Referral and Lost to System Rates of Two Newborn Hearing Screening Programs in Saudi Arabia


{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
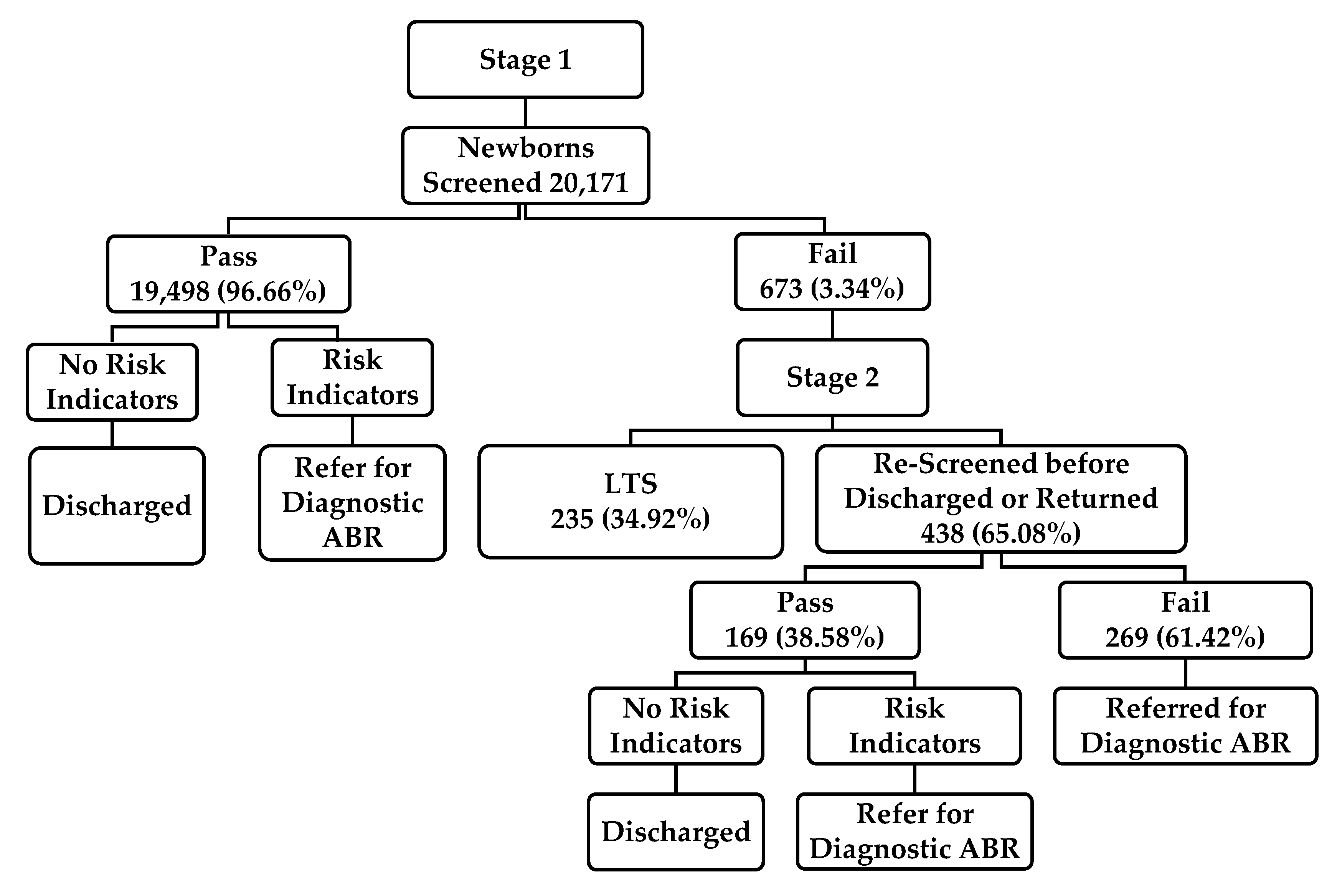
2.2. Screening Protocol
2.3. Instrumentation
3. Results
4. Discussion
5. Limitations
6. Recommendations and Future Research
7. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Deafness and Hearing Loss. Available online: https://www.who.int/news-room/fact-sheets/detail/deafness-and-hearing-loss (accessed on 14 June 2020).
