1. Introduction
Congenital hypothyroidism (CH) treatment shortly after birth effectively prevents intellectual disability [
1,
2,
3]. Most screening strategies use a postnatal thyrotropin (TSH) cutoff (on all infants or a subset with low thyroxine levels) to report a presumptive positive result [
2]. The following situations, however, may escape diagnosis due to a delay or lack of TSH elevation:
Infants with prematurity/low birthweight [
4,
5,
6,
7,
8,
9,
10,
11,
12], cardiac anomalies [
5,
13,
14], or Down syndrome (DS) [
15,
16,
17].
Monozygotic twins (same-sex twinning has been an adequate surrogate marker for screening) due to antenatal sharing of blood [
18,
19].
Central hypothyroidism [
20,
21] through inappropriately low TSH.
The first category does not have a clear causation although hypothalamic–pituitary immaturity and exposure to corticosteroids or dopamine (substances that lower TSH) have been proposed [
22,
23]. Conversely, exposure to iodine for procedures [
3,
24] and recovery from sick euthyroid syndrome [
25,
26] may transiently increase TSH in infants without CH. Various screening strategies to capture missed CH cases have been reported differing in timing (2–12 weeks of life), frequency (1–3 screens), TSH cutoff (>6 to >20 mIU/L), and use of thyroxine results [
1,
5,
8,
9,
12,
13,
27,
28,
29].
The last two categories have well-understood physiologic causes [
18]. Clinical recognition of central hypothyroidism will occur in many cases due to association with signs of hypopituitarism such as craniofacial/midline defects, genetic diagnoses, recurrent hypoglycemia, recalcitrant hypotension, or micropenis. Screening programs that report low thyroxine levels in absence of TSH elevation might also detect central hypothyroidism [
1].
Most previous studies have investigated national or regional databases for infants with very low birthweight or congenital heart disease and have suggested a prevalence of CH at least 10 times the rate described for the general infant population [
12]. Despite the documented risk for these and other groups, most infants do not receive mandated universal or targeted secondary screening [
2,
12,
30,
31]. We now report on targeted secondary screening in the long-term clinical experience of a large group practice which sought to identify more infants at risk for intellectual disability due to CH.
2. Materials and Methods
The clinical protocol started in 2009 at Kaiser Permanente Southern California facilities, a health care system serving >4.6 million people with approximately 37,000 annual births at 14 plan and 4 contracted hospitals. The physicians were members of the Southern California Permanente Medical Group that provides exclusive care to patients residing in Southern California enrolled in Kaiser Health Plan. Human subjects approval was obtained through the Kaiser Permanente Southern California Institutional Review Board. Initial and ongoing education was provided to all pediatricians and neonatologists to implement the secondary screening protocol.
The California Newborn Screen (“primary screen”) for hypothyroidism consists of TSH testing >12 h of life with abnormal cutoff >29 mIU/L. The targeted TSH secondary screen was developed by the Southern California Permanente Medical Group to clinically manage their patients and was not associated with the California Newborn Screening Program or specific guidelines from a professional society. The screening was performed at approximately 2 weeks of life at the SCPMG Regional Reference Laboratory using the Abbott Architect TSH assay on spun serum for same-sex multiple gestation (SSM) infants, infants with congenital heart disease (CHD) admitted to the Neonatal Intensive Care Unit (NICU), and very low birthweight infants ≤ 1500 g (VLBW). VLBW infants also received TSH screenings at 4 and 6 weeks. Infants with TSH values ≥10 mIU/L on secondary screens were considered abnormal (CH cases) if confirmed on follow-up testing. A pediatric endocrinologist was consulted on every positive case prior to instituting treatment. The clinical protocol relied on the relative simplicity of using TSH measurements due to:
The familiarity of pediatricians and neonatologists with the primary screen in California based solely on TSH.
The high prevalence of hypothyroxinemia without CH for the low-birth-weight population in the NICU.
The current practice of the 15 pediatric endocrinologists in the medical group that relies almost entirely on abnormal TSH and not thyroxine or thyroid imaging to make a diagnosis of presumed primary hypothyroidism.
The rationale of using VLBW rather than prematurity, a TSH specifically ≥10 mIU/L rather than other cutoffs, and the specific times for all the screenings were based on interpretation of the available data at the time [
2,
3,
4,
5,
6,
14,
15,
16,
18]. Thyroid imaging and urinary iodine testing were rarely clinically performed, so are not part of the analysis.
