
Landscape of Spinal Muscular Atrophy Newborn Screening in the United States: 2018–2021

Abstract
:1. Introduction
2. SMA Screening Method
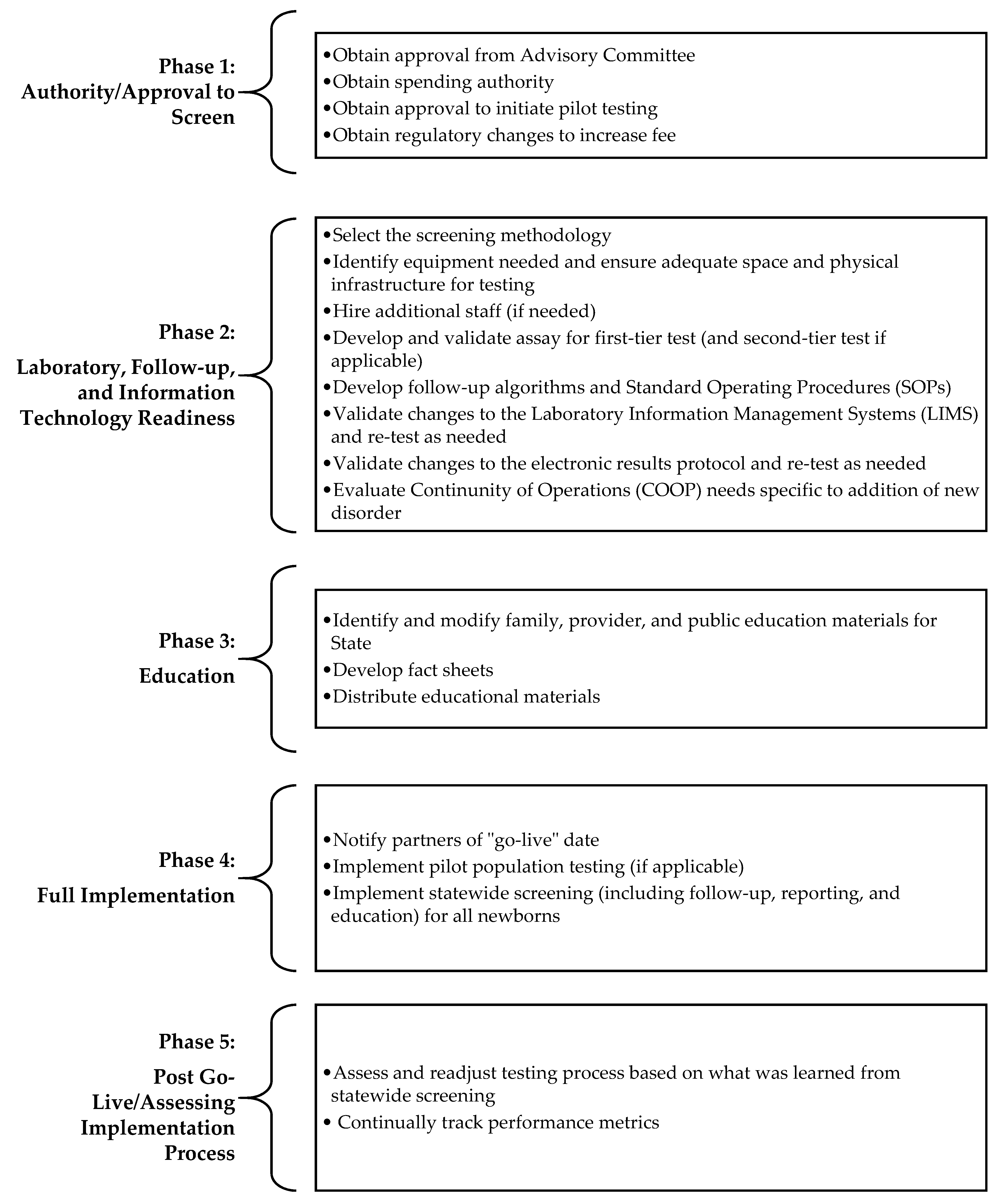
3. SMA Implementation Process and Screening Considerations
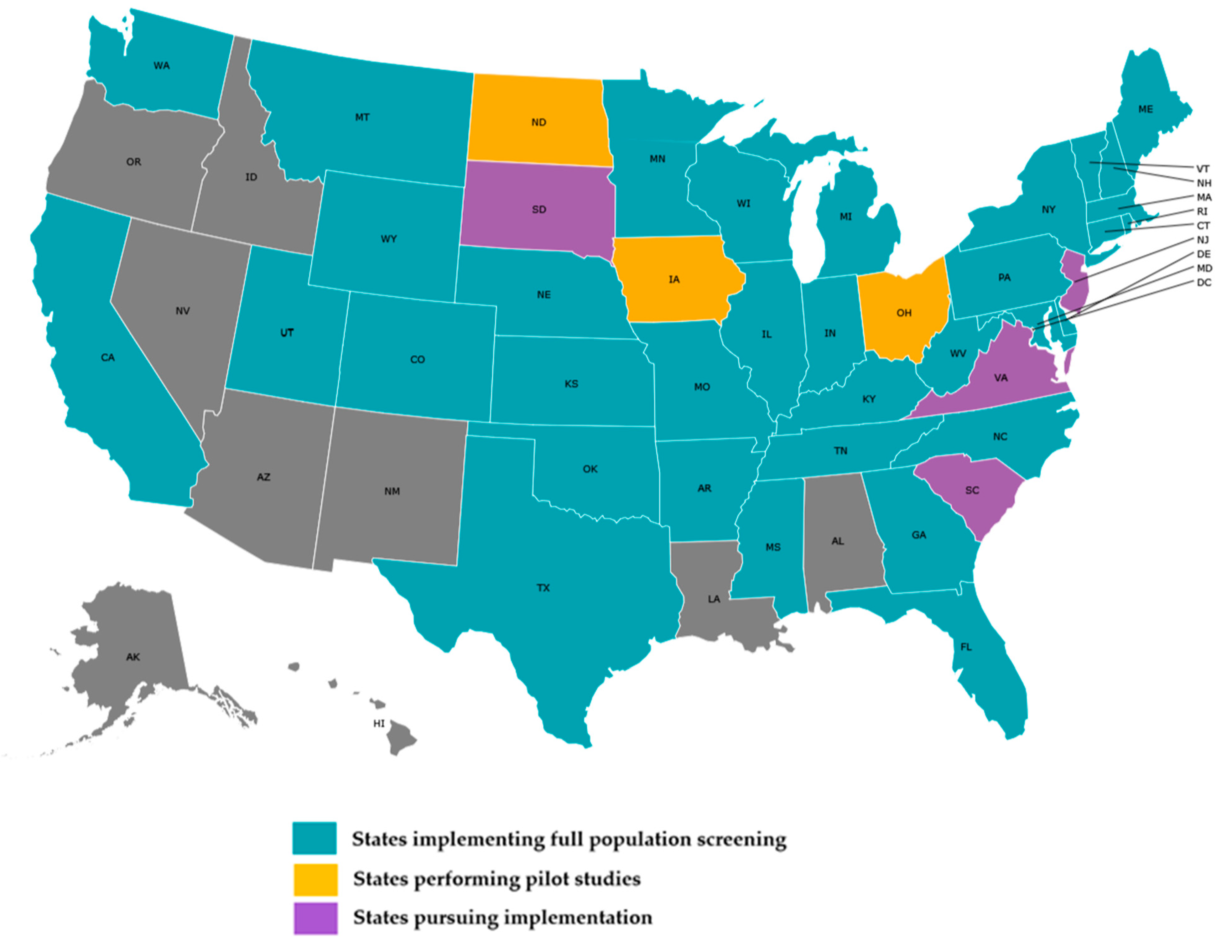
4. State of SMA NBS Implementation
5. Challenges
6. Lessons Learned and Recommendations
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| States Offering Population NBS for SMA as of June 2021 * | First-Tier Method | First-Tier Target | Second-Tier Method ^ | Second-Tier Target | Multiplex with SCID |
| Arkansas | qPCR | SMN1 | None | N/A | Yes |
| California | qPCR | SMN1 | None | N/A | No |
| Colorado | qPCR | SMN1 | None | N/A | Yes |
| Connecticut | qPCR | SMN1 | None | N/A | Yes |
| Delaware | qPCR | SMN1 | Multiplex Ligation PCR Amplification (MLPA) | SMN1and SMN2 | No |
| Florida | qPCR | SMN1 | None | N/A | Yes |
| Georgia | qPCR | SMN1 | None | N/A | Yes |
| Illinois | qPCR | SMN1 | None | N/A | Yes |
| Indiana | qPCR | SMN1 | None | N/A | Yes |
| Kansas | qPCR | SMN1 | Digital drop PCR | SMN2 | Yes |
| Kentucky | qPCR | SMN1 | None | N/A | Yes |
| Maine ** | qPCR | SMN1 | qPCR | SMN1exon 7 (Assay A) AND SMN1exon 7, SMN1intron 7 (Assay B) followed by sequencing as a third tier if all replicates show absent exon 7 (Assay A) and one or more replicates show present Exon 7 (Assay B) | No |
| Maryland | qPCR | SMN1 | None | N/A | Yes |