- Burke, M.; Shenton, R.C.; Taylor, M. The economics of screening infants at risk of hearing impairment: An international analysis. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 212–218. [Google Scholar] [CrossRef]
- Olusanya, B.O. Screening for neonatal deafness in resource-poor countries: challenges and solutions. Res. Rep. Neonatol. 2015, 2015, 51. [Google Scholar] [CrossRef] [Green Version]
- Olusanya, B.O.; Emokpae, A.; Renner, J.; Wirz, S. Costs and performance of early hearing detection programmes in Lagos, Nigeria. Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 179–186. [Google Scholar] [CrossRef]
- Bindawas, S.M.; Vennu, V. The National and Regional Prevalence Rates of Disability, Type, of Disability and Severity in Saudi Arabia—Analysis of 2016 Demographic Survey Data. Int. J. Environ. Res. Public Heal. 2018, 15, 419. [Google Scholar] [CrossRef] [Green Version]
- General Authority for Statistics. Disability Survey. Available online: https://www.stats.gov.sa/sites/default/files/disability_survey_2017_en.pdf (accessed on 14 June 2020).
- Alyami, H.; Soer, M.; Swanepoel, A.; Pottas, L. Deaf or hard of hearing children in Saudi Arabia: Status of early intervention services. Int. J. Pediatr. Otorhinolaryngol. 2016, 86, 142–149. [Google Scholar] [CrossRef] [Green Version]
- Abolfotouh, M.; Ghieth, M.M.; Badawi, I.A. Hearing Loss and Other Ear Problems among Schoolboys in Abha, Saudi Arabia. Ann. Saudi Med. 1995, 15, 323–326. [Google Scholar] [CrossRef] [Green Version]
- Al-Rowaily, M.A.; Alfayez, A.I.; AlJomiey, M.S.; Albadr, A.M.; Abolfotouh, M. Hearing impairments among Saudi preschool children. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 1674–1677. [Google Scholar] [CrossRef] [PubMed]
- Zakzouk, S.M.; Abul Fadle, K.A.; Al Anazy, F.H. Familial hereditary progressive sensorineural hearing loss among Saudi children. Int. J. Pediatr. Otorhinolaryngol. 1995, 32, 247–255. [Google Scholar] [CrossRef]
- Cunningham, M.; Cox, E.O.; Committee on Practice and Ambulatory Medicine and the Section on Otolaryngology and Bronchoesophagology. Hearing assessment in infants and children: Recommendations beyond neonatal screening. J. Pediatr. 2003, 111, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Joint Committee on Infant Hearing. Year 2007 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs. J. Pediatr. 2007, 120, 898–921. [Google Scholar] [CrossRef] [Green Version]
- Barnett, M.A.; Gustafsson, H.; Deng, M.; Mills-Koonce, W.R.; Cox, M. Bidirectional Associations Among Sensitive Parenting, Language Development, and Social Competence. Infant Child Dev. 2012, 21, 374–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bess, F.H.; Dodd-Murphy, J.; Parker, R.A. Children with Minimal Sensorineural Hearing Loss: Prevalence, Educational Performance, and Functional Status. Ear Hear. 1998, 19, 339–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henner, J.; Caldwell-Harris, C.L.; Novogrodsky, R.; Hoffmeister, R. American Sign Language Syntax and Analogical Reasoning Skills Are Influenced by Early Acquisition and Age of Entry to Signing Schools for the Deaf. Front. Psychol. 2016, 7, 167. [Google Scholar] [CrossRef] [PubMed]
- McKay, S.; Gravel, J.S.; Tharpe, A.M. Amplification Considerations for Children with Minimal or Mild Bilateral Hearing Loss and Unilateral Hearing Loss. Trends Amplif. 2008, 12, 43–54. [Google Scholar] [CrossRef] [Green Version]
- Tasker, S.L.; Nowakowski, M.E.; Schmidt, L.A. Joint Attention and Social Competence in Deaf Children with Cochlear Implants. J. Dev. Phys. Disabil. 2010, 22, 509–532. [Google Scholar] [CrossRef]
- Black, P.A.; Glickman, N.S. Demographics, Psychiatric Diagnoses, and Other Characteristics of North American Deaf and Hard-of-Hearing Inpatients. J. Deaf. Stud. Deaf. Educ. 2006, 11, 303–321. [Google Scholar] [CrossRef]
- Glickman, N. Do You Hear Voices? Problems in Assessment of Mental Status in Deaf Persons with Severe Language Deprivation. J. Deaf. Stud. Deaf. Educ. 2007, 12, 127–147. [Google Scholar] [CrossRef]
- Grosse, S.D. Education cost savings from early detection of hearing loss: New findings. Volta Voice 2007, 14, 38–40. [Google Scholar]
- Lieu, J.; Tye-Murray, N.; Karzon, R.K.; Piccirillo, J.F. Unilateral hearing loss is associated with worse speech-language scores in children. J. Pediatr. 2010, 125, e1348–e1355. [Google Scholar] [CrossRef] [Green Version]
- National Center for Hearing Assessment and Management. Issues and Evidence: Cost Efficiency of Newborn Hearing Screening (p. 7). Available online: http://www.infanthearing.org/summary/cost.html (accessed on 14 June 2020).
