
Effects of Pulmonary Vein Isolation for Atrial Fibrillation on Skin Sympathetic Nerve Activity in Association with Left Atrial Remodeling

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
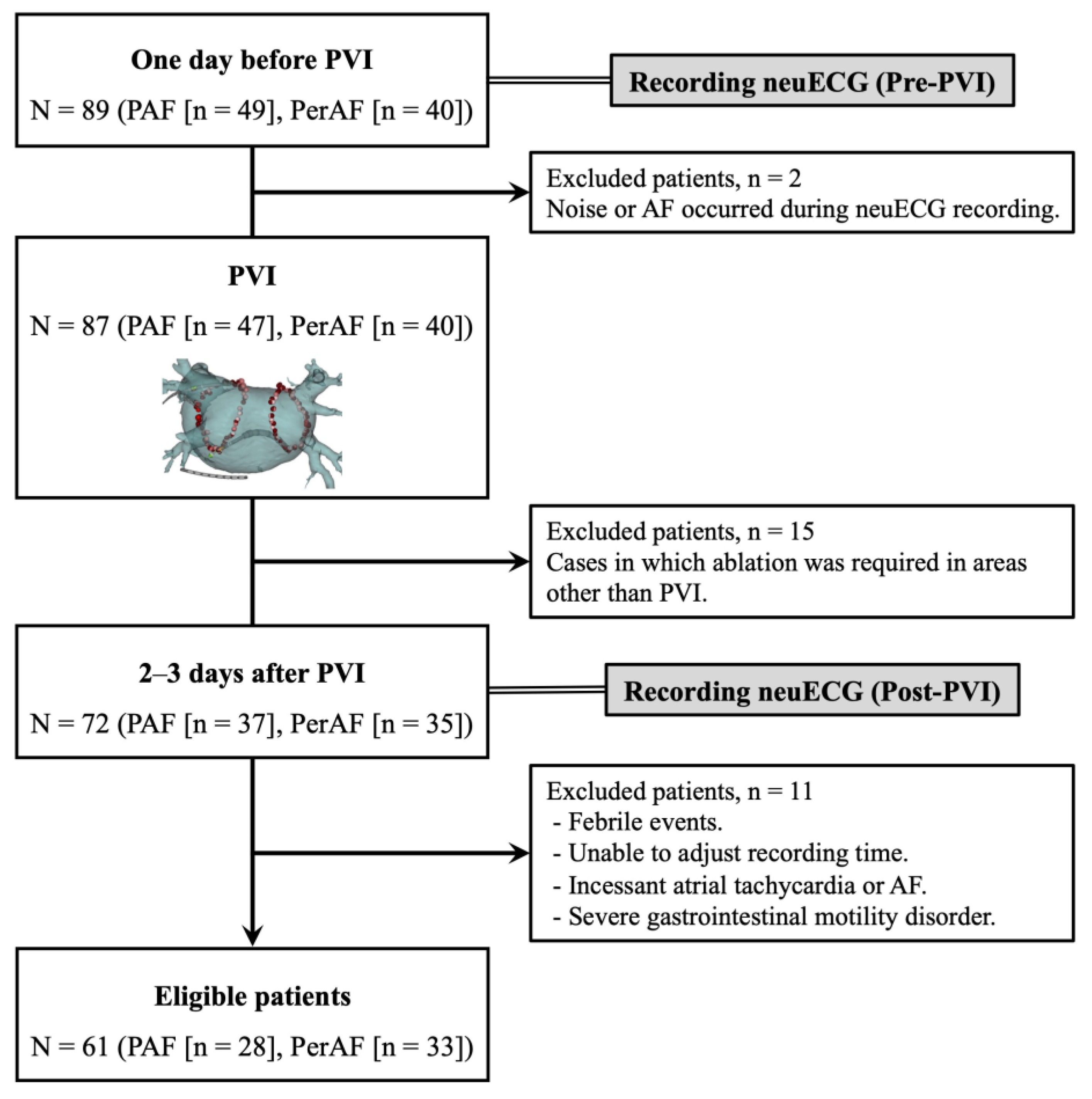
2.1. Participants
2.2. Pulmonary Vein Isolation
2.3. Echocardiography
2.4. Study Protocol
2.5. SKNA Recording and Analysis
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the AF Patients
3.2. Representative SKNA Waveforms
3.3. Differences in SKNA Depending on AF Type
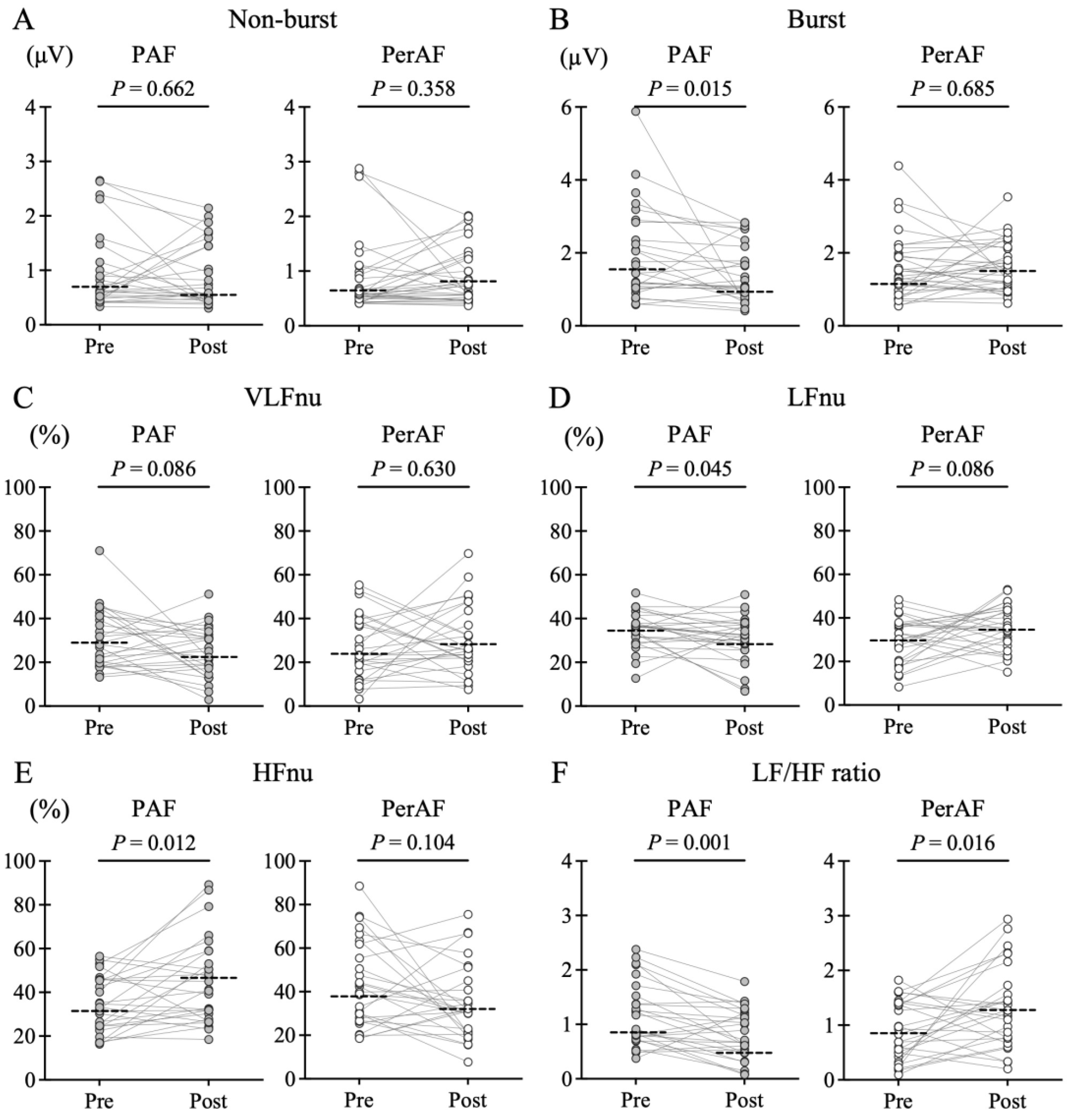
3.4. SKNA Changes Caused by PVI
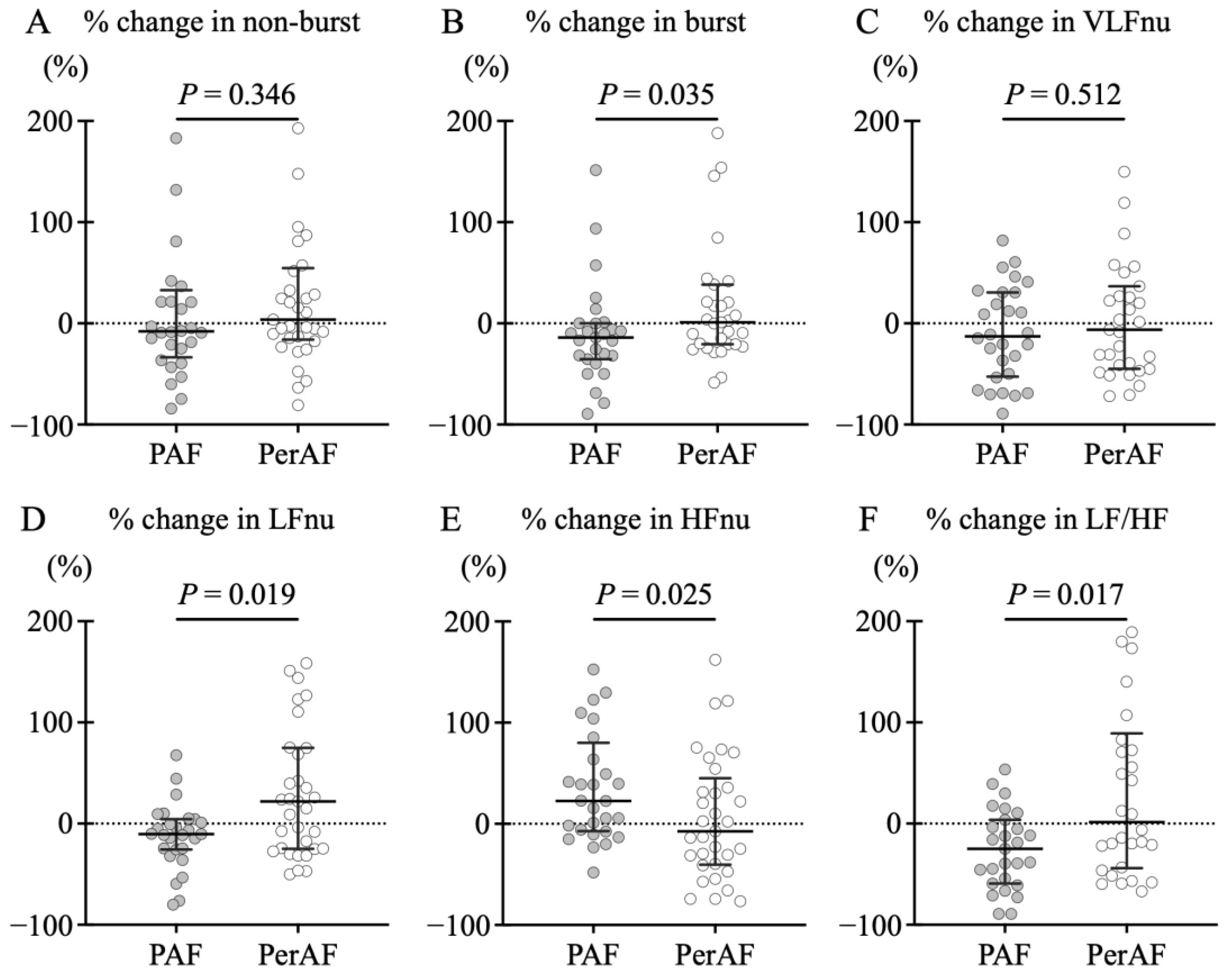
3.5. Comparison of PVI Strategies
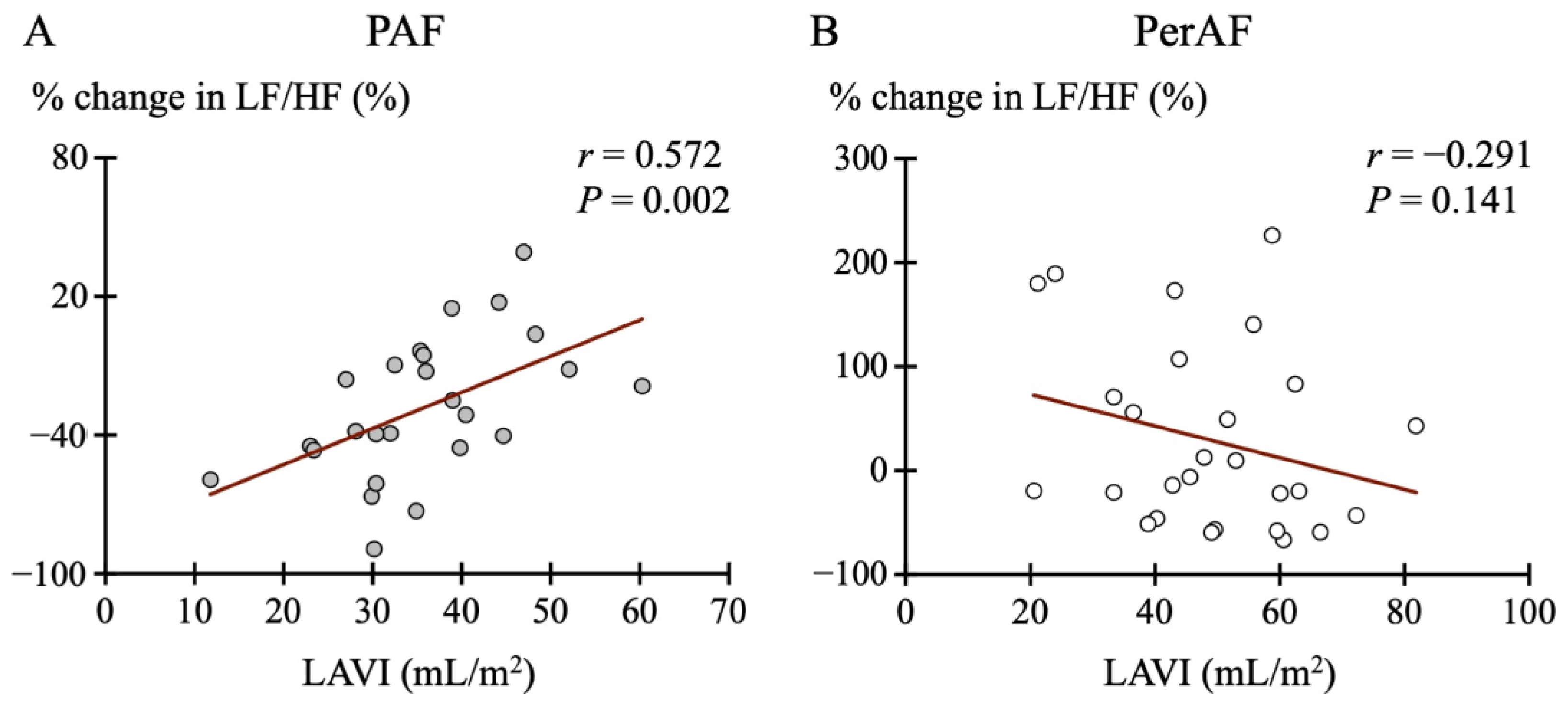
3.6. Association Between SKNA and Echocardiographic Parameters
3.7. Post Hoc Power of the Present Study
4. Discussion
4.1. Major Findings
4.2. Cardiac Autonomic Disorders in AF
4.3. PVI-Mediated Neuromodulation
4.4. Impairment of Neuromodulation Due to LA Remodeling
4.5. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benjamin, E.J.; Chen, P.S.; Bild, D.E.; Mascette, A.M.; Albert, C.M.; Alonso, A.; Calkins, H.; Connolly, S.J.; Curtis, A.B.; Darbar, D.; et al. Prevention of atrial fibrillation: Report from a national heart, lung, and blood institute workshop. Circulation 2009, 119, 606–618. [Google Scholar] [CrossRef] [PubMed]
- Kistler, P.M.; Chieng, D. Persistent atrial fibrillation in the setting of pulmonary vein isolation—Where to next? J. Cardiovasc. Electr. 2020, 31, 1857–1860. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.Y.; Zhou, S.; Ogawa, M.; Song, J.; Chu, M.; Li, H.; Fishbein, M.C.; Lin, S.F.; Chen, L.S.; Chen, P.S. Neural mechanisms of paroxysmal atrial fibrillation and paroxysmal atrial tachycardia in ambulatory canines. Circulation 2008, 118, 916–925. [Google Scholar] [CrossRef]