| Massachusetts ** | qPCR | SMN1 | qPCR | SMN1exon 7 (Assay A) AND SMN1exon 7, SMN1intron 7 (Assay B) followed by sequencing as a third tier if all replicates show absent exon 7 (Assay A) and one or more replicates show present Exon 7 (Assay B) | No |
| Michigan | qPCR | SMN1 | None | N/A | Yes |
| Minnesota | qPCR | SMN1 | None | N/A | Yes |
| Mississippi | qPCR | SMN1 | None | N/A | Yes |
| Missouri | qPCR | SMN1 | None | N/A | Yes |
| Montana | qPCR | SMN1 | Digital drop PCR | SMN2 | Yes |
| Nebraska | qPCR | SMN1 | None | N/A | Yes |
| New Hampshire ** | qPCR | SMN1 | qPCR | SMN1exon 7 (Assay A) AND SMN1exon 7, SMN1intron 7 (Assay B) followed by sequencing as a third tier if all replicates show absent exon 7 (Assay A) and one or more replicates show present Exon 7 (Assay B) | No |
| New York | qPCR | SMN1 | Digital drop PCR | SMN2 | Yes |
| North Carolina | qPCR | SMN1 | None | N/A | Yes |
| Oklahoma | qPCR | SMN1 | None | N/A | No |
| Pennsylvania | qPCR | SMN1 | Multiplex Ligation PCR Amplification (MLPA) | SMN2 | No |
| Rhode Island ** | qPCR | SMN1 | qPCR | SMN1exon 7 (Assay A) AND SMN1exon 7, SMN1intron 7 (Assay B) followed by sequencing as a third tier if all replicates show absent exon 7 (Assay A) and one or more replicates show present Exon 7 (Assay B) | No |
| Tennessee | qPCR | SMN1 | Multiplex Ligation PCR Amplification (MLPA) | SMN2 | Yes |
| Texas | qPCR | SMN1 | RT-PCR | SMN2 | Yes |
| Utah | qPCR | SMN1 | None | N/A | Yes |
