Insights from Second-Line Treatments for Idiopathic Dilated Cardiomyopathy

Abstract
:1. Introduction
2. Methods
3. Results
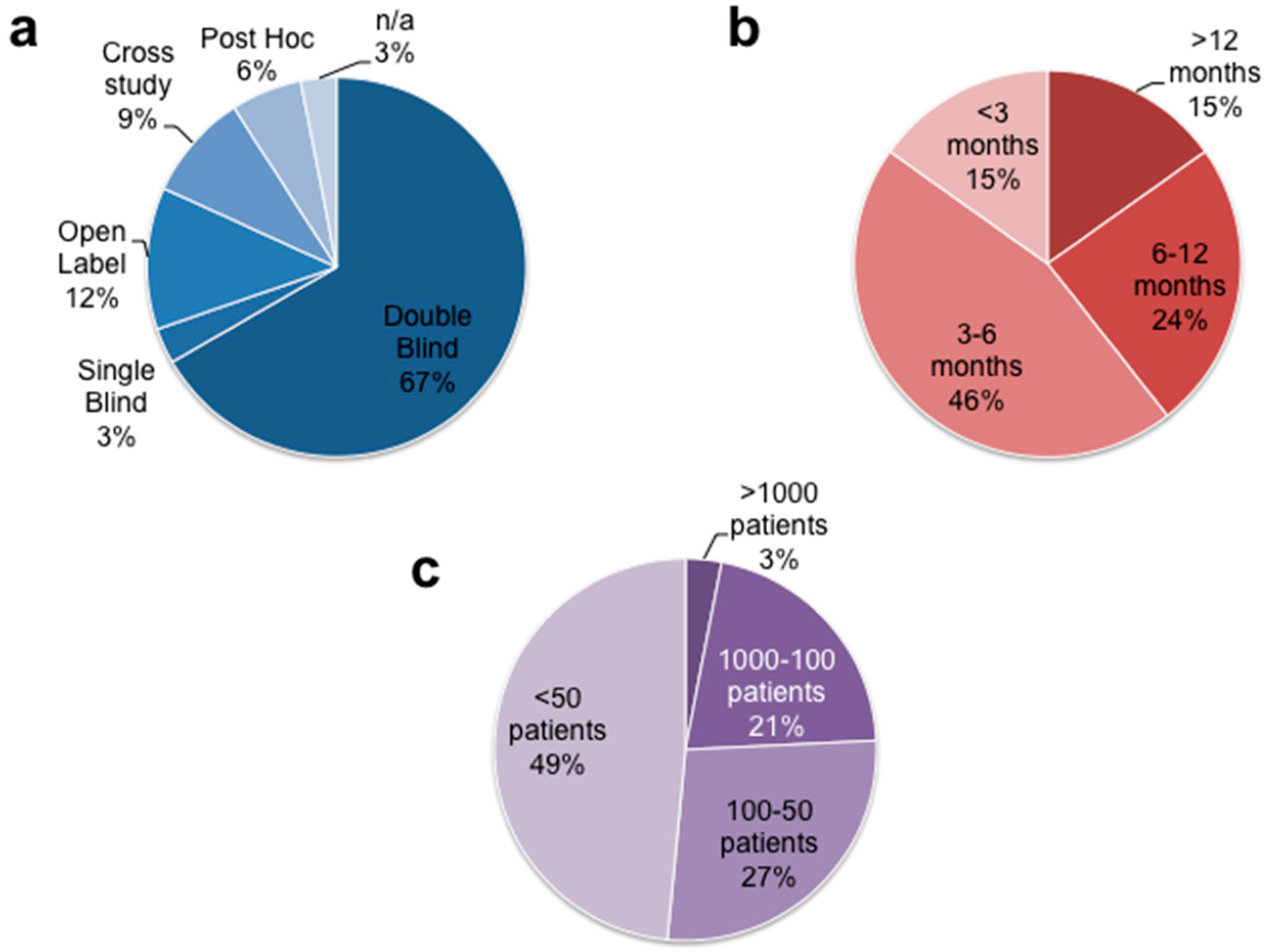
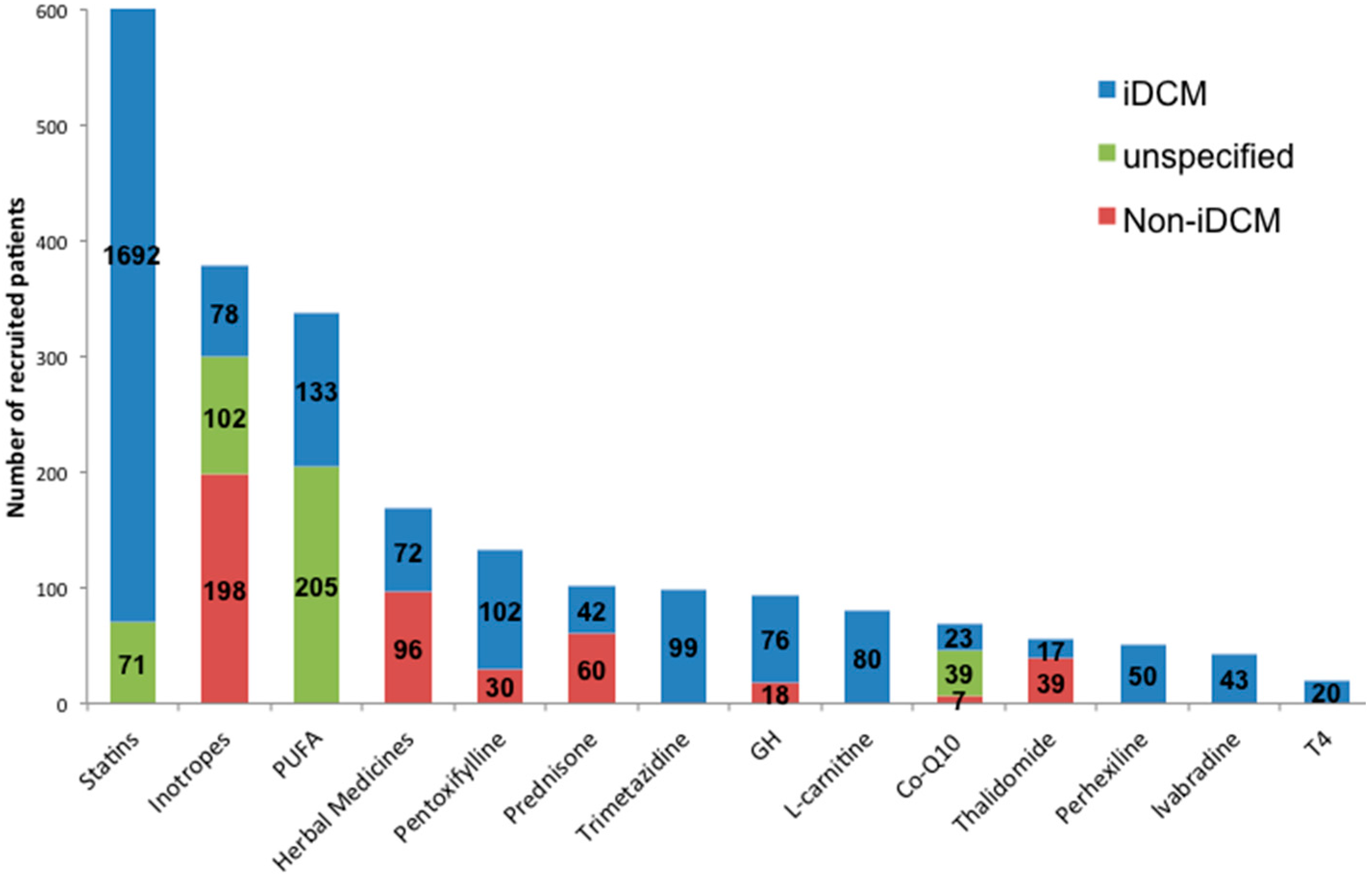
3.1. General Study Characteristics
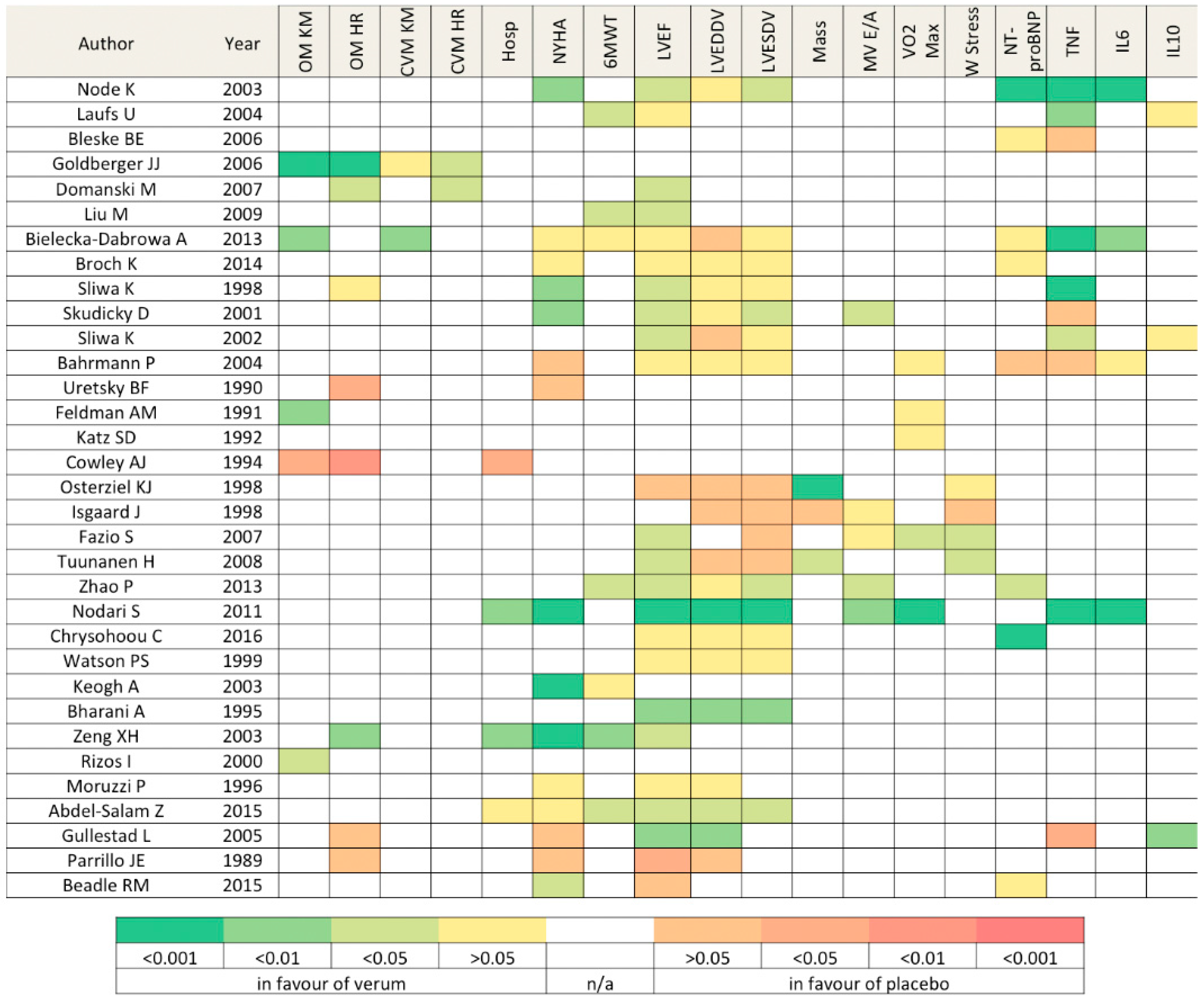
3.2. Overall Findings
4. Discussion
4.1. Not All Statins Were Created Equal
4.2. Inflammation Resolution: Is It Worth?
4.3. Inotropism Manipulation: A Double-Edged Knife
4.4. Mitochondrion: A Hijacked Powerhouse
4.5. Growth Hormone: New Bricks for a Crumbling Heart?
4.6. A Challenging Equation
5. Conclusions
6. Limitations
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Elliott, P. Cardiomyopathy: Diagnosis and management of dilated cardiomyopathy. Heart 2000, 84, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Japp, A.G.; Gulati, A.; Cook, S.A.; Cowie, M.R.; Prasad, S.K. The Diagnosis and Evaluation of Dilated Cardiomyopathy. J. Am. Coll. Cardiol. 2016, 67, 2996–3010. [Google Scholar] [CrossRef] [PubMed]
- Pecini, R.; Moller, D.V.; Torp-Pedersen, C.; Hassager, C.; Kober, L. Heart failure etiology impacts survival of patients with heart failure. Int. J. Cardiol. 2011, 149, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Kober, L.; Thune, J.J.; Nielsen, J.C.; Haarbo, J.; Videbæk, L.; Korup, E.; Jensen, G.; Hildebrandt, P.; Steffensen, F.H.; Bruun, N.E.; et al. Defibrillator Implantation in Patients with Nonischemic Systolic Heart Failure. N. Engl. J. Med. 2016, 375, 1221–1230. [Google Scholar] [CrossRef] [PubMed]
- Rose, E.A.; Gelijns, A.C.; Moskowitz, A.J.; Heitjan, D.F.; Stevenson, L.W.; Dembitsky, W.; Long, J.W.; Ascheim, D.D.; Tierney, A.R.; Levitan, R.G.; et al. Long-term use of a left ventricular assist device for end-stage heart failure. N. Engl. J. Med. 2001, 345, 1435–1443. [Google Scholar] [CrossRef] [PubMed]
- Slaughter, M.S.; Rogers, J.G.; Milano, C.A.; Russell, S.D.; Conte, J.V.; Feldman, D.; Sun, B.; Tatooles, A.J.; Delgado, R.M., 3rd; Long, J.W.; et al. Advanced heart failure treated with continuous-flow left ventricular assist device. N. Engl. J. Med. 2009, 361, 2241–2251. [Google Scholar] [CrossRef] [PubMed]
- Buckberg, G.; Athanasuleas, C.; Conte, J. Surgical ventricular restoration for the treatment of heart failure. Nat. Rev. Cardiol. 2012, 9, 703–716. [Google Scholar] [CrossRef] [PubMed]
- Bolli, R.; Ghafghazi, S. Current status of cell therapy for non-ischaemic cardiomyopathy: A brief overview. Eur. Heart J. 2015, 36, 2905–2908. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, R.G.; Semsarian, C.; Macdonald, P. Dilated cardiomyopathy. Lancet 2017, 390, 400–414. [Google Scholar] [CrossRef]
- Node, K.; Fujita, M.; Kitakaze, M.; Hori, M.; Liao, J.K. Short-term statin therapy improves cardiac function and symptoms in patients with idiopathic dilated cardiomyopathy. Circulation 2003, 108, 839–843. [Google Scholar] [CrossRef] [PubMed]
- Laufs, U.; Wassmann, S.; Schackmann, S.; Heeschen, C.; Böhm, M.; Nickenig, G. Beneficial effects of statins in patients with non-ischemic heart failure. Z. Kardiol. 2004, 93, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Bleske, B.E.; Nicklas, J.M.; Bard, R.L.; Brook, R.D.; Gurbel, P.A.; Bliden, K.P.; Rajagopalan, S.; Pitt, B. Neutral effect on markers of heart failure, inflammation, endothelial activation and function, and vagal tone after high-dose HMG-CoA reductase inhibition in non-diabetic patients with non-ischemic cardiomyopathy and average low-density lipoprotein level. J. Am. Coll. Cardiol. 2006, 47, 338–341. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, J.J.; Subacius, H.; Schaechter, A.; Howard, A.; Berger, R.; Shalaby, A.; Levine, J.; Kadish, A.H.; DEFINITE Investigators. Effects of statin therapy on arrhythmic events and survival in patients with nonischemic dilated cardiomyopathy. J. Am. Coll. Cardiol. 2006, 48, 1228–1233. [Google Scholar] [CrossRef] [PubMed]
