

Remnant-Like Particle Cholesterol and the Risk of Major Adverse Cardiovascular Events: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Method
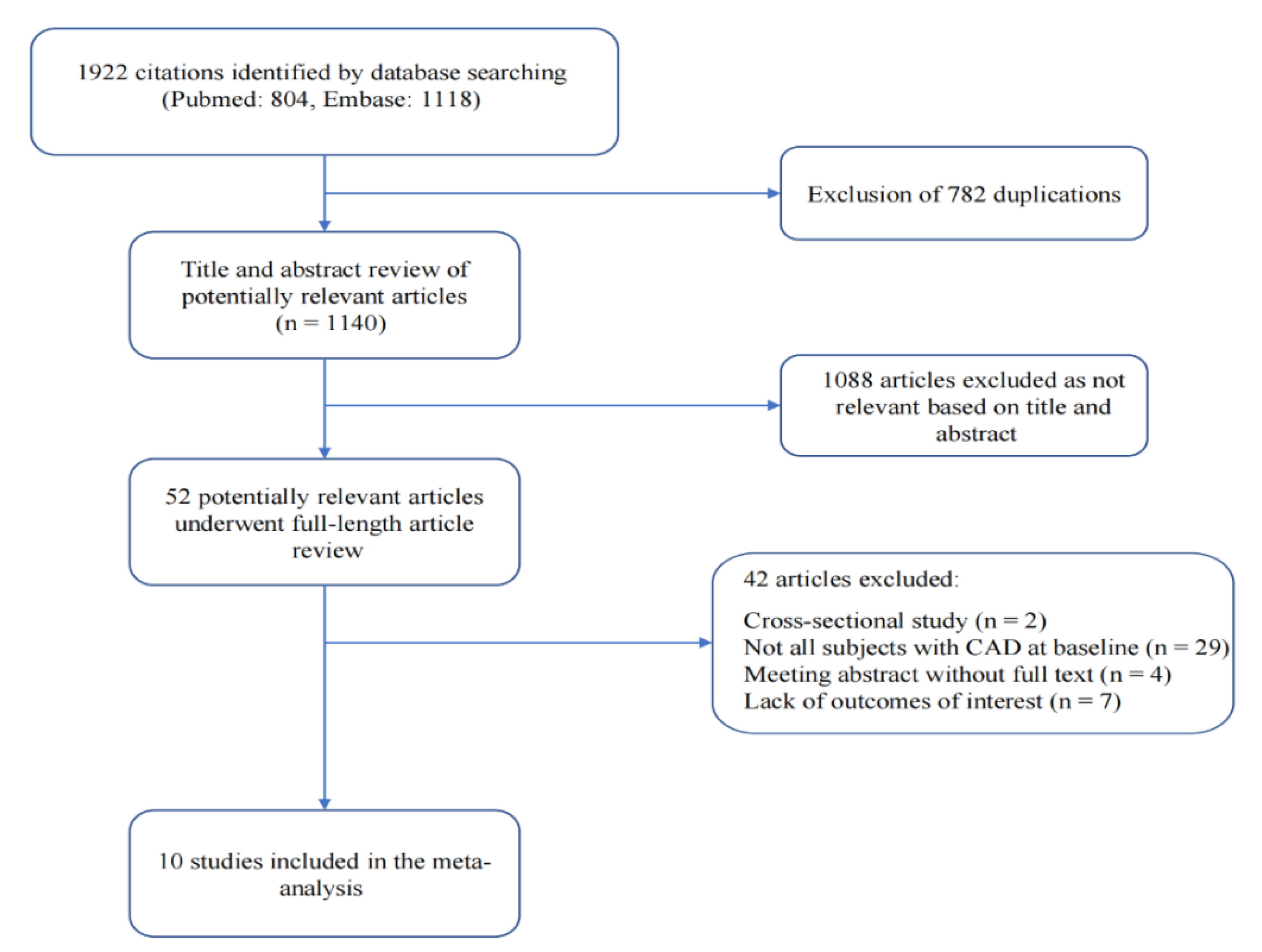
2.1. Literature Retrieval Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Included Studies
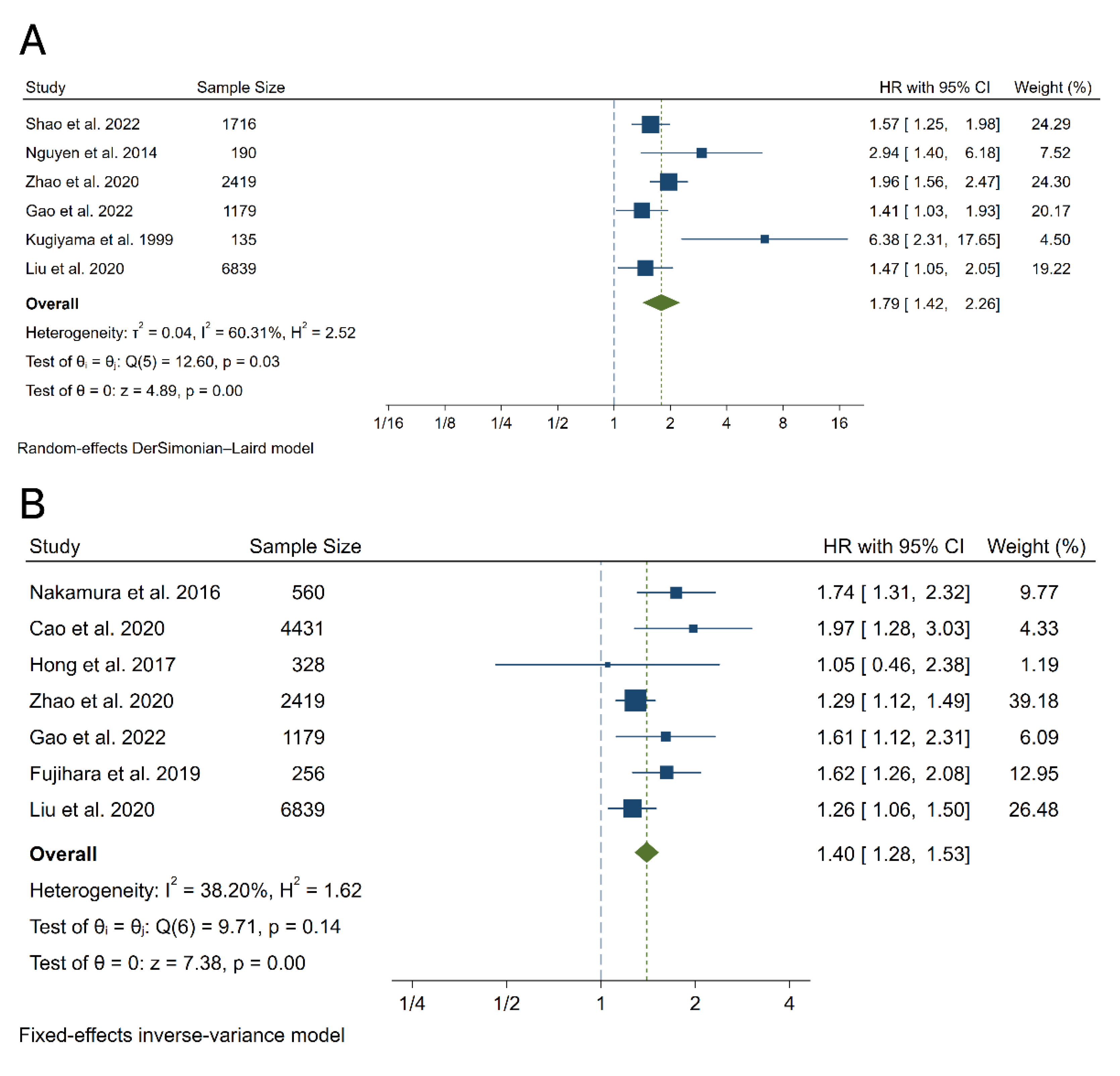
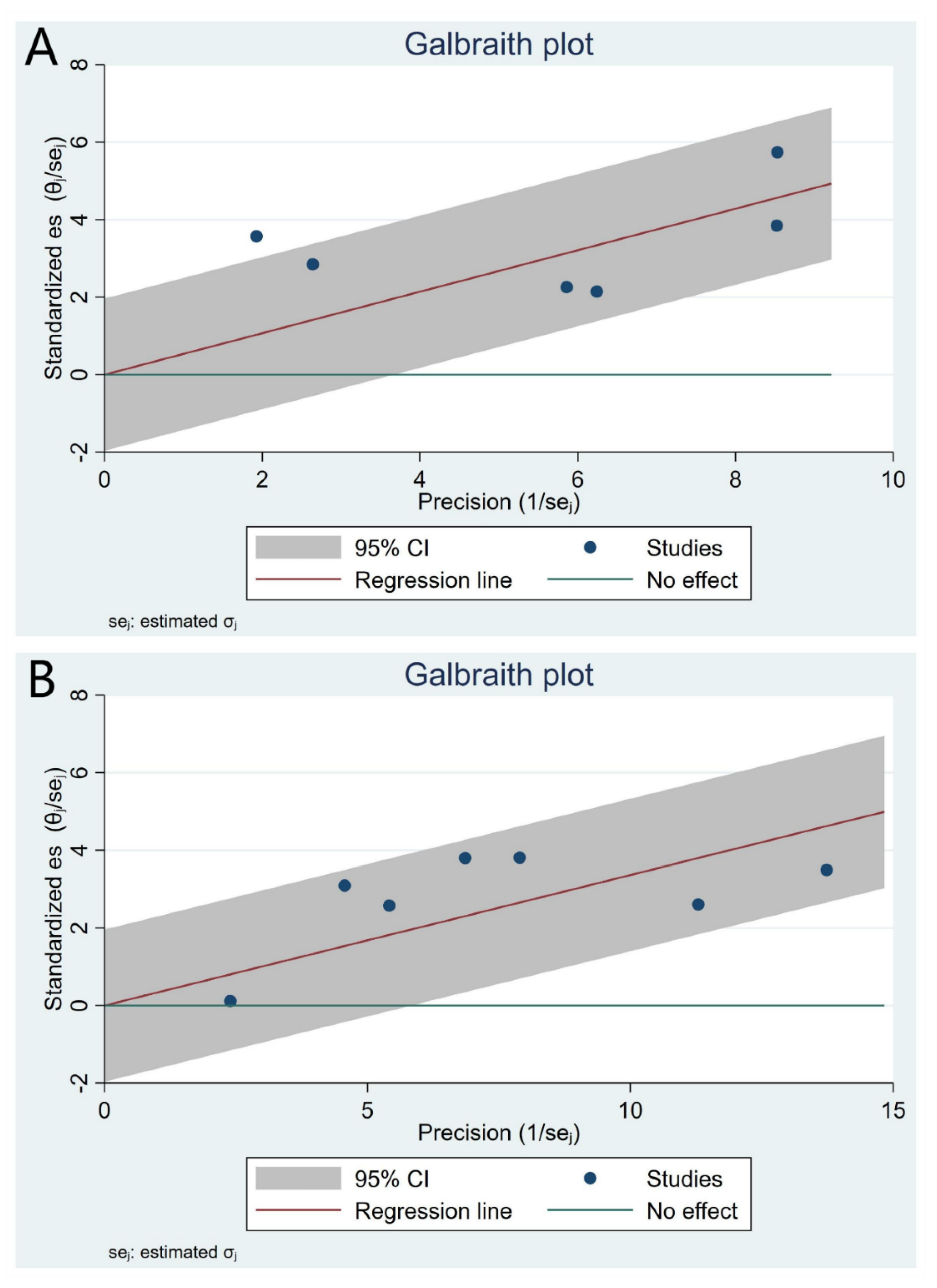
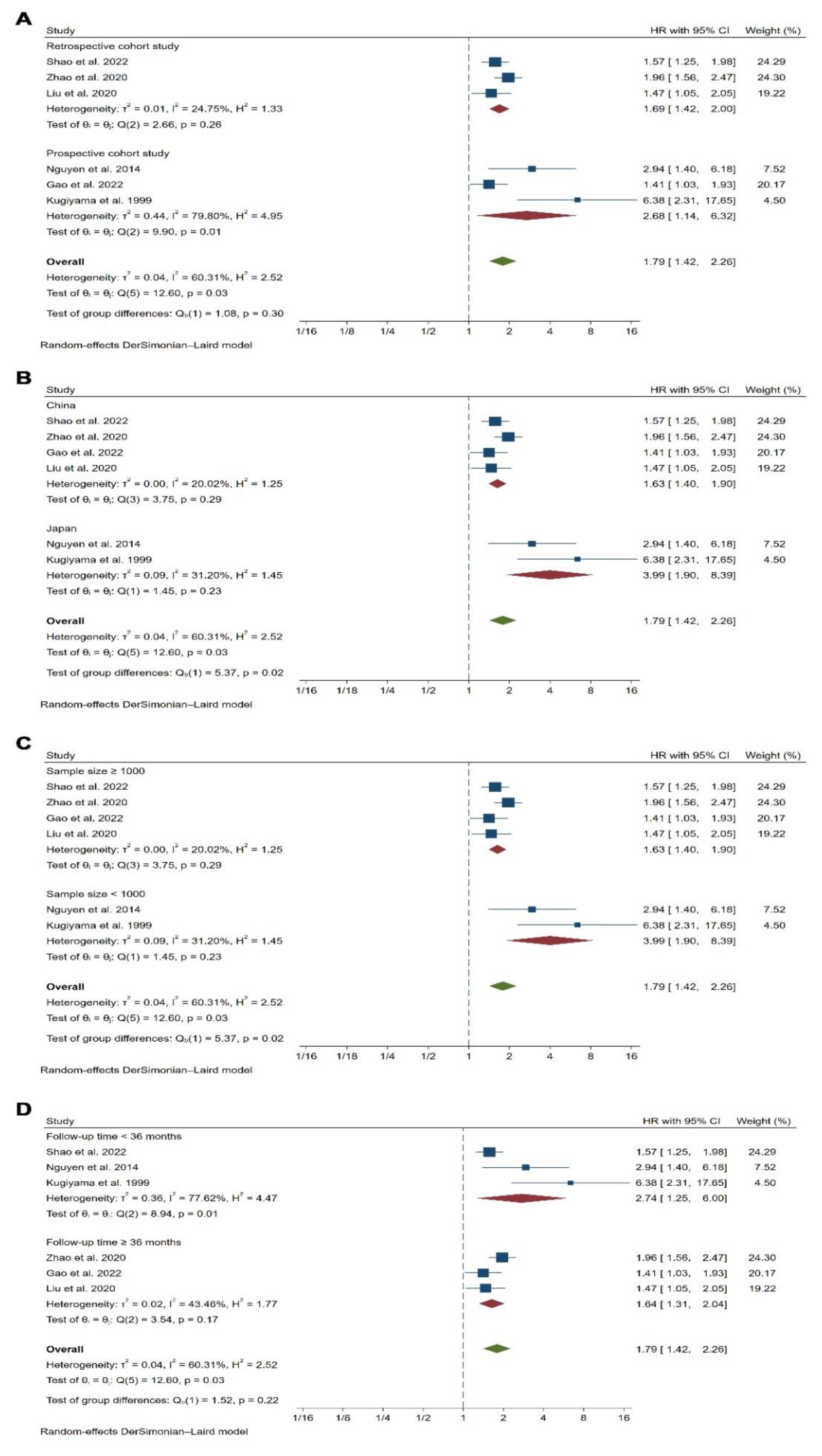
3.2. Meta-Analysis Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Ethics Declarations
References
- Sacco, R.L.; Roth, G.A.; Reddy, K.S.; Arnett, D.K.; Bonita, R.; Gaziano, T.A.; Heidenreich, P.A.; Huffman, M.D.; Mayosi, B.M.; Mendis, S.; et al. The Heart of 25 by 25: Achieving the Goal of Reducing Global and Regional Premature Deaths From Cardiovascular Diseases and Stroke: A Modeling Study From the American Heart Association and World Heart Federation. Glob. Heart 2016, 11, 251–264. [Google Scholar] [CrossRef] [PubMed]
- Duggan, J.P.; Peters, A.S.; Trachiotis, G.D.; Antevil, J.L. Epidemiology of Coronary Artery Disease. Surg. Clin. North Am. 2022, 102, 499–516. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Buring, J.E.; Badimon, L.; Hansson, G.K.; Deanfield, J.; Bittencourt, M.S.; Tokgözoğlu, L.; Lewis, E.F. Atherosclerosis. Nat. Rev. Dis. Primers 2019, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Bentzon, J.F.; Otsuka, F.; Virmani, R.; Falk, E. Mechanisms of plaque formation and rupture. Circ. Res. 2014, 114, 1852–1866. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; de Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Atherosclerosis 2019, 290, 140–205. [Google Scholar] [CrossRef] [Green Version]
- Navarese, E.P.; Robinson, J.G.; Kowalewski, M.; Kolodziejczak, M.; Andreotti, F.; Bliden, K.; Tantry, U.; Kubica, J.; Raggi, P.; Gurbel, P.A. Association between Baseline LDL-C Level and Total and Cardiovascular Mortality After LDL-C Lowering: A Systematic Review and Meta-analysis. JAMA 2018, 319, 1566–1579. [Google Scholar] [CrossRef]
