
Delivering Positive Newborn Screening Results: Cost Analysis of Existing Practice versus Innovative, Co-Designed Strategies from the ReSPoND Study

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Identifying the Relevant Resources
2.2. Measuring Resource Use
2.3. Valuing Costs per Pathway and National Costs
2.4. Sensitivity Analysis
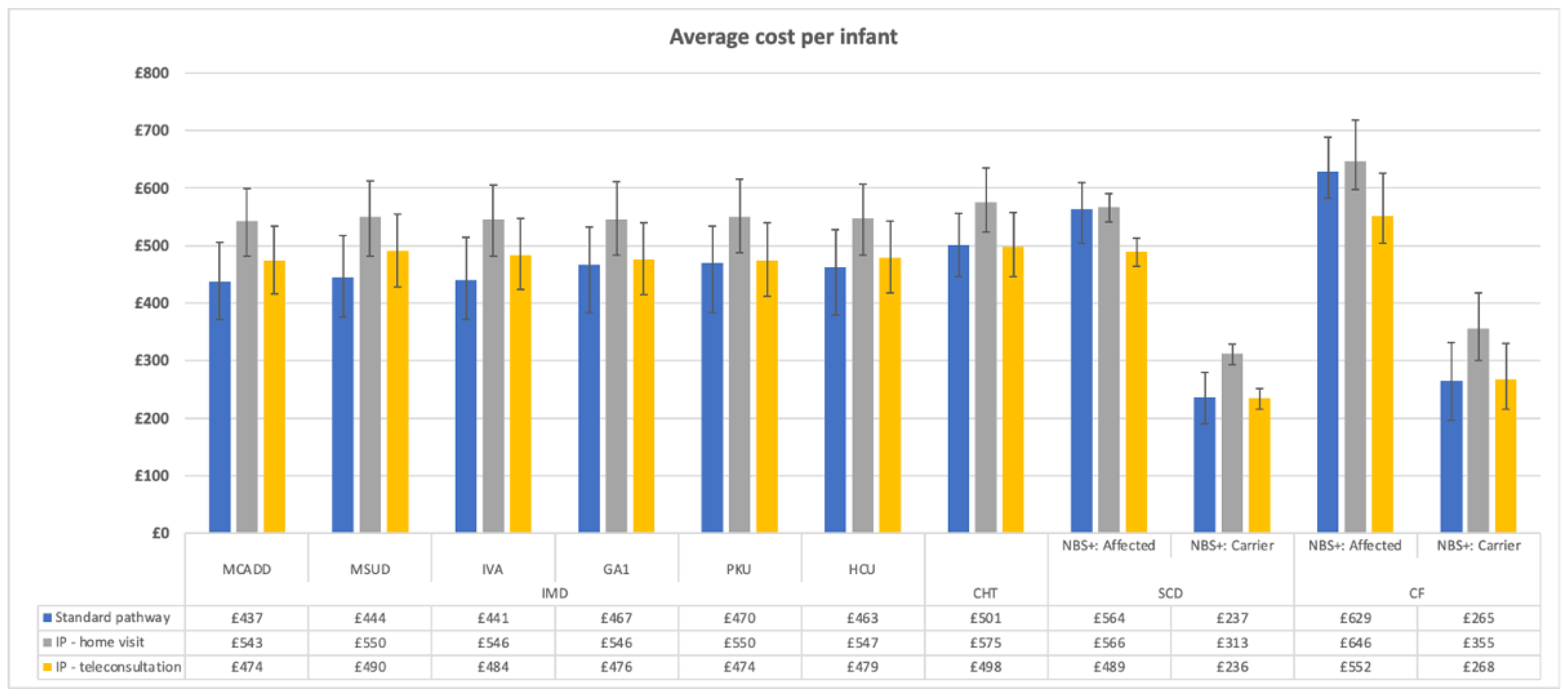
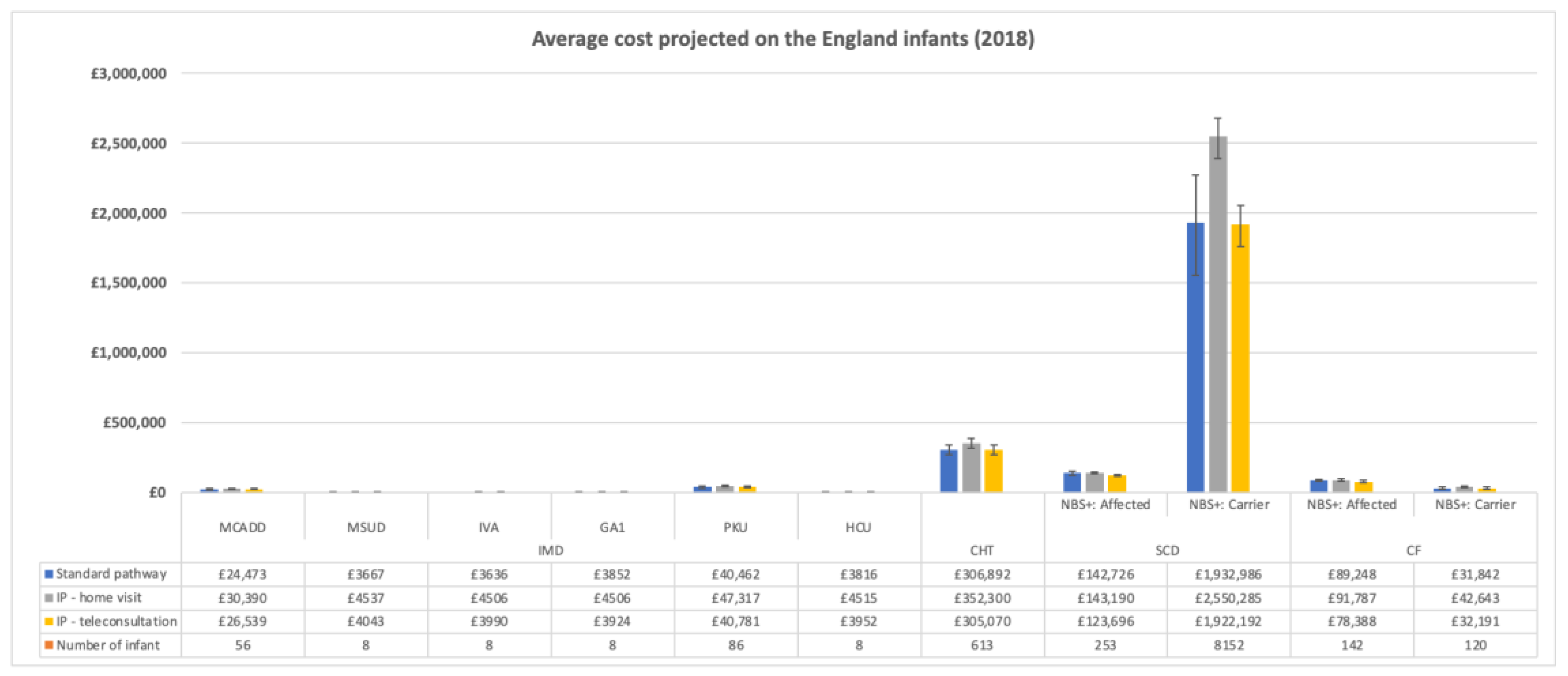
3. Results
Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Public Health England. Newborn Blood Spot Screening Programme in the UK: Data Collection and Performance Analysis Report 1 April 2018 to 31 March 2019; Public Health England: London, UK, 2021.
- Public Health England. NHS Sickle Cell and Thalassaemia Screening Programme Data Report 2017 to 2018; Public Health England: London, UK, 2020.
