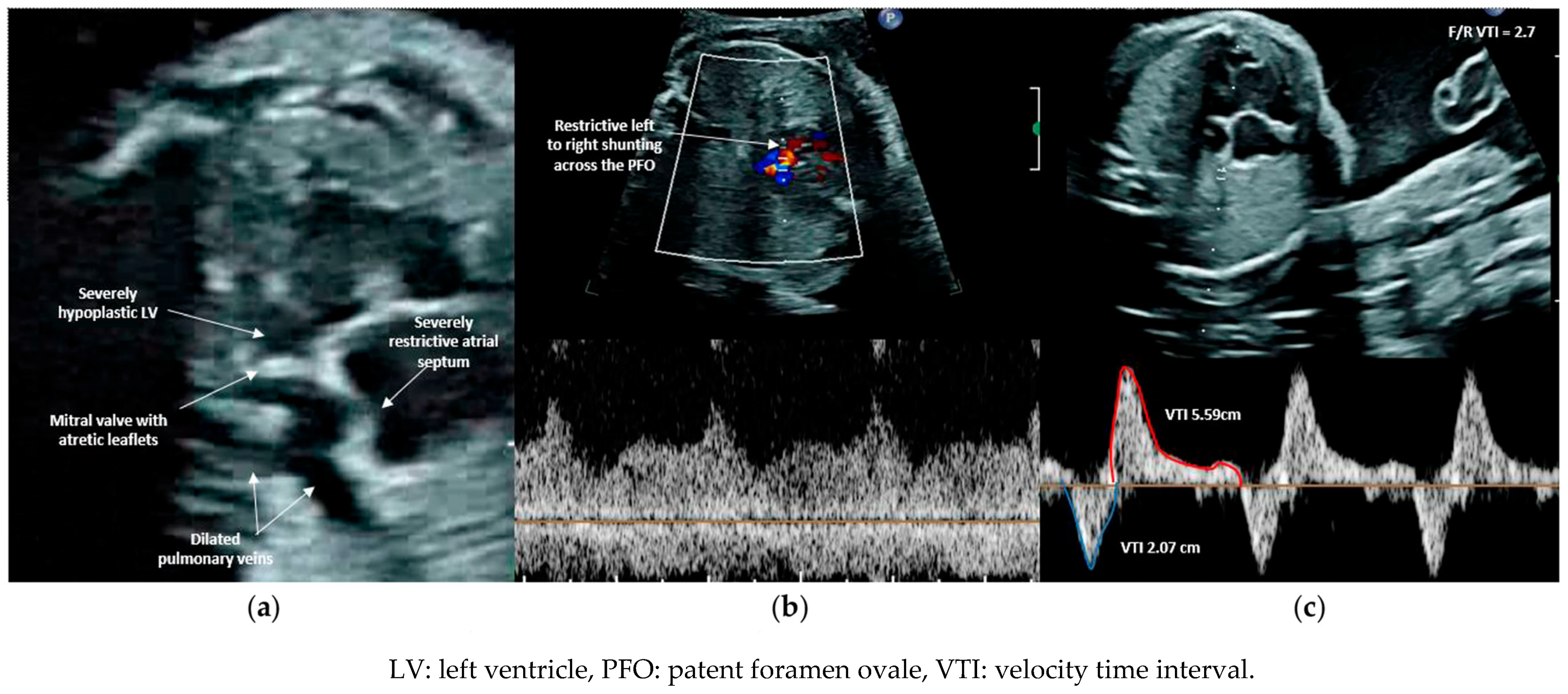
3.1. Patient Selection
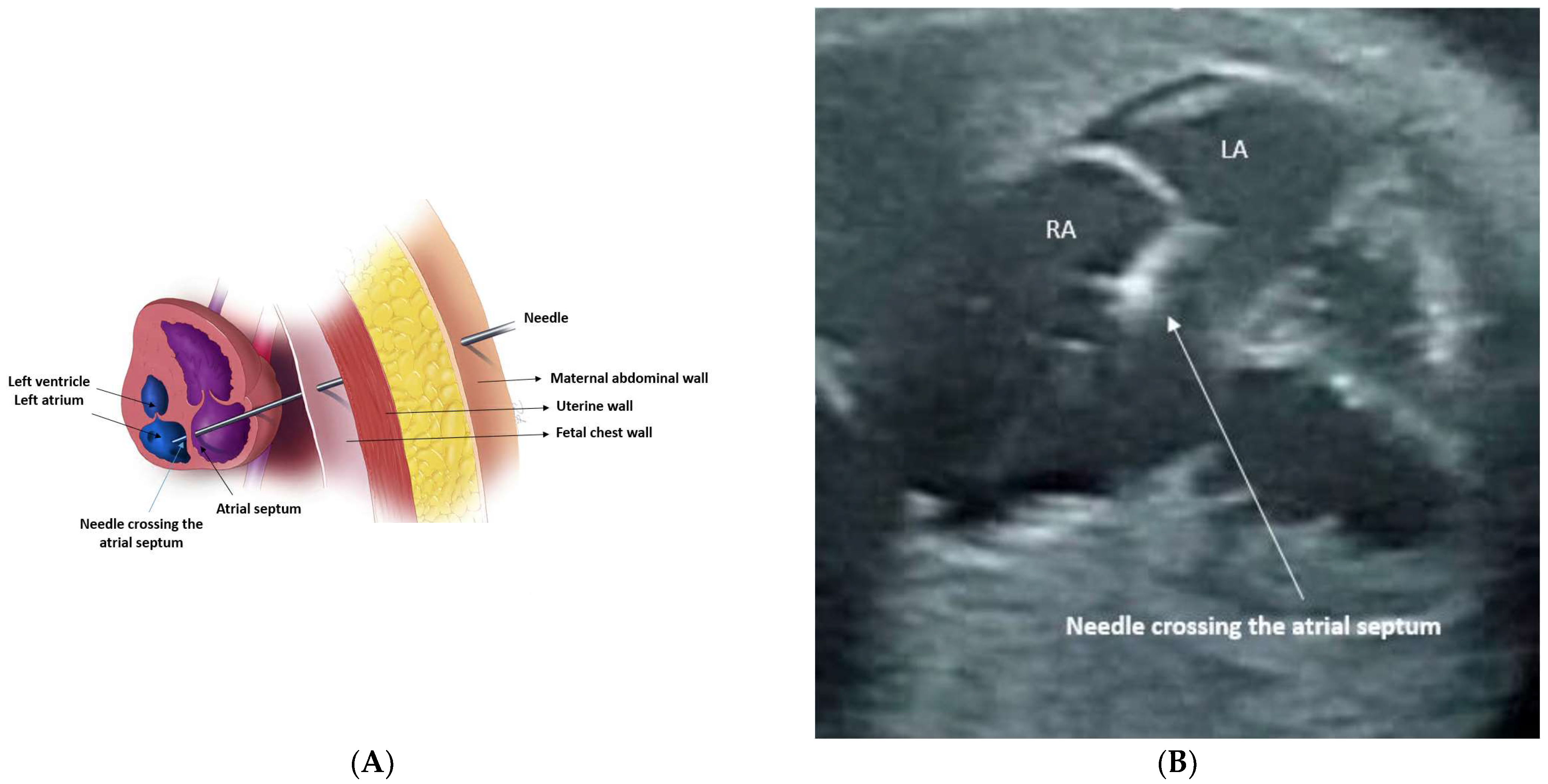
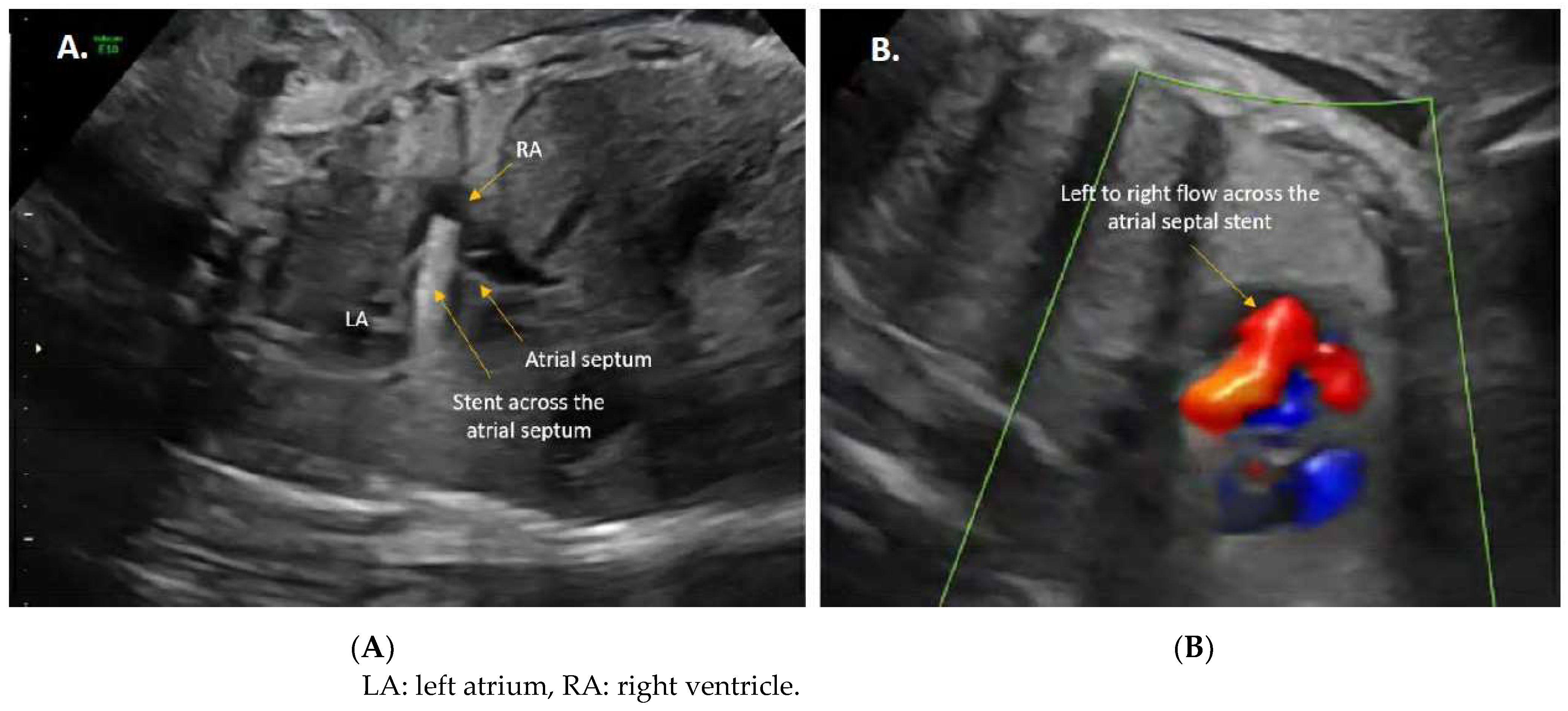
3.2. Procedural Technique
3.3. Procedural Outcomes
3.4. Postnatal Outcomes
4. Pulmonary Valvuloplasty for Pulmonary Atresia or Severe Pulmonary Stenosis with Intact Ventricular Septum (Pa/Ivs)
4.1. Patient Selection
4.2. Procedural Technique
4.3. Procedural Outcomes
4.4. Postnatal Outcomes
5. Discussion Regarding Maternal Risks
6. Conclusions
7. Future Directions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McElhinney, D.B.; Tworetzky, W.; Lock, J.E. Current Status of Fetal Cardiac Intervention. Circulation 2010, 121, 1256–1263. [Google Scholar] [CrossRef] [PubMed]
- Tulzer, A.; Arzt, W.; Scharnreitner, I.; Hochpoechler, J.; Bauer, C.; Tulzer, G. Complications Associated with Fetal Cardiac Interventions: Prevalence and Management—Experience from 213 Procedures. Fetal Diagn. Ther. 2023, 49, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Friedman, K.G.; Tworetzky, W. Fetal cardiac interventions: Where do we stand? Arch. Cardiovasc. Dis. 2020, 113, 121–128. [Google Scholar] [CrossRef]
- Maxwell, D.; Allan, L.; Tynan, M.J. Balloon dilatation of the aortic valve in the fetus: A report of two cases. Br. Heart J. 1991, 65, 256. [Google Scholar] [CrossRef]
- Rebizant, B.; Koleśnik, A.; Grzyb, A.; Chaberek, K.; Sękowska, A.; Witwicki, J.; Szymkiewicz-Dangel, J.; Dębska, M. Fetal Cardiac Interventions—Are They Safe for the Mothers? J. Clin. Med. 2021, 10, 851. [Google Scholar] [CrossRef]
- Zhou, K.; Hua, Y.; Zhu, Q.; Liu, H.; Yang, S.; Zhou, R.; Guo, N. Transplacental digoxin therapy for fetal tachyarrhythmia with multiple evaluation systems. J. Matern.-Fetal Neonatal Med. 2011, 24, 1378–1383. [Google Scholar] [CrossRef]
- Donofrio, M.T.; Moon-Grady, A.J.; Hornberger, L.K.; Copel, J.A.; Sklansky, M.S.; Abuhamad, A.; Cuneo, B.F.; Huhta, J.C.; Jonas, R.A.; Krishnan, A.; et al. Diagnosis and Treatment of Fetal Cardiac Disease. Circulation 2014, 129, 2183–2242. [Google Scholar] [CrossRef]
- Moon-Grady, A.J.; Donofrio, M.T.; Gelehrter, S.; Hornberger, L.; Kreeger, J.; Lee, W.; Michelfelder, E.; Morris, S.A.; Peyvandi, S.; Pinto, N.M.; et al. Guidelines and Recommendations for Performance of the Fetal Echocardiogram: An Update from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2023, 36, 679–723. [Google Scholar] [CrossRef]
- Freud, L.R.; Wilkins-Haug, L.E.; Beroukhim, R.S.; LaFranchi, T.; Phoon, C.K.; Glickstein, J.S.; Cumbermack, K.M.; Makhoul, M.; Morris, S.A.; Sun, H.Y.; et al. Effect of in Utero Non-Steroidal Anti-Inflammatory Drug Therapy for Severe Ebstein Anomaly or Tricuspid Valve Dysplasia (NSAID Therapy for Fetal Ebstein anomaly). Am. J. Cardiol. 2021, 141, 106–112. [Google Scholar] [CrossRef]
- Peña, F.L.; Emanuelson, T.W.; Todman, S.H.; Jones, R.C.; Mahajan, S. Fetal circular shunt in Ebstein’s anomaly and non-steroidal anti-inflammatory treatment. J. Neonatal-Perinat. Med. 2024, 17, 63–69. [Google Scholar] [CrossRef]
- Lara, D.A.; Morris, S.A.; Maskatia, S.A.; Challman, M.; Nguyen, M.; Feagin, D.K.; Schoppe, L.; Zhang, J.; Bhatt, A.; Sexson-Tejtel, S.K.; et al. Pilot study of chronic maternal hyperoxygenation and effect on aortic and mitral valve annular dimensions in fetuses with left heart hypoplasia. Ultrasound Obstet. Gynecol. 2016, 48, 365–372. [Google Scholar] [CrossRef]
- Edwards, L.A.; Lara, D.A.; Cortes, M.S.; Hunter, J.V.; Andreas, S.; Nguyen, M.J.; Schoppe, L.J.; Zhang, J.; Smith, E.M.; Maskatia, S.A.; et al. Chronic Maternal Hyperoxygenation and Effect on Cerebral and Placental Vasoregulation and Neurodevelopment in Fetuses with Left Heart Hypoplasia. Fetal Diagn. Ther. 2019, 46, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Nassr, A.A.; Shazly, S.A.; Morris, S.A.; Ayres, N.; Espinoza, J.; Erfani, H.; Olutoye, O.A.; Sexson, S.K.; Olutoye, O.O.; Fraser, C.D.; et al. Prenatal management of fetal intrapericardial teratoma: A systematic review. Prenat. Diagn. 2017, 37, 849–863. [Google Scholar] [CrossRef]
