
The Effect of Upright Posture on Left Atrial Strain in Competitive Athletes
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Conventional Echocardiographic Parameters
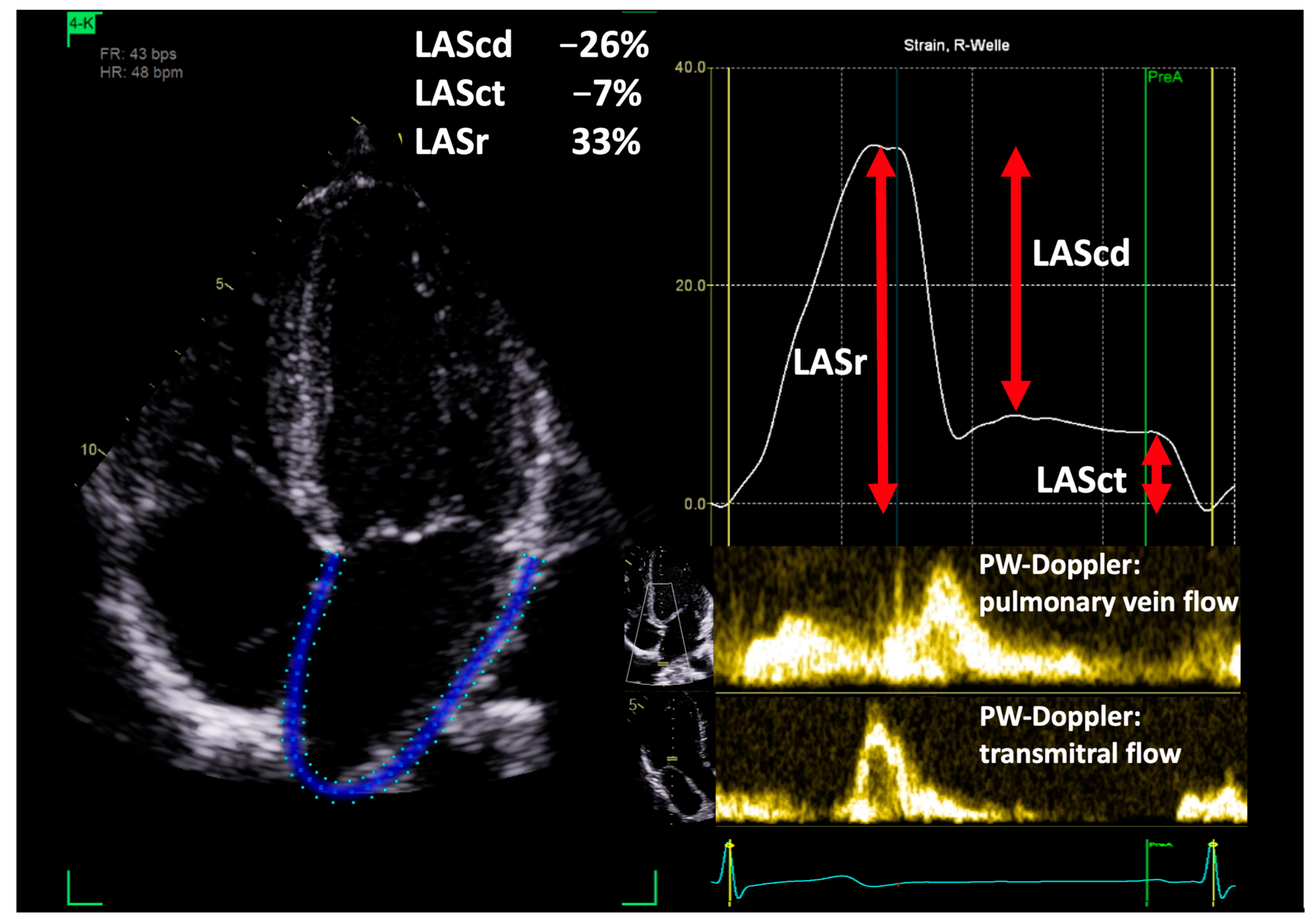
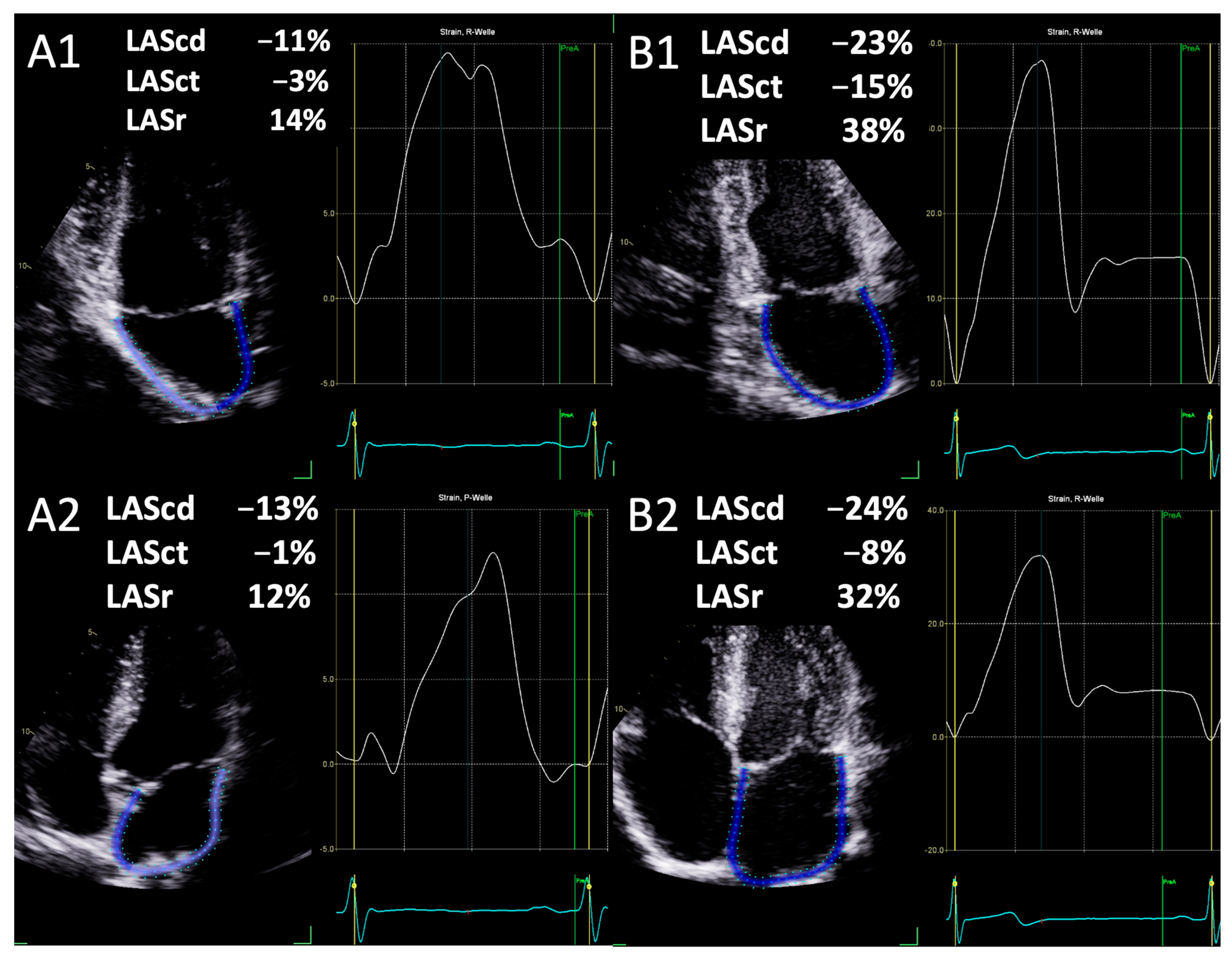
2.2. Parameters of Left Atrial Deformation
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kato, T.; Harada, T.; Kagami, K.; Obokata, M. The roles of global longitudinal strain imaging in contemporary clinical cardiology. J. Med. Ultrason. 2022, 49, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Abhayaratna, W.P.; Seward, J.B.; Appleton, C.P.; Douglas, P.S.; Oh, J.K.; Tajik, A.J.; Tsang, T.S.M. Left Atrial Size. J. Am. Coll. Cardiol. 2006, 47, 2357–2363. [Google Scholar] [CrossRef] [PubMed]
- Ferkh, A.; Clark, A.; Thomas, L. Left atrial phasic function: Physiology, clinical assessment and prognostic value. Heart 2023, 109, 1661–1669. [Google Scholar] [CrossRef]
- Goette, A.; Kalman, J.M.; Aguinaga, L.; Akar, J.; Cabrera, J.A.; Chen, S.A.; Chugh, S.S.; Corradi, D.; D’Avila, A.; Dobrev, D.; et al. EHRA/HRS/APHRS/SOLAECE expert consensus on atrial cardiomyopathies: Definition, characterization, and clinical implication. Europace 2016, 18, 1455–1490. [Google Scholar] [CrossRef]
- Casaclang-Verzosa, G.; Gersh, B.J.; Tsang, T.S.M. Structural and Functional Remodeling of the Left Atrium. J. Am. Coll. Cardiol. 2008, 51, 1–11. [Google Scholar] [CrossRef]
- Carpenito, M.; Fanti, D.; Mega, S.; Benfari, G.; Bono, M.C.; Rossi, A.; Ribichini, F.L.; Grigioni, F. The Central Role of Left Atrium in Heart Failure. Front. Cardiovasc. Med. 2021, 8, 704762. [Google Scholar] [CrossRef] [PubMed]
- Pathan, F.; D’Elia, N.; Nolan, M.T.; Marwick, T.H.; Negishi, K. Normal Ranges of Left Atrial Strain by Speckle-Tracking Echocardiography: A Systematic Review and Meta-Analysis. J. Am. Soc. Echocardiogr. 2017, 30, 59–70.e8. [Google Scholar] [CrossRef]
