
Association of Abnormal Cardiac Biomarkers and Cardiovascular Complications, with Mortality in Patients with SARS-CoV-2 Infection in Latin America
 , , ,
, , ,  , , , , , , , , , , and
, , , , , , , , , , and
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Supervision and Data Collection
2.2. Participants
- Group A: 3 positive biomarkers, with 118 patients
- Group B: 2 positive biomarkers, with 190 patients
- Group C: 1 positive biomarker, with 139 patients
- Group D: No positive biomarkers, with 29 patients

2.3. Para-Clinical Tests
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics at Admission
3.2. Paraclinical Tests at Admission
3.3. Imaging Studies during Hospital Stay
3.4. Cardiovascular Complications during Hospitalization
3.5. Treatment for COVID-19
3.6. Respiratory and Cardiovascular Support
3.7. Outcomes during Hospitalization
3.8. Outcomes at 30-Day Follow-Up after Hospital Discharge
3.9. Comparison between Two Abnormal Biomarkers (Group B)
4. Discussion
4.1. General Information
4.1.1. General Characteristics
4.1.2. Clinical Manifestations
4.1.3. Paraclinical Tests on Admission
4.1.4. In-Hospital Complications
4.1.5. ICU Interventions
4.1.6. Anticoagulant Treatment
4.1.7. Hospital Outcomes
4.1.8. Outcomes at 30-Day Follow-Up
4.1.9. Comparison between Subgroups
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- COVID-19 Map—Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 23 July 2023).
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef]
- Mohamadian, M.; Chiti, H.; Shoghli, A.; Biglari, S.; Parsamanesh, N.; Esmaeilzadeh, A. COVID-19: Virology, biology and novel laboratory diagnosis. J. Gene Med. 2021, 23, e3303. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Paulson, K.R.; Pease, S.A.; Watson, S.; Comfort, H.; Zheng, P.; Aravkin, A.Y.; Bisignano, C.; Barber, R.M.; Alam, T.; et al. Estimating excess mortality due to the COVID-19 pandemic: A systematic analysis of COVID-19-related mortality, 2020–2021. Lancet 2022, 399, 1513–1536. [Google Scholar] [CrossRef] [PubMed]
- Datadot. COVID-19 Deaths | WHO COVID-19 Dashboard. Available online: https://data.who.int/dashboards/covid19/cases (accessed on 25 May 2024).
- Liu, F.; Liu, F.; Wang, L. COVID-19 and cardiovascular diseases. J. Mol. Cell Biol. 2021, 13, 161–167. [Google Scholar] [CrossRef] [PubMed]
- González-Calle, D.; Eiros, R.; Sánchez, P.L. Corazón y SARS-CoV-2. Med. Clin. 2022, 159, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 28, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.; Chen, M.; Zhang, Y. The cardiovascular disorders and prognostic cardiac biomarkers in COVID-19. Mol. Biol. Rep. 2021, 48, 1763–1771. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected with SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef]