- Rychik, J.; Khalek, N.; Gaynor, J.W.; Johnson, M.P.; Adzick, N.S.; Flake, A.W.; Hedrick, H.L. Fetal intrapericardial teratoma: Natural history and management including successful in utero surgery. Am. J. Obstet. Gynecol. 2016, 215, 780.e1–780.e7. [Google Scholar] [CrossRef]
- Gardiner, H.M. Progression of fetal heart disease and rationale for fetal intracardiac interventions. Semin. Fetal Neonatal Med. 2005, 10, 578–585. [Google Scholar] [CrossRef]
- Simonini, C.; Strizek, B.; Berg, C.; Gembruch, U.; Mueller, A.; Heydweiller, A.; Geipel, A. Fetal teratomas—A retrospective observational single-center study. Prenat. Diagn. 2021, 41, 301–307. [Google Scholar] [CrossRef]
- Relan, J.; Swami, M.; Rana, A.; Chaudhary, P.; Ojha, V.; Devarapalli, S.; Dadhwal, V.; Verma, A.; Jagia, P.; Saxena, A. Prenatal Pericardiocentesis and Postnatal Sirolimus for a Giant Inoperable Cardiac Rhabdomyoma. JACC Case Rep. 2021, 3, 1473–1479. [Google Scholar] [CrossRef]
- Schoeneberg, L.A.; Zakaria, D.; Bolin, E.H.; Eble, B.K.; Miquel-Verges, F.; Sandlin, A.T.; Bornemeier, R.A. A Fetal Presentation of a Ruptured Right Ventricular Diverticulum. Pediatr. Cardiol. 2021, 42, 978–980. [Google Scholar] [CrossRef]
- Harrison, M.R.; Golbus, M.S.; Filly, R.A.; Nakayama, D.K.; Lorimier, A.A.D. Fetal Surgical Treatment. Pediatr. Ann. 1982, 11, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Farmer, D.L. Fetal surgery: A brief review. Pediatr. Radiol. 1998, 28, 409–413. [Google Scholar] [CrossRef]
- Hosie, S.; Wollmann, C.; Neff, W.; Holland-Cunz, S. Fetale Chirurgie. Chirurg 2005, 76, 757–764. [Google Scholar] [CrossRef]
- Deprest, J.A.; Flake, A.W.; Gratacos, E.; Ville, Y.; Hecher, K.; Nicolaides, K.; Johnson, M.P.; Luks, F.I.; Adzick, N.S.; Harrison, M.R. The making of fetal surgery. Prenat. Diagn. 2010, 30, 653–667. [Google Scholar] [CrossRef]
- Turley, K.; Vlahakes, G.J.; Harrison, M.R.; Messina, L.; Hanley, F.; Uhlig, P.N.; Ebert, P.A. Intrauterine Cardiothoracic Surgery: The Fetal Lamb Model. Ann. Thorac. Surg. 1982, 34, 422–426. [Google Scholar] [CrossRef]
- Bradley, S.M.; Hanley, F.L.; Duncan, B.W.; Jennings, R.W.; Jester, J.A.; Harrison, M.R.; Verrier, E.D. Fetal cardiac bypass alters regional blood flows, arterial blood gases, and hemodynamics in sheep. Am. J. Physiol.-Heart Circ. Physiol. 1992, 263, H919–H928. [Google Scholar] [CrossRef]
- Eibschitz, I.; Abinader, E.G.; Klein, A.; Sharf, M. Intrauterine diagnosis and control of fetal ventricular arrhythmia during labor. Am. J. Obstet. Gynecol. 1975, 122, 597–600. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, R.J.; Strasburger, J.F.; Garson, A.; Smith, R.T.; Deter, R.L.; Engelhardt, H.T. Fetal ventricular pacing for hydrops secondary to complete atrioventricular block. J. Am. Coll. Cardiol. 1986, 8, 1434–1436. [Google Scholar] [CrossRef]
- Moon-Grady, A.J.; Morris, S.A.; Belfort, M.; Chmait, R.; Dangel, J.; Devlieger, R.; Emery, S.; Frommelt, M.; Galindo, A.; Gelehrter, S.; et al. International Fetal Cardiac Intervention Registry A Worldwide Collaborative Description and Preliminary Outcomes. J. Am. Coll. Cardiol. 2015, 66, 388–399. [Google Scholar] [CrossRef]
- Edwards, A.; Menahem, S.; Veldman, A.; Schranz, D.; Chan, Y.; Nitsos, I.; Wong, F. Fetal cardiac catheterization using a percutaneous transhepatic access technique: Preliminary experience in a lamb model. Ultrasound Obstet. Gynecol. 2013, 42, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Edwards, A.; Veldman, A.; Nitsos, I.; Chan, Y.; Brew, N.; Teoh, M.; Menahem, S.; Schranz, D.; Wong, F.Y. A percutaneous fetal cardiac catheterization technique for pulmonary valvuloplasty and valvulotomy in a mid-gestation lamb model. Prenat. Diagn. 2015, 35, 74–80. [Google Scholar] [CrossRef]
- Rychik, J.; Szwast, A.; Natarajan, S.; Quartermain, M.; Donaghue, D.D.; Combs, J.; Gaynor, J.W.; Gruber, P.J.; Spray, T.L.; Bebbington, M.; et al. Perinatal and early surgical outcome for the fetus with hypoplastic left heart syndrome: A 5-year single institutional experience. Ultrasound Obstet. Gynecol. 2010, 36, 465–470. [Google Scholar] [CrossRef]
- Oster, M.E.; Knight, J.H.; Suthar, D.; Amin, O.; Kochilas, L.K. Long-Term Outcomes in Single-Ventricle Congenital Heart Disease. Circulation 2018, 138, 2718–2720. [Google Scholar] [CrossRef]