- Fitzgerald, G.; Kiernan, T. PCSK9 inhibitors and LDL reduction: Pharmacology, clinical implications, and future perspectives. Expert Rev. Cardiovasc. Ther. 2018, 16, 567–578. [Google Scholar] [CrossRef]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 73, e285–e350. [Google Scholar] [CrossRef]
- Gudbjartsson, D.F.; Thorgeirsson, G.; Sulem, P.; Helgadottir, A.; Gylfason, A.; Saemundsdottir, J.; Bjornsson, E.; Norddahl, G.L.; Jonasdottir, A.; Jonasdottir, A.; et al. Lipoprotein(a) Concentration and Risks of Cardiovascular Disease and Diabetes. J. Am. Coll. Cardiol. 2019, 74, 2982–2994. [Google Scholar] [CrossRef]
- Carr, S.S.; Hooper, A.J.; Sullivan, D.R.; Burnett, J.R. Non-HDL-cholesterol and apolipoprotein B compared with LDL-cholesterol in atherosclerotic cardiovascular disease risk assessment. Pathology 2019, 51, 148–154. [Google Scholar] [CrossRef]
- Varbo, A.; Benn, M.; Nordestgaard, B.G. Remnant cholesterol as a cause of ischemic heart disease: Evidence, definition, measurement, atherogenicity, high risk patients, and present and future treatment. Pharmacol. Ther. 2014, 141, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, H.N.; Packard, C.J.; Chapman, M.J.; Borén, J.; Aguilar-Salinas, C.A.; Averna, M.; Ference, B.A.; Gaudet, D.; Hegele, R.A.; Kersten, S.; et al. Triglyceride-rich lipoproteins and their remnants: Metabolic insights, role in atherosclerotic cardiovascular disease, and emerging therapeutic strategies-a consensus statement from the European Atherosclerosis Society. Eur. Heart J. 2021, 42, 4791–4806. [Google Scholar] [CrossRef]
- Chait, A.; Ginsberg, H.N.; Vaisar, T.; Heinecke, J.W.; Goldberg, I.J.; Bornfeldt, K.E. Remnants of the Triglyceride-Rich Lipoproteins, Diabetes, and Cardiovascular Disease. Diabetes 2020, 69, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Zhang, T.Y.; Cheng, Y.J.; Ma, Y.; Xu, Y.K.; Yang, J.Q.; Zhou, Y.J. Prognostic impact of estimated remnant-like particle cholesterol in patients with differing glycometabolic status: An observational cohort study from China. Lipids Health Dis. 2020, 19, 179. [Google Scholar] [CrossRef] [PubMed]