- Speranza, M.; López-López, J.D.; Schwartzmann, P.; Morr, I.; Rodríguez-González, M.J.; Buitrago, A.; Pow-Chon-Long, F.; Passos, L.C.; Rossel, V.; Perna, E.R.; et al. Cardiovascular Complications in Patients with Heart Failure and COVID-19: CARDIO COVID 19-20 Registry. J. Cardiovasc. Dev. Dis. 2024, 11, 34. [Google Scholar] [CrossRef]
- Márquez-Murillo, M.F.; Echeverri, J.M.M.; Torres, W.B.; Alarcón, N.A.F.; Escalante, M.; Figueiredo, E.L.; Gómez, R.E.L.; Sierra-Lara, D.; Herrera, C.; Lugo, J.; et al. Desenlaces cardiovasculares en fibrilación auricular y COVID-19 grave en Latinoamérica: Registro CARDIO COVID 19-20. REC CardioClin. 2024, 59, 23–34. [Google Scholar] [CrossRef]
- Gomez-Mesa, J.E.; Galindo, S.; Escalante-Forero, M.; Rodas, Y.; Valencia, A.; Perna, E.; Romero, A.; Mendoza, I.; Wyss, F.; Barisani, J.L.; et al. Latin-American Registry of Cardiovascular Disease and COVID-19: Final Results. Glob. Heart 2023, 18, 60. [Google Scholar] [CrossRef] [PubMed]
- Metkus, T.S.; Sokoll, L.J.; Barth, A.S.; Czarny, M.J.; Hays, A.G.; Lowenstein, C.J.; Michos, E.D.; Nolley, E.P.; Post, W.S.; Resar, J.R.; et al. Myocardial Injury in Severe COVID-19 Compared with Non–COVID-19 Acute Respiratory Distress Syndrome. Circulation 2021, 143, 553–565. [Google Scholar] [CrossRef]
- Rehman, A.; Yousuf, S.; Maken, G.R.; Naqvi, S.R.A.; Murtaza, G.; Ahmad, A. Cardiac Troponin-I, A Biomarker for Predicting COVID-Induced Myocardial Damage Prognosis. J. Coll. Physicians Surg. Pak. JCPSP 2023, 33, 498–503. [Google Scholar] [CrossRef]
- Sandoval, Y.; Januzzi, J.L., Jr.; Jaffe, A.S. Cardiac Troponin for Assessment of Myocardial Injury in COVID-19: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2020, 76, 1244–1258. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Wu, D.I.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef]
- Sorrentino, S.; Cacia, M.; Leo, I.; Polimeni, A.; Sabatino, J.; Spaccarotella, C.A.M.; Mongiardo, A.; De Rosa, S.; Indolfi, C. B-Type Natriuretic Peptide as Biomarker of COVID-19 Disease Severity—A Meta-Analysis. J. Clin. Med. 2020, 9, 2957. [Google Scholar] [CrossRef]
- Yang, C.; Liu, F.; Liu, W.; Cao, G.; Liu, J.; Huang, S.; Zhu, M.; Tu, C.; Wang, J.; Xiong, B. Myocardial injury and risk factors for mortality in patients with COVID-19 pneumonia. Int. J. Cardiol. 2021, 326, 230–236. [Google Scholar] [CrossRef]
- Zhan, H.; Chen, H.; Liu, C.; Cheng, L.; Yan, S.; Li, H.; Li, Y. Diagnostic Value of D-Dimer in COVID-19: A Meta-Analysis and Meta-Regression. Clin. Appl. Thromb. 2021, 27, 10760296211010976. [Google Scholar] [CrossRef]
- Díez, J.M.B.; García, J.L.d.V.; Pelegrina, J.T.; Martínez, J.L.M.; Peñacoba, R.M.; Tejón, I.G.; Quintana, E.M.R.; Sajkiewicz, M.P.; Boronat, A.A.; Pérez, B.; et al. Epidemiología de las enfermedades cardiovasculares y factores de riesgo en atención primaria. Rev. Esp. Cardiol. 2005, 58, 367–373. [Google Scholar] [CrossRef]
- Barzallo, P. Fin de la Pandemia COVID-19. Rev. Med. Ateneo 2023, 25, 12–15. Available online: http://www.colegiomedicosazuay.ec/ojs/index.php/ateneo/article/view/286 (accessed on 24 July 2023).