- Domanski, M.; Coady, S.; Fleg, J.; Tian, X.; Sachdev, V. Effect of statin therapy on survival in patients with nonischemic dilated cardiomyopathy (from the Beta-blocker Evaluation of Survival Trial [BEST]). Am. J. Cardiol. 2007, 99, 1448–1450. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Wang, F.; Wang, Y.; Jin, R. Atorvastatin improves endothelial function and cardiac performance in patients with dilated cardiomyopathy: The role of inflammation. Cardiovasc. Drugs Ther. 2009, 23, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Bielecka-Dabrowa, A.; Mikhailidis, D.P.; Rizzo, M.; von Haeling, S.; Rysz, J.; Banach, M. The influence of atorvastatin on parameters of inflammation left ventricular function, hospitalizations and mortality in patients with dilated cardiomyopathy—5-year follow-up. Lipids Health Dis. 2013, 12, 47. [Google Scholar] [CrossRef] [PubMed]
- Broch, K.; Askevold, E.T.; Gjertsen, E.; Ueland, T.; Yndestad, A.; Godang, K.; Stueflotten, W.; Andreassen, J.; Svendsmark, R.; Smith, H.J.; et al. The effect of rosuvastatin on inflammation, matrix turnover and left ventricular remodeling in dilated cardiomyopathy: A randomized, controlled trial. PLoS ONE 2014, 9, e89732. [Google Scholar] [CrossRef] [PubMed]
- Sliwa, K.; Skudicky, D.; Candy, G.; Wisenbaugh, T.; Sareli, P. Randomised investigation of effects of pentoxifylline on left-ventricular performance in idiopathic dilated cardiomyopathy. Lancet 1998, 351, 1091–1093. [Google Scholar] [CrossRef]
- Skudicky, D.; Bergemann, A.; Sliwa, K.; Candy, G.; Sareli, P. Beneficial effects of pentoxifylline in patients with idiopathic dilated cardiomyopathy treated with angiotensin-converting enzyme inhibitors and carvedilol: Results of a randomized study. Circulation 2001, 103, 1083–1088. [Google Scholar] [CrossRef] [PubMed]
- Sliwa, K.; Woodwiss, A.; Candy, G.; Badenhorst, D.; Libhaber, C.; Norton, G.; Skudicky, D.; Sareli, P. Effects of pentoxifylline on cytokine profiles and left ventricular performance in patients with decompensated congestive heart failure secondary to idiopathic dilated cardiomyopathy. Am. J. Cardiol. 2002, 90, 1118–1122. [Google Scholar] [CrossRef]
- Bahrmann, P.; Hengst, U.M.; Richartz, B.M.; Figulla, H.R. Pentoxifylline in ischemic, hypertensive and idiopathic-dilated cardiomyopathy: Effects on left-ventricular function, inflammatory cytokines and symptoms. Eur. J. Heart Fail. 2004, 6, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Uretsky, B.F.; Jessup, M.; Konstam, M.A.; Dec, W.; Leier, C.V.; Benotti, J.; Murali, S.; Herrman, H.C.; Sandberg, J.A. Multicenter trial of oral enoximone in patients with moderate to moderately severe congestive heart failure. Lack of benefit compared with placebo. Enoximone Multicenter Trial Group. Circulation 1990, 82, 774–780. [Google Scholar] [CrossRef] [PubMed]
- Feldman, A.M.; Baughman, K.L.; Lee, W.K.; Gottlieb, S.H.; Weiss, J.L.; Becker, L.C.; Strobeck, J.E. Usefulness of OPC-8212, a quinolinone derivative, for chronic congestive heart failure in patients with ischemic heart disease or idiopathic dilated cardiomyopathy. Am. J. Cardiol. 1991, 68, 1203–1210. [Google Scholar] [CrossRef]