- Malik, V.; McKitrick, D.J.; Lau, D.H.; Sanders, P.; Arnolda, L.F. Clinical evidence of autonomic dysfunction due to atrial fibrillation: Implications for rhythm control strategy. J. Interv. Card. Electrophysiol. 2019, 54, 299–307. [Google Scholar] [CrossRef]
- Kusayama, T.; Wong, J.; Liu, X.; He, W.; Doytchinova, A.; Robinson, E.A.; Adams, D.E.; Chen, L.S.; Lin, S.F.; Davoren, K.; et al. Simultaneous noninvasive recording of electrocardiogram and skin sympathetic nerve activity (neuECG). Nat. Protoc. 2020, 15, 1853–1877. [Google Scholar] [CrossRef] [PubMed]
- Kusayama, T.; Douglas, A.; Wan, J.; Doytchinova, A.; Wong, J.; Mitscher, G.; Straka, S.; Shen, C.; Everett, T.H.; Chen, P.S. Skin sympathetic nerve activity and ventricular rate control during atrial fibrillation. Heart Rhythm. 2020, 17, 544–552. [Google Scholar] [CrossRef]
- Kusayama, T.; Wan, J.; Doytchinova, A.; Wong, J.; Kabir, R.A.; Mitscher, G.; Straka, S.; Shen, C.; Everett, T.H.; Chen, P.S. Skin sympathetic nerve activity and the temporal clustering of cardiac arrhythmias. JCI Insight 2019, 4, e125853. [Google Scholar] [CrossRef] [PubMed]
- De With, R.R.; Marcos, E.G.; Dudink, E.; Spronk, H.M.; Crijns, H.; Rienstra, M.; Van Gelder, I.C. Atrial fibrillation progression risk factors and associated cardiovascular outcome in well-phenotyped patients: Data from the AF-RISK study. Europace 2020, 22, 352–360. [Google Scholar] [CrossRef]
- Linz, D.; Ukena, C.; Mahfoud, F.; Neuberger, H.R.; Böhm, M. Atrial autonomic innervation: A target for interventional antiarrhythmic therapy? J. Am. Coll. Cardiol. 2014, 63, 215–224. [Google Scholar] [CrossRef]
- Po, S.S.; Nakagawa, H.; Jackman, W.M. Localization of Left Atrial Ganglionated Plexi in Patients with Atrial Fibrillation. J. Cardiovasc. Electr. 2009, 20, 1186–1189. [Google Scholar] [CrossRef]