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Kompaniyets, L.; Pennington, A.F.; Goodman, A.B.; Rosenblum, H.G.; Belay, B.; Ko, J.Y.; Chevinsky, J.R.; Schieber, L.Z.; Summers, A.D.; Lavery, A.M.; et al. Underlying Medical Conditions and Severe Illness among 540,667 Adults Hospitalized with COVID-19, March 2020–March 2021. Prev. Chronic Dis. 2021, 18, E66. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Nalla, L.V.; Sharma, M.; Sharma, N.; Singh, A.A.; Malim, F.M.; Ghatage, M.; Mukarram, M.; Pawar, A.; Parihar, N.; et al. Association of COVID-19 with Comorbidities: An Update. ACS Pharmacol. Transl. Sci. 2023, 6, 334–354. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.; Wang, B.; Yuan, T.; Chen, X.; Ao, Y.; Fitzpatrick, T.; Li, P.; Zhou, Y.; Lin, Y.-F.; Duan, Q.; et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. J. Infect. 2020, 80, 656–665. [Google Scholar] [CrossRef]
- Talukder, A.; Razu, S.R.; Alif, S.M.; Rahman, M.A.; Islam, S.M.S. Association between Symptoms and Severity of Disease in Hospitalised Novel Coronavirus (COVID-19) Patients: A Systematic Review and Meta-Analysis. J. Multidiscip. Healthc. 2022, 15, 1101–1110. [Google Scholar] [CrossRef]
- Han, H.; Xie, L.; Liu, R.; Yang, J.; Liu, F.; Wu, K.; Chen, L.; Hou, W.; Feng, Y.; Zhu, C. Analysis of heart injury laboratory parameters in 273 COVID-19 patients in one hospital in Wuhan, China. J. Med. Virol. 2020, 92, 819–823. [Google Scholar] [CrossRef]
- Zhu, Z.; Wang, M.; Lin, W.; Cai, Q.; Zhang, L.; Chen, D.; Liu, F.; Xiong, X.; Chu, J.; Peng, J.; et al. Cardiac biomarkers, cardiac injury, and comorbidities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. Immun. Inflamm. Dis. 2021, 9, 1071–1100. [Google Scholar] [CrossRef]
- Cersosimo, A.; Cimino, G.; Amore, L.; Calvi, E.; Pascariello, G.; Inciardi, R.M.; Lombardi, C.M.; Vizzardi, E.; Metra, M. Cardiac biomarkers and mortality in COVID-19 infection: A review. Monaldi Arch. Chest Dis. 2022, 93, 2276. [Google Scholar] [CrossRef]
- Standl, E.; Schnell, O. Heart failure outcomes and COVID-19. Diabetes Res. Clin. Pract. 2021, 175, 108794. [Google Scholar] [CrossRef] [PubMed]
- Rey, J.R.; Caro-Codón, J.; Rosillo, S.O.; Iniesta, M.; Castrejón-Castrejón, S.; Marco-Clement, I.; Martín-Polo, L.; Merino-Argos, C.; Rodríguez-Sotelo, L.; García-Veas, J.M.; et al. Heart failure in COVID-19 patients: Prevalence, incidence and prognostic implications. Eur. J. Heart Fail. 2020, 22, 2205–2215. [Google Scholar] [CrossRef] [PubMed]