- Shao, Q.; Yang, Z.; Wang, Y.; Li, Q.; Han, K.; Liang, J.; Shen, H.; Liu, X.; Zhou, Y.; Ma, X.; et al. Elevated Remnant Cholesterol is Associated with Adverse Cardiovascular Outcomes in Patients with Acute Coronary Syndrome. J. Atheroscler. Thromb. 2022, 29, 63397. [Google Scholar] [CrossRef] [PubMed]
- Castañer, O.; Pintó, X.; Subirana, I.; Amor, A.J.; Ros, E.; Hernáez, Á.; Martínez-González, M.; Corella, D.; Salas-Salvadó, J.; Estruch, R.; et al. Remnant Cholesterol, Not LDL Cholesterol, Is Associated with Incident Cardiovascular Disease. J. Am. Coll. Cardiol. 2020, 76, 2712–2724. [Google Scholar] [CrossRef]
- Hong, L.F.; Yan, X.N.; Lu, Z.H.; Fan, Y.; Ye, F.; Wu, Q.; Luo, S.H.; Yang, B.; Li, J.J. Predictive value of non-fasting remnant cholesterol for short-term outcome of diabetics with new-onset stable coronary artery disease. Lipids Health Dis. 2017, 16, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, S.S.; Faridi, K.F.; Joshi, P.H.; Blaha, M.J.; Kulkarni, K.R.; Khokhar, A.A.; Maddox, T.M.; Havranek, E.P.; Toth, P.P.; Tang, F.; et al. Remnant Lipoprotein Cholesterol and Mortality After Acute Myocardial Infarction: Further Evidence for a Hypercholesterolemia Paradox From the TRIUMPH Registry. Clin. Cardiol. 2015, 38, 660–667. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, S.V.; Nakamura, T.; Kugiyama, K. High remnant lipoprotein predicts recurrent cardiovascular events on statin treatment after acute coronary syndrome. Circ. J. 2014, 78, 2492–2500. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Obata, J.E.; Hirano, M.; Kitta, Y.; Fujioka, D.; Saito, Y.; Kawabata, K.; Watanabe, K.; Watanabe, Y.; Mishina, H.; et al. Predictive value of remnant lipoprotein for cardiovascular events in patients with coronary artery disease after achievement of LDL-cholesterol goals. Atherosclerosis 2011, 218, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.X.; Zhang, H.W.; Jin, J.L.; Liu, H.H.; Zhang, Y.; Gao, Y.; Guo, Y.L.; Wu, N.Q.; Hua, Q.; Li, Y.F. The longitudinal association of remnant cholesterol with cardiovascular outcomes in patients with diabetes and pre-diabetes. Cardiovasc. Diabetol. 2020, 19, 104. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.; Xu, H.; Ma, W.; Yuan, J.; Yu, M. Remnant Cholesterol Predicts Risk of Cardiovascular Events in Patients with Myocardial Infarction with Nonobstructive Coronary Arteries. J. Am. Heart Assoc. 2022, 11, e024366. [Google Scholar] [CrossRef] [PubMed]
- Kugiyama, K.; Doi, H.; Takazoe, K.; Kawano, H.; Soejima, H.; Mizuno, Y.; Tsunoda, R.; Sakamoto, T.; Nakano, T.; Nakajima, K.; et al. Remnant lipoprotein levels in fasting serum predict coronary events in patients with coronary artery disease. Circulation 1999, 99, 2858–2860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujihara, Y.; Nakamura, T.; Horikoshi, T.; Obata, J.E.; Fujioka, D.; Watanabe, Y.; Watanabe, K.; Kugiyama, K. Remnant Lipoproteins Are Residual Risk Factor for Future Cardiovascular Events in Patients with Stable Coronary Artery Disease and On-Statin Low-Density Lipoprotein Cholesterol Levels <70 mg/dL. Circ. J. 2019, 83, 1302–1308. [Google Scholar] [PubMed] [Green Version]
- Liu, H.H.; Guo, Y.L.; Zhu, C.G.; Wu, N.Q.; Gao, Y.; Xu, R.X.; Dong, Q.; Qian, J.; Dou, K.F.; Li, J.J.; et al. Synergistic effect of the commonest residual risk factors, remnant cholesterol, lipoprotein(a), and inflammation, on prognosis of statin-treated patients with chronic coronary syndrome. J. Transl. Med. 2022, 20, 243. [Google Scholar] [PubMed]
- Nordestgaard, B.G. Triglyceride-Rich Lipoproteins and Atherosclerotic Cardiovascular Disease: New Insights From Epidemiology, Genetics, and Biology. Circ. Res. 2016, 118, 547–563. [Google Scholar] [CrossRef] [PubMed]