- Galderisi, M.; Cosyns, B.; Edvardsen, T.; Cardim, N.; Delgado, V.; Di Salvo, G.; Donal, E.; Sade, L.E.; Ernande, L.; Garbi, M.; et al. Standardization of adult transthoracic echocardiography reporting in agreement with recent chamber quantification, diastolic function, and heart valve disease recommendations: An expert consensus document of the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1301–1310. [Google Scholar] [CrossRef]
- Cotrim, C.; João, I.; Fazendas, P.; Almeida, A.R.; Lopes, L.; Stuart, B.; Cruz, I.; Caldeira, D.; Loureiro, M.J.; Morgado, G.; et al. Clinical applications of exercise stress echocardiography in the treadmill with upright evaluation during and after exercise. Cardiovasc. Ultrasound 2013, 11, 26. [Google Scholar] [CrossRef]
- Kandels, J.; Metze, M.; Hagendorff, A.; Marshall, R.P.; Hepp, P.; Laufs, U.; Stöbe, S. The impact of upright posture on left ventricular deformation in athletes. Int. J. Cardiovasc. Imaging 2023, 39, 1123–1131. [Google Scholar] [CrossRef]
- Suojanen, L.J.; Koskela, J.K.; Wilenius, M.; Choudhary, M.K.; Hautaniemi, E.J.; Viik, J.; Mustonen, J.T.; Pörsti, I.H. Individual changes of central blood pressure in response to upright posture: Different hemodynamic phenotypes. J. Hypertens. 2021, 39, 2403–2412. [Google Scholar] [CrossRef] [PubMed]
- Gottfridsson, P.; A’Roch, R.; Lindqvist, P.; Law, L.; Myrberg, T.; Hultin, M.; A’Roch, A.; Haney, M. Left atrial contraction strain and controlled preload alterations, a study in healthy individuals. Cardiovasc. Ultrasound 2022, 20, 8. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar] [CrossRef]
- Zhao, Y.; Sun, Q.; Han, J.; Lu, Y.; Zhang, Y.; Song, W.; Cheng, Y.; Cong, T.; Liu, Y.; Jiang, Y. Left atrial stiffness index as a marker of early target organ damage in hypertension. Hypertens Res. 2021, 44, 299–309. [Google Scholar] [CrossRef]
- Xu, T.-Y.; Sun, J.P.; Lee, A.P.-W.; Yang, X.S.; Ji, L.; Zhang, Z.; Li, Y.; Yu, C.-M.; Wang, J.-G. Left Atrial Function as Assessed by Speckle-Tracking Echocardiography in Hypertension. Medicine 2015, 94, e526. [Google Scholar] [CrossRef]
- Telles, F.; Nanayakkara, S.; Evans, S.; Patel, H.C.; Mariani, J.A.; Vizi, D.; William, J.; Marwick, T.H.; Kaye, D.M. Impaired left atrial strain predicts abnormal exercise haemodynamics in heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2019, 21, 495–505. [Google Scholar] [CrossRef]
