
Cancer and Heart Failure: Dangerous Liaisons

Abstract
:1. Introduction
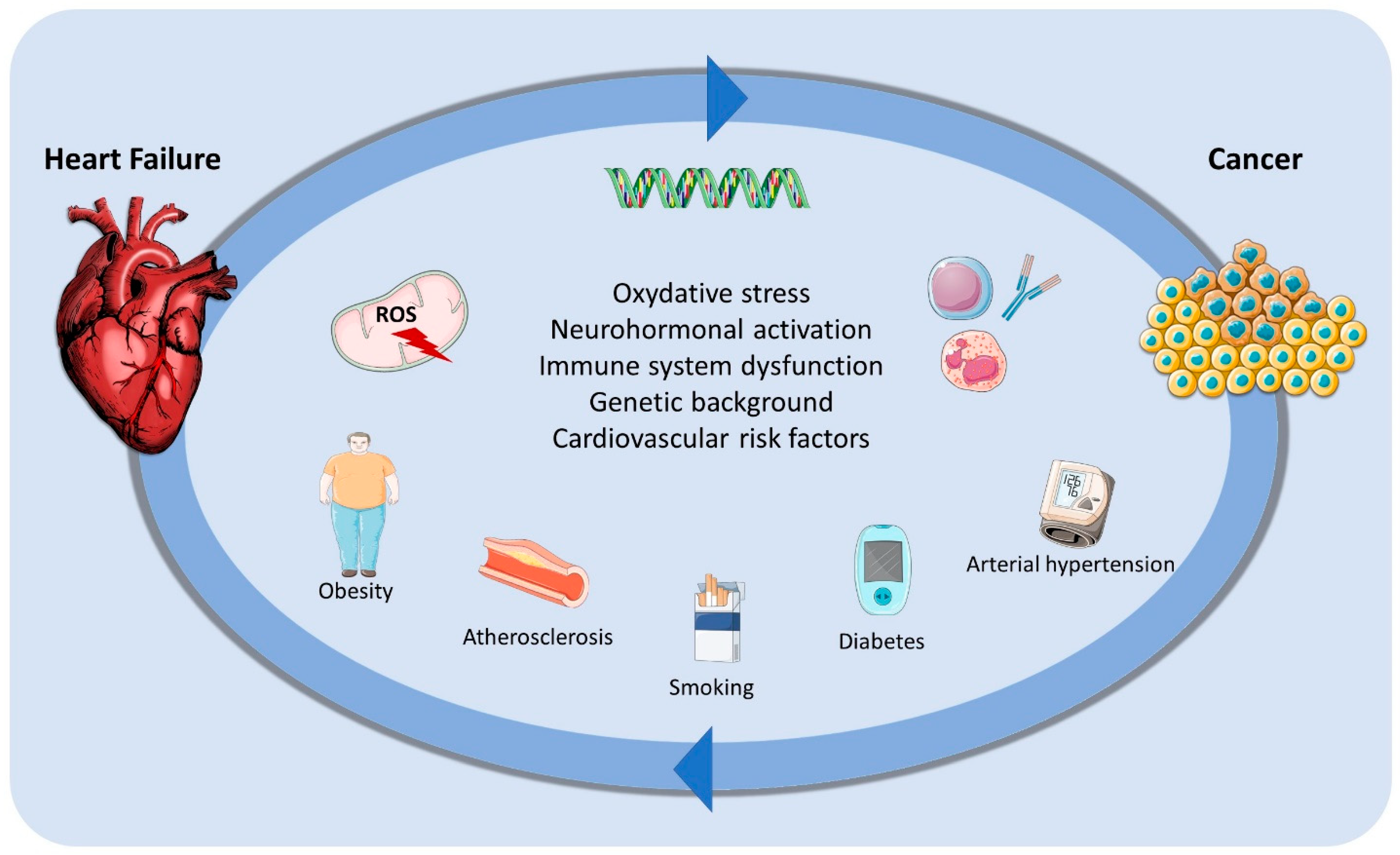
2. Cardiovascular Risk Factors and Cancer Development: The “Reverse Cardio-Oncology”
3. Heart Failure as a Complication of Cancer Therapy
4. Mechanisms of Cardiotoxicity of the Main Chemotherapy Agents and Their Association with Heart Failure
4.1. Anthracyclines
4.2. HER2 Inhibitors
4.3. VEGF Inhibitors
4.4. Hematological Therapies
4.5. BRAF/MEK Inhibitors
4.6. EGFR Inhibitors
4.7. Immune Checkpoint Inhibitors
5. Heart Failure Prevention in Cancer Patients
5.1. Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers
5.2. Beta-Blockers
5.3. Sacubitril Valsartan
5.4. Sodium–Glucose Co-Transporter Inhibitors
5.5. Other Mechanisms of Cardioprotection
5.6. Dyslipidemia and Diabetes Treatment
5.7. Practical Approach to Cardioprotection
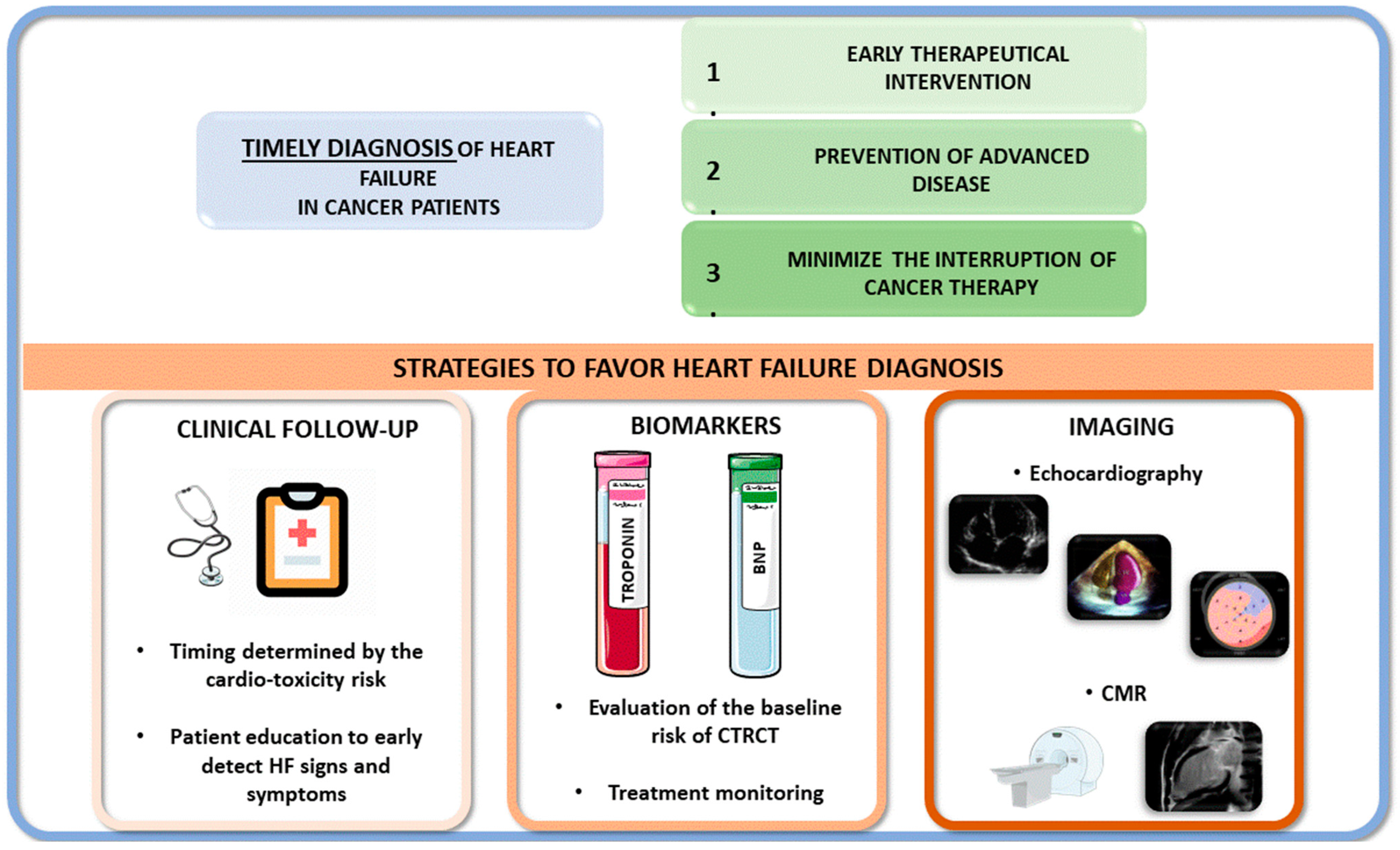
6. Heart Failure Diagnosis in Cancer Patients
7. Management of Chemotherapy-Induced Heart Failure
Device Therapy and Advanced HF Therapy in Cancer Patients
8. Follow-Up after Cancer
9. Future Perspectives
- (1)
- (2)
- Recognizing the role of genetics and hereditable tracts in identifying patients at risk of developing HF during chemotherapy and discovering new therapeutic targets [157];
- (3)
- (4)
- Adopting rigorous translational research protocols, trying to consider the heterogeneity observed in real-life patients [154];
- (5)
- Underscoring the impact of psychosocial stress, gender, ethnicity, and social status on the relationship between HF and cancer.
10. Conclusions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Max Roser, Hannah Ritchie and Fiona Spooner (2021)—“Burden of Disease” Published Online at OurWorldInData.Org. Available online: https://ourworldindata.org/burden-of-disease (accessed on 21 August 2024).