- Katz, S.D.; Kubo, S.H.; Jessup, M.; Brozena, S.; Troha, J.M.; Wahl, J.; Cohn, J.N.; Sonnenblick, E.H.; LeJemtel, T.H. A multicenter, randomized, double-blind, placebo-controlled trial of pimobendan, a new cardiotonic and vasodilator agent, in patients with severe congestive heart failure. Am. Heart J. 1992, 123, 95–103. [Google Scholar] [CrossRef]
- Cowley, A.J.; Skene, A.M. Treatment of severe heart failure: Quantity or quality of life? A trial of enoximone. Enoximone Investigators. Br. Heart J. 1994, 72, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Osterziel, K.J.; Strohm, O.; Schuler, J.; Friedrich, M.; Hänlein, D.; Willenbrock, R.; Anker, S.D.; Poole-Wilson, P.A.; Ranke, M.B.; Dietz, R. Randomised, double-blind, placebo-controlled trial of human recombinant growth hormone in patients with chronic heart failure due to dilated cardiomyopathy. Lancet 1998, 351, 1233–1237. [Google Scholar] [CrossRef]
- Isgaard, J.; Bergh, C.H.; Caidahl, K.; Lomsky, M.; Hjalmarson, A.; Bengtsson, B.A. A placebo-controlled study of growth hormone in patients with congestive heart failure. Eur. Heart J. 1998, 19, 1704–1711. [Google Scholar] [CrossRef] [PubMed]
- Fazio, S.; Palmieri, E.A.; Affuso, F.; Cittadini, A.; Castellano, G.; Russo, T.; Ruvolo, A.; Napoli, R.; Saccà, L. Effects of growth hormone on exercise capacity and cardiopulmonary performance in patients with chronic heart failure. J. Clin. Endocrinol. Metab. 2007, 92, 4218–4223. [Google Scholar] [CrossRef] [PubMed]
- Tuunanen, H.; Engblom, E.; Naum, A.; Nagren, K.; Scheinin, M.; Hesse, B.; Juhani Airaksinen, K.E.; Nuutila, P.; Iozzo, P.; Ukkonen, H.; et al. Trimetazidine, a metabolic modulator, has cardiac and extracardiac benefits in idiopathic dilated cardiomyopathy. Circulation 2008, 118, 1250–1258. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Zhang, J.; Yin, X.G.; Maharaj, P.; Narraindoo, P.; Cui, L.Q.; Tang, Y.S. The effect of trimetazidine on cardiac function in diabetic patients with idiopathic dilated cardiomyopathy. Life Sci. 2013, 92, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Nodari, S.; Triggiani, M.; Campia, U.; Manerba, A.; Milesi, G.; Cesana, B.M.; Gheorghiade, M.; Dei Cas, L. Effects of n-3 polyunsaturated fatty acids on left ventricular function and functional capacity in patients with dilated cardiomyopathy. J. Am. Coll. Cardiol. 2011, 57, 870–879. [Google Scholar] [CrossRef] [PubMed]
- Chrysohoou, C.; Metallinos, G.; Georgiopoulos, G.; Mendrinos, D.; Papanikolaou, A.; Magkas, N.; Pitsavos, C.; Vyssoulis, G.; Stefanadis, G.; Tousoulis, D. Short term omega-3 polyunsaturated fatty acid supplementation induces favorable changes in right ventricle function and diastolic filling pressure in patients with chronic heart failure; A randomized clinical trial. Vascul. Pharmacol. 2016, 79, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Watson, P.S.; Scalia, G.M.; Galbraith, A.; Burstow, D.J.; Bett, N.; Aroney, C.N. Lack of effect of coenzyme Q on left ventricular function in patients with congestive heart failure. J. Am. Coll. Cardiol. 1999, 33, 1549–1552. [Google Scholar] [CrossRef]
- Keogh, A.; Fenton, S.; Leslie, C.; Aboyoun, C.; Macdonald, P.; Zhao, Y.C.; Bailey, M.; Rosenfeldt, F. Randomised double-blind, placebo-controlled trial of coenzyme Q, therapy in class II and III systolic heart failure. Heart Lung Circ. 2003, 12, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.H.; Zeng, X.J.; Li, Y.Y. Efficacy and safety of berberine for congestive heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am. J. Cardiol. 2003, 92, 173–176. [Google Scholar] [CrossRef]