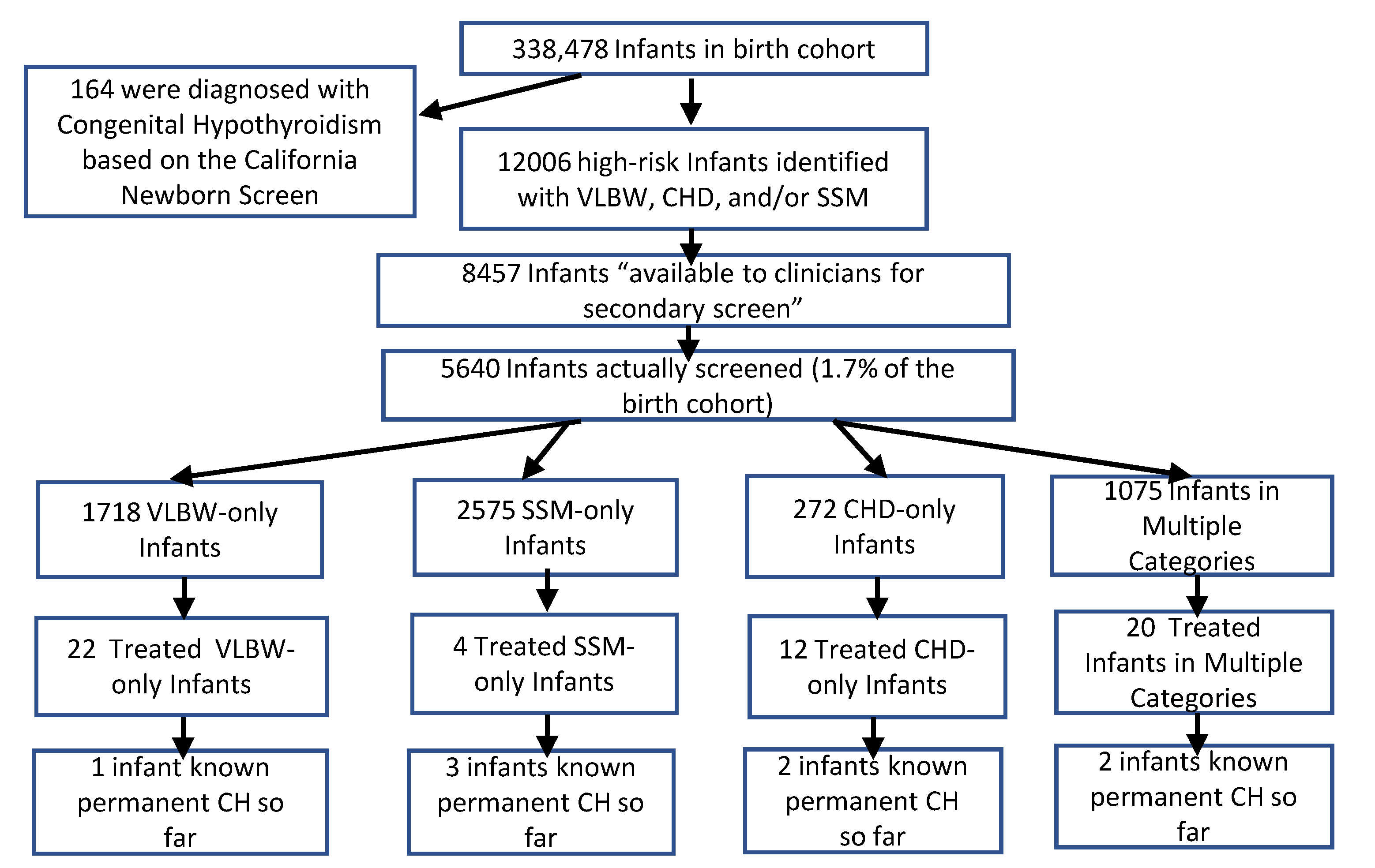
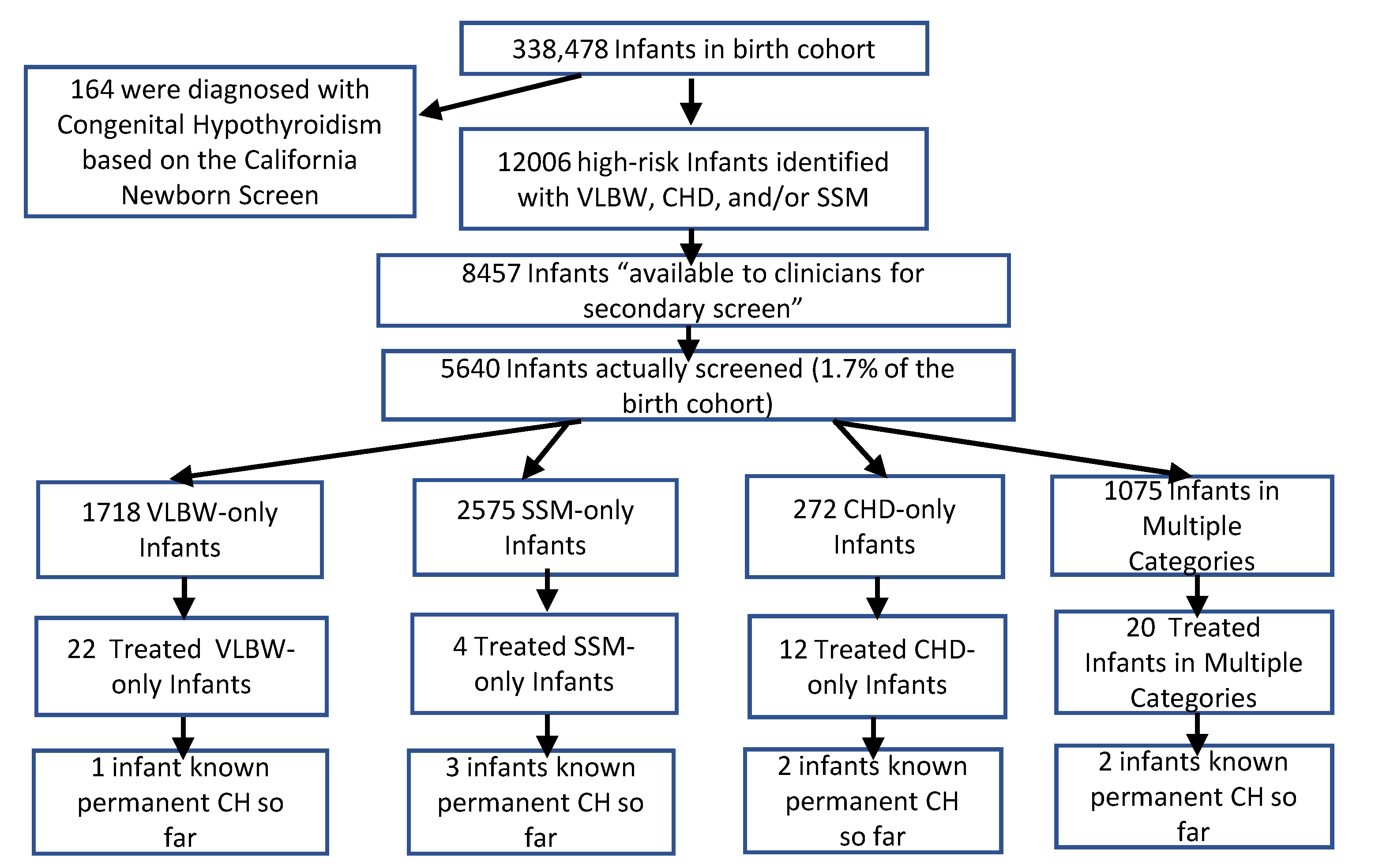
We searched electronic medical record data between 2010 and 2018 for all births and TSH measurements in high-risk infants in the first 60 days of life. International Classification of Diseases-9 and -10 diagnosis codes identified CH, all forms of congenital heart disease (excluding persistent remnants of fetal circulation), multiple gestation, and DS. We also sought evidence of active Kaiser insurance (and hospital admission for CHD and VLBW) at screening times (“available for secondary screening”). For VLBW, the first screen was expected at approximately day 14 of life (days 7–21), the second screen around day of life 28 (days 22–35) and the third screen around day of life 42 (days 36–60). The data collection for the third screen was extended because borderline results at 6 weeks potentially required an additional test. After finding every infant started on levothyroxine in the first 60 days of life, manual chart reviews confirmed this finding and divided these infants into four groupings:
CH by the California primary screen
CH by the secondary screen per the clinical guidelines
Infants started on levothyroxine who were screened or diagnosed due to incorrect or unanticipated use of the secondary screening guidelines
Infants diagnosed with CH (often central) due to clinical suspicion (not by primary or secondary screens).