- Bader, F.; Manla, Y.; Atallah, B.; Starling, R.C. Heart failure and COVID-19. Heart Fail. Rev. 2021, 26, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bader, M.W.; Adeen, A.M.A.; Hetta, O.E.; Fallata, M.H.; Alsiraihi, A.A.; Ahmed, M.E.; Kinsara, A.J.; Hetta, O.E.; Aloufi, A.K.; Alsiraihi, A.A.; et al. Association between COVID-19 Infection and Cardiac Biomarkers in Hospitalized Patients at a Tertiary Care Center. Cureus 2023, 15, e41527. [Google Scholar] [CrossRef] [PubMed]
- Al Oweidat, K.; Al-Amer, R.; Saleh, M.Y.; Albtoosh, A.S.; Toubasi, A.A.; Ribie, M.K.; Hasuneh, M.M.; Alfaqheri, D.L.; Alshurafa, A.H.; Ribie, M.; et al. Mortality, Intensive Care Unit Admission, and Intubation among Hospitalized Patients with COVID-19: A One-Year Retrospective Study in Jordan. J. Clin. Med. 2023, 12, 2651. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Anchan, R.K.; Besser, S.A.; Belkin, M.N.; Cruz, M.D.; Lee, L.; Yu, D.; Mehta, N.; Nguyen, A.B.; Alenghat, F.J. High sensitivity Troponin-T for prediction of adverse events in patients with COVID-19. Biomarkers 2020, 25, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, R.B.; Botelho, B.G.; de Hollanda, J.V.G.; Ferreira, L.V.L.; de Andrade, L.Z.J.; Oei, S.S.M.L.; Mello, T.d.S.; Muxfeldt, E.S. Covid-19 and the cardiovascular system: A comprehensive review. J. Hum. Hypertens. 2021, 35, 4–11. [Google Scholar] [CrossRef]
- Chung, M.K.; Zidar, D.A.; Bristow, M.R.; Cameron, S.J.; Chan, T.; Harding, C.V.; Kwon, D.H.; Singh, T.; Tilton, J.C.; Tsai, E.J.; et al. COVID-19 and Cardiovascular Disease. Circ. Res. 2021, 128, 1214–1236. [Google Scholar] [CrossRef]
- Gómez-Mesa, J.E.; Galindo-Coral, S.; Montes, M.C.; Martin, A.J.M. Thrombosis and Coagulopathy in COVID-19. Curr. Probl. Cardiol. 2021, 46, 100742. [Google Scholar] [CrossRef]
- Lo, Y.A.; Jok, C.; Tse, H. Cardiovascular complications of COVID-19. Hong Kong Med. J. 2022, 28, 249–256. [Google Scholar] [CrossRef]
- Asakura, H.; Ogawa, H. COVID-19-associated coagulopathy and disseminated intravascular coagulation. Int. J. Hematol. 2021, 113, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Flumignan, R.L.; Civile, V.T.; Tinôco, J.D.d.S.; Pascoal, P.I.; Areias, L.L.; Matar, C.F.; Tendal, B.; Trevisani, V.F.; Atallah, N.; Nakano, L.C. Anticoagulants for people hospitalised with COVID-19. Cochrane Database Syst. Rev. 2022, 2022, CD013739. [Google Scholar] [CrossRef]