- Torii, Y.; Kusunose, K.; Hirata, Y.; Nishio, S.; Ise, T.; Yamaguchi, K.; Fukuda, D.; Yagi, S.; Yamada, H.; Soeki, T.; et al. Left Atrial Strain Associated with Functional Recovery in Patients Receiving Optimal Treatment for Heart Failure. J. Am. Soc. Echocardiogr. 2021, 34, 966–975.e2. [Google Scholar] [CrossRef]
- Saijo, Y.; Van Iterson, E.; Vega Brizneda, M.; Desai, M.Y.; Lever, H.M.; Smedira, N.G.; Wierup, P.; Thamilarasan, M.; Popović, Z.B.; Grimm, R.A.; et al. Impact of left atrial strain mechanics on exercise intolerance and need for septal reduction therapy in hypertrophic cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 238–245. [Google Scholar] [CrossRef]
- Cerrito, L.F.; Maffeis, C.; Inciardi, R.M.; Tafciu, E.; Benfari, G.; Bergamini, C.; Ribichini, F.L.; Rossi, A. How to incorporate left atrial strain in the diagnostic algorithm of left ventricular diastolic dysfunction. Int. J. Cardiovasc. Imaging 2021, 37, 945–951. [Google Scholar] [CrossRef]
- Tsai, W.; Lee, C.; Lin, C.; Liu, Y.; Huang, Y.; Li, W.; Chen, J.; Lin, L. Association of Left Atrial Strain and Strain Rate Assessed by Speckle Tracking Echocardiography with Paroxysmal Atrial Fibrillation. Echocardiography 2009, 26, 1188–1194. [Google Scholar] [CrossRef]
- Ma, X.; Boldt, L.; Zhang, Y.; Zhu, M.; Hu, B.; Parwani, A.; Belyavskiy, E.; Radha Krishnan, A.K.; Krisper, M.; Köhncke, C.; et al. Clinical Relevance of Left Atrial Strain to Predict Recurrence of Atrial Fibrillation after Catheter Ablation: A Meta-Analysis. Echocardiography 2016, 33, 724–733. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, S.; Desai, R.; Andi, K.; Vyas, A.; Deliwala, S.; Sachdeva, R.; Kumar, G. Reduced left atrial strain can predict stroke in atrial fibrillation—A meta-analysis. IJC Heart Vasc. 2021, 36, 100859. [Google Scholar] [CrossRef] [PubMed]
- Donal, E.; Galli, E.; Schnell, F. Left Atrial Strain: A Must or a Plus for Routine Clinical Practice? Circ. Cardiovasc. Imaging 2017, 10, e007023. [Google Scholar] [CrossRef]