Infants were further categorized as to their demographic and laboratory information, combinations of high-risk categories, which screening in VLBW infants led to levothyroxine treatment, and presence of DS (a known risk factor for CH) [
15,
16]. We determined whether CH was transient or permanent when sufficient longitudinal data were available. Permanence was defined as TSH ≥ 10 mIU/L after 12 months (whether still on levothyroxine treatment or after discontinuation at 12–36 months leading to TSH ≥ 10 mIU/L) or continued levothyroxine after four years [
2].
Continuous characteristics were summarized with median (IQR) and categorical characteristics were calculated as frequencies/percentages. The chi square test for independence was used to compare the difference in CH prevalence, rates for primary and secondary screening, rates by risk factors and DS diagnosis, frequency of screening, degrees of TSH elevation and permanence of hypothyroidism. Relative risks and 95% confidence intervals were calculated to evaluate differences in CH prevalence for primary and secondary screening rates by risk factors and DS diagnosis. Statistical tests were performed at α = 0.05 level, using two-sided tests.
4. Discussion
This multicenter, retrospective review of a large cohort of demographically diverse infants assigned to a single medical group and health plan provides important insight into the virtue of adopting secondary screening programs for CH, specifically infants who receive a TSH-only newborn screen. Most previous studies observed CH cases in these high-risk groups identified by mandated programs, and many of these authors recommended wide acceptance of secondary screening [
4,
5,
6,
7,
8,
9,
10,
11,
12,
13,
14,
15,
16,
17,
18,
19]. It is not possible to strictly compare studies because of differences in race/ethnicity which affect CH prevalence, different NICU practices that affect TSH levels, iodine sufficiency in a particular region, and variation in protocol for both the primary and secondary screens. Of note, the main study that did not observe missed CH cases [
35] differed from this protocol in looking at only VLBW with one repeat sample at 6 weeks and a TSH cutoff of ≥15 mIU/L. They also did not find differences in developmental outcomes in those with transient elevations compared to matched controls, but their assessments may not have detected subtle changes.
We found VLBW and CHD infants are at high risk of being missed on the primary screen and, despite sub-perfect screening performance, are much more likely to be diagnosed with CH on the secondary screen compared to the primary screen. We did not investigate reasons for the lower screening performance in the SSM and CHD groups but speculate it would improve with better recognition of monochorionic twins (smaller cohort than same-sex) and that milder forms of CHD are a risk factor. We also found missed SSM cases have higher CH prevalence than that expected for singletons presumably due to the higher risk of concurrent VLBW or CHD (76% of SSM cases) and the fact that twins in general share common environmental and genetic factors (especially monozygotic twins) [
19,
36]. Two of the SSM-only cases we identified were in a single twin pairing (not consistent with blood admixture as the cause, suggesting such an environmental or genetic connection and potentially explaining the 3.2-fold higher risk seen in SSM-only infants.
Higher incidence of CH in TSH-only primary screen states, such as California, has been observed compared to those states with a thyroxine/TSH primary screen, though states which couple the thyroxine/TSH primary screen with a universal secondary screen may capture more CH cases [
30]. Our study describes a TSH-only primary screening strategy coupled with a targeted TSH-only secondary screening strategy resulting in the identification of an additional 35% of CH cases, with 27% of those additional cases permanent so far. These results suggest that a targeted secondary screening strategy for <3% of the birth cohort may overcome a shortcoming of TSH-only primary screening- missing CH cases in infants with delayed TSH rise. The strategy (without the use of thyroxine values) was not designed to detect central hypothyroidism cases but clinical suspicion was able to identify cases within our cohort consistent with published expectations of 1:20,000 to 1:50,000 [
20]. We did not address more complex thyroxine/TSH screening strategies to detect rarer genetic forms of central hypothyroidism.