- Quisp, R.; Martin, S.S.; Michos, E.D.; Lamba, I.; Blumenthal, R.S.; Saeed, A.; Lima, J.; Puri, R.; Nomura, S.; Tsai, M.; et al. Remnant cholesterol predicts cardiovascular disease beyond LDL and ApoB: A primary prevention study. Eur. Heart J. 2021, 42, 4324–4332. [Google Scholar] [CrossRef]
- Batt, K.V.; Avella, M.; Moore, E.H.; Jackson, B.; Suckling, K.E.; Botham, K.M. Differential effects of low-density lipoprotein and chylomicron remnants on lipid accumulation in human macrophages. Exp. Biol. Med. 2004, 229, 528–537. [Google Scholar] [CrossRef]
- Varbo, A.; Benn, M.; Tybjærg-Hansen, A.; Nordestgaard, B.G. Elevated remnant cholesterol causes both low-grade inflammation and ischemic heart disease, whereas elevated low-density lipoprotein cholesterol causes ischemic heart disease without inflammation. Circulation 2013, 128, 1298–1309. [Google Scholar] [CrossRef]
- Zheng, X.Y.; Liu, L. Remnant-like lipoprotein particles impair endothelial function: Direct and indirect effects on nitric oxide synthase. J. Lipid Res. 2007, 48, 1673–1680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawka, A.M.; Singh, R.J.; Hiddinga, H.J.; McConnell, J.P.; Eberhardt, N.L.; Caplice, N.M.; O’Brien, T. Remnant lipoproteins induce endothelial plasminogen activator inhibitor-1. Biochem. Biophys. Res. Commun. 2001, 285, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Saniabadi, A.R.; Umemura, K.; Shimoyama, M.; Adachi, M.; Nakano, M.; Nakashima, M. Aggregation of human blood platelets by remnant like lipoprotein particles of plasma chylomicrons and very low density lipoproteins. Thromb. Haemost. 1997, 77, 996–1001. [Google Scholar] [CrossRef] [PubMed]