- Allan, L.D.; Sharland, G.; Tynan, M.J. The natural history of the hypoplastic left heart syndrome. Int. J. Cardiol. 1989, 25, 341–343. [Google Scholar] [CrossRef] [PubMed]
- Mäkikallio, K.; McElhinney, D.B.; Levine, J.C.; Marx, G.R.; Colan, S.D.; Marshall, A.C.; Lock, J.E.; Marcus, E.N.; Tworetzky, W. Fetal Aortic Valve Stenosis and the Evolution of Hypoplastic Left Heart Syndrome. Circulation 2006, 113, 1401–1405. [Google Scholar] [CrossRef] [PubMed]
- Venardos, A.; Colquitt, J.; Morris, S.A. Fetal growth of left-sided structures and postnatal surgical outcomes in the “borderline” left heart varies by cardiac phenotype. Ultrasound Obstet. Gynecol. 2022, 59, 642–650. [Google Scholar] [CrossRef] [PubMed]
- Colquitt, J.L.; Loar, R.W.; Bolin, E.H.; Ezon, D.S.; Heinle, J.S.; Morris, S.A. Left heart hypoplasia in the fetus: Echocardiographic predictors of outcome. Prenat. Diagn. 2022, 42, 447–460. [Google Scholar] [CrossRef]
- Hornberger, L.K.; Sanders, S.P.; Rein, A.J.J.T.; Spevak, P.J.; Parness, I.A.; Colan, S.D. Left Heart Obstructive Lesions and Left Ventricular Growth in the Midtrimester Fetus. Circulation 1995, 92, 1531–1538. [Google Scholar] [CrossRef]
- Simpson, J.M.; Sharland, G.K. Natural history and outcome of aortic stenosis diagnosed prenatally. Heart 1997, 77, 205. [Google Scholar] [CrossRef]
- Schidlow, D.; Tworetzky, W.; Wilkins-Haug, L. Percutaneous Fetal Cardiac Interventions for Structural Heart Disease. Am. J. Perinatol. 2014, 31, 629–636. [Google Scholar]
- Danford, D.A.; Cronican, P. Hypoplastic left heart syndrome: Progression of left ventricular dilation and dysfunction to left ventricular hypoplasia in utero. Am. Heart J. 1992, 123, 1712–1713. [Google Scholar] [CrossRef]
- Gardiner, H.M.; Kovacevic, A.; Tulzer, G.; Sarkola, T.; Herberg, U.; Dangel, J.; Öhman, A.; Bartrons, J.; Carvalho, J.S.; Jicinska, H.; et al. Natural history of 107 cases of fetal aortic stenosis from a European multicenter retrospective study. Ultrasound Obstet. Gynecol. 2016, 48, 373–381. [Google Scholar] [CrossRef]
- Tworetzky, W.; Wilkins-Haug, L.; Jennings, R.W.; Velde, M.E.V.D.; Marshall, A.C.; Marx, G.R.; Colan, S.D.; Benson, C.B.; Lock, J.E.; Perry, S.B. Balloon Dilation of Severe Aortic Stenosis in the Fetus. Circulation 2004, 110, 2125–2131. [Google Scholar] [CrossRef] [PubMed]
- Hunter, L.E.; Chubb, H.; Miller, O.; Sharland, G.; Simpson, J.M. Fetal aortic valve stenosis: A critique of case selection criteria for fetal intervention. Prenat. Diagn. 2015, 35, 1176–1181. [Google Scholar] [CrossRef] [PubMed]
- Friedman, K.G.; Sleeper, L.A.; Freud, L.R.; Marshall, A.C.; Godfrey, M.E.; Drogosz, M.; Lafranchi, T.; Benson, C.B.; Wilkins-Haug, L.E.; Tworetzky, W. Improved technical success, postnatal outcome and refined predictors of outcome for fetal aortic valvuloplasty. Ultrasound Obstet. Gynecol. 2018, 52, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Allan, L.D.; Maxwell, D.J.; Carminat, M.; Tynan, M.J. Survival after fetal aortic balloon valvoplasty. Ultrasound Obstet. Gynecol. 1995, 5, 90–91. [Google Scholar] [CrossRef] [PubMed]
- Kohl, T.; Sharland, G.; Allan, L.D.; Gembruch, U.; Chaoui, R.; Lopes, L.M.; Zielinsky, P.; Huhta, J.; Silverman, N.H. World experience of percutaneous ultrasound-guided balloon valvuloplasty in human fetuses with severe aortic valve obstruction. Am. J. Cardiol. 2000, 85, 1230–1233. [Google Scholar] [CrossRef] [PubMed]
- Marshall, A.C.; Tworetzky, W.; Bergersen, L.; McElhinney, D.B.; Benson, C.B.; Jennings, R.W.; Wilkins-Haug, L.E.; Marx, G.R.; Lock, J.E. Aortic valvuloplasty in the fetus: Technical characteristics of successful balloon dilation. J. Pediatr. 2005, 147, 535–539. [Google Scholar] [CrossRef] [PubMed]
- McElhinney, D.B.; Marshall, A.C.; Wilkins-Haug, L.E.; Brown, D.W.; Benson, C.B.; Silva, V.; Marx, G.R.; Mizrahi-Arnaud, A.; Lock, J.E.; Tworetzky, W. Predictors of Technical Success and Postnatal Biventricular Outcome after in Utero Aortic Valvuloplasty for Aortic Stenosis with Evolving Hypoplastic Left Heart Syndrome. Circulation 2009, 120, 1482–1490. [Google Scholar] [CrossRef]