- Bharani, A.; Ganguly, A.; Bhargava, K.D. Salutary effect of Terminalia Arjuna in patients with severe refractory heart failure. Int. J. Cardiol. 1995, 49, 191–199. [Google Scholar] [CrossRef]
- Rizos, I. Three-year survival of patients with heart failure caused by dilated cardiomyopathy and l-carnitine administration. Am. Heart J. 2000, 139 Pt 3, S120–S123. [Google Scholar] [CrossRef] [PubMed]
- Moruzzi, P.; Doria, E.; Agostoni, P.G. Medium-term effectiveness of l-thyroxine treatment in idiopathic dilated cardiomyopathy. Am. J. Med. 1996, 101, 461–467. [Google Scholar] [CrossRef]
- Abdel-Salam, Z.; Rayan, M.; Saleh, A.; Abdel-Barr, M.G.; Hussain, M.; Nammas, W. I(f) current inhibitor ivabradine in patients with idiopathic dilated cardiomyopathy: Impact on the exercise tolerance and quality of life. Cardiol. J. 2015, 22, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Gullestad, L.; Ueland, T.; Fjeld, J.G.; Holt, E.; Gundersen, T.; Breivik, K.; Skardal, R.; Kjekshus, J.; Andreassen, A.; Kjekshus, E.; et al. Effect of thalidomide on cardiac remodeling in chronic heart failure: Results of a double-blind, placebo-controlled study. Circulation 2005, 112, 3408–3414. [Google Scholar] [CrossRef] [PubMed]
- Parrillo, J.E.; Cunnion, R.E.; Epstein, S.E.; Parker, M.M.; Suffredini, A.F.; Brenner, M.; Schaer, G.L.; Palmieri, S.T.; Cannon, R.O., 3rd; et al. A prospective, randomized, controlled trial of prednisone for dilated cardiomyopathy. N. Engl. J. Med. 1989, 321, 1061–1068. [Google Scholar] [CrossRef] [PubMed]
- Beadle, R.M.; Williams, L.K.; Kuehl, M.; Bowater, S.; Abozguia, K.; Leyva, F.; Yousef, Z.; Wagenmakers, A.; Thies, F.; Horowitz, J.; et al. Improvement in cardiac energetics by perhexiline in heart failure due to dilated cardiomyopathy. JACC Heart Fail. 2015, 3, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Chien, K.R. Stress pathways and heart failure. Cell 1999, 98, 555–558. [Google Scholar] [CrossRef]
- Tsutamoto, T.; Sakai, H.; Ibe, K.; Yamaji, M.; Kawahara, C.; Nakae, I.; Fujii, M.; Yamamoto, T.; Horie, M. Effect of atorvastatin vs. rosuvastatin on cardiac sympathetic nerve activity in non-diabetic patients with dilated cardiomyopathy. Circ. J. 2011, 75, 2160–2166. [Google Scholar] [CrossRef] [PubMed]
- Oesterle, A.; Laufs, U.; Liao, J.K. Pleiotropic Effects of Statins on the Cardiovascular System. Circ. Res. 2017, 120, 229–243. [Google Scholar] [CrossRef] [PubMed]
- Sawada, N.; Li, Y.; Liao, J.K. Novel aspects of the roles of Rac1 GTPase in the cardiovascular system. Curr. Opin. Pharmacol. 2010, 10, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.J.; Hill, M.M.; Chigurupati, S.; Du, G.; Parton, R.G.; Hancock, J.F. Therapeutic levels of the hydroxmethylglutaryl-coenzyme A reductase inhibitor lovastatin activate ras signaling via phospholipase D2. Mol. Cell. Biol. 2011, 31, 1110–1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noma, K.; Oyama, N.; Liao, J.K. Physiological role of ROCKs in the cardiovascular system. Am. J. Physiol. Cell Physiol. 2006, 290, C661–C668. [Google Scholar] [CrossRef] [PubMed]
- Takemoto, M.; Node, K.; Nakagami, H.; Liao, Y.; Grimm, M.; Takemoto, Y.; Kitakaze, M.; Liao, J.K. Statins as antioxidant therapy for preventing cardiac myocyte hypertrophy. J. Clin. Investig. 2001, 108, 1429–1437. [Google Scholar] [CrossRef] [PubMed]