- Ulph, F.; Cullinan, T.; Qureshi, N.; Kai, J. Parents’ responses to receiving sickle cell or cystic fibrosis carrier results for their child following newborn screening. Eur. J. Hum. Genet. 2014, 23, 459–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulph, F.; Cullinan, T.; Qureshi, N.; Kai, J. The impact on parents of receiving a carrier result for sickle cell or cystic fibrosis for their child via newborn screening. Eur. J. Hum. Genet. 2014, 22, 459–465. [Google Scholar]
- Chudleigh, J.; Buckingham, S.; Dignan, J.; O’Driscoll, S.; Johnson, K.; Rees, D.; Wyatt, H.; Metcalfe, A. Parents’ Experiences of Receiving the Initial Positive Newborn Screening (NBS) Result for Cystic Fibrosis and Sickle Cell Disease. J. Genet. Couns. 2016, 25, 1215–1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salm, A.; Yetter, E.; Tluczek, A. Informing parents about positive newborn screening results: Parents’ recommendations. J. Child Health Care 2012, 16, 367–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tluczek, A.; Clark, R.; McKechnie, A.; Brown, R.L. Factors Affecting Parent-Child Relationships One Year After Positive Newborn Screening for Cystic Fibrosis or Congenital Hypothyroidism. J. Dev. Behav. Pediatr. 2015, 36, 24–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UK Newborn Screening Programme Centre. Health Professional Handbook: A Guide to Newborn Blood Spot Screening for Healthcare Professionals; UK Newborn Screening Programme Centre: London, UK, 2012; pp. 1–56.
- Public Health England. Newborn Blood Spot Screening: Programme Handbook; Public Health England: London, UK, 2018.
- Chudleigh, J.; Shakespeare, L.; Holder, P.; Chinnery, H.; Hack, G.; Gill, T.; Gould, R.; Southern, K.W.; Olander, E.K.; Morris, S.; et al. Communicating newborn screening results to parents: Use of online co-design. 2021; in press. [Google Scholar]
- Chudleigh, J.; Holder, P.; Moody, L.; Simpson, A.; Southern, K.; Morris, S.; Fusco, F.; Ulph, F.; Bryon, M.; Bonham, J.R.; et al. Process evaluation of co-designed interventions to improve communication of positive newborn bloodspot screening results. BMJ Open 2021, 11, e050773. [Google Scholar] [CrossRef] [PubMed]
- Chudleigh, J.; Chinnery, H.; Holder, P.; Carling, R.S.; Southern, K.; Olander, E.; Moody, L.; Morris, S.; Ulph, F.; Bryon, M.; et al. Processing of positive newborn screening results: A qualitative exploration of current practice in England. BMJ Open 2020, 10, e044755. [Google Scholar] [CrossRef]
- Chudleigh, J.; Bonham, J.; Bryon, M.; Francis, J.; Moody, L.; Morris, S.; Simpson, A.; Ulph, F.; Southern, K. Rethinking Strategies for Positive Newborn Screening Result (NBS+) Delivery (ReSPoND): A process evaluation of co-designing interventions to minimise impact on parental emotional well-being and stress. Pilot Feasibility Stud. 2019, 5, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chudleigh, J.; Chinnery, H.; Bonham, J.R.; Olander, E.; Moody, L.; Simpson, A.; Morris, S.; Ulph, F.; Bryon, M.; Southern, K. Qualitative exploration of health professionals’ experiences of communicating positive newborn bloodspot screening results for nine conditions in England. BMJ Open 2020, 10, e037081. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. Newborn Blood Spot Screening Programme in the UK Data collection and Performance Analysis Report 1 April 2017 to 31 March 2018; Public Health England: London, UK, 2020; pp. 1–59.