With secondary screening, questions persist regarding the likelihood of permanent CH, predictive value of the TSH result, use of thyroxine results, role of other patient characteristics to clarify high-risk groups better, and ideal time frames for secondary screening. Thyroxine levels were performed on any TSH result > 6 mIU/L by reflex testing through the clinical laboratory, but we found no evidence in manual chart reviews these levels influenced decision-making with TSH > 10 mIU/L screens. We believe our analysis demonstrates that the frequency of positive results justifies continuing the current screening program, though it does not inform us if different high-risk criteria or a different laboratory strategy would be more useful. DS, birth weight ≤1000 g, maternal age > 35 years (data not shown), and extreme prematurity (data not shown) were associated with a higher frequency of these delayed CH cases, but our data do not directly inform us about incorporating this information into a more focused screening strategy. More education to limit misapplication of the screening protocol would likely prevent unnecessary levothyroxine starts (30 infants).
Our data showed, not unexpectedly, that infants can be in multiple high-risk categories. More risk factors increased the frequency of screening SSM and CHD infants. We obtained more accurate information about each category (e.g., CHD) by looking at the infants with only a single risk factor (e.g., CHD only), and comparing that to combinations of risk factors (e.g., CHD/VLBW, CHD/SSM, or CHD/VLBW/SSM). For example, SSM cases showed higher CH prevalence than SSM-only primarily due to its association with VLBW. CH prevalence in CHD combinations was lower compared to CHD-only likely due to CHD-only being low volume but representing a higher percentage of DS, with resultant increased risk of CH from DS as described in Results. VLBW-only prevalence was similar to any VLBW combination likely due to the high prevalence of VLBW in the cohort and the high prevalence of VLBW in the other two risk groups. The subcategories within the VLBW group were also informative, with extremely low birthweight infants (≤1000 g) having a much higher incidence of CH than the larger VLBW infants (1001–1500 g). Among CHD cases, only 2 of 21 had complex cyanotic defects suggesting the need to look broadly at all CHD for screening and not its most severe forms.
In VLBW infants, the relatively even distribution by screening time (2, 4, or 6 weeks) of abnormal TSH levels leading to treatment suggests virtue in multiple secondary screens. This aligns with previous findings suggesting that varied protocols of repeat screening from 1–12 weeks [
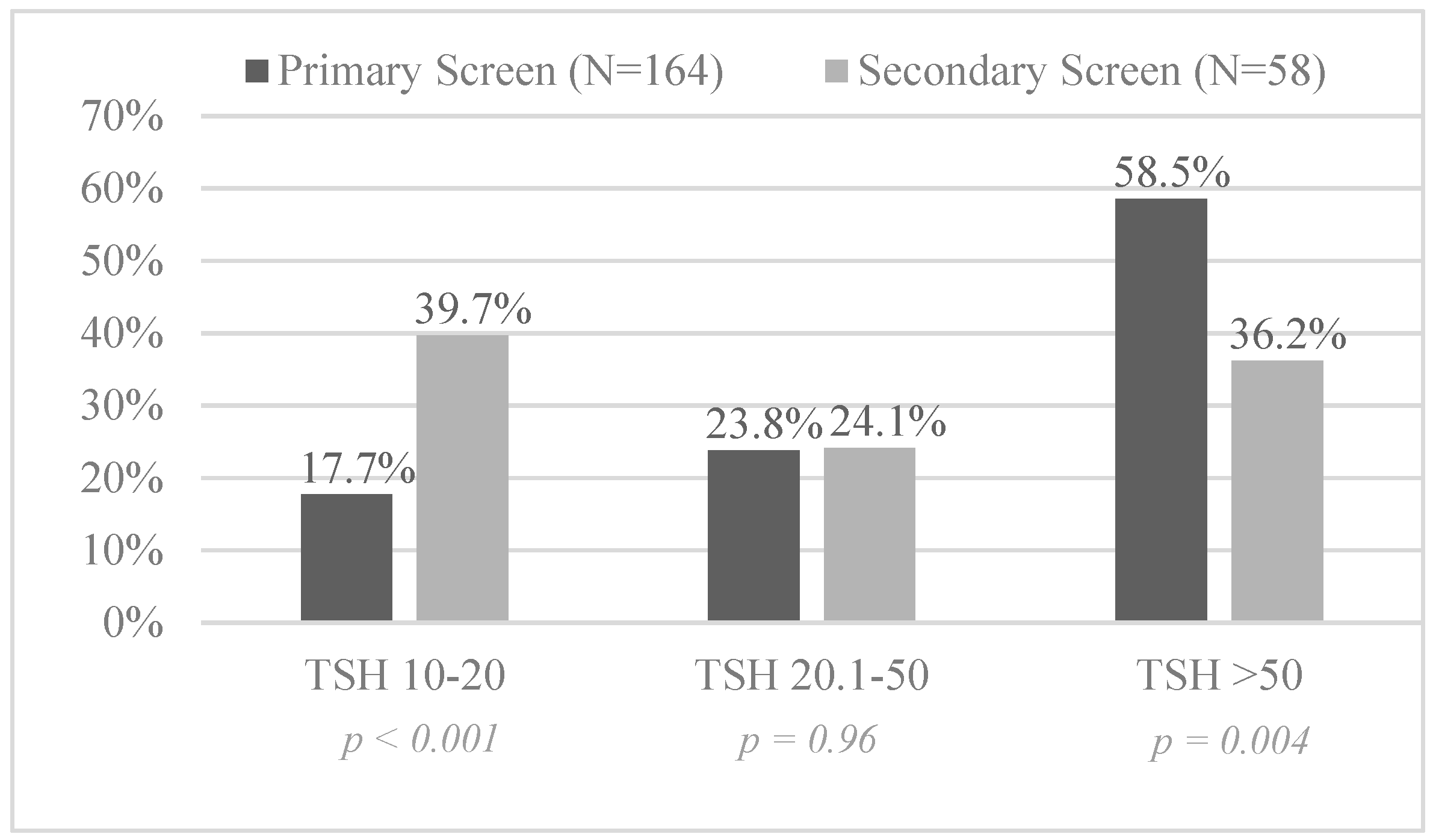
12] all have potential to identify VLBW infants with negative primary screens. Perhaps the varied pathophysiology of VLBW infants with respect to gestational age, associated comorbidities, exposures, and clinical course all lead to variable delays in TSH rise so multiple secondary screens for this select population are needed. With an urgency to identify CH cases as soon as possible, we advocate not waiting more than 2 weeks for the first test given we identified ~1/3 of the cases at 2 weeks. Even children with mild TSH elevations should be treated because the degree of elevation was not predictive of permanence.