- Yano, M.; Matsumura, T.; Senokuchi, T.; Ishii, N.; Murata, Y.; Taketa, K.; Motoshima, H.; Taguchi, T.; Sonoda, K.; Kukidome, D.; et al. Statins activate peroxisome proliferator-activated receptor gamma through extracellular signal-regulated kinase 1/2 and p38 mitogen-activated protein kinase-dependent cyclooxygenase-2 expression in macrophages. Circ. Res. 2007, 100, 1442–1451. [Google Scholar] [CrossRef] [PubMed]
- Feldman, A.M.; Combes, A.; Wagner, D.; Kadakomi, T.; Kubota, T.; Li, Y.Y.; McTiernan, C. The role of tumor necrosis factor in the pathophysiology of heart failure. J. Am. Coll. Cardiol. 2000, 35, 537–544. [Google Scholar] [CrossRef]
- Levine, B.; Kalman, J.; Mayer, L.; Fillit, H.M.; Packer, M. Elevated circulating levels of tumor necrosis factor in severe chronic heart failure. N. Engl. J. Med. 1990, 323, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Habib, F.M.; Springall, D.R.; Davies, G.J.; Oakley, C.M.; Yacoub, M.H.; Polak, J.M. Tumour necrosis factor and inducible nitric oxide synthase in dilated cardiomyopathy. Lancet 1996, 347, 1151–1155. [Google Scholar] [CrossRef]
- Torre-Amione, G.; Kapadia, S.; Benedict, C.; Oral, H.; Young, J.B.; Mann, D.L. Proinflammatory cytokine levels in patients with depressed left ventricular ejection fraction: A report from the Studies of Left Ventricular Dysfunction (SOLVD). J. Am. Coll. Cardiol. 1996, 27, 1201–1206. [Google Scholar] [CrossRef]
- Torre-Amione, G.; Kapadia, S.; Lee, J.; Durand, J.B.; Bies, R.D.; Young, J.B.; Mann, D.L. Tumor necrosis factor-alpha and tumor necrosis factor receptors in the failing human heart. Circulation 1996, 93, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Bristow, M.R. Tumor necrosis factor-alpha and cardiomyopathy. Circulation 1998, 97, 1340–1341. [Google Scholar] [CrossRef] [PubMed]
- Kubota, T.; McTiernan, C.F.; Frye, C.S.; Slawson, S.E.; Lemster, B.H.; Koretsky, A.P.; Demetris, A.J.; Feldman, A.J. Dilated cardiomyopathy in transgenic mice with cardiac-specific overexpression of tumor necrosis factor-alpha. Circ. Res. 1997, 81, 627–635. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.S.; Packer, M.; Lo, K.H.; Fasanmade, A.A.; Willerson, J.T.; ATTACH Investigators. Randomized, double-blind, placebo-controlled, pilot trial of infliximab, a chimeric monoclonal antibody to tumor necrosis factor-alpha, in patients with moderate-to-severe heart failure: Results of the anti-TNF Therapy Against Congestive Heart Failure (ATTACH) trial. Circulation 2003, 107, 3133–3140. [Google Scholar] [PubMed]
- Mann, D.L.; McMurray, J.J.; Packer, M.; Swedberg, K.; Borer, J.S.; Colucci, W.S.; Djian, J.; Drexler, H.; Feldman, A.; Kober, L.; et al. Targeted anticytokine therapy in patients with chronic heart failure: Results of the Randomized Etanercept Worldwide Evaluation (RENEWAL). Circulation 2004, 109, 1594–1602. [Google Scholar] [CrossRef] [PubMed]
- Yndestad, A.; Damas, J.K.; Oie, E.; Ueland, T.; Gullestad, L.; Aukrust, P. Role of inflammation in the progression of heart failure. Curr. Cardiol. Rep. 2007, 9, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Wojnicz, R.; Nowalany-Kozielska, E.; Wojciechowska, C.; Gianowska, G.; Wilczewski, P.; Niklewski, T.; Zembala, M.; Polonski, L.; Rozek, M.M.; Wodniecki, J. Randomized, placebo-controlled study for immunosuppressive treatment of inflammatory dilated cardiomyopathy: Two-year follow-up results. Circulation 2001, 104, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Colucci, W.S.; Wright, R.F.; Braunwald, E. New positive inotropic agents in the treatment of congestive heart failure. Mechanisms of action and recent clinical developments. 1. N. Engl. J. Med. 1986, 314, 290–299. [Google Scholar] [CrossRef] [PubMed]