- Kemp, D.T. Otoacoustic emissions, their origin in cochlear function, and use. Br. Med Bull. 2002, 63, 223–241. [Google Scholar] [CrossRef]
- MacNeil, J.R.; Liu, C.-L.; Stone, S.; Farrell, J.M. Evaluating Families’ Satisfaction with Early Hearing Detection and Intervention Services in Massachusetts. Am. J. Audiol. 2007, 16, 29–56. [Google Scholar] [CrossRef]
- Berg, A.L.; Prieve, B.A.; Serpanos, Y.C.; Wheaton, M.A. Ba Hearing Screening in a Well-Infant Nursery: Profile of Automated ABR-Fail/OAE-Pass. J. Pediatr. 2011, 127, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Vohr, B.R.; Oh, W.; Stewart, E.J.; Bentkover, J.D.; Gabbard, S.; Lemons, J.; Papile, L.-A.; Pye, R. Comparison of costs and referral rates of 3 universal newborn hearing screening protocols. J. Pediatr. 2001, 139, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Joint Committee on Infant Hearing. Year 2000 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs. J. Pediatr. 2000, 106, 798–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widen, J.E.; Folsom, R.C.; Cone-Wesson, B.; Carty, L.; Dunnell, J.J.; Koebsell, K.; Levi, A.; Mancl, L.; Ohlrich, B.; Trouba, S.; et al. Identification of neonatal hearing impairment: Hearing status at 8–12 months corrected age using a visual reinforcement audiometry protocol. Ear Hear. 2000, 21, 471–487. [Google Scholar] [CrossRef] [PubMed]
- Stapells, D.R. Threshold estimation by the tone-evoked auditory brainstem response: A literature meta-analysis. Am. J. Speech Lang Pathol. 2000, 24, 74–83. [Google Scholar]
- U. S. Preventive Services Task Force. Newborn hearing screening: recommendations and rationale. Am. Fam. Physician 2001, 64, 1995–2000. [Google Scholar]
- Centers for Disease Control and Prevention. Hearing Loss in Children: Data and Statistics. Newborn Hearing Screening and Diagnosis. 2019. Available online: http://www.cdc.gov/ncbddd/hearingloss/data.html (accessed on 14 June 2020).
- Harrison, M.; Roush, J.; Wallace, J. Trends in Age of Identification and Intervention in Infants with Hearing Loss. Ear Hear. 2003, 24, 89–95. [Google Scholar] [CrossRef]
- Hoffman, J.; Beauchaine, K. Babies with Hearing Loss: Steps for Effective Intervention. ASHA Lead. 2007, 12, 8–23. [Google Scholar] [CrossRef]
- Kennedy, C.; McCann, D.; Campbell, M.J.; Kimm, L.; Thornton, R. Universal newborn screening for permanent childhood hearing impairment: an 8-year follow-up of a controlled trial. Lancet 2005, 366, 660–662. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Summary of 2017 National EHDI Data. Available online: https://www.cdc.gov/ncbddd/hearingloss/2017-data/01-data-summary.html (accessed on 14 June 2020).
- Khoza-Shangase, K.; Michal, G. Early Intervention in Audiology: Exploring the Current Status from a Developing Country Context. Br. J. Med. Med Res. 2014, 4, 2238–2249. [Google Scholar] [CrossRef]
- Council of Cooperative Health Insurance Council News. Available online: https://www.cchi.gov.sa/MediaCenter/NEWS/Pages/news04-02-2018-02.aspx (accessed on 15 June 2020).
- Saudi Health Council. Health Insurance Companies Cover Hearing Aids. Available online: https://shc.gov.sa/Arabic/CouncilDecisions/Pages/Decisions139.aspx (accessed on 15 June 2020).
- Saudi Health Council. National Program for Hearing Impairment. Available online: https://shc.gov.sa/Arabic/CouncilDecisions/Pages/Decisions4.aspx (accessed on 15 June 2020).
- Ministry of Health. MOH News: MOH Launches the 1st Phase of Newborn Screening for Hearing-Loss and CCHD Program. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2016-10-09-001.aspx (accessed on 15 June 2020).
- Ministry of Health. MOH News: 90% of the Newborns had Cardiac Diagnosis. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/news-2018-03-12-003.aspx (accessed on 15 June 2020).
- American Speech-Language-Hearing Association. Newborn Hearing Screening. Available online: https://www.asha.org/PRPSpecificTopic.aspx?folderid=8589935234§ion=Key_Issues#Protocols (accessed on 15 June 2020).