- Cipriani, A.; Capone, F.; Donato, F.; Molinari, L.; Ceccato, D.; Saller, A.; Previato, L.; Pesavento, R.; Sarais, C.; Fioretto, P.; et al. Cardiac injury and mortality in patients with Coronavirus disease 2019 (COVID-19): Insights from a mediation analysis. Intern. Emerg. Med. 2021, 16, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, C.M.; Carubelli, V.; Iorio, A.; Inciardi, R.M.; Bellasi, A.; Canale, C.; Camporotondo, R.; Catagnano, F.; Dalla Vecchia, L.A.; Giovinazzo, S.; et al. Association of Troponin Levels with Mortality in Italian Patients Hospitalized with Coronavirus Disease 2019: Results of a Multicenter Study. JAMA Cardiol. 2020, 5, 1274–1280. [Google Scholar] [CrossRef] [PubMed]
- Battaglini, D.; Lopes-Pacheco, M.; Castro-Faria-Neto, H.C.; Pelosi, P.; Rocco, P.R.M. Laboratory Biomarkers for Diagnosis and Prognosis in COVID-19. Front. Immunol. 2022, 13, 857573. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Gao, J.; Zhu, W.; Feng, R.; Liu, Q.; Chen, X.; Huang, J.; Yang, Z.; Lin, X.; Zhang, Z.; et al. Indicators and prediction models for the severity of Covid-19. Int. J. Clin. Pract. 2021, 75, e14571. [Google Scholar] [CrossRef] [PubMed]
- Qin, J.-J.; Cheng, X.; Zhou, F.; Lei, F.; Akolkar, G.; Cai, J.; Zhang, X.-J.; Blet, A.; Xie, J.; Zhang, P.; et al. Redefining Cardiac Biomarkers in Predicting Mortality of Inpatients with COVID-19. Hypertension 2020, 76, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Peiris, S.; Nates, J.L.; Toledo, J.; Ho, Y.-L.; Sosa, O.; Stanford, V.; Aldighieri, S.; Reveiz, L. Hospital readmissions and emergency department re-presentation of COVID-19 patients: A systematic review. Rev. Panam. Salud Pública 2022, 46, e142. [Google Scholar] [CrossRef]
- Lionte, C.; Sorodoc, V.; Haliga, R.E.; Bologa, C.; Ceasovschih, A.; Petris, O.R.; Coman, A.E.; Stoica, A.; Sirbu, O.; Puha, G.; et al. Inflammatory and Cardiac Biomarkers in Relation with Post-Acute COVID-19 and Mortality: What We Know after Successive Pandemic Waves. Diagnostics 2022, 12, 1373. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N | Number of Positive Biomarkers | p-Value 2 | ||||
|---|---|---|---|---|---|---|---|
| Overall, | Group A, | Group B, | Group C, | Group D, | |||
| N = 476 1 | N = 118 1 | N = 190 1 | N = 139 1 | N = 29 1 | |||
| Sociodemographic characteristics | |||||||
| Age | 476 | 64.0 | 69.0 | 65.5 | 58.0 | 49.0 | <0.001 |
| (52.0–73.0) | (58.0–77.0) | (55.2–74.0) | (46.5–68.0) | (40.0–69.0) | |||
| Gender | 476 | 0.3 | |||||
| Female | 151 (31.7%) | 44 (37.3%) | 60 (31.6%) | 41 (29.5%) | 6 (20.7%) | ||
| Male | 325 (68.3%) | 74 (62.7%) | 130 (68.4%) | 98 (70.5%) | 23 (79.3%) | ||