Still, most cases detected on the secondary screen represent transient CH or in some cases “non-hypothyroidism.” Exposures to iodine for procedures associated with birth or NICU treatments may elevate TSH [
24,
25]. High TSH seen in the recovery phase of sick euthyroid syndrome following acute illness may be another factor to consider [
3,
26]. Regardless, we cannot anticipate which cases will be transient, how long the hypothyroid state will continue, and what effect the hypothyroid state can permanently have on neurodevelopment [
34,
37]. Therefore, the relatively high rate of transient CH in our opinion is not a valid argument for deferring secondary screening or delaying treatment when CH is detected.
The clinical protocol did not seek DS for secondary screening, yet one quarter of the DS population met the criteria for testing and half were tested. We observed a notably high prevalence of CH in DS (8.3%) on the secondary screen beyond the known prevalence on primary screens [
15,
38]. Without testing all DS infants, we could not determine the relative contribution of DS, CHD, or endocardial cushion defect (with 8 CH cases in DS with CHD). Currently, national screening guidelines in DS recommend evaluation for acquired hypothyroidism starting at 6 months of age [
39] and recognize somewhat higher TSH in younger DS infants [
17]. Our findings, in conjunction with Purdy et al. [
16] suggest screening much sooner due to delayed rise in TSH may have superior value, and van Trotsensburg, et al. [
40] show that even with mild TSH elevations, treatment may preserve intellectual development to the extent possible.
Limitations
Our analysis is limited by its retrospective design and by clinical work performed by hundreds of providers in many hospitals and offices over a wide geographic area. While there were over 300,000 infants studied, the population treated with levothyroxine in the first 60 days was relatively small (248) limiting our power to interpret results. For example, we lacked the power to perform sub-analyses on some specific individual or combined demographic and clinical variables that may have been of interest (e.g., determining if maternal age or gestational age were independent risk factors or just associated with the high-risk groups). For CHD, we limited our analysis to infants in the NICU with CHD (matching the clinical protocol), so we cannot comment on the risk for all infants with CHD. We also cannot determine if gestational age could have been a superior criterion compared to birth weight but we do believe that with advances in EMR and prenatal care, monochorionic status would be superior criteria to the same-sex designation used here. Lastly, we can only speculate that the population of high-risk infants who were not screened would yield similar results to those screened.






{kind=link}
{kind=link}
{kind=link}