- Freud, L.R.; McElhinney, D.B.; Marshall, A.C.; Marx, G.R.; Friedman, K.G.; Nido, P.J.D.; Emani, S.M.; Lafranchi, T.; Silva, V.; Wilkins-Haug, L.E.; et al. Fetal aortic valvuloplasty for evolving hypoplastic left heart syndrome: Postnatal outcomes of the first 100 patients. Circulation 2014, 130, 638–645. [Google Scholar] [CrossRef]
- Olutoye, O.A.; Morris, S. Fetal Cardiac Intervention [Internet]. In Olutoye, Anesthesia for Maternal-Fetal Surgery: Concepts and Clinical Practice; Olutoyin, A., Ed.; Cambridge University Press: Cambridge, UK, 2021; pp. 103–118. [Google Scholar]
- Patel, N.D.; Nageotte, S.; Ing, F.F.; Armstrong, A.K.; Chmait, R.; Detterich, J.A.; Galindo, A.; Gardiner, H.; Grinenco, S.; Herberg, U.; et al. Procedural, pregnancy, and short-term outcomes after fetal aortic valvuloplasty. Catheter. Cardiovasc. Interv. 2020, 96, 626–632. [Google Scholar] [CrossRef]
- Pickard, S.S.; Wong, J.B.; Bucholz, E.M.; Newburger, J.W.; Tworetzky, W.; Lafranchi, T.; Benson, C.B.; Wilkins-Haug, L.E.; Porras, D.; Callahan, R.; et al. Fetal Aortic Valvuloplasty for Evolving Hypoplastic Left Heart Syndrome: A Decision Analysis. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e006127. [Google Scholar] [CrossRef]
- Prosnitz, A.R.; Drogosz, M.; Marshall, A.C.; Wilkins-Haug, L.E.; Benson, C.B.; Sleeper, L.A.; Tworetzky, W.; Friedman, K.G. Early hemodynamic changes after fetal aortic stenosis valvuloplasty predict biventricular circulation at birth. Prenat. Diagn. 2018, 38, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.W.; Dipilato, A.E.; Chong, E.C.; Lock, J.E.; McElhinney, D.B. Aortic Valve Reinterventions After Balloon Aortic Valvuloplasty for Congenital Aortic Stenosis Intermediate and Late Follow-Up. J. Am. Coll. Cardiol. 2010, 56, 1740–1749. [Google Scholar] [CrossRef] [PubMed]
- Vlahos, A.P.; Lock, J.E.; McElhinney, D.B.; Velde, M.E.V.D. Hypoplastic Left Heart Syndrome with Intact or Highly Restrictive Atrial Septum. Circulation 2004, 109, 2326–2330. [Google Scholar] [CrossRef] [PubMed]
- Schneider, K.; Hahn, E.; Statile, C.; Hirsch, R.; Khoury, P.R.; Cnota, J.; Divanovic, A. Pulmonary venous Doppler patterns and midterm outcomes in fetuses with left-sided obstructive lesions and restrictive atrial septum. Prenat. Diagn. 2020, 40, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Rychik, J.; Rome, J.J.; Collins, M.H.; DeCampli, W.M.; Spray, T.L. The hypoplastic left heart syndrome with intact atrial septum: Atrial morphology, pulmonary vascular histopathology and outcome. J. Am. Coll. Cardiol. 1999, 34, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Glatz, J.A.; Tabbutt, S.; Gaynor, J.W.; Rome, J.J.; Montenegro, L.; Spray, T.L.; Rychik, J. Hypoplastic Left Heart Syndrome with Atrial Level Restriction in the Era of Prenatal Diagnosis. Ann. Thorac. Surg. 2007, 84, 1633–1638. [Google Scholar] [CrossRef] [PubMed]
- Forbess, J.M.; Cook, N.; Roth, S.J.; Serraf, A.; Mayer, J.E.; Jonas, R.A. Ten-Year Institutional Experience with Palliative Surgery for Hypoplastic Left Heart Syndrome: Risk Factors Related to Stage I Mortality. Circulation 1995, 92, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Atz, A.M.; Feinstein, J.A.; Jonas, R.A.; Perry, S.B.; Wessel, D.L. Preoperative management of pulmonary venous hypertension in hypoplastic left heart syndrome with restrictive atrial septal defect. Am. J. Cardiol. 1999, 83, 1224–1228. [Google Scholar] [CrossRef] [PubMed]
- Taketazu, M.; Barrea, C.; Smallhorn, J.F.; Wilson, G.J.; Hornberger, L.K. Intrauterine pulmonary venous flow and restrictive foramen ovale in fetal hypoplastic left heart syndrome. J. Am. Coll. Cardiol. 2004, 43, 1902–1907. [Google Scholar] [CrossRef]
- Jantzen, D.W.; Moon-Grady, A.J.; Morris, S.A.; Armstrong, A.K.; Berg, C.; Dangel, J.; Fifer, C.G.; Frommelt, M.; Gembruch, U.; Herberg, U.; et al. Hypoplastic Left Heart Syndrome with Intact or Restrictive Atrial Septum. Circulation 2017, 136, 1346–1349. [Google Scholar] [CrossRef]
- Serrano, R.M.; Hussain, S.; Brown, B.; Ebenroth, E.S.; Farrell, A. Risk stratification of patients with hypoplastic left heart syndrome and intact atrial septum using fetal MRI and echocardiography. Cardiol. Young 2020, 30, 790–798. [Google Scholar] [CrossRef] [PubMed]