| Comorbidities | |||||||
| Hypertension | 476 | 273 (57.4%) | 79 (66.9%) | 114 (60.0%) | 69 (49.6%) | 11 (37.9%) | 0.005 |
| Diabetes mellitus | 476 | 162 (34.0%) | 43 (36.4%) | 71 (37.4%) | 41 (29.5%) | 7 (24.1%) | 0.3 |
| Dyslipidemia | 476 | 79 (16.6%) | 28 (23.7%) | 39 (20.5%) | 10 (7.2%) | 2 (6.9%) | <0.001 |
| Overweight/obesity | 476 | 277 (58.2%) | 60 (50.8%) | 121 (63.7%) | 81 (58.3%) | 15 (51.7%) | 0.14 |
| Coronary heart disease | 476 | 0.5 | |||||
| Clinical | 29 (6.1%) | 13 (11.0%) | 9 (4.7%) | 6 (4.3%) | 1 (3.4%) | ||
| Stent | 18 (3.8%) | 7 (5.9%) | 7 (3.7%) | 3 (2.2%) | 1 (3.4%) | ||
| Myocardial revascularization | 5 (1.1%) | 1 (0.8%) | 2 (1.1%) | 2 (1.4%) | 0 (0.0%) | ||
| Both | 1 (0.2%) | 0 (0.0%) | 1 (0.5%) | 0 (0.0%) | 0 (0.0%) | ||
| Heart failure | 476 | 41 (8.6%) | 21 (17.8%) | 14 (7.4%) | 4 (2.9%) | 2 (6.9%) | <0.001 |
| LVEF | 36 | 0.3 | |||||
| LVEF < 40% | 23 (63.9%) | 12 (66.7%) | 7 (53.8%) | 3 (100.0%) | 1 (50.0%) | ||
| LVEF 40–50% | 5 (13.9%) | 4 (22.2%) | 1 (7.7%) | 0 (0.0%) | 0 (0.0%) | ||
| LVEF > 50% | 8 (22.2%) | 2 (11.1%) | 5 (38.5%) | 0 (0.0%) | 1 (50.0%) | ||
| Atrial fibrillation | 476 | 25 (5.3%) | 9 (7.6%) | 10 (5.3%) | 5 (3.6%) | 1 (3.4%) | 0.5 |
| Stroke | 476 | 10 (2.1%) | 3 (2.5%) | 6 (3.2%) | 1 (0.7%) | 0 (0.0%) | 0.4 |
| Variables | N | Number of Positive Biomarkers | p-Value 2 | ||||
|---|---|---|---|---|---|---|---|
| Overall, | Group A, | Group B, | Group C, | Group D, | |||
| N = 476 1 | N = 118 1 | N = 190 1 | N = 139 1 | N = 29 1 | |||
| Chest X-ray | 476 | 455 (95.6%) | 112 (94.9%) | 180 (94.7%) | 135 (97.1%) | 28 (96.6%) | 0.7 |
| Pulmonary infiltrates | 455 | 0.032 | |||||
| Unilateral | 35 (7.7%) | 4 (3.6%) | 17 (9.4%) | 10 (7.4%) | 4 (14.3%) | ||
| Bilateral | 371 (81.5%) | 99 (88.4%) | 142 (78.9%) | 113 (83.7%) | 17 (60.7%) | ||
| cardiomegaly | 455 | 84 (18.5%) | 36 (32.1%) | 32 (17.8%) | 15 (11.1%) | 1 (3.6%) | <0.001 |
| Lung congestion | 455 | <0.001 | |||||
| Unilateral | 11 (2.4%) | 3 (2.7%) | 5 (2.8%) | 3 (2.2%) | 0 (0.0%) | ||
| Bilateral | 93 (20.4%) | 41 (36.6%) | 34 (18.9%) | 18 (13.3%) | 0 (0.0%) | ||
| Pleural effusion | 455 | <0.001 | |||||
| Unilateral | 25 (5.5%) | 8 (7.1%) | 14 (7.8%) | 2 (1.5%) | 1 (3.6%) | ||
| Bilateral | 27 (5.9%) | 16 (14.3%) | 8 (4.4%) | 2 (1.5%) | 1 (3.6%) | ||
| Transthoracic echocardiogram | 476 | 120 (25.2%) | 44 (37.3%) | 46 (24.2%) | 26 (18.7%) | 4 (13.8%) | 0.002 |
| Systolic function | 119 | 0.3 | |||||
| Normal | 78 (65.5%) | 22 (50.0%) | 32 (71.1%) | 21 (80.8%) | 3 (75.0%) | ||