- Nordestgaard, B.G.; Varbo, A. Triglycerides and cardiovascular disease. Lancet 2014, 384, 626–635. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Study Design | Subjects | Sample Size | Sex Female | Age (Years) | RLP-C Analysis | Mean LDL-C (mmol/L) | Follow-Up Time (Months) | Outcome Reported | Confounder Adjustment | Quality Assessment (Newcastle–Ottawa Scale) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Shao et al. 2022 [15] | China | Retrospective cohort study | Patients with ACS undergoing PCI | 1716 | 23.3% | 60 ± 10 | RLP-C > 75th vs. RLP-C ≤ 75th | 2.44 ± 0.80 | 30.9 | MACE (354) | Age, sex, BMI, current smoking, hypertension, diabetes, past MI, past PCI, CKD, statins on admission, discharged drugs, complete revascularization, STEMI, hs-CRP, GRACE risk score, left main or multivessel disease. | Selection: 4 Comparability: 2 Outcome: 2 |
| Nguyen et al. 2014 [20] | Japan | Prospective cohort study | Patients with ACS undergoing PCI | 190 | 27.9% | 70.2 (63.0 − 79.0) | RLP-C ≥ 5.4 mg/dL vs. RLP-C < 5.4 mg/dL | 2.57 ± 0.80 | 30 | MACE (42), Cardiac death (2), MI (10), Ischemia-driven revascularization (25), Stroke (30) | Age, sex, smoking, BMI, DM, HTN, Multivessel CAD, hs-CRP, HbA1c, TG, HDL-C, and LDL-C. | Selection: 4 Comparability: 2 Outcome: 2 |
| Nakamura et al. 2016 [21] | Japan | Prospective cohort study | Patients with stable CAD | 560 | 43.0% | 64 ± 9 | Continuous | 2.31 (1.92–2.51) | 33 | MACE (40), Cardiac death (13), MI (2), Ischemia-driven revascularization (17), Stroke (8) | Multivessel CAD, CRP, eGFR, BNP, non-HDL-C, and ApoA-I. | Selection: 4 Comparability: 1 Outcome: 2 |
| Cao et al. 2020 [22] | China | Retrospective cohort study | Patients with CAD | 4431 | 28.9% | 58.32 ± 12.29 | Continuous | 2.44 ± 0.89 | 61.2 | MACE (541), Cardiac death (75), UAP requiring hospitalization (132), MI (44), Repeat revascularization (181), Stroke (109) | Age, sex, smoking, BMI, DM, HTN, Family history of CAD, Baseline statin, TC, TG, HDL-C, non-HDL-C, Apo B, and LDL-C. | Selection: 4 Comparability: 2 Outcome: 2 |