- Miyoshi, M.; Kondo, H.; Ishii, Y.; Shinohara, T.; Yonezu, K.; Harada, T.; Sato, H.; Yano, Y.; Yoshimura, S.; Abe, I.; et al. Baroreflex Sensitivity in Patients with Atrial Fibrillation. J. Am. Heart Assoc. 2020, 9, e018019. [Google Scholar] [CrossRef]
- Mukai, Y.; Murai, H.; Hamaoka, T.; Sugimoto, H.; Inoue, O.; Goten, C.; Kusayama, T.; Takashima, S.-I.; Kato, T.; Usui, S.; et al. Effect of pulmonary vein isolation on the relationship between left atrial reverse remodeling and sympathetic nerve activity in patients with atrial fibrillation. Clin. Auton. Res. 2022, 32, 229–235. [Google Scholar] [CrossRef]
- Joglar, J.A.; Chung, M.K.; Armbruster, A.L.; Benjamin, E.J.; Chyou, J.Y.; Cronin, E.M.; Deswal, A.; Eckhardt, L.L.; Goldberger, Z.D.; Gopinathannair, R.; et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation. J. Am. Coll. Cardiol. 2024, 83, 109–279. [Google Scholar] [CrossRef]
- Field, M.E.; Wasmund, S.L.; Page, R.L.; Hamdan, M.H. Restoring Sinus Rhythm Improves Baroreflex Function in Patients with Persistent Atrial Fibrillation. J. Am. Heart Assoc. 2016, 5, e002997. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, T.; Morimoto, M.; Taniguchi, Y.; Takasaka, M.; Totoki, T. Cutaneous distribution of sympathetic postganglionic fibers from stellate ganglion: A retrograde axonal tracing study using wheat germ agglutinin conjugated with horseradish peroxidase. J. Anesth. 1994, 8, 441–449. [Google Scholar] [CrossRef]
- Liu, X.; Yuan, Y.; Wong, J.; Meng, G.; Ueoka, A.; Woiewodski, L.M.; Chen, L.S.; Shen, C.; Li, X.; Lin, S.-F.; et al. The frequency spectrum of sympathetic nerve activity and arrhythmogenicity in ambulatory dogs. Heart Rhythm. 2021, 18, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Meng, G.; He, W.; Wong, J.; Li, X.; Mitscher, G.A.; Straka, S.; Adams, D.; Everett, T.H.; Manchanda, S.; Liu, X.; et al. Successful continuous positive airway pressure treatment reduces skin sympathetic nerve activity in patients with obstructive sleep apnea. Heart Rhythm. 