- Tanem, J.; Rudd, N.; Rauscher, J.; Scott, A.; Frommelt, M.A.; Hill, G.D. Survival After Norwood Procedure in High-Risk Patients. Ann. Thorac. Surg. 2020, 109, 828–833. [Google Scholar] [CrossRef]
- Divanović, A.; Hor, K.; Cnota, J.; Hirsch, R.; Kinsel-Ziter, M.; Michelfelder, E. Prediction and perinatal management of severely restrictive atrial septum in fetuses with critical left heart obstruction: Clinical experience using pulmonary venous Doppler analysis. J. Thorac. Cardiovasc. Surg. 2011, 141, 988–994. [Google Scholar] [CrossRef] [PubMed]
- Michelfelder, E.; Gomez, C.; Border, W.; Gottliebson, W.; Franklin, C. Predictive Value of Fetal Pulmonary Venous Flow Patterns in Identifying the Need for Atrial Septoplasty in the Newborn with Hypoplastic Left Ventricle. Circulation 2005, 112, 2974–2979. [Google Scholar] [CrossRef] [PubMed]
- Marshall, A.C.; Velde, M.E.V.D.; Tworetzky, W.; Gomez, C.A.; Wilkins-Haug, L.; Benson, C.B.; Jennings, R.W.; Lock, J.E. Creation of an Atrial Septal Defect in Utero for Fetuses with Hypoplastic Left Heart Syndrome and Intact or Highly Restrictive Atrial Septum. Circulation 2004, 110, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Marshall, A.C.; Levine, J.; Morash, D.; Silva, V.; Lock, J.E.; Benson, C.B.; Wilkins-Haug, L.E.; McElhinney, D.B.; Tworetzky, W. Results of in utero atrial septoplasty in fetuses with hypoplastic left heart syndrome. Prenat. Diagn. 2008, 28, 1023–1028. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, R.R.; Ryan, G.; Seed, M.; Arsdell, G.V.; Jaeggi, E.T. Fetal stenting of the atrial septum: Technique and initial results in cardiac lesions with left atrial hypertension. Int. J. Cardiol. 2013, 168, 2029–2036. [Google Scholar] [CrossRef]
- Kalish, B.T.; Tworetzky, W.; Benson, C.B.; Wilkins-Haug, L.; Mizrahi-Arnaud, A.; McElhinney, D.B.; Lock, J.E.; Marshall, A.C. Technical challenges of atrial septal stent placement in fetuses with hypoplastic left heart syndrome and intact atrial septum. Catheter. Cardiovasc. Interv. 2014, 84, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Pedra, S.R.F.F.; Peralta, C.F.A.; Crema, L.; Jatene, I.B.; Costa, R.N.D.; Pedra, C.A.C. Fetal Interventions for Congenital Heart Disease in Brazil. Pediatr. Cardiol. 2014, 35, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Quintero, R.A.; Huhta, J.; Suh, E.; Chmait, R.; Romero, R.; Angel, J. In utero cardiac fetal surgery: Laser atrial septotomy in the treatment of hypoplastic left heart syndrome with intact atrial septum. Am. J. Obstet. Gynecol. 2005, 193, 1424–1428. [Google Scholar] [CrossRef]
- Szwast, A.; Tian, Z.; McCann, M.; Donaghue, D.; Rychik, J. Vasoreactive Response to Maternal Hyperoxygenation in the Fetus with Hypoplastic Left Heart Syndrome. Circ. Cardiovasc. Imaging 2010, 3, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Enzensberger, C.; Axt-Fliedner, R.; Degenhardt, J.; Kawecki, A.; Tenzer, A.; Kohl, T.; Krapp, M. Pulmonary Vasoreactivity to Materno-Fetal Hyperoxygenation Testing in Fetuses with Hypoplastic Left Heart. Ultraschall Med. 2015, 37, 195–200. [Google Scholar] [CrossRef]
- Schidlow, D.; Donofrio, M. Prenatal Maternal Hyperoxygenation Testing and Implications for Critical Care Delivery Planning among Fetuses with Congenital Heart Disease: Early Experience. Am. J. Perinatol. 2017, 35, 016–023. [Google Scholar]
- Mardy, C.; Kaplinski, M.; Peng, L.; Blumenfeld, Y.J.; Kwiatkowski, D.M.; Tacy, T.A.; Maskatia, S.A. Maternal Hyperoxygenation Testing in Fetuses with Hypoplastic Left-Heart Syndrome: Association with Postnatal Atrial Septal Restriction. Fetal Diagn. Ther. 2021, 48, 678–689. [Google Scholar] [CrossRef]
- Belfort, M.A.; Morris, S.A.; Espinoza, J.; Shamshirsaz, A.A.; Cortes, M.S.; Justino, H.; Ayres, N.A.; Qureshi, A.M. Thulium laser-assisted atrial septal stent placement: First use in fetal hypoplastic left heart syndrome and intact atrial septum. Ultrasound Obstet. Gynecol. 2019, 53, 417–418. [Google Scholar] [CrossRef] [PubMed]