- Colucci, W.S.; Wright, R.F.; Braunwald, E. New positive inotropic agents in the treatment of congestive heart failure. Mechanisms of action and recent clinical developments. 2. N. Engl. J. Med. 1986, 314, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Pollesello, P.; Papp, Z.; Papp, J.G. Calcium sensitizers: What have we learned over the last 25 years? Int. J. Cardiol. 2016, 203, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Gwathmey, J.K.; Copelas, L.; MacKinnon, R.; Schoen, F.J.; Feldman, M.D.; Grossman, W.; Morgan, J.P. Abnormal intracellular calcium handling in myocardium from patients with end-stage heart failure. Circ. Res. 1987, 61, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Mercadier, J.J.; Lompré, A.M.; Duc, P.; Boheler, K.R.; Fraysse, J.B.; Wisnewsky, C.; Allen, P.D.; Komajda, M.; Schwartz, K. Altered sarcoplasmic reticulum Ca2(+)-ATPase gene expression in the human ventricle during end-stage heart failure. J. Clin. Investig. 1990, 85, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Hasenfuss, G.; Reinecke, H.; Studer, R.; Meyer, M.; Pieske, B.; Holtz, J.; Holubarsch, C.; Posival, H.; Just, H.; Drexler, H. Relation between myocardial function and expression of sarcoplasmic reticulum Ca(2+)-ATPase in failing and nonfailing human myocardium. Circ. Res. 1994, 75, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Dec, G.W.; Fifer, M.A.; Herrmann, H.C.; Cocca-Spofford, D.; Semigran, M.J. Long-term outcome of enoximone therapy in patients with refractory heart failure. Am. Heart J. 1993, 125 Pt 1, 423–429. [Google Scholar] [CrossRef]
- Brown, D.A.; Perry, J.B.; Allen, M.E.; Sabbah, H.N.; Stauffer, B.L.; Shaikh, S.R.; Cleland, J.G.; Colucci, W.S.; Butler, J.; Voors, A.A.; et al. Expert consensus document: Mitochondrial function as a therapeutic target in heart failure. Nat. Rev. Cardiol. 2017, 14, 238–250. [Google Scholar] [CrossRef] [PubMed]
- Hershberger, R.E.; Hedges, D.J.; Morales, A. Dilated cardiomyopathy: The complexity of a diverse genetic architecture. Nat. Rev. Cardiol. 2013, 10, 531–547. [Google Scholar] [CrossRef] [PubMed]
- Bione, S.; D’Adamo, P.; Maestrini, E.; Gedeon, A.K.; Bolhuis, P.A.; Toniolo, D. A novel X-linked gene, G4.5. is responsible for Barth syndrome. Nat. Genet. 1996, 12, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Davila-Roman, V.G.; Vedala, G.; Herrero, P.; de las Fuentes, L.; Rogers, J.G.; Kelly, D.P.; Gropler, R.J. Altered myocardial fatty acid and glucose metabolism in idiopathic dilated cardiomyopathy. J. Am. Coll. Cardiol. 2002, 40, 271–277. [Google Scholar] [CrossRef]
- Sack, M.N.; Rader, T.A.; Park, S.; Bastin, J.; McCune, S.A.; Kelly, D.P. Fatty acid oxidation enzyme gene expression is downregulated in the failing heart. Circulation 1996, 94, 2837–2842. [Google Scholar] [CrossRef] [PubMed]
- Witteles, R.M.; Tang, W.H.; Jamali, A.H.; Chu, J.W.; Reaven, G.M.; Fowler, M.B. Insulin resistance in idiopathic dilated cardiomyopathy: A possible etiologic link. J. Am. Coll. Cardiol. 2004, 44, 78–81. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Fonarow, G.C.; Butler, J.; Ezekowitz, J.A.; Felker, G.M. Coenzyme Q10 and Heart Failure: A State-of-the-Art Review. Circ. Heart Fail. 2016, 9, e002639. [Google Scholar] [CrossRef] [PubMed]