2022, 19, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.; Mishima, R.; Elliott, A.D.; Lau, D.H.; Sanders, P. The “Road” to Atrial Fibrillation: The Role of the Cardiac Autonomic Nervous System. J. Atr. Fibrillation 2020, 13, 2400. [Google Scholar] [CrossRef]
- Chen, P.S.; Chen, L.S.; Fishbein, M.C.; Lin, S.F.; Nattel, S. Role of the autonomic nervous system in atrial fibrillation: Pathophysiology and therapy. Circ. Res. 2014, 114, 1500–1515. [Google Scholar] [CrossRef]
- Chen, P.S.; Tan, A.Y. Autonomic nerve activity and atrial fibrillation. Heart Rhythm. 2007, 4, S61–S64. [Google Scholar] [CrossRef]
- Jayachandran, J.V.; Sih, H.J.; Winkle, W.; Zipes, D.P.; Hutchins, G.D.; Olgin, J.E. Atrial Fibrillation Produced by Prolonged Rapid Atrial Pacing Is Associated with Heterogeneous Changes in Atrial Sympathetic Innervation. Circulation 2000, 101, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.; Elliott, A.D.; Thomas, G.; Mishima, R.S.; Pitman, B.; Middeldorp, M.E.; Fitzgerald, J.L.; Young, G.D.; Roberts-Thomson, K.C.; Arnolda, L.F.; et al. Autonomic Afferent Dysregulation in Atrial Fibrillation. JACC Clin. Electrophysiol. 2022, 8, 152–164. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Wei, C.; Liu, L.; Lian, A.L.; Qu, X.F.; Yu, G. Atrial Fibrillation Increases Sympathetic and Parasympathetic Neurons in the Intrinsic Cardiac Nervous System. Pacing Clin. Electrophysiol. 2014, 37, 1462–1469. [Google Scholar] [CrossRef]
- Nishikimi, T.; Maeda, N.; Matsuoka, H. The role of natriuretic peptides in cardioprotection. Cardiovasc. Res. 2006, 69, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, T.; Murai, H.; Kaneko, S.; Usui, S.; Kobayashi, D.; Nakano, M.; Ikeda, K.; Takashima, S.; Kato, T.; Okajima, M.; et al. Augmented single-unit muscle sympathetic nerve activity in heart failure with chronic atrial fibrillation. J. Physiol. 2012, 590, 509–518. [Google Scholar] [CrossRef]