- Genovese, D.; Singh, A.; Volpato, V.; Kruse, E.; Weinert, L.; Yamat, M.; Mor-Avi, V.; Addetia, K.; Lang, R.M. Load Dependency of Left Atrial Strain in Normal Subjects. J. Am. Soc. Echocardiogr. 2018, 31, 1221–1228. [Google Scholar] [CrossRef]
- Santoro, A.; Alvino, F.; Antonelli, G.; Molle, R.; Mondillo, S. Left atrial strain after maximal exercise in competitive waterpolo players. Int. J. Cardiovasc. Imaging 2016, 32, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-H.; Kim, K.H.; Rink, L.; Hornsby, K.; Cho, J.Y.; Cho, G.-Y.; Lee, J.-H.; Seong, I.-W.; Jeong, M.H.; Cho, J.G.; et al. Left atrial enlargement and its association with left atrial strain in university athletes participated in 2015 Gwangju Summer Universiade. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Cicetti, M.; Bagate, F.; Lapenta, C.; Gendreau, S.; Masi, P.; Mekontso Dessap, A. Effect of volume infusion on left atrial strain in acute circulatory failure. Ann. Intensive Care 2024, 14, 53. [Google Scholar] [CrossRef]
- Park, C.S.; Kim, Y.-K.; Song, H.C.; Choi, E.J.; Ihm, S.-H.; Kim, H.-Y.; Youn, H.-J.; Seung, K.B. Effect of preload on left atrial function: Evaluated by tissue Doppler and strain imaging. Eur. Heart J. Cardiovasc. Imaging 2012, 13, 938–947. [Google Scholar] [CrossRef]
- Stefani, L.D.; Trivedi, S.J.; Ferkh, A.; Emerson, P.; Marschner, S.; Gan, G.; Altman, M.; Thomas, L. Left atrial mechanics evaluated by two-dimensional strain analysis: Alterations in essential hypertension. J. Hypertens. 2024, 42, 274–282. [Google Scholar] [CrossRef]
- Gastl, M.; Bejinariu, A.; Behm, P.; Lindert, A.; Kelm, M.; Makimoto, H.; Bönner, F.; Perings, S. Role of CMR-derived atrial deformation analysis in the prediction of atrial fibrillation recurrence rate after pulmonary vein isolation. Eur. J. Radiol. 2022, 155, 110452. [Google Scholar] [CrossRef]