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 354 Diseases and Injuries for 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Aboumsallem, J.P.; Moslehi, J.; De Boer, R.A. Reverse Cardio-Oncology: Cancer Development in Patients with Cardiovascular Disease. J. Am. Heart Assoc. 2020, 9, e013754. [Google Scholar] [CrossRef]
- Lund, L.H.; Donal, E.; Oger, E.; Hage, C.; Persson, H.; Haugen-Löfman, I.; Ennezat, P.; Sportouch-Dukhan, C.; Drouet, E.; Daubert, J.; et al. Association between Cardiovascular vs. Non-cardiovascular Co-morbidities and Outcomes in Heart Failure with Preserved Ejection Fraction. Eur. J. Heart Fail. 2014, 16, 992–1001. [Google Scholar] [CrossRef]
- Tribouilloy, C.; Rusinaru, D.; Mahjoub, H.; Souliere, V.; Levy, F.; Peltier, M.; Slama, M.; Massy, Z. Prognosis of Heart Failure with Preserved Ejection Fraction: A 5 Year Prospective Population-Based Study. Eur. Heart J. 2008, 29, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Patel, R.B.; Michel, A.; Shah, S.J.; Senni, M.; Gheorghiade, M.; Butler, J. Mode of Death in Heart Failure with Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2017, 69, 556–569. [Google Scholar] [CrossRef]
- Massie, B.M.; Carson, P.E.; McMurray, J.J.; Komajda, M.; McKelvie, R.; Zile, M.R.; Anderson, S.; Donovan, M.; Iverson, E.; Staiger, C.; et al. Irbesartan in Patients with Heart Failure and Preserved Ejection Fraction. N. Engl. J. Med. 2008, 359, 2456–2467. [Google Scholar] [CrossRef]
- Pitt, B.; Pfeffer, M.A.; Assmann, S.F.; Boineau, R.; Anand, I.S.; Claggett, B.; Clausell, N.; Desai, A.S.; Diaz, R.; Fleg, J.L.; et al. Spironolactone for Heart Failure with Preserved Ejection Fraction. N. Engl. J. Med. 2014, 370, 1383–1392. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.V.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin–Neprilysin Inhibition versus Enalapril in Heart Failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef]
- Moliner, P.; Lupón, J.; De Antonio, M.; Domingo, M.; Santiago-Vacas, E.; Zamora, E.; Cediel, G.; Santesmases, J.; Díez-Quevedo, C.; Troya, M.I.; et al. Trends in Modes of Death in Heart Failure over the Last Two Decades: Less Sudden Death but Cancer Deaths on the Rise. Eur. J. Heart Fail. 2019, 21, 1259–1266. [Google Scholar] [CrossRef]
- Conrad, N.; Judge, A.; Canoy, D.; Tran, J.; Pinho-Gomes, A.-C.; Millett, E.R.C.; Salimi-Khorshidi, G.; Cleland, J.G.; McMurray, J.J.V.; Rahimi, K. Temporal Trends and Patterns in Mortality After Incident Heart Failure: A Longitudinal Analysis of 86000 Individuals. JAMA Cardiol. 2019, 4, 1102. [Google Scholar] [CrossRef] [PubMed]
- Bertero, E.; Robusto, F.; Rulli, E.; D’Ettorre, A.; Bisceglia, L.; Staszewsky, L.; Maack, C.; Lepore, V.; Latini, R.; Ameri, P. Cancer Incidence and Mortality According to Pre-Existing Heart Failure in a Community-Based Cohort. JACC CardioOncology 2022, 4, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Roderburg, C.; Loosen, S.H.; Jahn, J.K.; Gänsbacher, J.; Luedde, T.; Kostev, K.; Luedde, M. Heart Failure Is Associated with an Increased Incidence of Cancer Diagnoses. ESC Heart Fail. 2021, 8, 3628–3633. [Google Scholar] [CrossRef] [PubMed]
- Camilli, M.; Chiabrando, J.G.; Lombardi, M.; Del Buono, M.G.; Montone, R.A.; Lombardo, A.; Crea, F.; Minotti, G. Cancer Incidence and Mortality in Patients Diagnosed with Heart Failure: Results from an Updated Systematic Review and Meta-Analysis. Cardio-Oncology 2023, 9, 8. [Google Scholar] [CrossRef]
- Jaiswal, V.; Ang, S.P.; Agrawal, V.; Hameed, M.; Saleeb, M.R.A.; Jaiswal, A.; Shah, M.; Lao, N.M.; Chia, J.E.; Paudel, K.; et al. Association between Heart Failure and the Incidence of Cancer: A Systematic Review and Meta-Analysis. Eur. Heart J. Open 2023, 3, oead073. [Google Scholar] [CrossRef]
- Banke, A.; Schou, M.; Videbæk, L.; Møller, J.E.; Torp-Pedersen, C.; Gustafsson, F.; Dahl, J.S.; Køber, L.; Hildebrandt, P.R.; Gislason, G.H. Incidence of Cancer in Patients with Chronic Heart Failure: A Long-term Follow-up Study. Eur. J. Heart Fail. 2016, 18, 260–266. [Google Scholar] [CrossRef]
- Bertero, E.; Canepa, M.; Maack, C.; Ameri, P. Linking Heart Failure to Cancer: Background Evidence and Research Perspectives. Circulation 2018, 138, 735–742. [Google Scholar] [CrossRef]
- De Boer, R.A.; Meijers, W.C.; Van Der Meer, P.; Van Veldhuisen, D.J. Cancer and Heart Disease: Associations and Relations. Eur. J. Heart Fail. 2019, 21, 1515–1525. [Google Scholar] [CrossRef]
- Pfeffer, T.J.; Pietzsch, S.; Hilfiker-Kleiner, D. Common Genetic Predisposition for Heart Failure and Cancer. Herz 2020, 45, 632–636. [Google Scholar] [CrossRef]
- Meijers, W.C.; De Boer, R.A. Common Risk Factors for Heart Failure and Cancer. Cardiovasc. Res. 2019, 115, 844–853. [Google Scholar] [CrossRef]
- Meijers, W.C.; Maglione, M.; Bakker, S.J.L.; Oberhuber, R.; Kieneker, L.M.; De Jong, S.; Haubner, B.J.; Nagengast, W.B.; Lyon, A.R.; Van Der Vegt, B.; et al. Heart Failure Stimulates Tumor Growth by Circulating Factors. Circulation 2018, 138, 678–691. [Google Scholar] [CrossRef]
- Jacobs, L.; Efremov, L.; Ferreira, J.P.; Thijs, L.; Yang, W.; Zhang, Z.; Latini, R.; Masson, S.; Agabiti, N.; Sever, P.; et al. Risk for Incident Heart Failure: A Subject-Level Meta-Analysis From the Heart “OMics” in AGEing (HOMAGE) Study. J. Am. Heart Assoc. 2017, 6, e005231. [Google Scholar] [CrossRef] [PubMed]
- Bayliss, E.A.; Reifler, L.M.; Zeng, C.; McQuillan, D.B.; Ellis, J.L.; Steiner, J.F. Competing Risks of Cancer Mortality and Cardiovascular Events in Individuals with Multimorbidity. J. Comorbidity 2014, 4, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Akinyemiju, T.; Wiener, H.; Pisu, M. Cancer-Related Risk Factors and Incidence of Major Cancers by Race, Gender and Region; Analysis of the NIH-AARP Diet and Health Study. BMC Cancer 2017, 17, 597. [Google Scholar] [CrossRef] [PubMed]
- Tu, H.; Wen, C.P.; Tsai, S.P.; Chow, W.-H.; Wen, C.; Ye, Y.; Zhao, H.; Tsai, M.K.; Huang, M.; Dinney, C.P.; et al. Cancer Risk Associated with Chronic Diseases and Disease Markers: Prospective Cohort Study. BMJ 2018, 360, k134. [Google Scholar] [CrossRef]
- Opie, L.H.; Lopaschuk, G.D. What Is Good for the Circulation Also Lessens Cancer Risk. Eur. Heart J. 2015, 36, 1157–1162. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen-Torvik, L.J.; Shay, C.M.; Abramson, J.G.; Friedrich, C.A.; Nettleton, J.A.; Prizment, A.E.; Folsom, A.R. Ideal Cardiovascular Health Is Inversely Associated with Incident Cancer: The Atherosclerosis Risk in Communities Study. Circulation 2013, 127, 1270–1275. [Google Scholar] [CrossRef]
- Kushi, L.H.; Doyle, C.; McCullough, M.; Rock, C.L.; Demark-Wahnefried, W.; Bandera, E.V.; Gapstur, S.; Patel, A.V.; Andrews, K.; Gansler, T.; et al. American Cancer Society Guidelines on Nutrition and Physical Activity for Cancer Prevention: Reducing the Risk of Cancer with Healthy Food Choices and Physical Activity. CA Cancer J. Clin. 2012, 62, 30–67. [Google Scholar] [CrossRef]
- Herrmann, J.; Lenihan, D.; Armenian, S.; Barac, A.; Blaes, A.; Cardinale, D.; Carver, J.; Dent, S.; Ky, B.; Lyon, A.R.; et al. Defining Cardiovascular Toxicities of Cancer Therapies: An International Cardio-Oncology Society (IC-OS) Consensus Statement. Eur. Heart J. 2022, 43, 280–299. [Google Scholar] [CrossRef]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on Cardio-Oncology Developed in Collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Muñoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.H.; Lyon, A.R.; et al. 2016 ESC Position Paper on Cancer Treatments and Cardiovascular Toxicity Developed under the Auspices of the ESC Committee for Practice Guidelines: The Task Force for Cancer Treatments and Cardiovascular Toxicity of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef] [PubMed]
- Boekel, N.B.; Jacobse, J.N.; Schaapveld, M.; Hooning, M.J.; Gietema, J.A.; Duane, F.K.; Taylor, C.W.; Darby, S.C.; Hauptmann, M.; Seynaeve, C.M.; et al. Cardiovascular Disease Incidence after Internal Mammary Chain Irradiation and Anthracycline-Based Chemotherapy for Breast Cancer. Br. J. Cancer 2018, 119, 408–418. [Google Scholar] [CrossRef]