- Kampaktsis, P.N.; Oikonomou, E.K.; Choi, D.Y.; Cheung, J.W. Efficacy of ganglionated plexi ablation in addition to pulmonary vein isolation for paroxysmal versus persistent atrial fibrillation: A meta-analysis of randomized controlled clinical trials. J. Interv. Card. Electrophysiol. 2017, 50, 253–260. [Google Scholar] [CrossRef]
- Pappone, C.; Santinelli, V.; Manguso, F.; Vicedomini, G.; Gugliotta, F.; Augello, G.; Mazzone, P.; Tortoriello, V.; Landoni, G.; Zangrillo, A.; et al. Pulmonary Vein Denervation Enhances Long-Term Benefit After Circumferential Ablation for Paroxysmal Atrial Fibrillation. Circulation 2004, 109, 327–334. [Google Scholar] [CrossRef]
- Sung, W.-T.; Lo, L.-W.; Lin, Y.-J.; Chang, S.-L.; Hu, Y.-F.; Chung, F.-P.; Liao, J.-N.; Tuan, T.-C.; Chao, T.-F.; Lin, C.-Y.; et al. Alteration of Skin Sympathetic Nerve Activity after Pulmonary Vein Isolation in Patients with Paroxysmal Atrial Fibrillation. J. Pers. Med. 2022, 12, 1286. [Google Scholar] [CrossRef]
- Weng, C.J.; Li, C.H.; Lin, Y.J.; Chang, S.L.; Hu, Y.F.; Chung, F.P.; Liao, J.N.; Tuan, T.C.; Chao, T.F.; Lin, C.Y.; et al. Skin sympathetic nerve activity in different ablation settings for atrial fibrillation. J. Cardiol. 2024, 83, 306–312. [Google Scholar] [CrossRef]
- Yanagisawa, S.; Inden, Y.; Fujii, A.; Kamikubo, Y.; Kanzaki, Y.; Ando, M.; Funabiki, J.; Murase, Y.; Takenaka, M.; Otake, N.; et al. Assessment of autonomic nervous system modulation after novel catheter ablation techniques for atrial fibrillation using multiple short-term electrocardiogram recordings. J. Interv. Card. Electrophysiol. 2018, 51, 35–44. [Google Scholar] [CrossRef]