- Guazzi, M.; Maltagliati, A.; Tamborini, G.; Celeste, F.; Pepi, M.; Muratori, M.; Berti, M.; Guazzi, M.D. How the left and right sides of the heart, as well as pulmonary venous drainage, adapt to an increasing degree of head-up tilting in hypertrophic cardiomyopathy: Differences from the normal heart. J. Am. Coll. Cardiol. 2000, 36, 185–193. [Google Scholar] [CrossRef]
- Bjällmark, A.; Larsson, M.; Shahgaldi, K.; Lind, B.; Winter, R.; Brodin, L. Differences in myocardial velocities during supine and upright exercise stress echocardiography in healthy adults. Clin. Physio Funct. Imaging 2009, 29, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Reuss, C.S.; Moreno, C.A.; Appleton, C.P.; Lester, S.J. Doppler Tissue Imaging During Supine and Upright Exercise in Healthy Adults. J. Am. Soc. Echocardiogr. 2005, 18, 1343–1348. [Google Scholar] [CrossRef] [PubMed]
- Thorstensen, A.; Dalen, H.; Amundsen, B.H.; Aase, S.A.; Stoylen, A. Reproducibility in echocardiographic assessment of the left ventricular global and regional function, the HUNT study. Eur. J. Echocardiogr. 2010, 11, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.E.; Hahn, R.T.; Stein, K.M.; Markowitz, S.M.; Okin, P.M.; Devereux, R.B.; Lerman, B.B. Left Ventricular Geometry and Function Preceding Neurally Mediated Syncope. Circulation 2000, 101, 777–783. [Google Scholar] [CrossRef] [PubMed]
- St. Pierre, S.R.; Peirlinck, M.; Kuhl, E. Sex Matters: A Comprehensive Comparison of Female and Male Hearts. Front. Physiol. 2022, 13, 831179. [Google Scholar] [CrossRef] [PubMed]
- Eckstein, J.; Körperich, H.; Paluszkiewicz, L.; Burchert, W.; Piran, M. Multi-parametric analyses to investigate dependencies of normal left atrial strain by cardiovascular magnetic resonance feature tracking. Sci. Rep. 2022, 12, 12233. [Google Scholar] [CrossRef]
- Pathan, F.; Zainal Abidin, H.A.; Vo, Q.H.; Zhou, H.; D’Angelo, T.; Elen, E.; Negishi, K.; Puntmann, V.O.; Marwick, T.H.; Nagel, E. Left atrial strain: A multi-modality, multi-vendor comparison study. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 102–110. [Google Scholar] [CrossRef]
- Wang, Y.; Li, Z.; Fei, H.; Yu, Y.; Ren, S.; Lin, Q.; Li, H.; Tang, Y.; Hou, Y.; Li, M. Left atrial strain reproducibility using vendor-dependent and vendor-independent software. Cardiovasc. Ultrasound 2019, 17, 9. [Google Scholar] [CrossRef]