| Focal decrease | 14 (11.8%) | 8 (18.2%) | 4 (8.9%) | 1 (3.8%) | 1 (25.0%) | ||
| Global decrease | 25 (21.0%) | 13 (29.5%) | 8 (17.8%) | 4 (15.4%) | 0 (0.0%) | ||
| Right ventricular dysfunction | 118 | 17 (14.4%) | 14 (32.6%) | 2 (4.4%) | 1 (3.8%) | 0 (0.0%) | <0.001 |
| Variables | N | Number of Positive Biomarkers | p-Value 2 | ||||
|---|---|---|---|---|---|---|---|
| Overall, | Group A, | Group B, | Group C, | Group D, | |||
| N = 476 1 | N = 118 1 | N = 190 1 | N = 139 1 | N = 29 1 | |||
| Acute heart failure | 476 | 84 (17.6%) | 42 (35.6%) | 35 (18.4%) | 7 (5.0%) | 0 (0.0%) | <0.001 |
| Cardiac arrythmia | 476 | 62 (13.0%) | 27 (22.9%) | 26 (13.7%) | 7 (5.0%) | 2 (6.9%) | <0.001 |
| Miocarditis | 476 | 13 (2.7%) | 6 (5.1%) | 5 (2.6%) | 2 (1.4%) | 0 (0.0%) | 0.2 |
| Pulmonary tromboembolism | 476 | 22 (4.6%) | 5 (4.2%) | 8 (4.2%) | 9 (6.5%) | 0 (0.0%) | 0.5 |
| Other | 476 | 75 (15.8%) | 30 (25.4%) | 27 (14.2%) | 17 (12.2%) | 1 (3.4%) | 0.004 |
| Variables | N | Number of Positive Biomarkers | p-Value 2 | ||||
|---|---|---|---|---|---|---|---|
| Overall, | Group A, | Group B, | Group C, | Group D, | |||
| N = 476 1 | N = 118 1 | N = 190 1 | N = 139 1 | N = 29 1 | |||
| Vasopressors | 476 | 208 (43.7%) | 59 (50.0%) | 83 (43.7%) | 60 (43.2%) | 6 (20.7%) | 0.043 |
| Inotropes | 476 | 83 (17.4%) | 34 (28.8%) | 32 (16.8%) | 17 (12.2%) | 0 (0.0%) | <0.001 |
| Vasodilators | 476 | 30 (6.3%) | 14 (11.9%) | 10 (5.3%) | 6 (4.3%) | 0 (0.0%) | 0.024 |
| IMV | 476 | 240 (50.4%) | 63 (53.4%) | 99 (52.1%) | 71 (51.1%) | 7 (24.1%) | 0.034 |
| NIVM | 476 | 87 (18.3%) | 15 (12.7%) | 43 (22.6%) | 25 (18.0%) | 4 (13.8%) | 0.2 |
| Variables | N | Number of Positive Biomarkers | p-Value 2 | ||||
|---|---|---|---|---|---|---|---|
| Overall, | Group A, | Group B, | Group C, | Group D, | |||
| N = 476 1 | N = 118 1 | N = 190 1 | N = 139 1 | N = 29 1 | |||
| ICU admission | 476 | 335 (70.4%) | 87 (73.7%) | 129 (67.9%) | 103 (74.1%) | 16 (55.2%) | 0.15 |
| Condition at discharge | 476 | <0.001 | |||||
| Alive | 333 (70.0%) | 59 (50.0%) | 131 (68.9%) | 114 (82.0%) | 29 (100.0%) | ||
| Dead | 143 (30.0%) | 59 (50.0%) | 59 (31.1%) | 25 (18.0%) | 0 (0.0%) | ||
| Type of death | 143 | 0.066 | |||||
| Cardiovascular | 42 (29.4%) | 22 (37.3%) | 17 (28.8%) | 3 (12.0%) | 0 (NA%) | ||
| Not cardiovascular | 101 (70.6%) | 37 (62.7%) | 42 (71.2%) | 22 (88.0%) | 0 (NA%) | ||
| Variables | N | Number of Positive Biomarkers | p-Value 2 | ||||
|---|---|---|---|---|---|---|---|