- Tang, L.Y.W.; Hawkins, N.M.; Ho, K.; Tam, R.; Deyell, M.W.; Macle, L.; Verma, A.; Khairy, P.; Sheldon, R.; Andrade, J.G. CIRCA-DOSE Study Investigators. Autonomic Alterations After Pulmonary Vein Isolation in the CIRCA-DOSE (Cryoballoon vs Irrigated Radiofrequency Catheter Ablation) Study. J. Am. Heart Assoc. 2021, 10, e018610. [Google Scholar] [CrossRef]
- Kuck, K.-H.; Brugada, J.; Fürnkranz, A.; Metzner, A.; Ouyang, F.; Chun, K.R.J.; Elvan, A.; Arentz, T.; Bestehorn, K.; Pocock, S.J.; et al. Cryoballoon or Radiofrequency Ablation for Paroxysmal Atrial Fibrillation. N. Engl. J. Med. 2016, 374, 2235–2245. [Google Scholar] [CrossRef] [PubMed]
- Kurose, J.; Kiuchi, K.; Fukuzawa, K.; Mori, S.; Ichibori, H.; Konishi, H.; Taniguchi, Y.; Hyogo, K.; Imada, H.; Suehiro, H.; et al. The lesion characteristics assessed by LGE-MRI after the cryoballoon ablation and conventional radiofrequency ablation. J. Arrhythmia 2018, 34, 158–166. [Google Scholar] [CrossRef]
- Allessie, M. Electrical, contractile and structural remodeling during atrial fibrillation. Cardiovasc. Res. 2002, 54, 230–246. [Google Scholar] [CrossRef] [PubMed]
- Qu, X.; Yu, Y.; Jiang, J.; Bai, B.; Guo, H.; Song, Y. Variance of Peptidic Nerve Innervation in a Canine Model of Atrial Fibrillation Produced by Prolonged Atrial Pacing. Pacing Clin. Electrophysiol. 2008, 31, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Dudley, S.C.; Hoch, N.E.; McCann, L.A.; Honeycutt, C.; Diamandopoulos, L.; Fukai, T.; Harrison, D.G.; Dikalov, S.I.; Langberg, J. Atrial Fibrillation Increases Production of Superoxide by the Left Atrium and Left Atrial Appendage. Circulation 2005, 112, 1266–1273. [Google Scholar] [CrossRef]
- Kubo, T.; Azevedo, E.R.; Newton, G.E.; Picton, P.; Parker, J.D.; Floras, J.S. β-blockade restores muscle sympathetic rhythmicity in human heart failure. Circ. J. 2011, 75, 1400–1408. [Google Scholar] [CrossRef]