- Cavarretta, E.; D’Ascenzi, F.; Bianco, M.; Castelletti, S.; Cavigli, L.; Cecchi, F.; D’Andrea, A.; De Luca, A.; Di Salvo, G.; Nistri, S.; et al. The role of echocardiography in sports cardiology: An expert opinion statement of the Italian Society of Sports Cardiology (SIC sport). Int. J. Cardiol. 2024, 410, 132230. [Google Scholar] [CrossRef] [PubMed]
- Niederseer, D.; Rossi, V.A.; Kissel, C.; Scherr, J.; Caselli, S.; Tanner, F.C.; Bohm, P.; Schmied, C. Role of echocardiography in screening and evaluation of athletes. Heart 2021, 107, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, R.T.; Forster, J.; Ackrill, M.; Chatrath, N.; Finocchiaro, G.; Fyyaz, S.; MacLachlan, H.; Malhotra, A.; Marwaha, S.; Papadakis, M.; et al. Coronary artery anomalies and the role of echocardiography in pre-participation screening of athletes: A practical guide. Echo Res. Pract. 2024, 11, 5. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variables (n = 50) | |
|---|---|
| Age (years) | 25.7 ± 7.3 |
| Male (%) | 100 |
| Weight (kg) | 83.9 ± 12.2 |
| Height (cm) | 186.2 ± 6.5 |
| BSA (m2) | 2.08 ± 0.17 |
| BMI (kg/m2) | 24.1 ± 2.3 |
| Variables | Upright Posture | Left Lateral Position | p Value |
|---|---|---|---|
| sBP (mmHg) | 128.3 ± 8.3 | 125.3 ± 9.9 | 0.104 |
| dBP (mmHg) | 74.3 ± 6.8 | 72.9 ± 12.2 | 0.482 |
| HR (1/min) | 79.1 ± 13.9 | 61.0 ± 10.1 | <0.001 |
| IVSD (mm) | 9.9 ± 1.2 | 9.7 ± 1.4 | 0.299 |
| LVPWD (mm) | 9.6 ± 1.1 | 9.3 ± 1.2 | 0.383 |
| LVEDD (mm) | 48.2 ± 4.2 | 54.8 ± 5.0 | <0.001 |
| LVESD (mm) | 31.9 ± 3.7 | 34.8 ± 4.7 | <0.001 |
| LVEDV biplane (mL) | 117.4 ± 29.5 | 157.9 ± 30.8 | <0.001 |
| LVESV biplane (mL) | 48.3 ± 15.3 | 62.7 ± 19.1 | <0.001 |
| LVMi (g/m2) | 98.3 ± 21.0 | 106.0 ± 16.8 | 0.072 |
| RWT | 0.40 ± 0.05 | 0.35 ± 0.05 | <0.001 |
| LVSV Doppler (mL) | 65.3 ± 14.2 | 94.7 ± 15.8 | <0.001 |
| LVSVi Doppler (mL/m2) | 31.2 ± 6.0 | 45.4 ± 7.2 | <0.001 |
| LVSV biplane (mL) | 69.1 ± 16.3 | 95.1 ± 16.0 | <0.001 |