- Drummond, M.F.; Sculpher, M.J.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programmes; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Personal Social Services Research Unit. Unit Costs of Health and Social Care 2019; University of Kent: Canterbury, UK, 2019. [Google Scholar]
- Chudleigh, J.; Ren, C.; Barben, J.; Southern, K. International approaches for delivery of positive newborn bloodspot screening results for CF. J. Cyst. Fibros. 2019, 18, 614–621. [Google Scholar] [CrossRef] [Green Version]
- Parker, H.; Qureshi, N.; Ulph, F.; Kai, J. Imparting carrier status results detected by universal newborn screening for sickle cell and cystic fibrosis in England: A qualitative study of current practice and policy challenges. BMC Health Serv. Res. 2007, 7, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchbinder, M.; Timmermans, S. Newborn screening for metabolic disorders: Parental perceptions of the initial communication of results. Clin. Pediatr. 2012, 51, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Rueegg, C.S.; Barben, J.; Hafen, G.M.; Moeller, A.; Jurca, M.; Fingerhut, R.; Kuehni, C.E. Newborn screening for cystic fibrosis—The parent perspective. J. Cyst. Fibros. 2015, 15, 443–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Time (Minutes) | Cost per Minute | Cost per Contact | Source of Cost per Minute | |
|---|---|---|---|---|
| Clinical nurse specialist | ||||
| home-visit + | 88.33 | £1.18 | £103.87 | PSSRU 2019 [17] |
| surgery/hospital visit | 55 | £1.18 | £64.68 | PSSRU 2019 [17] |
| not face-to-face external interaction | 22.81 | £1.18 | £26.83 | PSSRU 2019 [17] |
| not face-to-face internal interaction | 15 | £1.18 | £17.64 | PSSRU 2019 [17] |
| Health visitor/midwife | ||||
| home-visit + | 88.33 | £1.18 | £103.87 | PSSRU 2019 [17] |
| surgery/hospital visit | 55 | £1.18 | £64.68 | PSSRU 2019 [17] |
| not face-to-face external interaction | 22.81 | £1.18 | £26.83 | PSSRU 2019 [17] |
| not face-to-face internal interaction | 15 | £1.18 | £17.64 | PSSRU 2019 [17] |
| Consumables | ||||
| Leaflet | £2.50 | £2.50 | Assumption | |
| GP | ||||
| home-visit + | 88.33 | £3.65 | £322.82 | PSSRU 2019 [17] |
| surgery/hospital visit | 55 | £3.65 | £201.00 | PSSRU 2019 [17] |
| not face-to-face external interaction | 22.81 | £3.83 | £87.37 | PSSRU 2019 [17] |
| not face-to-face internal interaction | 15 | £2.30 | £34.49 | PSSRU 2019 [17] |
| Consultant (hospital-based) | PSSRU 2019 [17] | |||
| home-visit + | 88.33 | £1.64 | £144.77 | PSSRU 2019 [17] |
| surgery/hospital visit | 55 | £1.64 | £90.14 | PSSRU 2019 [17] |
| not face-to-face external interaction | 22.81 | £1.64 | £37.39 | PSSRU 2019 [17] |
| not face-to-face internal interaction | 15 | £1.64 | £24.58 | PSSRU 2019 [17] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fusco, F.; Chudleigh, J.; Holder, P.; Bonham, J.R.; Southern, K.W.; Simpson, A.; Moody, L.; Olander, E.K.; Chinnery, H.; Morris, S. Delivering Positive Newborn Screening Results: Cost Analysis of Existing Practice versus Innovative, Co-Designed Strategies from the ReSPoND Study. Int. J. Neonatal Screen. 2022, 8, 19. https://doi.org/10.3390/ijns8010019
Fusco F, Chudleigh J, Holder P, Bonham JR, Southern KW, Simpson A, Moody L, Olander EK, Chinnery H, Morris S. Delivering Positive Newborn Screening Results: Cost Analysis of Existing Practice versus Innovative, Co-Designed Strategies from the ReSPoND Study. International Journal of Neonatal Screening. 2022; 8(1):19. https://doi.org/10.3390/ijns8010019
Chicago/Turabian StyleFusco, Francesco, Jane Chudleigh, Pru Holder, James R. Bonham, Kevin W. Southern, Alan Simpson, Louise Moody, Ellinor K. Olander, Holly Chinnery, and Stephen Morris. 2022. "Delivering Positive Newborn Screening Results: Cost Analysis of Existing Practice versus Innovative, Co-Designed Strategies from the ReSPoND Study" International Journal of Neonatal Screening 8, no. 1: 19. https://doi.org/10.3390/ijns8010019
APA StyleFusco, F., Chudleigh, J., Holder, P., Bonham, J. R., Southern, K. W., Simpson, A., Moody, L., Olander, E. K., Chinnery, H., & Morris, S. (2022). Delivering Positive Newborn Screening Results: Cost Analysis of Existing Practice versus Innovative, Co-Designed Strategies from the ReSPoND Study. International Journal of Neonatal Screening, 8(1), 19. https://doi.org/10.3390/ijns8010019