- Buijs, R.M.; Escobar, C.; Swaab, D.F. The circadian system and the balance of the autonomic nervous system. Handb. Clin. Neurol. 2013, 117, 173–191. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | PAF (n = 28) | PerAF (n = 33) | p-Value |
|---|---|---|---|
| Age (years) | 70.0 (59.5–73.8) | 64.0 (56.5–74.0) | 0.365 |
| Female sex, n (%) | 20 (71.4) | 21 (63.4) | 0.518 |
| BMI (kg/m2) | 23.4 (21.7–25.4) | 24.1 (21.7–26.3) | 0.572 |
| eGFR (mL/min/1.73 m2) | 75.2 (69.9–84.4) | 63.3 (54.1–69.1) | <0.001 |
| BNP (pg/mL) | 34.3 (19.7–72.3) | 217.2 (133.7–372.4) | <0.001 |
| Echocardiographic results | |||
| LVEF (%) | 62.7 (59.8–68.5) | 51.0 (40.0–57.0) | <0.001 |
| LAD (mm) | 38.8 (32.9–43.2) | 41.9 (38.8–45.5) | 0.026 |
| LAVI (mL/m2) | 36.0 (30.1–47.7) | 49.1 (38.9–60.1) | 0.014 |
| Average E/e’ ratio | 8.4 (7.4–12.0) | 8.8 (7.4–11.8) | 0.884 |
| Peak TR velocity (m/s) | 2.3 (2.1–2.6) | 2.2 (1.9–2.4) | 0.113 |
| Medications before PVI | |||
| AADs, n (%) | 6 (21.4) | 3 (9.1) | 0.178 |
| β-blockers, n (%) | 13 (46.4) | 18 (54.6) | 0.528 |
| Ablation results | |||
| RFA, n (%) | 18 (64.3) | 24 (72.7) | 0.487 |
| CBA, n (%) | 10 (35.7) | 9 (27.3) | 0.487 |
| Procedure time (min) | 137.5 (121.3–157.5) | 145.0 (119.0–175.0) | 0.357 |
| Fluoroscopy time (min) | 15.7 (12.1–23.6) | 18.5 (10.6–23.3) | 0.983 |
| Early recurrence, n (%) | 5 (17.9) | 14 (42.4) | 0.039 |
| Distant recurrence, n (%) | 1 (3.6) | 3 (9.1) | 0.386 |
| Variables | Estimate | SE | t-Value | p-Value |
|---|---|---|---|---|
| PAF | ||||
| LVEF (%) | 1.981 | 1.017 | −1.95 | 0.073 |
| LAD (mm) | 1.648 | 1.351 | 1.22 | 0.244 |
| LAVI (mL/m2) | 1.599 | 0.690 | 2.32 | 0.037 |
| Average E/e’ ratio | 0.851 | 2.476 | 0.34 | 0.736 |
| Peak TR velocity (m/) | 25.302 | 16.331 | 0.34 | 0.145 |
| PerAF | ||||