- Iliopoulos, I.; Mastropietro, C.W.; Flores, S.; Cheung, E.; Amula, V.; Radman, M.; Kwiatkowski, D.; Puente, B.N.; Buckley, J.R.; Allen, K.Y.; et al. Pulmonary Atresia with Intact Ventricular Septum: Midterm Outcomes from a Multicenter Cohort. Pediatr. Cardiol. 2024, 45, 847–857. [Google Scholar] [CrossRef]
- Karamlou, T.; McCrindle, B.W.; Blackstone, E.H.; Cai, S.; Jonas, R.A.; Bradley, S.M.; Ashburn, D.A.; Caldarone, C.A.; Williams, W.G. Lesion-specific outcomes in neonates undergoing congenital heart surgery are related predominantly to patient and management factors rather than institution or surgeon experience: A Congenital Heart Surgeons Society Study. J. Thorac. Cardiovasc. Surg. 2010, 139, 569–577.e1. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Tian, Z.; Rychik, J. Prenatal Echocardiographic Predictors of Postnatal Management Strategy in the Fetus with Right Ventricle Hypoplasia and Pulmonary Atresia or Stenosis. Pediatr. Cardiol. 2017, 38, 1562–1568. [Google Scholar] [CrossRef]
- Roman, K.S.; Fouron, J.-C.; Nii, M.; Smallhorn, J.F.; Chaturvedi, R.; Jaeggi, E.T. Determinants of Outcome in Fetal Pulmonary Valve Stenosis or Atresia with Intact Ventricular Septum. Am. J. Cardiol. 2007, 99, 699–703. [Google Scholar] [CrossRef]
- Hasan, B.S.; Bautista-Hernandez, V.; McElhinney, D.B.; Salvin, J.; Laussen, P.C.; Prakash, A.; Geggel, R.L.; Pigula, F.A. Outcomes of transcatheter approach for initial treatment of pulmonary atresia with intact ventricular septum. Catheter. Cardiovasc. Interv. 2013, 81, 111–118. [Google Scholar] [CrossRef]
- Zampi, J.D.; Hirsch-Romano, J.C.; Goldstein, B.H.; Shaya, J.A.; Armstrong, A.K. Hybrid approach for pulmonary atresia with intact ventricular septum: Early single center results and comparison to the standard surgical approach. Catheter. Cardiovasc. Interv. 2014, 83, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Daubeney, P.E.F.; Sharland, G.K.; Cook, A.C.; Keeton, B.R.; Anderson, R.H.; Webber, S.A. Pulmonary Atresia with Intact Ventricular Septum. Circulation 1998, 98, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Spigel, Z.; Qureshi, A.M.; Morris, S.A.; Mery, C.M.; Sexson-Tejtel, S.K.; Zea-Vera, R.; Binsalamah, Z.; Imamura, M.; Heinle, J.; Adachi, I. Right Ventricle Dependent Coronary Circulation: Location of Obstruction is Associated with Survival. Ann. Thorac. Surg. 2020, 109, 1480–1487. [Google Scholar] [CrossRef]
- Todros, T.; Paladini, D.; Chiappa, E.; Russo, M.G.; Gaglioti, P.; Pacileo, G.; Cau, M.A.; Martinelli, P. Pulmonary stenosis and atresia with intact ventricular septum during prenatal life. Ultrasound Obstet. Gynecol. 2003, 21, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Silverman, N.H.; McElhinney, D.B. Which two ventricles cannot be used for a biventricular repair? Echocardiographic assessment. Ann. Thorac. Surg. 1998, 66, 634–640. [Google Scholar] [CrossRef]
- Galindo, A.; Gutiérrez-Larraya, F.; Velasco, J.M.; de la Fuente, P. Pulmonary Balloon Valvuloplasty in a Fetus with Critical Pulmonary Stenosis/Atresia with Intact Ventricular Septum and Heart Failure. Fetal Diagn. Ther. 2005, 21, 100–104. [Google Scholar] [CrossRef]
- Gardiner, H.M.; Belmar, C.; Tulzer, G.; Barlow, A.; Pasquini, L.; Carvalho, J.S.; Daubeney, P.E.F.; Rigby, M.L.; Gordon, F.; Kulinskaya, E.; et al. Morphologic and Functional Predictors of Eventual Circulation in the Fetus with Pulmonary Atresia or Critical Pulmonary Stenosis with Intact Septum. J. Am. Coll. Cardiol. 2008, 51, 1299–1308. [Google Scholar] [CrossRef] [PubMed]
- Salvin, J.W.; McElhinney, D.B.; Colan, S.D.; Gauvreau, K.; Nido, P.J.D.; Jenkins, K.J.; Lock, J.E.; Tworetzky, W. Fetal Tricuspid Valve Size and Growth as Predictors of Outcome in Pulmonary Atresia with Intact Ventricular Septum. Pediatrics 2006, 118, e415–e420. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Wang, H.; Cui, C.; Li, Y.; Liu, Y.; Wang, Y.; Fan, T.; Peng, B. Prenatal echocardiographic classification and prognostic evaluation strategy in fetal pulmonary atresia with intact ventricular septum. Medicine 2019, 98, e17492. [Google Scholar] [CrossRef] [PubMed]