| Hong et al. 2017 [17] | China | Retrospective Cohort study | Patients with stable CAD and diabetes mellitus | 328 | 36.2% | 59.2 ± 9.4 | Continuous | 2.50 ± 1.00 | 12 | MACE (47), Cardiac death (3), UAP requiring hospitalization (5), MI (8), Repeat revascularization (32) | Age, sex, smoking, BMI, HTN, Family history of CAD, Gensini scores, Lp (a), HbA1c, hs-CRP, Fibrinogen, Neutrophil count and LDL-C. | Selection: 4 Comparability: 2 Outcome: 1 |
| Zhao et al. 2020 [14] | China | Retrospective cohort study | Patients with NSTE-ACS undergoing PCI | 2419 | 28.2% | 60.08 ± 8.97 | RLP-C > 50th vs. RLP-C ≤ 50th, Continuous | 2.50 ± 0.88 | 36 | MACE (454), all-cause death (21), MI (117), ischemia-driven revascularization (316) | Age, BMI, heart rate, SBP, DM, prior MI, prior PCI, prior CABG, prior stroke, TG, TC, HDL-C, hs-CRP, eGFR, FBG, HbA1c, LVEF, principal diagnosis, discharged drugs, Left main disease, muti-vessel disease, CTO disease, diffuse disease, bifurcation disease, and number of stents. | Selection: 4 Comparability: 2 Outcome: 1 |
| Gao et al. 2022 [23] | China | Prospective cohort study | Patients with MINOCA | 1179 | 36.5% | 55.70 ± 11.8 | RLP-C > 50th vs. RLP-C ≤ 50th, Continuous | 2.29 ± 0.76 | 41.7 | MACE (168), All-cause death (18), UAP or HF requiring hospitalization (119), MI (41), Repeat revascularization (46), Stroke (109) | Age, sex, BMI, MI type, HTN, DM, and dyslipidemia. | Selection: 4 Comparability: 2 Outcome: 2 |
| Kugiyama et al. 1999 [24] | Japan | Prospective cohort study | Patients with CAD | 135 | 34.0% | 65.00 ± 9.70 | T3 vs. T1-T2 | NA | 26.8 | MACE (45) | Age, sex, smoking, HTN, DM, hypercholesterolemia, hypertriglyceridemia, low levels of HDL cholesterol, stenosis of left main coronary artery, and the number of diseased coronary arteries. | Selection: 4 Comparability: 2 Outcome: 1 |