| Overall, | Group A, | Group B, | Group C, | Group D, | |||
| N = 333 1 | N = 59 1 | N = 131 1 | N = 114 1 | N = 29 1 | |||
| Status | 307 | 0.2 | |||||
| Alive | 305 (99.3%) | 50 (100.0%) | 125 (99.2%) | 102 (100.0%) | 28 (96.6%) | ||
| Dead | 2 (0.7%) | 0 (0.0%) | 1 (0.8%) | 0 (0.0%) | 1 (3.4%) | ||
| Rehospitalization | 293 | 19 (6.5%) | 5 (10.6%) | 7 (5.8%) | 6 (6.1%) | 1 (3.7%) | 0.6 |
| Death cause | 2 | ||||||
| Non cardiovascular | 2 (100.0%) | 0 (NA%) | 1 (100.0%) | 0 (NA%) | 1 (100.0%) | ||
| Overall, N = 190 | Troponine + Natriuretic Peptide. N = 44 | Troponine + D-Dimer. N = 25 | D-Dimer + Natriuretic Peptide. N = 121 | ||
|---|---|---|---|---|---|
| Condition at discharge | 190 | ||||
| Alive | 131 (68.9%) | 25 (56.9%) | 14 (56.0%) | 92 (76.0%) | |
| Dead | 59 (31.1%) | 19 (43.2%) | 11 (44.0%) | 29 (24.0%) | |
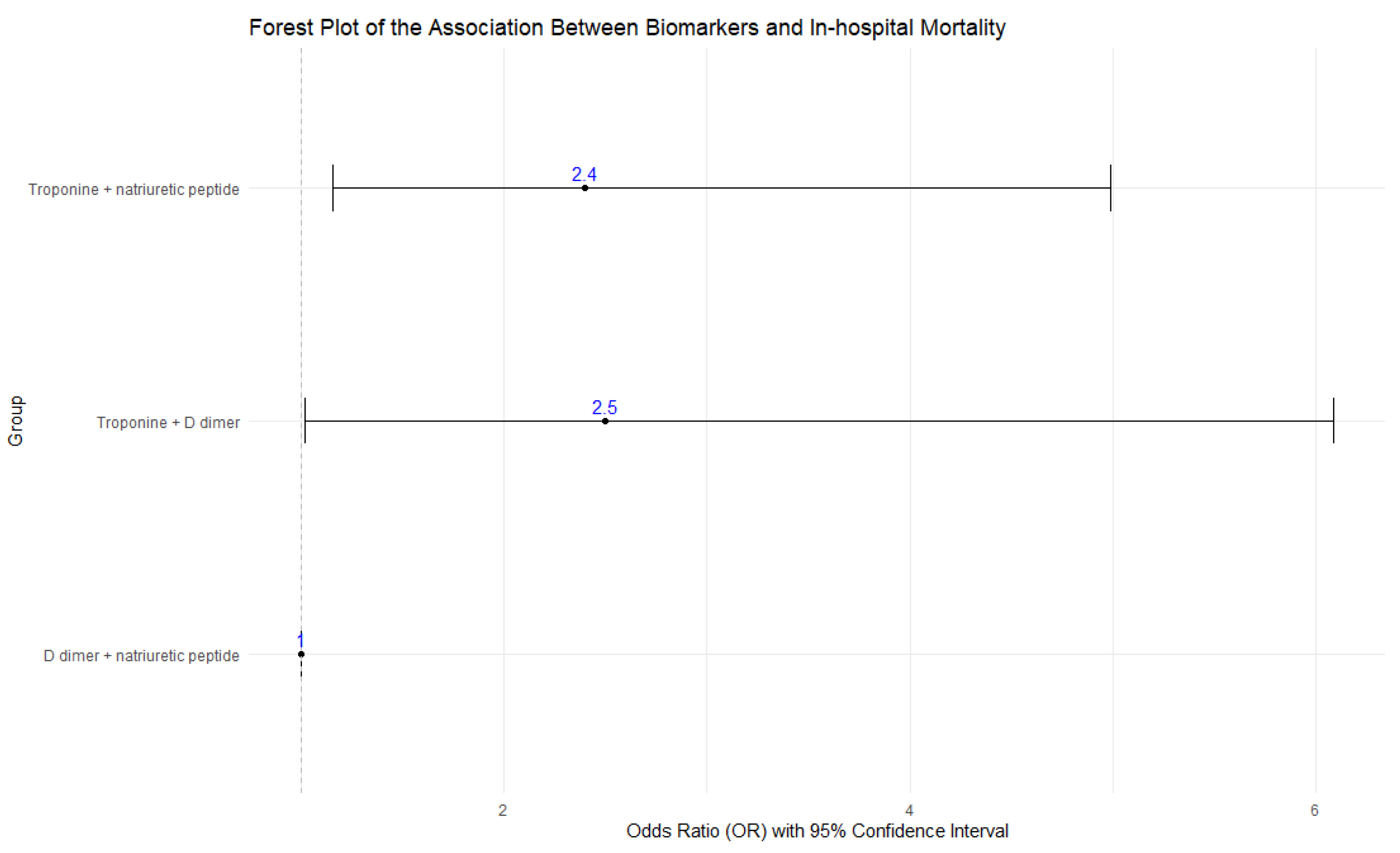
| N | OR | CI 95% | p-value | ||
| D dimer + natriuretic peptide | 121 | 1 | |||
| Troponine + natriuretic peptide | 44 | 2.4 | 1.16–4.99 | 0.018 | |
| Troponine + D dimer | 25 | 2.5 | 1.02–6.09 | 0.045 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Mesa, J.E.; Escalante, M.; Muñoz-Ordoñez, J.A.; Azcárate-Rodriguez, V.; Peláez-Martínez, J.D.; Arteaga-Tobar, A.A.; León-Giraldo, H.; Valencia-Orozco, A.; Perna, E.R.; Romero, A.; et al. Association of Abnormal Cardiac Biomarkers and Cardiovascular Complications, with Mortality in Patients with SARS-CoV-2 Infection in Latin America. J. Cardiovasc. Dev. Dis. 2024, 11, 205. https://doi.org/10.3390/jcdd11070205
Gómez-Mesa JE, Escalante M, Muñoz-Ordoñez JA, Azcárate-Rodriguez V, Peláez-Martínez JD, Arteaga-Tobar AA, León-Giraldo H, Valencia-Orozco A, Perna ER, Romero A, et al. Association of Abnormal Cardiac Biomarkers and Cardiovascular Complications, with Mortality in Patients with SARS-CoV-2 Infection in Latin America. Journal of Cardiovascular Development and Disease. 2024; 11(7):205. https://doi.org/10.3390/jcdd11070205
Chicago/Turabian StyleGómez-Mesa, Juan Esteban, Manuela Escalante, Juan Andrés Muñoz-Ordoñez, Valeria Azcárate-Rodriguez, Juan David Peláez-Martínez, Andrea Alejandra Arteaga-Tobar, Hoover León-Giraldo, Andrea Valencia-Orozco, Eduardo Roque Perna, Alexander Romero, and et al. 2024. "Association of Abnormal Cardiac Biomarkers and Cardiovascular Complications, with Mortality in Patients with SARS-CoV-2 Infection in Latin America" Journal of Cardiovascular Development and Disease 11, no. 7: 205. https://doi.org/10.3390/jcdd11070205