| Vermont ** | qPCR | SMN1 | qPCR | SMN1exon 7 (Assay A) AND SMN1exon 7, SMN1intron 7 (Assay B) followed by sequencing as a third tier if all replicates show absent exon 7 (Assay A) and one or more replicates show present Exon 7 (Assay B) | No |
| Washington | qPCR | SMN1 | None | N/A | Yes |
| West Virginia | qPCR | SMN1 | None | N/A | Yes |
| Wisconsin | qPCR | SMN1 | Digital drop PCR | SMN2 | Yes |
| Wyoming | qPCR | SMN1 | None | N/A | Yes |
- * Not all states have a newborn screening laboratory; some newborn screening programs send their dried blood spot specimens to another laboratory. ^ While many states do not have a second-tier screen for SMA, many will perform a confirmation duplicate by using the same dried blood spot to repeat the qPCR for SMN1 exon 7 deletion the following day. ** Massachusetts has developed, validated and implemented a three-tier, high-throughput algorithm for the detection of SMA-detected infants in Massachusetts, Maine, New Hampshire, Rhode Island, and Vermont [11].
References
- Health Resources and Services Administration. Advisory Committee on Heritable Disorders in Newborns and Children. Available online: https://www.hrsa.gov/advisory-committees/heritable-disorders/index.html (accessed on 17 December 2020).
- Association of Public Health Laboratories. NewSTEPs. Newborn Screening Status for All Disorders. Available online: https://www.newsteps.org/resources/data-visualizations/newborn-screening-status-all-disorders (accessed on 5 May 2021).
- CureSMA. SMA Overview. Available online: https://www.curesma.org/about-sma/ (accessed on 10 May 2021).