| Fujihara et al. 2019 [25] | Japan | Prospective cohort study | Patients with stable CAD | 256 | 9.0% | 67.0 (60.0 –74.0) | Continuous | 1.60 (1.45–1.73) | 38 | MACE (33), Cardiac death (2), HF requiring hospitalization (9), MI (1), ischemia-driven revascularization (13), Stroke (30), PAD requiring endovascular treatment (1), aortic aneurysms requiring surgical treatment (3) | Smoking, TG, Lp (a), HbA1c, and ApoB. | Selection: 4 Comparability: 1 Outcome: 2 |
| Liu et al. 2020 [26] | China | Retrospective cohort study | Patients with stable CAD | 6839 | 27.6% | 58.10 ± 10.70 | RLP-C > 50th vs. RLP-C ≤ 50th, Continuous | 2.44 ± 0.92 | 54.9 | MACE (462), Cardiac death (197), MI (94), Stroke (171) | Age, sex, smoking status, prior MI, HTN, DM, LVEF, TG, LDL-C, HDL-C creatinine, statin use and types at admission, and statintypes on discharge. | Selection: 4 Comparability: 2 Outcome: 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.; Wang, Y.; Xi, Z.; Ma, Y.; Shao, C.; Wang, W.; Tang, Y.-D. Remnant-Like Particle Cholesterol and the Risk of Major Adverse Cardiovascular Events: A Systematic Review and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2022, 9, 452. https://doi.org/10.3390/jcdd9120452
Yang J, Wang Y, Xi Z, Ma Y, Shao C, Wang W, Tang Y-D. Remnant-Like Particle Cholesterol and the Risk of Major Adverse Cardiovascular Events: A Systematic Review and Meta-Analysis. Journal of Cardiovascular Development and Disease. 2022; 9(12):452. https://doi.org/10.3390/jcdd9120452
Chicago/Turabian StyleYang, Jie, Yuangengshuo Wang, Ziwei Xi, Yue Ma, Chunli Shao, Wenyao Wang, and Yi-Da Tang. 2022. "Remnant-Like Particle Cholesterol and the Risk of Major Adverse Cardiovascular Events: A Systematic Review and Meta-Analysis" Journal of Cardiovascular Development and Disease 9, no. 12: 452. https://doi.org/10.3390/jcdd9120452
APA StyleYang, J., Wang, Y., Xi, Z., Ma, Y., Shao, C., Wang, W., & Tang, Y.-D. (2022). Remnant-Like Particle Cholesterol and the Risk of Major Adverse Cardiovascular Events: A Systematic Review and Meta-Analysis. Journal of Cardiovascular Development and Disease, 9(12), 452. https://doi.org/10.3390/jcdd9120452