- Boekel, N.B.; Duane, F.K.; Jacobse, J.N.; Hauptmann, M.; Schaapveld, M.; Sonke, G.S.; Gietema, J.A.; Hooning, M.J.; Seynaeve, C.M.; Maas, A.H.E.M.; et al. Heart Failure after Treatment for Breast Cancer. Eur. J. Heart Fail. 2020, 22, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Bowles, E.J.A.; Wellman, R.; Feigelson, H.S.; Onitilo, A.A.; Freedman, A.N.; Delate, T.; Allen, L.A.; Nekhlyudov, L.; Goddard, K.A.B.; Davis, R.L.; et al. Risk of Heart Failure in Breast Cancer Patients After Anthracycline and Trastuzumab Treatment: A Retrospective Cohort Study. JNCI J. Natl. Cancer Inst. 2012, 104, 1293–1305. [Google Scholar] [CrossRef]
- Jacobse, J.N.; Schaapveld, M.; Boekel, N.B.; Hooning, M.J.; Jager, A.; Baaijens, M.H.A.; Hauptmann, M.; Russell, N.S.; Rutgers, E.J.T.; Aleman, B.M.P.; et al. Risk of heart failure after systemic treatment for early breast cancer: Results of a cohort study. Breast Cancer Res. Treat. 2021, 185, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Lotrionte, M.; Biondi-Zoccai, G.; Abbate, A.; Lanzetta, G.; D’Ascenzo, F.; Malavasi, V.; Peruzzi, M.; Frati, G.; Palazzoni, G. Review and Meta-Analysis of Incidence and Clinical Predictors of Anthracycline Cardiotoxicity. Am. J. Cardiol. 2013, 112, 1980–1984. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Colombo, A.; Bacchiani, G.; Tedeschi, I.; Meroni, C.A.; Veglia, F.; Civelli, M.; Lamantia, G.; Colombo, N.; Curigliano, G.; et al. Early Detection of Anthracycline Cardiotoxicity and Improvement with Heart Failure Therapy. Circulation 2015, 131, 1981–1988. [Google Scholar] [CrossRef]
- Von Hoff, D.D. Risk Factors for Doxorubicin-Lnduced Congestive Heart Failure. Ann. Intern. Med. 1979, 91, 710. [Google Scholar] [CrossRef]
- Swain, S.M.; Whaley, F.S.; Ewer, M.S. Congestive Heart Failure in Patients Treated with Doxorubicin: A Retrospective Analysis of Three Trials. Cancer 2003, 97, 2869–2879. [Google Scholar] [CrossRef] [PubMed]
- Pinder, M.C.; Duan, Z.; Goodwin, J.S.; Hortobagyi, G.N.; Giordano, S.H. Congestive Heart Failure in Older Women Treated With Adjuvant Anthracycline Chemotherapy for Breast Cancer. J. Clin. Oncol. 2007, 25, 3808–3815. [Google Scholar] [CrossRef]
- Thavendiranathan, P.; Abdel-Qadir, H.; Fischer, H.D.; Camacho, X.; Amir, E.; Austin, P.C.; Lee, D.S. Breast Cancer Therapy–Related Cardiac Dysfunction in Adult Women Treated in Routine Clinical Practice: A Population-Based Cohort Study. J. Clin. Oncol. 2016, 34, 2239–2246. [Google Scholar] [CrossRef]
- Ganz, P.A.; Hussey, M.A.; Moinpour, C.M.; Unger, J.M.; Hutchins, L.F.; Dakhil, S.R.; Giguere, J.K.; Goodwin, J.W.; Martino, S.; Albain, K.S. Late Cardiac Effects of Adjuvant Chemotherapy in Breast Cancer Survivors Treated on Southwest Oncology Group Protocol S8897. J. Clin. Oncol. 2008, 26, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Biasillo, G.; Salvatici, M.; Sandri, M.T.; Cipolla, C.M. Using Biomarkers to Predict and to Prevent Cardiotoxicity of Cancer Therapy. Expert Rev. Mol. Diagn. 2017, 17, 245–256. [Google Scholar] [CrossRef]
- Qiu, S.; Zhou, T.; Qiu, B.; Zhang, Y.; Zhou, Y.; Yu, H.; Zhang, J.; Liu, L.; Yuan, L.; Yang, G.; et al. Risk Factors for Anthracycline-Induced Cardiotoxicity. Front. Cardiovasc. Med. 2021, 8, 736854. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Cardinale, D.; Dent, S.; Criscitiello, C.; Aseyev, O.; Lenihan, D.; Cipolla, C.M. Cardiotoxicity of Anticancer Treatments: Epidemiology, Detection, and Management. CA Cancer J. Clin. 2016, 66, 309–325. [Google Scholar] [CrossRef] [PubMed]
- Slamon, D.J.; Leyland-Jones, B.; Shak, S.; Fuchs, H.; Paton, V.; Bajamonde, A.; Fleming, T.; Eiermann, W.; Wolter, J.; Pegram, M.; et al. Use of Chemotherapy plus a Monoclonal Antibody against HER2 for Metastatic Breast Cancer That Overexpresses HER2. N. Engl. J. Med. 2001, 344, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Moja, L.; Tagliabue, L.; Balduzzi, S.; Parmelli, E.; Pistotti, V.; Guarneri, V.; D’Amico, R. Trastuzumab Containing Regimens for Early Breast Cancer. Cochrane Database Syst. Rev. 2012, 2021, CD006243. [Google Scholar] [CrossRef]
- De Azambuja, E.; Ponde, N.; Procter, M.; Rastogi, P.; Cecchini, R.S.; Lambertini, M.; Ballman, K.; Aspitia, A.M.; Zardavas, D.; Roca, L.; et al. A Pooled Analysis of the Cardiac Events in the Trastuzumab Adjuvant Trials. Breast Cancer Res. Treat. 2020, 179, 161–171. [Google Scholar] [CrossRef]
- Ewer, M.S.; Ewer, S.M. Cardiotoxicity of Anticancer Treatments. Nat. Rev. Cardiol. 2015, 12, 547–558. [Google Scholar] [CrossRef]
- De Azambuja, E.; Procter, M.J.; Van Veldhuisen, D.J.; Agbor-Tarh, D.; Metzger-Filho, O.; Steinseifer, J.; Untch, M.; Smith, I.E.; Gianni, L.; Baselga, J.; et al. Trastuzumab-Associated Cardiac Events at 8 Years of Median Follow-Up in the Herceptin Adjuvant Trial (BIG 1-01). J. Clin. Oncol. 2014, 32, 2159–2165. [Google Scholar] [CrossRef]
- Goldhirsch, A.; Gelber, R.D.; Piccart-Gebhart, M.J.; De Azambuja, E.; Procter, M.; Suter, T.M.; Jackisch, C.; Cameron, D.; Weber, H.A.; Heinzmann, D.; et al. 2 Years versus 1 Year of Adjuvant Trastuzumab for HER2-Positive Breast Cancer (HERA): An Open-Label, Randomised Controlled Trial. Lancet 2013, 382, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Romond, E.H.; Jeong, J.-H.; Rastogi, P.; Swain, S.M.; Geyer, C.E.; Ewer, M.S.; Rathi, V.; Fehrenbacher, L.; Brufsky, A.; Azar, C.A.; et al. Seven-Year Follow-Up Assessment of Cardiac Function in NSABP B-31, a Randomized Trial Comparing Doxorubicin and Cyclophosphamide Followed by Paclitaxel (ACP) With ACP Plus Trastuzumab As Adjuvant Therapy for Patients With Node-Positive, Human Epidermal Growth Factor Receptor 2–Positive Breast Cancer. J. Clin. Oncol. 2012, 30, 3792–3799. [Google Scholar] [CrossRef]
- Advani, P.P.; Ballman, K.V.; Dockter, T.J.; Colon-Otero, G.; Perez, E.A. Long-Term Cardiac Safety Analysis of NCCTG N9831 (Alliance) Adjuvant Trastuzumab Trial. J. Clin. Oncol. 2016, 34, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Kitani, T.; Ong, S.-G.; Lam, C.K.; Rhee, J.-W.; Zhang, J.Z.; Oikonomopoulos, A.; Ma, N.; Tian, L.; Lee, J.; Telli, M.L.; et al. Human-Induced Pluripotent Stem Cell Model of Trastuzumab-Induced Cardiac Dysfunction in Patients with Breast Cancer. Circulation 2019, 139, 2451–2465. [Google Scholar] [CrossRef]
- Crone, S.A.; Zhao, Y.-Y.; Fan, L.; Gu, Y.; Minamisawa, S.; Liu, Y.; Peterson, K.L.; Chen, J.; Kahn, R.; Condorelli, G.; et al. ErbB2 Is Essential in the Prevention of Dilated Cardiomyopathy. Nat. Med. 2002, 8, 459–465. [Google Scholar] [CrossRef]
- Özcelik, C.; Erdmann, B.; Pilz, B.; Wettschureck, N.; Britsch, S.; Hübner, N.; Chien, K.R.; Birchmeier, C.; Garratt, A.N. Conditional Mutation of the ErbB2 (HER2) Receptor in Cardiomyocytes Leads to Dilated Cardiomyopathy. Proc. Natl. Acad. Sci. USA 2002, 99, 8880–8885. [Google Scholar] [CrossRef]
- De Azambuja, E.; Bedard, P.L.; Suter, T.; Piccart-Gebhart, M. Cardiac Toxicity with Anti-HER-2 Therapies-What Have We Learned so Far? Target. Oncol. 2009, 4, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Touyz, R.M.; Herrmann, J. Cardiotoxicity with Vascular Endothelial Growth Factor Inhibitor Therapy. NPJ Precis. Oncol. 2018, 2, 13. [Google Scholar] [CrossRef]
- Abdel-Qadir, H.; Ethier, J.-L.; Lee, D.S.; Thavendiranathan, P.; Amir, E. Cardiovascular Toxicity of Angiogenesis Inhibitors in Treatment of Malignancy: A Systematic Review and Meta-Analysis. Cancer Treat. Rev. 2017, 53, 120–127. [Google Scholar] [CrossRef]
- Cameron, D.; Brown, J.; Dent, R.; Jackisch, C.; Mackey, J.; Pivot, X.; Steger, G.G.; Suter, T.M.; Toi, M.; Parmar, M.; et al. Adjuvant Bevacizumab-Containing Therapy in Triple-Negative Breast Cancer (BEATRICE): Primary Results of a Randomised, Phase 3 Trial. Lancet Oncol. 2013, 14, 933–942. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Mayer, E.L.; Je, Y.; Rosenberg, J.E.; Nguyen, P.L.; Azzi, G.R.; Bellmunt, J.; Burstein, H.J.; Schutz, F.A.B. Congestive Heart Failure Risk in Patients with Breast Cancer Treated With Bevacizumab. J. Clin. Oncol. 2011, 29, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Hutson, T.E.; Cella, D.; Reeves, J.; Hawkins, R.; Guo, J.; Nathan, P.; Staehler, M.; De Souza, P.; Merchan, J.R.; et al. Pazopanib versus Sunitinib in Metastatic Renal-Cell Carcinoma. N. Engl. J. Med. 2013, 369, 722–731. [Google Scholar] [CrossRef]