- Kemper, A.R.; Ream, M.A.; Lam, K.K. Review of Newborn Screening Implementation for Spinal Muscular Atrophy Final Report. Available online: https://www.hrsa.gov/sites/default/files/hrsa/advisory-committees/heritable-disorders/reports-recommendations/sma-nbs-implementation-report.pdf (accessed on 8 June 2021).
- Kay, D.M.; Stevens, C.F.; Parker, A.; Saavedra-Matiz, C.A.; Sack, V.; Chung, W.K.; Chiriboga, C.A.; Engelstad, K.; Laureta, E.; Farooq, O.; et al. Implementation of population-based newborn screening reveals low incidence of spinal muscular atrophy. Genet. Med. 2020, 22, 1296–1302. [Google Scholar] [CrossRef]
- Verhaart, I.E.; Robertson, A.; Leary, R.; McMacken, G.; König, K.; Kirschner, J.; Jones, C.C.; Cook, S.F.; Lochmüller, H. A Multi-source Approach to Determine SMA Incidence and Research Ready Population. Available online: https://link.springer.com/content/pdf/10.1007/s00415-017-8549-1.pdf (accessed on 10 June 2021).
- CureSMA. SMA and Genetics. Available online: https://www.curesma.org/genetics/ (accessed on 10 May 2021).
- National Center for Biotechnology Information. “PubChem Gene Summary for NCBI Gene 6606” PubChem. Available online: https://pubchem.ncbi.nlm.nih.gov/gene/SMN1/human (accessed on 5 January 2021).
- National Institutes of Health. National Institute of Neurological Disorders and Stroke Spinal Muscular Atrophy Fact Sheet”, NINDS, Publication Date May 2019, NIH Publication No. 19-NS-5597. Available online: https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Spinal-Muscular-Atrophy-Fact-Sheet (accessed on 10 May 2021).
- National Organization for Rare Disorders. Rare Disease Database: Spinal Muscular Atrophy. Available online: https://rarediseases.org/rare-diseases/spinal-muscular-atrophy/ (accessed on 6 January 2021).
- Hale, J.; Darras, B.; Swoboda, K.; Estrella, E.; Chen, J.; Abbott, M.-A.; Hay, B.; Kumar, B.; Counihan, A.; Gerstel-Thompson, J.; et al. Massachusetts’ Findings from Statewide Newborn Screening for Spinal Muscular Atrophy. Int. J. Neonatal Screen. 2021, 7, 26. [Google Scholar] [CrossRef] [PubMed]
- Dangouloff, T.; Servais, L. Clinical Evidence Supporting Early Treatment of Patients with Spinal Muscular Atrophy: Current Perspectives. Ther. Clin. Risk Manag. 2019, ume 15, 1153–1161. [Google Scholar] [CrossRef] [Green Version]
- Association of Public Health Laboratories. NewSTEPs New Disorder Readiness Scale. Available online: https://www.newsteps.org/sites/default/files/newdisorderreadinessstool_May2021_.pdf (accessed on 30 April 2021).
- Pass, K.; Green, N.S.; Lorey, F.; Sherwin, J.; Comeau, A.M. Pilot programs in newborn screening. Ment. Retard. Dev. Disabil. Res. Rev. 2006, 12, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Kemper, A.R.; Lam, K.K. Newborn Screening for Spinal Muscular Atrophy Phase I: Update of the Evidence Review. Available online: https://www.hrsa.gov/sites/default/files/hrsa/advisory-committees/heritable-disorders/meetings/20170803/kemper.pdf (accessed on 8 June 2021).
- Hale, K.; Kellar-Guenther, Y.; McKasson, S.; Singh, S.; Ojodu, J. Expanding Newborn Screening for Pompe Disease in the United States: The NewSTEPs New Disorders Implementation Project, a Resource for New Disorder Implementation. Int. J. Neonatal Screen. 2020, 6, 48. [Google Scholar] [CrossRef]


| SMA Screening Methodologies | # of States |
|---|---|
| Multiplex with SCID | 25 |
| First-tier SMA screen using teal-time PCR for detection of homozygous deletion of exon 7 in SMN1 | 34 |
| First- and second-tier SMA screen | 8 |
| First-, second-, and third-tier SMA screen | 5 |
| Laboratory Considerations |
|---|
What screening method should be utilized?