- Montes, E.G.; Herraiz, I.; Mendoza, A.; Galindo, A. Fetal Intervention in Right Outflow Tract Obstructive Disease: Selection of Candidates and Results. Cardiol. Res. Pract. 2012, 2012, 592403. [Google Scholar]
- Tworetzky, W.; McElhinney, D.B.; Marx, G.R.; Benson, C.B.; Brusseau, R.; Morash, D.; Wilkins-Haug, L.E.; Lock, J.E.; Marshall, A.C. In Utero Valvuloplasty for Pulmonary Atresia with Hypoplastic Right Ventricle: Techniques and Outcomes. Pediatrics 2009, 124, e510–e518. [Google Scholar] [CrossRef] [PubMed]
- Tulzer, G.; Arzt, W.; Franklin, R.C.; Loughna, P.V.; Mair, R.; Gardiner, H.M. Fetal pulmonary valvuloplasty for critical pulmonary stenosis or atresia with intact septum. Lancet 2002, 360, 1567–1568. [Google Scholar] [CrossRef]
- Arzt, W.; Tulzer, G.; Aigner, M.; Mair, R.; Hafner, E. Invasive intrauterine treatment of pulmonary atresia/intact ventricular septum with heart failure. Ultrasound Obstet. Gynecol. 2003, 21, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Tulzer, A.; Arzt, W.; Gitter, R.; Prandstetter, C.; Grohmann, E.; Mair, R.; Tulzer, G. Immediate effects and outcome of in-utero pulmonary valvuloplasty in fetuses with pulmonary atresia with intact ventricular septum or critical pulmonary stenosis. Ultrasound Obstet. Gynecol. 2018, 52, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Hogan, W.J.; Grinenco, S.; Armstrong, A.; Devlieger, R.; Dangel, J.; Ferrer, Q.; Frommelt, M.; Galindo, A.; Gardiner, H.; Gelehrter, S.; et al. Fetal Cardiac Intervention for Pulmonary Atresia with Intact Ventricular Septum: International Fetal Cardiac Intervention Registry. Fetal Diagn. Ther. 2020, 47, 731–739. [Google Scholar] [CrossRef]
- Wohlmuth, C.; Tulzer, G.; Arzt, W.; Gitter, R.; Wertaschnigg, D. Maternal aspects of fetal cardiac intervention. Ultrasound Obstet. Gynecol. 2014, 44, 532–537. [Google Scholar] [CrossRef]
- Vorisek, C.N.; Zurakowski, D.; Tamayo, A.; Axt-Fliedner, R.; Siepmann, T.; Friehs, I. Postnatal outcome in patients with aortic stenosis undergoing fetal aortic valvuloplasty: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2022, 59, 576–584. [Google Scholar] [CrossRef]
- Mustafa, H.J.; Aghajani, F.; Jawwad, M.; Shah, N.; Abuhamad, A.; Khalil, A. Fetal cardiac intervention in hypoplastic left heart syndrome with intact or restrictive atrial septum, systematic review, and meta-analysis. Prenat. Diagn. 2023. online ahead of print. [Google Scholar] [CrossRef]
- Cruz-Lemini, M.; Alvarado-Guaman, M.; Nieto-Castro, B.; Luna-Garcia, J.; Martínez-Rodríguez, M.; Juarez-Martínez, I.; Palacios-Macedo, A.; Cruz-Martínez, R. Outcomes of hypoplastic left heart syndrome and fetal aortic valvuloplasty in a country with suboptimal postnatal management. Prenat. Diagn. 2019, 39, 563–570. [Google Scholar] [CrossRef]
- Kovacevic, A.; Öhman, A.; Tulzer, G.; Herberg, U.; Dangel, J.; Carvalho, J.S.; Fesslova, V.; Jicinska, H.; Sarkola, T.; Pedroza, C.; et al. Fetal hemodynamic response to aortic valvuloplasty and postnatal outcome: A European multicenter study. Ultrasound Obstet. Gynecol. 2018, 52, 221–229. [Google Scholar] [CrossRef]
- Galindo, A.; Gómez-Montes, E.; Gómez, O.; Bennasar, M.; Crispi, F.; Herraiz, I.; Mendoza, A.; Escribano, D.; García-Torres, E.; Carretero, J.M.; et al. Fetal Aortic Valvuloplasty: Experience and Results of Two Tertiary Centers in Spain. Fetal Diagn. Ther. 2017, 42, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Wohlmuth, C.; Wertaschnigg, D.; Wieser, I.; Arzt, W.; Tulzer, G. Tissue Doppler imaging in fetuses with aortic stenosis and evolving hypoplastic left heart syndrome before and after fetal aortic valvuloplasty. Ultrasound Obstet. Gynecol. 2016, 47, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Arzt, W.; Wertaschnigg, D.; Veit, I.; Klement, F.; Gitter, R.; Tulzer, G. Intrauterine aortic valvuloplasty in fetuses with critical aortic stenosis: Experience and results of 24 procedures. Ultrasound Obstet. Gynecol. 2011, 37, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Corroenne, R.; Meot, M.; Salomon, L.J.; Szezepanski, I.; Baghdadi, H.; Stos, B.; Levy, M.; Bidois, J.L.; Laux, D.; Gaudin, R.; et al. Fetal aortic valvuloplasty for critical aortic stenosis: Single-center retrospective study focusing on postnatal outcome. Ultrasound Obstet. Gynecol. 