- Chu, T.F.; Rupnick, M.A.; Kerkela, R.; Dallabrida, S.M.; Zurakowski, D.; Nguyen, L.; Woulfe, K.; Pravda, E.; Cassiola, F.; Desai, J.; et al. Cardiotoxicity Associated with Tyrosine Kinase Inhibitor Sunitinib. Lancet 2007, 370, 2011–2019. [Google Scholar] [CrossRef]
- Richards, C.J.; Je, Y.; Schutz, F.A.B.; Heng, D.Y.C.; Dallabrida, S.M.; Moslehi, J.J.; Choueiri, T.K. Incidence and Risk of Congestive Heart Failure in Patients with Renal and Nonrenal Cell Carcinoma Treated With Sunitinib. J. Clin. Oncol. 2011, 29, 3450–3456. [Google Scholar] [CrossRef] [PubMed]
- Ewer, M.S.; Suter, T.M.; Lenihan, D.J.; Niculescu, L.; Breazna, A.; Demetri, G.D.; Motzer, R.J. Cardiovascular Events among 1090 Cancer Patients Treated with Sunitinib, Interferon, or Placebo: A Comprehensive Adjudicated Database Analysis Demonstrating Clinically Meaningful Reversibility of Cardiac Events. Eur. J. Cancer 2014, 50, 2162–2170. [Google Scholar] [CrossRef]
- Qi, W.; Shen, Z.; Tang, L.; Yao, Y. Congestive Heart Failure Risk in Cancer Patients Treated with Vascular Endothelial Growth Factor Tyrosine Kinase Inhibitors: A Systematic Review and Meta-analysis of 36 Clinical Trials. Br. J. Clin. Pharmacol. 2014, 78, 748–762. [Google Scholar] [CrossRef]
- Maurea, N.; Coppola, C.; Piscopo, G.; Galletta, F.; Riccio, G.; Esposito, E.; De Lorenzo, C.; De Laurentiis, M.; Spallarossa, P.; Mercuro, G. Pathophysiology of Cardiotoxicity from Target Therapy and Angiogenesis Inhibitors. J. Cardiovasc. Med. 2016, 17, e19–e26. [Google Scholar] [CrossRef]
- Force, T.; Krause, D.S.; Van Etten, R.A. Molecular Mechanisms of Cardiotoxicity of Tyrosine Kinase Inhibition. Nat. Rev. Cancer 2007, 7, 332–344. [Google Scholar] [CrossRef]
- Verweij, J.; Casali, P.G.; Kotasek, D.; Le Cesne, A.; Reichard, P.; Judson, I.R.; Issels, R.; Van Oosterom, A.T.; Van Glabbeke, M.; Blay, J.-Y. Imatinib Does Not Induce Cardiac Left Ventricular Failure in Gastrointestinal Stromal Tumours Patients: Analyis of EORTC-ISG-AGITG Study 62005. Eur. J. Cancer 2007, 43, 974–978. [Google Scholar] [CrossRef] [PubMed]
- Druker, B.J.; Guilhot, F.; O’Brien, S.G.; Gathmann, I.; Kantarjian, H.; Gattermann, N.; Deininger, M.W.N.; Silver, R.T.; Goldman, J.M.; Stone, R.M.; et al. Five-Year Follow-up of Patients Receiving Imatinib for Chronic Myeloid Leukemia. N. Engl. J. Med. 2006, 355, 2408–2417. [Google Scholar] [CrossRef]
- Moslehi, J.J. Cardiovascular Toxic Effects of Targeted Cancer Therapies. N. Engl. J. Med. 2016, 375, 1457–1467. [Google Scholar] [CrossRef]
- Barber, M.C.; Mauro, M.J.; Moslehi, J. Cardiovascular Care of Patients with Chronic Myeloid Leukemia (CML) on Tyrosine Kinase Inhibitor (TKI) Therapy. Hematology 2017, 2017, 110–114. [Google Scholar] [CrossRef]
- Sestier, M.; Hillis, C.; Fraser, G.; Leong, D. Bruton’s Tyrosine Kinase Inhibitors and Cardiotoxicity: More Than Just Atrial Fibrillation. Curr. Oncol. Rep. 2021, 23, 113. [Google Scholar] [CrossRef]
- Salem, J.-E.; Manouchehri, A.; Bretagne, M.; Lebrun-Vignes, B.; Groarke, J.D.; Johnson, D.B.; Yang, T.; Reddy, N.M.; Funck-Brentano, C.; Brown, J.R.; et al. Cardiovascular Toxicities Associated With Ibrutinib. J. Am. Coll. Cardiol. 2019, 74, 1667–1678. [Google Scholar] [CrossRef]
- Abdel-Qadir, H.; Sabrie, N.; Leong, D.; Pang, A.; Austin, P.C.; Prica, A.; Nanthakumar, K.; Calvillo-Argüelles, O.; Lee, D.S.; Thavendiranathan, P. Cardiovascular Risk Associated With Ibrutinib Use in Chronic Lymphocytic Leukemia: A Population-Based Cohort Study. J. Clin. Oncol. 2021, 39, 3453–3462. [Google Scholar] [CrossRef]
- Quartermaine, C.; Ghazi, S.M.; Yasin, A.; Awan, F.T.; Fradley, M.; Wiczer, T.; Kalathoor, S.; Ferdousi, M.; Krishan, S.; Habib, A.; et al. Cardiovascular Toxicities of BTK Inhibitors in Chronic Lymphocytic Leukemia: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncology 2023, 5, 570–590. [Google Scholar] [CrossRef]
- Brown, J.R.; Byrd, J.C.; Ghia, P.; Sharman, J.P.; Hillmen, P.; Stephens, D.M.; Sun, C.; Jurczak, W.; Pagel, J.M.; Ferrajoli, A.; et al. Cardiovascular Adverse Events in Patients with Chronic Lymphocytic Leukemia Receiving Acalabrutinib Monotherapy: Pooled Analysis of 762 Patients. Haematologica 2021, 107, 1335–1346. [Google Scholar] [CrossRef]
- Dimopoulos, M.A.; Moreau, P.; Palumbo, A.; Joshua, D.; Pour, L.; Hájek, R.; Facon, T.; Ludwig, H.; Oriol, A.; Goldschmidt, H.; et al. Carfilzomib and Dexamethasone versus Bortezomib and Dexamethasone for Patients with Relapsed or Refractory Multiple Myeloma (ENDEAVOR): A Randomised, Phase 3, Open-Label, Multicentre Study. Lancet Oncol. 2016, 17, 27–38. [Google Scholar] [CrossRef]
- Das, A.; Dasgupta, S.; Gong, Y.; Shah, U.A.; Fradley, M.G.; Cheng, R.K.; Roy, B.; Guha, A. Cardiotoxicity as an Adverse Effect of Immunomodulatory Drugs and Proteasome Inhibitors in Multiple Myeloma: A Network Meta-analysis of Randomized Clinical Trials. Hematol. Oncol. 2022, 40, 233–242. [Google Scholar] [CrossRef]
- Georgiopoulos, G.; Makris, N.; Laina, A.; Theodorakakou, F.; Briasoulis, A.; Trougakos, I.P.; Dimopoulos, M.-A.; Kastritis, E.; Stamatelopoulos, K. Cardiovascular Toxicity of Proteasome Inhibitors: Underlying Mechanisms and Management Strategies. JACC CardioOncology 2023, 5, 1–21. [Google Scholar] [CrossRef]
- Waxman, A.J.; Clasen, S.; Hwang, W.-T.; Garfall, A.; Vogl, D.T.; Carver, J.; O’Quinn, R.; Cohen, A.D.; Stadtmauer, E.A.; Ky, B.; et al. Carfilzomib-Associated Cardiovascular Adverse Events: A Systematic Review and Meta-Analysis. JAMA Oncol. 2018, 4, e174519. [Google Scholar] [CrossRef] [PubMed]
- Russell, S.D.; Lyon, A.; Lenihan, D.J.; Moreau, P.; Joshua, D.; Chng, W.-J.; Palumbo, A.; Goldschmidt, H.; Hájek, R.; Facon, T.; et al. Serial Echocardiographic Assessment of Patients (Pts) with Relapsed Multiple Myeloma (RMM) Receiving Carfilzomib and Dexamethasone (Kd) Vs Bortezomib and Dexamethasone (Vd): A Substudy of the Phase 3 Endeavor Trial (NCT01568866). Blood 2015, 126, 4250. [Google Scholar] [CrossRef]
- Glen, C.; Tan, Y.Y.; Waterston, A.; Evans, T.R.J.; Jones, R.J.; Petrie, M.C.; Lang, N.N. Mechanistic and Clinical Overview Cardiovascular Toxicity of BRAF and MEK Inhibitors. JACC CardioOncology 2022, 4, 1–18. [Google Scholar] [CrossRef]
- Mincu, R.I.; Mahabadi, A.A.; Michel, L.; Mrotzek, S.M.; Schadendorf, D.; Rassaf, T.; Totzeck, M. Cardiovascular Adverse Events Associated With BRAF and MEK Inhibitors: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2019, 2, e198890. [Google Scholar] [CrossRef]
- Bronte, E.; Bronte, G.; Novo, G.; Rinaldi, G.; Bronte, F.; Passiglia, F.; Russo, A. Cardiotoxicity Mechanisms of the Combination of BRAF-Inhibitors and MEK-Inhibitors. Pharmacol. Ther. 2018, 192, 65–73. [Google Scholar] [CrossRef]
- Lyon, A.R.; Dent, S.; Stanway, S.; Earl, H.; Brezden-Masley, C.; Cohen-Solal, A.; Tocchetti, C.G.; Moslehi, J.J.; Groarke, J.D.; Bergler-Klein, J.; et al. Baseline Cardiovascular Risk Assessment in Cancer Patients Scheduled to Receive Cardiotoxic Cancer Therapies: A Position Statement and New Risk Assessment Tools from the Cardio-Oncology Study Group of the H Eart Failure A Sociation of the European Society of Cardiology in Collaboration with the International Cardio-Oncology Society. Eur. J. Heart Fail. 2020, 22, 1945–1960. [Google Scholar] [CrossRef]
- Chitturi, K.R.; Burns, E.A.; Muhsen, I.N.; Anand, K.; Trachtenberg, B.H. Cardiovascular Risks with Epidermal Growth Factor Receptor (EGFR) Tyrosine Kinase Inhibitors and Monoclonal Antibody Therapy. Curr. Oncol. Rep. 2022, 24, 475–491. [Google Scholar] [CrossRef]
- Anand, K.; Ensor, J.; Trachtenberg, B.; Bernicker, E.H. Osimertinib-Induced Cardiotoxicity. JACC CardioOncology 2019, 1, 172–178. [Google Scholar] [CrossRef]