- Olivetti, G.; Abbi, R.; Quaini, F.; Kajstura, J.; Cheng, W.; Nitahara, J.A.; Quaini, E.; Di Loreto, C.; Beltrami, C.A.; Krajewski, S.; et al. Apoptosis in the failing human heart. N. Engl. J. Med. 1997, 336, 1131–1141. [Google Scholar] [CrossRef] [PubMed]
- Narula, J.; Haider, N.; Virmani, R.; DiSalvo, T.G.; Kolodgie, F.D.; Hajjar, R.J.; Schmidt, U.; Semigran, M.J.; Dec, G.W.; Khaw, B.A. Apoptosis in myocytes in end-stage heart failure. N. Engl. J. Med. 1996, 335, 1182–1189. [Google Scholar] [CrossRef] [PubMed]
- Pluess, M.; Daeubler, G.; Dos Remedios, C.G.; Ehler, E. Adaptations of cytoarchitecture in human dilated cardiomyopathy. Biophys. Rev. 2015, 7, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.E.; Rotwein, P. Growth, differentiation, and survival: Multiple physiological functions for insulin-like growth factors. Physiol. Rev. 1996, 76, 1005–1026. [Google Scholar] [PubMed]
- Fazio, S.; Sabatini, D.; Capaldo, B.; Vigorito, C.; Giordano, A.; Guida, R.; Pardo, F.; Biondi, B.; Saccà, L. A preliminary study of growth hormone in the treatment of dilated cardiomyopathy. N. Engl. J. Med. 1996, 334, 809–814. [Google Scholar] [CrossRef] [PubMed]
- Dreifuss, P. Growth hormone in dilated cardiomyopathy (advantages and disadvantages). Eur. Heart J. 1999, 20, 243–244. [Google Scholar] [PubMed]
- Maison, P.; Chanson, P. Cardiac effects of growth hormone in adults with growth hormone deficiency: A meta-analysis. Circulation 2003, 108, 2648–2652. [Google Scholar] [CrossRef] [PubMed]
- Eryol, N.K.; Güven, M.; Topsakal, R.; Sungur, M.; Ozdogru, I.; Inanç, T.; Oguzhan, A. The effects of octreotide in dilated cardiomyopathy: An open-label trial in 12 patients. Jpn. Heart J. 2004, 45, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Lamberts, S.W.; van der Lely, A.J.; de Herder, W.W.; Hofland, L.J. Octreotide. N. Engl. J. Med. 1996, 334, 246–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bierer, B.E.; Crosas, M.; Pierce, H.H. Data Authorship as an Incentive to Data Sharing. N. Engl. J. Med. 2017, 376, 1684–1687. [Google Scholar] [CrossRef] [PubMed]
- Braunwald, E. The war against heart failure: The Lancet lecture. Lancet 2015, 385, 812–824. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | No. of Patients iDCM/Total (%) | Study Type and Design | Active Drug Target | Follow-up (Months) | LVEF % | |
|---|---|---|---|---|---|---|---|
| Threshold | Baseline Average | ||||||
| Statins | |||||||
| Node K [10] | 2003 | 48/48 (100%) | Double blind | Simvastatin (10 mg/day) | 3 | 40 | 34 |
| Laufs U [11] | 2004 | 15/15 (100%) | Double blind | Cerivastatin (0.4 mg/day) | 5 | n/a | 40 |
| Bleske BE [12] | 2006 | 15/15 (100%) | Crossed | Atorvastatin (80 mg/day) | 3 | 45 | 25 |
| Goldberger JJ [13] | 2006 | 458/458 (100%) | Post hoc analysis | Any statin at any dosage | 24 | 35 | 20 |
| Domanski M [14] | 2007 | 1024/1024 (100%) | Post hoc analysis | Any statin at any dosage | 24 | 35 | 25 |
| Liu M [15] | 2009 | 64/64 (100%) | Double blind | Atorvastatin (10mg/day) | 3 | 40 | 35 |
| Bielecka-Dabrowa A [16] | 2013 | 68/68 (100%) | Open | Atorvastatin (10 or 20 mg/day) | 60 | n/a | 32 |
| Broch K [17] | 2014 | 71 unspecified | Double blind | Rosuvastatin (10 mg/day) | 6 | 40 | 36 |
| Pentoxifylline | |||||||
| Sliwa K [18] | 1998 | 28/28 (100%) | Double blind | Pentoxifylline (400 mg/tid) | 6 | 40 | 22 |
| Skudicky D [19] | 2001 | 39/39 (100%) | Double blind | Pentoxifylline (400 mg/tid) | 6 | 40 | 24 |