2024. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Tulzer, A.; Arzt, W.; Gitter, R.; Sames-Dolzer, E.; Kreuzer, M.; Mair, R.; Tulzer, G. Valvuloplasty in 103 fetuses with critical aortic stenosis: Outcome and new predictors for postnatal circulation. Ultrasound Obstet. Gynecol. 2022, 59, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Walter, A.; Strizek, B.; Weber, E.C.; Gottschalk, I.; Geipel, A.; Herberg, U.; Gembruch, U.; Berg, C. Intrauterine Valvuloplasty in Severe Aortic Stenosis—A Ten Years Single Center Experience. J. Clin. Med. 2022, 11, 3058. [Google Scholar] [CrossRef] [PubMed]
- Luo, G.; Zhang, B.; Wang, D.; Pan, S.; Sun, Y.; Wang, S. Fetal pulmonary valvuloplasty for pulmonary atresia with intact ventricular septum: A single-center clinical experience. Chin. Med. J. 2022, 136, 740–742. [Google Scholar] [CrossRef]
- Strainic, J. Fetal cardiac intervention for right sided heart disease: Pulmonary atresia with intact ventricular septum. Birth Defects Res. 2019, 111, 395–399. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Catheter-Based FCI | Goal | Maternal Risk | Risk of Fetal Demise | Need for Early Postnatal Intervention | Short-Term Outcomes FCI Vs. No or Unsuccessful FCI | Long-Term Outcomes |
|---|---|---|---|---|---|---|
| FAV | Improve likelihood of biventricular circulation | Minimal (see maternal risks) | 4–32%, pooled 16% | Common * | BiV no/unsuccessful FAV: 0–41% BiV FAV all comers: 28–45%, pooled 37% BiV among TS FAV liveborn: 39–68%, pooled 52% Survival (last FU) no/unsuccessful FAV: 0–100% Survival (last FU) FAV all comers: 21–75%, pooled 73% at 1 y Survival (last FU) among TS FAV liveborn: 55–74% (no pooled est.) Summary: reasonable evidence for higher likelihood of BiV repair. Insufficient data for improved survival to date, as many survival reports are limited to those who successfully achieved BiV repair and do not account for overall survival. Expectant management (no FAV but meeting criteria) also inconsistently reported. | Unknown |
| FASI | Improve stability at birth, improve survival | Minimal (see maternal risks) | 8–33% pooled 10% | Common * | Postnatal R/IAS among no/unsuccessful FASI: 41–100%, pooled 89% Postnatal R/IAS among FASI all comers: 38–50%, pooled 47% Postnatal R/IAS among TS FASI liveborn: 17–50% (no pooled est.) Survival to DC among no/unsuccessful FASI: 33–76%, pooled 57% Survival to DC among FASI all comers: 29–100%, pooled 46% Survival to DC among TS FASI liveborn: 44–60% (no pooled est.) Summary: reasonable evidence for less restriction at birth, although inclusion criteria for FASI are variable. Insufficient data for improved hospital discharge survival. | Unknown |
| FPV | Improve likelihood of biventricular circulation | Minimal (see maternal risks) | 0–36%, IFCIR 16% | Common * | BiV no FPV: 0–100%, IFCIR 33% BiV all FPV comers: 31–65%, IFCIR 56% BiV among TS FPV liveborn: 70–83%, IFCIR 77% Survival to DC no FPV: IFCIR 75% Survival to DC FPV all comers: IFCIR 75% Survival to DC among TS FPV liveborn: 89% Summary: FPV seems associated with a high likelihood of BiV repair, but no standard inclusion criteria or standard controls. Many subjects in the studies seem likely to have progressed to 1.5 or BiV based on prediction algorithms without intervention. Still insufficient data if FPV better than expectant management or who optimally would benefit from intervention. Insufficient data for improved survival to date. | Unknown |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yilmaz Furtun, B.; Morris, S.A. Catheter-Based Fetal Cardiac Interventions. J. Cardiovasc. Dev. Dis. 2024, 11, 167. https://doi.org/10.3390/jcdd11060167
Yilmaz Furtun B, Morris SA. Catheter-Based Fetal Cardiac Interventions. Journal of Cardiovascular Development and Disease. 2024; 11(6):167. https://doi.org/10.3390/jcdd11060167
Chicago/Turabian StyleYilmaz Furtun, Betul, and Shaine Alaine Morris. 2024. "Catheter-Based Fetal Cardiac Interventions" Journal of Cardiovascular Development and Disease 11, no. 6: 167. https://doi.org/10.3390/jcdd11060167