- Postow, M.A.; Callahan, M.K.; Wolchok, J.D. Immune Checkpoint Blockade in Cancer Therapy. J. Clin. Oncol. 2015, 33, 1974–1982. [Google Scholar] [CrossRef]
- Lyon, A.R.; Yousaf, N.; Battisti, N.M.L.; Moslehi, J.; Larkin, J. Immune Checkpoint Inhibitors and Cardiovascular Toxicity. Lancet Oncol. 2018, 19, e447–e458. [Google Scholar] [CrossRef]
- Rubio-Infante, N.; Ramírez-Flores, Y.A.; Castillo, E.C.; Lozano, O.; García-Rivas, G.; Torre-Amione, G. Cardiotoxicity Associated with Immune Checkpoint Inhibitor Therapy: A Meta-analysis. Eur. J. Heart Fail. 2021, 23, 1739–1747. [Google Scholar] [CrossRef]
- Dolladille, C.; Akroun, J.; Morice, P.-M.; Dompmartin, A.; Ezine, E.; Sassier, M.; Da-Silva, A.; Plane, A.-F.; Legallois, D.; L’Orphelin, J.-M.; et al. Cardiovascular Immunotoxicities Associated with Immune Checkpoint Inhibitors: A Safety Meta-Analysis. Eur. Heart J. 2021, 42, 4964–4977. [Google Scholar] [CrossRef]
- Escudier, M.; Cautela, J.; Malissen, N.; Ancedy, Y.; Orabona, M.; Pinto, J.; Monestier, S.; Grob, J.-J.; Scemama, U.; Jacquier, A.; et al. Clinical Features, Management, and Outcomes of Immune Checkpoint Inhibitor–Related Cardiotoxicity. Circulation 2017, 136, 2085–2087. [Google Scholar] [CrossRef] [PubMed]
- Dolladille, C.; Ederhy, S.; Allouche, S.; Dupas, Q.; Gervais, R.; Madelaine, J.; Sassier, M.; Plane, A.-F.; Comoz, F.; Cohen, A.A.; et al. Late Cardiac Adverse Events in Patients with Cancer Treated with Immune Checkpoint Inhibitors. J. Immunother. Cancer 2020, 8, e000261. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, M.; Nielsen, D.; Svane, I.M.; Iversen, K.; Rasmussen, P.V.; Madelaire, C.; Fosbøl, E.; Køber, L.; Gustafsson, F.; Andersson, C.; et al. The Risk of Cardiac Events in Patients Receiving Immune Checkpoint Inhibitors: A Nationwide Danish Study. Eur. Heart J. 2021, 42, 1621–1631. [Google Scholar] [CrossRef]
- Lancellotti, P.; Suter, T.M.; López-Fernández, T.; Galderisi, M.; Lyon, A.R.; Van Der Meer, P.; Cohen Solal, A.; Zamorano, J.-L.; Jerusalem, G.; Moonen, M.; et al. Cardio-Oncology Services: Rationale, Organization, and Implementation. Eur. Heart J. 2019, 40, 1756–1763. [Google Scholar] [CrossRef] [PubMed]
- Bosch, X.; Rovira, M.; Sitges, M.; Domènech, A.; Ortiz-Pérez, J.T.; De Caralt, T.M.; Morales-Ruiz, M.; Perea, R.J.; Monzó, M.; Esteve, J. Enalapril and Carvedilol for Preventing Chemotherapy-Induced Left Ventricular Systolic Dysfunction in Patients With Malignant Hemopathies. J. Am. Coll. Cardiol. 2013, 61, 2355–2362. [Google Scholar] [CrossRef]
- Gulati, G.; Heck, S.L.; Ree, A.H.; Hoffmann, P.; Schulz-Menger, J.; Fagerland, M.W.; Gravdehaug, B.; Von Knobelsdorff-Brenkenhoff, F.; Bratland, Å.; Storås, T.H.; et al. Prevention of Cardiac Dysfunction during Adjuvant Breast Cancer Therapy (PRADA): A 2 × 2 Factorial, Randomized, Placebo-Controlled, Double-Blind Clinical Trial of Candesartan and Metoprolol. Eur. Heart J. 2016, 37, 1671–1680. [Google Scholar] [CrossRef] [PubMed]
- Guglin, M.; Krischer, J.; Tamura, R.; Fink, A.; Bello-Matricaria, L.; McCaskill-Stevens, W.; Munster, P.N. Randomized Trial of Lisinopril Versus Carvedilol to Prevent Trastuzumab Cardiotoxicity in Patients With Breast Cancer. J. Am. Coll. Cardiol. 2019, 73, 2859–2868. [Google Scholar] [CrossRef]
- Fang, K.; Zhang, Y.; Liu, W.; He, C. Effects of Angiotensin-Converting Enzyme Inhibitor/Angiotensin Receptor Blocker Use on Cancer Therapy-Related Cardiac Dysfunction: A Meta-Analysis of Randomized Controlled Trials. Heart Fail. Rev. 2021, 26, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Yao, L.; Wang, M.; Wang, M.; Li, X.; Sun, X.; Yu, X.; Guo, J.; Li, X.; Xu, Y. Can ACEI/ARB Prevent the Cardiotoxicity Caused by Chemotherapy in Early-Stage Breast Cancer?—A Meta-Analysis of Randomized Controlled Trials. Transl. Cancer Res. 2020, 9, 7034–7043. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, P.A.; Hall, P.; MacPherson, I.R.; Joshi, S.S.; Singh, T.; Maclean, M.; Lewis, S.; Rodriguez, A.; Fletcher, A.; Everett, R.J.; et al. Multicenter, Prospective, Randomized Controlled Trial of High-Sensitivity Cardiac Troponin I–Guided Combination Angiotensin Receptor Blockade and Beta-Blocker Therapy to Prevent Anthracycline Cardiotoxicity: The Cardiac CARE Trial. Circulation 2023, 148, 1680–1690. [Google Scholar] [CrossRef] [PubMed]
- Alizadehasl, A.; Ghadimi, N.; Kaveh, S.; Maleki, M.; Ghavamzadeh, A.; Noohi, F.; Hosseinifard, H. Prevention of Anthracycline-Induced Cardiotoxicity: A Systematic Review and Network Meta-Analysis. Int. J. Clin. Pharm. 2021, 43, 25–34. [Google Scholar] [CrossRef]
- Huang, S.; Zhao, Q.; Yang, Z.; Diao, K.; He, Y.; Shi, K.; Shen, M.; Fu, H.; Guo, Y. Protective Role of Beta-Blockers in Chemotherapy-Induced Cardiotoxicity—A Systematic Review and Meta-Analysis of Carvedilol. Heart Fail. Rev. 2019, 24, 325–333. [Google Scholar] [CrossRef]
- Pituskin, E.; Mackey, J.R.; Koshman, S.; Jassal, D.; Pitz, M.; Haykowsky, M.J.; Pagano, J.J.; Chow, K.; Thompson, R.B.; Vos, L.J.; et al. Multidisciplinary Approach to Novel Therapies in Cardio-Oncology Research (MANTICORE 101–Breast): A Randomized Trial for the Prevention of Trastuzumab-Associated Cardiotoxicity. J. Clin. Oncol. 2017, 35, 870–877. [Google Scholar] [CrossRef] [PubMed]
- Tajstra, M.; Dyrbuś, M.; Rutkowski, T.; Składowski, K.; Sosnowska-Pasiarska, B.; Góźdź, S.; Radecka, B.; Staszewski, M.; Majsnerowska, A.; Myrda, K.; et al. Sacubitril/Valsartan for Cardioprotection in Breast Cancer (MAINSTREAM): Design and Rationale of the Randomized Trial. ESC Heart Fail. 2023, 10, 3174–3183. [Google Scholar] [CrossRef] [PubMed]
- Avagimyan, A.; Sheibani, M.; Pogosova, N.; Mkrtchyan, L.; Yeranosyan, H.; Aznauryan, A.; Sahaakyan, K.; Fogacci, F.; Cicero, A.; Shafie, D.; et al. Possibilities of Dapagliflozin-Induced Cardioprotection on Doxorubicin + Cyclophosphamide Mode of Chemotherapy-Induced Cardiomyopathy. Int. J. Cardiol. 2023, 391, 131331. [Google Scholar] [CrossRef] [PubMed]
- Barış, V.Ö.; Dinçsoy, A.B.; Gedikli, E.; Zırh, S.; Müftüoğlu, S.; Erdem, A. Empagliflozin Significantly Prevents the Doxorubicin-Induced Acute Cardiotoxicity via Non-Antioxidant Pathways. Cardiovasc. Toxicol. 2021, 21, 747–758. [Google Scholar] [CrossRef]
- Cvetković, R.S.; Scott, L.J. Dexrazoxane: A Review of Its Use for Cardioprotection during Anthracycline Chemotherapy. Drugs 2005, 65, 1005–1024. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, P.A. Anthracycline Cardiotoxicity: An Update on Mechanisms, Monitoring and Prevention. Heart 2018, 104, 971–977. [Google Scholar] [CrossRef]
- Macedo, A.V.S.; Hajjar, L.A.; Lyon, A.R.; Nascimento, B.R.; Putzu, A.; Rossi, L.; Costa, R.B.; Landoni, G.; Nogueira-Rodrigues, A.; Ribeiro, A.L.P. Efficacy of Dexrazoxane in Preventing Anthracycline Cardiotoxicity in Breast Cancer. JACC CardioOncology 2019, 1, 68–79. [Google Scholar] [CrossRef]
- Neilan, T.G.; Quinaglia, T.; Onoue, T.; Mahmood, S.S.; Drobni, Z.D.; Gilman, H.K.; Smith, A.; Heemelaar, J.C.; Brahmbhatt, P.; Ho, J.S.; et al. Atorvastatin for Anthracycline-Associated Cardiac Dysfunction: The STOP-CA Randomized Clinical Trial. JAMA 2023, 330, 528. [Google Scholar] [CrossRef] [PubMed]
- Onoue, T.; Kang, Y.; Lefebvre, B.; Smith, A.M.; Denduluri, S.; Carver, J.; Fradley, M.G.; Chittams, J.; Scherrer-Crosbie, M. The Association of Metformin With Heart Failure in Patients With Diabetes Mellitus Receiving Anthracycline Chemotherapy. JACC CardioOncology 2023, 5, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Zamorano, J.L.; Gottfridsson, C.; Asteggiano, R.; Atar, D.; Badimon, L.; Bax, J.J.; Cardinale, D.; Cardone, A.; Feijen, E.A.M.; Ferdinandy, P.; et al. The Cancer Patient and Cardiology. Eur. J. Heart Fail. 2020, 22, 2290–2309. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Lenihan, D.; Fradley, M.; Ganatra, S.; Barac, A.; Blaes, A.; Herrmann, J.; Porter, C.; Lyon, A.R.; Lancellotti, P.; et al. Management of Cardiac Disease in Cancer Patients throughout Oncological Treatment: ESMO Consensus Recommendations. Ann. Oncol. 2020, 31, 171–190. [Google Scholar] [CrossRef] [PubMed]