| Sliwa K [20] | 2002 | 18/18 (100%) | Double blind | Pentoxifylline (400 mg/tid) | 1 | 40 | 16 |
| Bahrmann P [21] | 2004 | 17/47 (36.2%) | Double blind | Pentoxifylline (600 mg/bid) | 6 | 40 | 29 |
| Inotropes | |||||||
| Uretsky BF [22] | 1990 | 102 unspecified | Double blind | Enoximone (100 or 150 mg/tid) | 4 | n/a | 22 |
| Feldman AM [23] | 1991 | 38/76 (50%) | Double blind | Vesnarinone (60 mg/day) | 3 | n/a | 24 |
| Katz SD [24] | 1992 | 14/49 (28.6%) | Double blind | Pimobendan (5 or 10 mg/day) | 3 | n/a | 19 |
| Cowley AJ [25] | 1994 | 26/151 (16.6%) | Double blind | Enoximone (50 or 100 mg/tid) | 12 | n/a | n/a |
| Growth Hormone (GH) | |||||||
| Osterziel KJ [26] | 1998 | 50/50 (100%) | Double blind | rhGH subq (2 IU/qd) | 3 | 45 | 26 |
| Isgaard J [27] | 1998 | 13/22 (59.1%) | Double blind | rhGH subq (to 4 IU/qd) | 3 | 45 | 30 |
| Fazio S [28] | 2007 | 13/22 (59.1%) | Double blind | rhGH subq (to 4 IU/qod) | 3 | 40 | 32 |
| Trimetazidine | |||||||
| Tuunanen H [29] | 2008 | 19/19 (100%) | Single blind | Trimetazidine (35 mg/bid) | 3 | 47 | 31 |
| Zhao P [30] | 2013 | 80/80 (100%) | Double blind | Trimetazidine(20mg/tid) | 6 | 40 | 34 |
| Polyunsaturated Fatty Acids (PUFAs) | |||||||
| Nodari S [31] | 2011 | 133/133 (100%) | Double blind | EPA/DHA850 mg/bid | 12 | 45 | 36 |
| Chrysohoou C [32] | 2016 | 205 unspecified | Open | PUFA 1000 mg/day | 6 | 40 | 28 |
| CoQ10 | |||||||
| Watson PS [33] | 1999 | 23/30 (76.7%) | Cross | CoQ10 (33 mg/tid) | 3 | 35 | 26 |
| Keogh A [34] | 2003 | 39 unspecified | Double blind | CoQ10 (150 mg/day) | 3 | 40 | n/a |
| Herbal Medications | |||||||
| Bharani A [35] | 1995 | 10/12 (83.3%) | Cross | Terminalia Arjuna (500 mg/tid) | 0.5 | n/a | 30 |
| Zeng XH [36] | 2003 | 62/156 (39.8%) | Double blind | Berberine (up to 0.5 g/qid) | 2 | n/a | 22 |
| L-carnitine | |||||||
| Rizos I [37] | 2000 | 80/80 (100%) | Open | L-carnitine (2 g/day) | 34 | n/a | 27 |
| Levotyroxine (T4) | |||||||
| Moruzzi P [38] | 1996 | 20/20 (100%) | n/a | Levotyroxine (100 ug/day) | 3 | 40 | 30 |
| Ivabradine | |||||||
| Abdel-Salam Z [39] | 2015 | 43/43 (100%) | Double blind | Ivabradine(2.5 mg/tid) | 3 | 40 | 34 |
| Thalidomide | |||||||
| Gullestad L [40] | 2005 | 17/56 (30.4%) | Double blind | Thalidomide (200 mg/qd) | 3 | 40 | 24 |
| Steroids | |||||||
| Parrillo JE [41] | 1989 | 42/102 (41.2%) | Open | Prednisone (60 mg/day) for 3 months | 15 | 35 | 18 |
| Perhexelline | |||||||
| Beadle RM [42] | 2015 | 50/50 (100%) | Double blind | Perhexelline (200 mg/day) | 2 | 40 | 27 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luciani, M.; Del Monte, F. Insights from Second-Line Treatments for Idiopathic Dilated Cardiomyopathy. J. Cardiovasc. Dev. Dis. 2017, 4, 12. https://doi.org/10.3390/jcdd4030012
Luciani M, Del Monte F. Insights from Second-Line Treatments for Idiopathic Dilated Cardiomyopathy. Journal of Cardiovascular Development and Disease. 2017; 4(3):12. https://doi.org/10.3390/jcdd4030012
Chicago/Turabian StyleLuciani, Marco, and Federica Del Monte. 2017. "Insights from Second-Line Treatments for Idiopathic Dilated Cardiomyopathy" Journal of Cardiovascular Development and Disease 4, no. 3: 12. https://doi.org/10.3390/jcdd4030012
APA StyleLuciani, M., & Del Monte, F. (2017). Insights from Second-Line Treatments for Idiopathic Dilated Cardiomyopathy. Journal of Cardiovascular Development and Disease, 4(3), 12. https://doi.org/10.3390/jcdd4030012