|
| What will be the cutoff value and reference gene? |
| What reference materials to use in order to calibrate instrumentation? |
| What material should be utilized for daily positive quality control (QC), and from where do you obtain it? |
| Should the SMN2 copy number be determined within the screening lab? If yes, why and by what method? |
| How will you validate your Laboratory Information Management Systems (LIMS) |
Considerations for multiplexing with SCID:Platforms used
|
| Follow-up Program Considerations |
| What are the reporting and follow-up guidelines? |
| What follow-up data should be collected? Both upon diagnosis and after diagnosis? Lab results? Clinical findings? Other? |
| What does surveillance look like for SMA? |
| How to interpret results of multiplexed assays? |
| What specialists need to be involved in the follow-up process? |
| Are specialists determining SMA type based on SMN2 copy numbers and clinical symptoms present at diagnosis? |
| What wording should be used for the interpretation of normal results/positive results on the NBS report? |
Specialist involvement:
|
| What is the referral rate? How many (or what % of) released results to primary care physician/specialist yielded an SMA diagnosis? |
| Disorder | No. of States | Mean (Months) | Median (Months) | Min (Months) | Max (Months) | Range (Months) |
|---|---|---|---|---|---|---|
| Pompe | 11 | 39.64 | 28 | 13 | 99 | 86 |
| MPS I | 13 | 36.92 | 28 | 13 | 75 | 62 |
| X-ALD | 8 | 27.63 | 30.5 | 16 | 36 | 20 |
| SMA | 5 | 24.40 | 20 | 17 | 38 | 21 |
| Disorder | Activity | Average Time (Months) |
|---|---|---|
| Pompe | Develop and gain buy-in for STFU protocols for abnormal screens | 15.13 |
| MPS I | Identify screening methodology/assay for first-tier testing | 14.80 |
| X-ALD | Develop/validate assay for second-tier testing | 19.67 |
| SMA | Obtain approval from the state budget authority | 10 |
| Challenges | Description |
|---|---|
| Competing Priorities/Shift of Duties | Several states experienced delays as a result of the COVID-19 pandemic. NBS program staff from all areas shifted focus from routine duties to address the crisis, including providing testing for COVID-19. This affected NBS staff, fiscal/accounting staff, and other support staff in public health laboratories. |
| Procurement of Lab Supplies | The COVID-19 pandemic affected the ability to procure lab supplies needed for SMA screening, such as pipette tips and reagents. |
| External Partners | The COVID-19 pandemic impacted staffing situations with external partners. |
| Legislative Delays | The COVID-19 pandemic delayed the legislative process, resulting in a delay in the approval and implementation of SMA screening. |
| Malfunctioning of Instrumentation | One program experienced problems with liquid handling instruments. The instruments were not functioning correctly due to manufacturing errors. The program reported that one system had to be replaced and the other modified. The manufacturer was responsive and spent several days working onsite to fix the issue. This issue took approximately six weeks to resolve. |
| Steps | Recommendation |
|---|---|
| Step 1 | Order supplies needed with a longer lead time to ensure that manufacturing and transportation delays do not negatively impact validation timelines. |
| Step 2 | Continue to meet with implementation team composed of laboratory leadership, technical experts, follow-up leadership, and informatics support staff to ensure that all parties are informed of validation and regulatory progress. |
| Step 3 | Hire additional staff whenever possible before staffing shortages force timeline delays. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hale, K.; Ojodu, J.; Singh, S. Landscape of Spinal Muscular Atrophy Newborn Screening in the United States: 2018–2021. Int. J. Neonatal Screen. 2021, 7, 33. https://doi.org/10.3390/ijns7030033
Hale K, Ojodu J, Singh S. Landscape of Spinal Muscular Atrophy Newborn Screening in the United States: 2018–2021. International Journal of Neonatal Screening. 2021; 7(3):33. https://doi.org/10.3390/ijns7030033
Chicago/Turabian StyleHale, Kshea, Jelili Ojodu, and Sikha Singh. 2021. "Landscape of Spinal Muscular Atrophy Newborn Screening in the United States: 2018–2021" International Journal of Neonatal Screening 7, no. 3: 33. https://doi.org/10.3390/ijns7030033
APA StyleHale, K., Ojodu, J., & Singh, S. (2021). Landscape of Spinal Muscular Atrophy Newborn Screening in the United States: 2018–2021. International Journal of Neonatal Screening, 7(3), 33. https://doi.org/10.3390/ijns7030033