- Plana, J.C.; Thavendiranathan, P.; Bucciarelli-Ducci, C.; Lancellotti, P. Multi-Modality Imaging in the Assessment of Cardiovascular Toxicity in the Cancer Patient. JACC Cardiovasc. Imaging 2018, 11, 1173–1186. [Google Scholar] [CrossRef] [PubMed]
- Waliany, S.; Zhu, H.; Wakelee, H.; Padda, S.K.; Das, M.; Ramchandran, K.; Myall, N.J.; Chen, T.; Witteles, R.M.; Neal, J.W. Pharmacovigilance Analysis of Cardiac Toxicities Associated With Targeted Therapies for Metastatic NSCLC. J. Thorac. Oncol. 2021, 16, 2029–2039. [Google Scholar] [CrossRef]
- Vallabhaneni, S.; Zhang, K.W.; Alvarez-Cardona, J.A.; Mitchell, J.D.; Steen, H.; Woodard, P.K.; Lenihan, D.J. Role of Cardiovascular Magnetic Resonance in Early Detection and Treatment of Cardiac Dysfunction in Oncology Patients. Int. J. Cardiovasc. Imaging 2021, 37, 3003–3017. [Google Scholar] [CrossRef]
- Giusca, S.; Korosoglou, G.; Montenbruck, M.; Geršak, B.; Schwarz, A.K.; Esch, S.; Kelle, S.; Wülfing, P.; Dent, S.; Lenihan, D.; et al. Multiparametric Early Detection and Prediction of Cardiotoxicity Using Myocardial Strain, T1 and T2 Mapping, and Biochemical Markers: A Longitudinal Cardiac Resonance Imaging Study During 2 Years of Follow-Up. Circ. Cardiovasc. Imaging 2021, 14, e012459. [Google Scholar] [CrossRef]
- Mousavi, N.; Tan, T.C.; Ali, M.; Halpern, E.F.; Wang, L.; Scherrer-Crosbie, M. Echocardiographic Parameters of Left Ventricular Size and Function as Predictors of Symptomatic Heart Failure in Patients with a Left Ventricular Ejection Fraction of 50–59% Treated with Anthracyclines. Eur. Heart J.-Cardiovasc. Imaging 2015, 16, jev113. [Google Scholar] [CrossRef] [PubMed]
- Araujo-Gutierrez, R.; Chitturi, K.R.; Xu, J.; Wang, Y.; Kinder, E.; Senapati, A.; Chebrolu, L.B.; Kassi, M.; Trachtenberg, B.H. Baseline Global Longitudinal Strain Predictive of Anthracycline-Induced Cardiotoxicity. Cardio-Oncology 2021, 7, 4. [Google Scholar] [CrossRef] [PubMed]
- Van Der Linde, D.; Van Hagen, I.; Veen, K.; Zuetenhorst, H.; Van Dalen, B. Global Longitudinal Strain: An Early Marker for Cardiotoxicity in Patients Treated for Breast Cancer. Neth. Heart J. 2023, 31, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Oikonomou, E.K.; Kokkinidis, D.G.; Kampaktsis, P.N.; Amir, E.A.; Marwick, T.H.; Gupta, D.; Thavendiranathan, P. Assessment of Prognostic Value of Left Ventricular Global Longitudinal Strain for Early Prediction of Chemotherapy-Induced Cardiotoxicity: A Systematic Review and Meta-Analysis. JAMA Cardiol. 2019, 4, 1007. [Google Scholar] [CrossRef]
- Negishi, T.; Thavendiranathan, P.; Penicka, M.; Lemieux, J.; Murbraech, K.; Miyazaki, S.; Shirazi, M.; Santoro, C.; Cho, G.-Y.; Popescu, B.A.; et al. Cardioprotection Using Strain-Guided Management of Potentially Cardiotoxic Cancer Therapy: 3-Year Results of the SUCCOUR Trial. JACC Cardiovasc. Imaging 2023, 16, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Pudil, R.; Mueller, C.; Čelutkienė, J.; Henriksen, P.A.; Lenihan, D.; Dent, S.; Barac, A.; Stanway, S.; Moslehi, J.; Suter, T.M.; et al. Role of serum biomarkers in cancer patients receiving cardiotoxic cancer therapies: A position statement from the Cardio-Oncology Study Group of the Heart Failure Association and the Cardio-Oncology Council of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 1966–1983. [Google Scholar] [CrossRef] [PubMed]
- Michel, L.; Mincu, R.I.; Mahabadi, A.A.; Settelmeier, S.; Al-Rashid, F.; Rassaf, T.; Totzeck, M. Troponins and Brain Natriuretic Peptides for the Prediction of Cardiotoxicity in Cancer Patients: A Meta-analysis. Eur. J. Heart Fail. 2020, 22, 350–361. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Pareek, N.; Cevallos, J.; Moliner, P.; Shah, M.; Tan, L.L.; Chambers, V.; Baksi, A.J.; Khattar, R.S.; Sharma, R.; Rosen, S.D.; et al. Activity and Outcomes of a Cardio-oncology Service in the United Kingdom—A Five-year Experience. Eur. J. Heart Fail. 2018, 20, 1721–1731. [Google Scholar] [CrossRef] [PubMed]
- Martín-Garcia, A.; López-Fernández, T.; Mitroi, C.; Chaparro-Muñoz, M.; Moliner, P.; Martin-Garcia, A.C.; Martinez-Monzonis, A.; Castro, A.; Lopez-Sendon, J.L.; Sanchez, P.L. Effectiveness of Sacubitril-Valsartan in Cancer Patients with Heart Failure. ESC Heart Fail. 2020, 7, 763–767. [Google Scholar] [CrossRef] [PubMed]
- Hussain, Y.; Drill, E.; Dang, C.T.; Liu, J.E.; Steingart, R.M.; Yu, A.F. Cardiac Outcomes of Trastuzumab Therapy in Patients with HER2-Positive Breast Cancer and Reduced Left Ventricular Ejection Fraction. Breast Cancer Res. Treat. 2019, 175, 239–246. [Google Scholar] [CrossRef]
- Ewer, M.S.; Vooletich, M.T.; Durand, J.-B.; Woods, M.L.; Davis, J.R.; Valero, V.; Lenihan, D.J. Reversibility of Trastuzumab-Related Cardiotoxicity: New Insights Based on Clinical Course and Response to Medical Treatment. J. Clin. Oncol. 2005, 23, 7820–7826. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.P.; Solomon, S.D.; Fradley, M.G.; Barac, A.; Kremer, K.A.; Beck, C.A.; Brown, M.W.; McNitt, S.; Schleede, S.; Zareba, W.; et al. Association of Cardiac Resynchronization Therapy with Change in Left Ventricular Ejection Fraction in Patients With Chemotherapy-Induced Cardiomyopathy. JAMA 2019, 322, 1799. [Google Scholar] [CrossRef] [PubMed]
- Christensen, A.M.; Bjerre, J.; Schou, M.; Jons, C.; Vinther, M.; Gislason, G.H.; Johansen, J.B.; Nielsen, J.C.; Petersen, H.H.; Riahi, S.; et al. Clinical Outcome in Patients with Implantable Cardioverter-Defibrillator and Cancer: A Nationwide Study. EP Europace 2019, 21, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Knops, R.E.; Olde Nordkamp, L.R.A.; Delnoy, P.-P.H.M.; Boersma, L.V.A.; Kuschyk, J.; El-Chami, M.F.; Bonnemeier, H.; Behr, E.R.; Brouwer, T.F.; Kääb, S.; et al. Subcutaneous or Transvenous Defibrillator Therapy. N. Engl. J. Med. 2020, 383, 526–536. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, G.H.; Dupont, M.; Naftel, D.; Myers, S.L.; Yuan, Y.; Tang, W.H.W.; Gonzalez-Stawinski, G.; Young, J.B.; Taylor, D.O.; Starling, R.C. Increased Need for Right Ventricular Support in Patients With Chemotherapy-Induced Cardiomyopathy Undergoing Mechanical Circulatory Support. J. Am. Coll. Cardiol. 2014, 63, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, G.H.; Qattan, M.Y.; Al-Kindi, S.; Park, S.J. Advanced Heart Failure Therapies for Patients With Chemotherapy-Induced Cardiomyopathy. Circ. Heart Fail. 2014, 7, 1050–1058. [Google Scholar] [CrossRef]
- Oliveira, G.H.; Hardaway, B.W.; Kucheryavaya, A.Y.; Stehlik, J.; Edwards, L.B.; Taylor, D.O. Characteristics and Survival of Patients with Chemotherapy-Induced Cardiomyopathy Undergoing Heart Transplantation. J. Heart Lung Transplant. 2012, 31, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Lenneman, A.J.; Wang, L.; Wigger, M.; Frangoul, H.; Harrell, F.E.; Silverstein, C.; Sawyer, D.B.; Lenneman, C.G. Heart Transplant Survival Outcomes for Adriamycin-Dilated Cardiomyopathy. Am. J. Cardiol. 2013, 111, 609–612. [Google Scholar] [CrossRef] [PubMed]
- DePasquale, E.C.; Nasir, K.; Jacoby, D.L. Outcomes of Adults with Restrictive Cardiomyopathy after Heart Transplantation. J. Heart Lung Transplant. 2012, 31, 1269–1275. [Google Scholar] [CrossRef]
- Oeffinger, K.C.; Mertens, A.C.; Sklar, C.A.; Kawashima, T.; Hudson, M.M.; Meadows, A.T.; Friedman, D.L.; Marina, N.; Hobbie, W.; Kadan-Lottick, N.S.; et al. Chronic Health Conditions in Adult Survivors of Childhood Cancer. N. Engl. J. Med. 2006, 355, 1572–1582. [Google Scholar] [CrossRef]
- Fidler, M.M.; Reulen, R.C.; Henson, K.; Kelly, J.; Cutter, D.; Levitt, G.A.; Frobisher, C.; Winter, D.L.; Hawkins, M.M. Population-Based Long-Term Cardiac-Specific Mortality Among 34 489 Five-Year Survivors of Childhood Cancer in Great Britain. Circulation 2017, 135, 951–963. [Google Scholar] [CrossRef] [PubMed]
- Geenen, M.M.; Cardous-Ubbink, M.C.; Kremer, L.C.M.; Van Den Bos, C.; Van Der Pal, H.J.H.; Heinen, R.C.; Jaspers, M.W.M.; Koning, C.C.E.; Oldenburger, F.; Langeveld, N.E.; et al. Medical Assessment of Adverse Health Outcomes in Long-Term Survivors of Childhood Cancer. JAMA 2007, 297, 2705. [Google Scholar] [CrossRef] [PubMed]