- Alexander, D.; Van Dyck, P.C. A Vision of the Future of Newborn Screening. J. Pediatr. 2006, 117, S350–S354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Speech-Language-Hearing Association. Loss to Follow-Up in Early Hearing Detection and Intervention. Available online: http://www.infanthearing.org/coordinator_toolkit/section13/46_follow_up.pdf (accessed on 15 June 2020).
- Al-Sayed, A.A.; AlSanosi, A. Cochlear implants in children: A cross-sectional investigation on the influence of geographic location in Saudi Arabia. J. Fam. Commun. Med. 2017, 24, 118–121. [Google Scholar]
- Folsom, R.C.; Widen, J.E.; Vohr, B.R.; Cone-Wesson, B.; Gorga, M.P.; Sininger, Y.S.; Norton, S.J. Identification of Neonatal Hearing Impairment: Recruitment and Follow-Up. Ear Hear. 2000, 21, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-L.; Farrell, J.; MacNeil, J.R.; Stone, S.; Barfield, W. Evaluating Loss to Follow-up in Newborn Hearing Screening in Massachusetts. J. Pediatr. 2008, 121, e335–e343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheepers, L.J.; Swanepoel, D.W.; Le Roux, T. Why parents refuse newborn hearing screening and default on follow-up rescreening—A South African perspective. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 652–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, K.R. The current status of EHDI programs in the United States. Ment. Retard. Dev. Disabil. Res. Rev. 2003, 9, 79–88. [Google Scholar] [CrossRef]
- Meyer, M.E.; Swanepoel, D.W. Newborn hearing screening in the private health care sector - a national survey. S. Afr. Med J. 2011, 101, 665–667. [Google Scholar]
- Arnold, C.L.; Davis, T.C.; Humiston, S.G.; Bocchini, J.A.; Bass, P.F.; Bocchini, A.; Kennen, E.M.; White, K.; Forsman, I. Infant Hearing Screening: Stakeholder Recommendations for Parent-Centered Communication. J. Pediatr. 2006, 117, S341–S354. [Google Scholar] [CrossRef] [Green Version]
- Theunissen, M.; Swanepoel, D.W. Early hearing detection and intervention services in the public health sector in South Africa. Int. J. Audiol. 2008, 47, S23–S29. [Google Scholar] [CrossRef]
- Habib, H.S.; Abdelgaffar, H. Neonatal hearing screening with transient evoked otoacoustic emissions in Western Saudi Arabia. Int. J. Pediatr. Otorhinolaryngol. 2005, 69, 839–842. [Google Scholar] [CrossRef] [PubMed]
- Al-Shaikh, A.H.; Zakzouk, S.M. The prevalence of severe to profound sensorineural hearing loss in Saudi children and the need for cochlear implants. Int. Congr. Ser. 2003, 1240, 339–343. [Google Scholar] [CrossRef]
- World Health Organization. Global Estimates on Prevalence of Hearing Loss. Available online: https://www.who.int/pbd/deafness/WHO_GE_HL.pdf (accessed on 15 June 2020).
- Moeller, M.P. Early intervention and language development in children who are deaf and hard of hearing. J. Pediatr. 2000, 106, e43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saudi Vision 2030. National Transformation Program: Strategic Objectives. Available online: https://vision2030.gov.sa/sites/default/files/attachments/NTP%20English%20Public%20Document_2810.pdf (accessed on 15 June 2020).
- Luterman, D. The Counseling Relationship. ASHA Lead. 2006, 11, 8–33. [Google Scholar] [CrossRef]
- Joint Committee on Infant Hearing. Year 2019 position statement: Principles and guidelines for early hearing detection and intervention programs. J. Ear Hear. Detec. Interv. 2019, 4, 1–44. [Google Scholar]

© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alanazi, A.A. Referral and Lost to System Rates of Two Newborn Hearing Screening Programs in Saudi Arabia. Int. J. Neonatal Screen. 2020, 6, 50. https://doi.org/10.3390/ijns6030050
Alanazi AA. Referral and Lost to System Rates of Two Newborn Hearing Screening Programs in Saudi Arabia. International Journal of Neonatal Screening. 2020; 6(3):50. https://doi.org/10.3390/ijns6030050
Chicago/Turabian StyleAlanazi, Ahmad A. 2020. "Referral and Lost to System Rates of Two Newborn Hearing Screening Programs in Saudi Arabia" International Journal of Neonatal Screening 6, no. 3: 50. https://doi.org/10.3390/ijns6030050
APA StyleAlanazi, A. A. (2020). Referral and Lost to System Rates of Two Newborn Hearing Screening Programs in Saudi Arabia. International Journal of Neonatal Screening, 6(3), 50. https://doi.org/10.3390/ijns6030050