| LVSVi biplane (mL/m2) | 33.2 ± 7.0 | 45.7 ± 6.4 | <0.001 |
| MV E Max (m/s) | 0.78 ± 0.13 | 0.77 ± 0.15 | 0.924 |
| MV A Max (m/s) | 0.48 ± 0.10 | 0.40 ± 0.08 | <0.001 |
| E/A | 1.65 ± 0.26 | 1.99 ± 0.48 | <0.001 |
| LVOT VTI (cm) | 15.7 ± 3.1 | 22.8 ± 3.7 | <0.001 |
| EF (%) | 59.7 ± 5.3 | 61.1 ± 5.5 | 0.197 |
| CO (L/min) | 4.72 ± 1.12 | 5.28 ± 0.98 | <0.001 |
| CI ((L/min)/m2) | 2.26 ± 0.49 | 2.54 ± 0.43 | 0.003 |
| Variables | Upright Posture | Left Lateral Position | p Value |
|---|---|---|---|
| 4 Chamber View | |||
| Conduction Strain (%) | −13.9 ± 6.5 | −26.9 ±6.9 | <0.001 |
| Contraction Strain (%) | −4.0 ± 3.3 | −9.0 ± 4.1 | <0.001 |
| Reservoir Strain (%) | 17.9 ± 7.5 | 34.4 ± 13.4 | <0.001 |
| Maximum Volume (mL) | 20.8 ± 8.0 | 41.8 ± 15.7 | <0.001 |
| 2 Chamber View | |||
| Conduction Strain (%) | −14.0 ± 7.8 | −27.7 ± 9.0 | <0.001 |
| Contraction Strain (%) | −5.4 ± 4.9 | −12.2 ± 9.9 | <0.001 |
| Reservoir Strain (%) | 19.6 ± 10.4 | 41.6 ± 9.7 | <0.001 |
| Maximum Volume (mL) | 27.1 ± 11.0 | 54.4 ± 17.2 | <0.001 |
| Biplane | |||
| Conduction Strain (%) | −14.0 ± 5.9 | −27.4 ± 7.1 | <0.001 |
| Contraction Strain (%) | −4.6 ± 3.5 | −11.3 ± 4.1 | <0.001 |
| Reservoir Strain (%) | 18.7 ± 7.6 | 38.7 ± 8.0 | <0.001 |
| Maximum Volume (mL) | 24.4 ± 8.8 | 50.0 ± 14.2 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kandels, J.; Stöbe, S.; Marshall, R.P.; Hagendorff, A.; Metze, M. The Effect of Upright Posture on Left Atrial Strain in Competitive Athletes. J. Cardiovasc. Dev. Dis. 2024, 11, 284. https://doi.org/10.3390/jcdd11090284
Kandels J, Stöbe S, Marshall RP, Hagendorff A, Metze M. The Effect of Upright Posture on Left Atrial Strain in Competitive Athletes. Journal of Cardiovascular Development and Disease. 2024; 11(9):284. https://doi.org/10.3390/jcdd11090284
Chicago/Turabian StyleKandels, Joscha, Stephan Stöbe, Robert Percy Marshall, Andreas Hagendorff, and Michael Metze. 2024. "The Effect of Upright Posture on Left Atrial Strain in Competitive Athletes" Journal of Cardiovascular Development and Disease 11, no. 9: 284. https://doi.org/10.3390/jcdd11090284