- Armenian, S.H.; Xu, L.; Ky, B.; Sun, C.; Farol, L.T.; Pal, S.K.; Douglas, P.S.; Bhatia, S.; Chao, C. Cardiovascular Disease Among Survivors of Adult-Onset Cancer: A Community-Based Retrospective Cohort Study. J. Clin. Oncol. 2016, 34, 1122–1130. [Google Scholar] [CrossRef] [PubMed]
- Armenian, S.H.; Hudson, M.M.; Mulder, R.L.; Chen, M.H.; Constine, L.S.; Dwyer, M.; Nathan, P.C.; Tissing, W.J.E.; Shankar, S.; Sieswerda, E.; et al. Recommendations for Cardiomyopathy Surveillance for Survivors of Childhood Cancer: A Report from the International Late Effects of Childhood Cancer Guideline Harmonization Group. Lancet Oncol. 2015, 16, e123–e136. [Google Scholar] [CrossRef] [PubMed]
- Leerink, J.M.; Van Der Pal, H.J.H.; Kremer, L.C.M.; Feijen, E.A.M.; Meregalli, P.G.; Pourier, M.S.; Merkx, R.; Bellersen, L.; Van Dalen, E.C.; Loonen, J.; et al. Refining the 10-Year Prediction of Left Ventricular Systolic Dysfunction in Long-Term Survivors of Childhood Cancer. JACC CardioOncology 2021, 3, 62–72. [Google Scholar] [CrossRef]
- Fardman, A.; Banschick, G.D.; Rabia, R.; Percik, R.; Fourey, D.; Segev, S.; Klempfner, R.; Grossman, E.; Maor, E. Cardiorespiratory Fitness and Survival Following Cancer Diagnosis. Eur. J. Prev. Cardiol. 2021, 28, 1242–1249. [Google Scholar] [CrossRef] [PubMed]
- Groarke, J.D.; Payne, D.L.; Claggett, B.; Mehra, M.R.; Gong, J.; Caron, J.; Mahmood, S.S.; Hainer, J.; Neilan, T.G.; Partridge, A.H.; et al. Association of Post-Diagnosis Cardiorespiratory Fitness with Cause-Specific Mortality in Cancer. Eur. Heart J.-Qual. Care Clin. Outcomes 2020, 6, 315–322. [Google Scholar] [CrossRef]
- Scott, J.M.; Zabor, E.C.; Schwitzer, E.; Koelwyn, G.J.; Adams, S.C.; Nilsen, T.S.; Moskowitz, C.S.; Matsoukas, K.; Iyengar, N.M.; Dang, C.T.; et al. Efficacy of Exercise Therapy on Cardiorespiratory Fitness in Patients With Cancer: A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2018, 36, 2297–2305. [Google Scholar] [CrossRef] [PubMed]
- Wallen, M.P.; Hennessy, D.; Brown, S.; Evans, L.; Rawstorn, J.C.; Wong Shee, A.; Hall, A. High-intensity Interval Training Improves Cardiorespiratory Fitness in Cancer Patients and Survivors: A Meta-analysis. Eur. J. Cancer Care 2020, 29, e13267. [Google Scholar] [CrossRef]
- Gilchrist, S.C.; Barac, A.; Ades, P.A.; Alfano, C.M.; Franklin, B.A.; Jones, L.W.; La Gerche, A.; Ligibel, J.A.; Lopez, G.; Madan, K.; et al. Cardio-Oncology Rehabilitation to Manage Cardiovascular Outcomes in Cancer Patients and Survivors: A Scientific Statement from the American Heart Association. Circulation 2019, 139, e997–e1012. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.M.; Stone, C.R.; Cheung, W.Y.; Hayes, S.C. Physical Activity and Mortality in Cancer Survivors: A Systematic Review and Meta-Analysis. JNCI Cancer Spectr. 2020, 4, pkz080. [Google Scholar] [CrossRef]
- Reding, K.W.; Cheng, R.K.; Vasbinder, A.; Ray, R.M.; Barac, A.; Eaton, C.B.; Saquib, N.; Shadyab, A.H.; Simon, M.S.; Langford, D.; et al. Lifestyle and Cardiovascular Risk Factors Associated with Heart Failure Subtypes in Postmenopausal Breast Cancer Survivors. JACC CardioOncology 2022, 4, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Salloum, F.N.; Tocchetti, C.G.; Ameri, P.; Ardehali, H.; Asnani, A.; de Boer, R.A.; Burridge, P.; Cabrera, J.-Á.; de Castro, J.; Córdoba, R.; et al. Priorities in Cardio-Oncology Basic and Translational Science: GCOS 2023 Symposium Proceedings: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncology 2023, 5, 715–731. [Google Scholar] [CrossRef] [PubMed]
- De Boer, R.A.; Hulot, J.; Tocchetti, C.G.; Aboumsallem, J.P.; Ameri, P.; Anker, S.D.; Bauersachs, J.; Bertero, E.; Coats, A.J.S.; Čelutkienė, J.; et al. Common mechanistic pathways in cancer and heart failure. A scientific roadmap on behalf of the Translational Research Committee of the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2020, 22, 2272–2289. [Google Scholar] [CrossRef] [PubMed]
- Omland, T.; Heck, S.L.; Gulati, G. The Role of Cardioprotection in Cancer Therapy Cardiotoxicity. JACC CardioOncology 2022, 4, 19–37. [Google Scholar] [CrossRef] [PubMed]
- Cejas, R.B.; Petrykey, K.; Sapkota, Y.; Burridge, P.W. Anthracycline Toxicity: Light at the End of the Tunnel? Annu. Rev. Pharmacol. Toxicol. 2024, 64, 115–134. [Google Scholar] [CrossRef] [PubMed]
- Lenihan, D.J.; Fradley, M.G.; Dent, S.; Brezden-Masley, C.; Carver, J.; Filho, R.K.; Neilan, T.G.; Blaes, A.; Melloni, C.; Herrmann, J.; et al. Proceedings from the Global Cardio-Oncology Summit. JACC CardioOncology 2019, 1, 256–272. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Symptomatic | ||
|---|---|---|
| Very severe | HF requiring inotropic support, mechanical circulatory support, or transplantation | |
| Severe | HF hospitalization | |
| Moderate | Need for outpatient intensification of diuretic and HF therapy | |
| Mild | Mild HF symptoms, no intensification of therapy required | |
| Asymptomatic | ||
| Severe | New LVEF reduction to >40% | |
| Moderate |
OR
| |
| Mild | LVEF ≥ 50% AND new relative decline in GLS by >15% from baseline AND/OR new rise in cardiac biomarkers |
| Drug Family | Type of Treated Cancer | Cardiotoxicity | Main HF Risk Factors | Percentage of Cardiotoxicity | Citations Author, Journal, Year (Ref.) |
|---|---|---|---|---|---|
| Anthracyclines Doxorubicin Daunorubicin Epirubicin Idarubicin Mitoxantrone | Breast, small-cell lung, bladder, esophagus, stomach, liver and thyroid, leukemias, lymphomas, sarcomas | Cardiomyocytes topoisomerase 2β irreversible inhibition leading to ROS release and myocyte apoptosis. Dose-dependent cardiotoxicity | Previous HF, CTR-CVT, advanced age, previous radiotherapy, previous anthracyclines exposure, LVEF < 50% | 3 to 48% HF incidence, depending on the dose, specific drug, and risk profile of patients | Boeker et al. Br. J. Cancer 2018 [33] Boeker et al. Eur. J. Heart Fail. 2020 [34] Bowles et al. Natl. Cancer Inst. 2012 [35] Jacobse et al. Breast Cancer Res. Treat. 2021 [36] Lotrionte et al. Am. J. Cardiol. 2013 [37] Cardinale et al. Circulation 2015 [38] Von Hoff DD. Ann. Intern. Med. 1979 [39] Swain et al. Cancer 2003 [40] Pinder et al. J. Clin. Oncol. 2007 [41] Thavendiranathan et al. J. Clin. Oncol. 2016 [42] J. Clin. Oncol. 2008 [43] |
| HER-2 inhibitors Antibodies: Trastuzumab, Pertuzumab, TrastuzumaB-emtansine TKI-inhibitors Lapatinib Neratinib Tucatinib | Breast cancers Metastatic gastric adenocarcinoma | Inhibition of the human epidermal receptor 2 leading to mitochondrial dysfunction and impaired contractile LV function, without cardiomyocyte death. Dose-independent, often reversible cardiotoxicity | Previous HF, CTR-CVT, advanced age, previous radiotherapy, previous exposure to trastuzumab, LVEF < 50% | 8.7% incidence of asymptomatic or mildly symptomatic HF; 2.3% incidence of severe HF | Slamon et al. N. Engl. J. Med. 2001 [47] Moja et al. Cochrane Database Syst. Rev. 2012 [48] De Azambuja Breast Cancer Res. Treat. 2020 [49] De Asambuja etal. J. Clin. Oncol. 2014 [51] Goldhirsch et al. The Lancet 2013 [52] Romond et al. J. Clin. Oncol. 2012 [53] Advani et al. J. Clin. Oncol. 2016 [54] Kitani et al. Circulation 2019 [55] |
| VEGF inhibitors Monoclonal antibodies: Bevacizumab TKI-inhibitors Axitinib Cabozantinib Lenvatinib Pazopanib Regorafenib Sorafenib Sunitinib Vandetanib | Solid cancers, such as renal, thyroid, and hepatocellular carcinomas | Endothelial dysfunction and impaired myocardial perfusion, increased afterload | Previous HF, CTR-CVT, previous anthracyclines exposure, VTE or PE, LVEF < 50%, QRS width > 480 msec, age ≥ 75 years, arterial hypertension | Hypertension is the main CV side effect (class effect). HF is common (1–10%) for bevacizumab, axitinib, levantinib, and sorafenib. HF is uncommon (<1%) with the other drugs | Touyz et al. Npj Precis. Oncol. 2018 [59] Abdel-Qadir Cancer Treat. Rev. 2017 [60] Cameron et al. Lancet Oncol. 2013 [61] Choueiri J. Clin. Oncol. 2011 [62] Mozter et al. N. Engl. J. Med. 2013 [63] Chu et al. The Lancet 2007 [64] Richards et al. J. Clin. Oncol. 2011 [65] Ewer et al. Eur. J. Cancer 2014 [66] Qi et al. Br. J. Clin. Pharmacol. 2014 [67] Maurea et al. J. Cardiovasc. Med. 2016 [68] Force et al. Nat. Rev. Cancer 2007 [69] |