| LVEF (%) | −0.856 | 5.279 | −0.16 | 0.873 |
| LAD (mm) | −16.170 | 15.631 | −1.03 | 0.315 |
| LAVI (mL/m2) | −4.891 | 4.664 | −1.05 | 0.308 |
| Average E/e’ ratio | 14.293 | 11.455 | 1.25 | 0.228 |
| Peak TR velocity (m/s) | −27.220 | 155.754 | −0.17 | 0.863 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakagawa, Y.; Kusayama, T.; Morita, M.; Nagamori, Y.; Takeuchi, K.; Iwaisako, S.; Tsuda, T.; Kato, T.; Usui, S.; Sakata, K.; et al. Effects of Pulmonary Vein Isolation for Atrial Fibrillation on Skin Sympathetic Nerve Activity in Association with Left Atrial Remodeling. J. Cardiovasc. Dev. Dis. 2025, 12, 123. https://doi.org/10.3390/jcdd12040123
Nakagawa Y, Kusayama T, Morita M, Nagamori Y, Takeuchi K, Iwaisako S, Tsuda T, Kato T, Usui S, Sakata K, et al. Effects of Pulmonary Vein Isolation for Atrial Fibrillation on Skin Sympathetic Nerve Activity in Association with Left Atrial Remodeling. Journal of Cardiovascular Development and Disease. 2025; 12(4):123. https://doi.org/10.3390/jcdd12040123
Chicago/Turabian StyleNakagawa, Yoichiro, Takashi Kusayama, Mayumi Morita, Yuta Nagamori, Kazutaka Takeuchi, Shuhei Iwaisako, Toyonobu Tsuda, Takeshi Kato, Soichiro Usui, Kenji Sakata, and et al. 2025. "Effects of Pulmonary Vein Isolation for Atrial Fibrillation on Skin Sympathetic Nerve Activity in Association with Left Atrial Remodeling" Journal of Cardiovascular Development and Disease 12, no. 4: 123. https://doi.org/10.3390/jcdd12040123
APA StyleNakagawa, Y., Kusayama, T., Morita, M., Nagamori, Y., Takeuchi, K., Iwaisako, S., Tsuda, T., Kato, T., Usui, S., Sakata, K., Hayashi, K., & Takamura, M. (2025). Effects of Pulmonary Vein Isolation for Atrial Fibrillation on Skin Sympathetic Nerve Activity in Association with Left Atrial Remodeling. Journal of Cardiovascular Development and Disease, 12(4), 123. https://doi.org/10.3390/jcdd12040123