| BCR-ABL multi-targeted tyrosine kinase inhibitors 1st generation: Imatinib 2nd generation: Dasatinib, Bosutininb 3rd generation: Ponatinib | Chronic myeloid leukemia | Off-target TKI leading to SERCA dysfunction, mitochondrial dysfunction, and myocyte death; endothelial dysfunction, pulmonary capillary medial hypertrophy, pulmonary infiltrates, and pulmonary hypertension | Previous HF, CTR-CVT, previous anthracyclines exposure, arterial vascular disease, previous arterial thrombosis under TKI, PH, LVEF < 50%, QRS width > 480 msec, age ≥ 75 years, CVD 10-year risk score 0.20%, current smoking | HF is common (1–10%) with dasatininb and ponatininb; uncommon (<1%) with imatininb. Pulmonary hypertension is common with dasatinib and ponatinib; uncommon with bosutininb | Verweij et al. Eur. J. Cancer 2007 [70] Druker et al. N. Engl. J. Med. 2006 [71] Barber et al. Hematology 2017 [73] |
| Bruton tyrosine kinase inhibitors Ibrutininb Acalabrutininb | Chronic lymphocytic leukemia, B-cell malignancies, Waldenström macroglobulinemia, and marginal zone lymphomas | Off-target myocardial TKI leading to myocardial cell disarray, fibrosis, disruptions in calcium signaling, and death | Previous HF/cardiomyopathy, AF, myocardial fibrosis | Up to 7% with ibrutininb; <1% with acalabrutininb | Sestier et al. Curr. Oncol. Rep. 2021 [74] Salem et al. J. Am. Coll. Cardiol. 2019 [75] Abdel-Qadir et al. J. Clin. Oncol. 2021 [76] Quartermaine et al. JACC CardioOncology 2023 [77] Brown et al. Haematologica 2021 [78] |
| Proteasome Inhibitors Bortezomib Carfilzomib | Multiple myeloma | Myocyte proteasome instability, mitochondrial dysfunction, ROS accumulation, genetic instability, sarcomericdysfunction | Previous HF, CTR-CVT, previous anthracyclines exposure, arterial vascular disease, VTE or PE, previous cardiac toxicity under PI or immunomodulators, PH, LVEF < 50%, cardiac amyloidosis, age ≥ 75 years | Up to 10% with carfilzomib + dexamethasome 4% with bortezomib + dexamethasone | Dimopoulos Lancet Oncol. 2016 [79] Das et al. Hematol. Oncol. 2022 [80] Georgiopoulos et al. JACC CardioOncology 2023 [81] Waxman et al. JAMA Oncol. 2018 [82] Russel et al. Blood 2015 [83] |
| BRAF inhibitors Vemurafenib Dabrafeniband Encorafenib MEK inhibitors Trametinib Cobimetinib Binimetinib Selumetinib | BRAF-mutated melanoma | Cardiomyocyte RAF-MEK extracellular signal-regulated kinases (ERKs) pathway modulation. Impact on myocyte hypertrophy, cardiac remodeling, and myocardial cell death | Previous HF, CTR-CVT, previous anthracyclines exposure, LVEF < 50%, cardiac amyloidosis, age ≥ 75 years | 2% to 12% incidence of HF | Glen et al. JACC CardioOncology 2022 [84] Mincu et al. JAMA Netw. Open 2019 [85] Bronte et al. Pharmacol. Ther. 2018 [86] |
| EGFR inhibitors Osimertinib | Non-small-cell lung cancer | Irreversible EGFR-TKI, leading to a cross-inhibition of HER2 as a potential mechanism of cardiotoxicity | Pre-existing hypertension and older age | 5.5% incidence of HF | Chitturi et al. Curr. Oncol. Rep. 2022 [88] Anand et al. JACC CardioOncology 2019 [89] |
| Immune checkpoint inhibitors CTLA-4 blockers: Ipilimumab Tremelimumab PD-1 blockers: Nivolumab Cemiplimab Pembrolizumab PD-L1 blockers Atezolizumab Avelumab Durvalumab | Several kinds of cancers | Overactivation of T cells in the myocardium leading to immune-related adverse events | Dual ICI therapy, combination ICI therapy with other cardiotoxic therapies, and patients with ICI-related non-CV events or prior CTRCD or CVD | 8% incidence of HF | Postow et al. J. Clin. Oncol. 2015 [90] Lyon et al. Lancet Oncol. 2018 [91] Rubio-Infante Eur. J. Heart Fail. 2021 [92] Dolladille et al. Eur. Heart J. 2021 [93] Escudier et al. Circulation 2017 [94] D’Souza et al. Eur. Heart J. 2021 [95] |
| Name of the Trial (If Any) Author, Journal, Year (Ref) | Trial Design | Population | Endpoints | Results |
|---|---|---|---|---|
| OVERCOME trial Bosch et al., JACC, 2013 [98] | Randomized, controlled study | 90 patients with malignant hemopathies needing treatment without LVSD | Absolute change in LVEF in patients receiving carvedilol + enalapril vs. placebo | Candesartan, but not metoprolol, provides protection against early decline in LVEF |
| PRADA trial Gulati et al., European Heart Journal, 2016 [99] | Randomized placebo-controlled, double-blind trial | 130 women with breast cancer receiving anthracyclines with or without trastuzumab assigned to candesartan, metoprolol, or matching placebo | Change in LVEF via cardiac magnetic resonance imaging | Candesartan, but not metoprolol, provides protection against early decline in LVEF |
| Guglin et al. JACC 2019 [100] | Double-blind, multicenter, placebo-controlled trial | 468 women with breast cancer receiving trastuzumab with or without anthracyclines, randomized to receive lisinopril, carvedilol, or placebo | Average change in mean LVEF over time and distribution of cardiotoxicity for each group | Cardiotoxicity-free survival was longer on both carvedilol (hazard ratio: 0.49; 95% confidence interval: 0.27 to 0.89; p ¼ 0.009) and lisinopril (hazard ratio: 0.53; 95% confidence interval: 0.30 to 0.94; p ¼ 0.015) than on placebo |
| CARE trial Henriksen et al. Circulation 2023 [103] | Multicenter, prospective, randomized, open-label, blinded end-point trial | 175 high-risk patients with breast cancer and non-Hodgkin lymphoma receiving anthracycline chemotherapy randomized to carvedilol and candesartan vs. standard care | Adjusted change in left ventricular ejection fraction at 6 months measured at CMR | The estimated mean difference in 6-month left ventricular ejection fraction between the cardioprotection and standard care groups was −0.37% (95% CI, −3.59% to 2.85%; p = 0.82) |
| MANTICORE trial Pituskin et al. J. Clin. Oncol. 2017 [106] | Double-blinded, placebo-controlled trial | 94 patients with HER2-positive early breast cancer were randomly assigned to receive treatment with perindopril, bisoprolol, or placebo (1:1:1) | Change in indexed left ventricular end-diastolic volume and LVEF | Perindopril and bisoprolol prevented changes in LVEF at follow-up (β = 2.594, 95% CI: 0.495–4.693, p = 0.016; β = 4.560, 95% CI: 2.440–6.6800, p < 0.001, respectively) |
| Neilan et al. JAMA 2023 [113] | Double-blind multicenter randomized clinical trial | 300 patients with lymphoma scheduled to receive anthracycline-based chemotherapy were randomized to atorvastatin 40 mg or placebo | Absolute LVEF decline ≥ 10% from before chemotherapy to a final value of <55% over 12 months | Prevalence of the primary endpoint: 9% (13/150) in the atorvastatin group and 22% (33/150) in the placebo group (p = 0.002) |
| Onoue et al. JACC CardioOncology 2023 [114] | Retrospective study applying propensity score matching to compare patients with or without metformin treatment | 315 patients with diabetes receiving anthracyclines for breast cancer | New onset symptomatic HF occurring within 1 year of the initiation of anthracyclines | Metformin was associated with a lower incidence of HF (3.6% vs. 10.5%; p = 0.022; HR: 0.35; 95% CI: 0.14–0.90; p = 0.029) and lower mortality (HR: 0.71; 95% CI:0.50–1.00; p = 0.049) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertolini, D.; Pizzi, C.; Donal, E.; Galli, E. Cancer and Heart Failure: Dangerous Liaisons. J. Cardiovasc. Dev. Dis. 2024, 11, 263. https://doi.org/10.3390/jcdd11090263
Bertolini D, Pizzi C, Donal E, Galli E. Cancer and Heart Failure: Dangerous Liaisons. Journal of Cardiovascular Development and Disease. 2024; 11(9):263. https://doi.org/10.3390/jcdd11090263
Chicago/Turabian StyleBertolini, Davide, Carmine Pizzi, Erwan Donal, and Elena Galli. 2024. "Cancer and Heart Failure: Dangerous Liaisons" Journal of Cardiovascular Development and Disease 11, no. 9: 263. https://doi.org/10.3390/jcdd11090263