1. Introduction
Whole body PET (WBPET) using the radiotracer FDG is being increasingly utilized in breast cancer diagnosis, staging, and evaluation of treatment response [
1,
2,
3]. Over the past 25 years, interest in the detection of smaller, earlier stage breast cancers has led to the development of a number of dedicated breast PET (dbPET) scanners with improved spatial resolution compared to WBPET. The first dbPET systems used two opposing planar detectors between which the breast was compressed [
4]. The PEM Flex Solo II breast PET scanner, marketed by Naviscan (CMR Naviscan, Carlsbad, CA, USA), uses two opposing rectangular planar detectors that are scanned in synchrony in the left–right direction above and below the compressed breast [
5]. Its in-plane spatial resolution of ~2.4 mm has been shown to lead to increased sensitivity for detection of small lesions [
6,
7]. However, the limited angular span of the lines of response (LORs) available with the static opposing planar detector geometry result in tomosynthesis-like limited angle acquisition and therefore poorer spatial resolution in the direction normal to the detector surfaces [
5].
For more isotropic spatial resolution, dbPET/CT systems have been developed that use one or more pairs of opposing planar detectors on a rotation stage for step-and-shoot image acquisition over 180° [
8,
9]. Shimadzu (Kyoto, Japan) developed semi-prone full ring (O-PET) and partial ring (C-PET) systems, both designed to provide nearly isotropic spatial resolution while improving photon sensitivity [
10,
11]. Two prone, full-ring commercial systems have recently become available; the MAMMI system from Oncovision (Valencia, Spain) [
12] and the Elmammo system from Shimadzu [
13,
14].
Human studies of dbPET systems have found that visualization of posterior breast tissue is often poor because unlike WBPET, the dbPET geometry places the posterior breast at the boundary of the volume of view (VoV), where the probability of coincident events, and thus photon sensitivity, approaches zero. The problem can be further exacerbated in prone imaging systems due to the thickness of the table, which has the effect of pushing the posterior breast region further out of the VoV. While each of the above dbPET systems, with spatial resolutions ranging from 1 to 2.5 mm FWHM [
8,
10,
12,
13], successfully improved the resolution compared to WBPET systems, only the C-shaped Shimadzu system was specifically designed with the goal of improving visualization of posterior breast tissue [
10].
In an attempt to improve the visualization of the posterior breast tissue compared to previous dbPET scanners, the breast ring PET (BRPET) system was developed and tested in a collaborative effort among the University of Virginia, West Virginia University, and the Jefferson Lab (Newport News, VA, USA). The BRPET dbPET scanner comprises a single 12-module PET ring mounted below a Lorad prone biopsy table.
The following sections present the characterization of the BRPET imaging performance, as well as the results of a pilot human study comparing BRPET to contrast-enhanced MRI (CEMRI).
4. Discussion
The BRPET system was designed with a primary goal of improving visualization of posterior breast tissue compared to other systems for dbPET, while maintaining the spatial resolution and system sensitivity of comparable single ring systems [
12,
13]. The results reported here indicate that in terms of the posterior limit of the VoV and spatial resolution these goals were reached.
The measured spatial resolution of BRPET is comparable to that of other dbPET systems [
12,
13,
24] (
Table 6), and like that of the other dedicated systems, is superior to that of WBPET (FWHM transaxial and axial resolutions 1 cm from isocenter of 4.3–5.8 mm and 4.1–4.2 mm, respectively) [
25].
Figure 4 shows that the full ring geometry of BRPET also enables nearly isotropic spatial resolution near the center of the VoV. This is unlike limited angle dbPET systems for which the resolution in one of the three dimensions is much poorer than in the other two. For planes midway between the ring’s central and peripheral planes the BRPET tangential resolution is somewhat degraded towards the VoV periphery, while the axial and radial resolutions remain nearly constant.
The highest photon sensitivity in any PET system is at the center of the VoV, where the number of geometrically possible lines of response is greatest. As anticipated, the BRPET sensitivity falls approximately linearly as a function of the axial distance from the ring’s central plane. The peak sensitivity is lower than that reported for the MAMMI system (0.97 and 1.8% peak for BRPET and MAMMI, respectively), while the total system sensitivity is comparable (19.3 and 20%, respectively) [
12].
The results of the VoV experiments showed that under high contrast conditions (e.g., high lesion uptake and/or high LBR) the BRPET system is capable of imaging tissue up to within ~6 mm of the top surface of the table’s breast aperture. However, as shown in
Figure 6, detection of small or low uptake lesions presents a more difficult imaging challenge in terms of SNR. The lesions used in the breast phantom study were intentionally chosen to have very low LBR (~2 to 3) compared to what would be encountered clinically (~17 for ductal cancer and ~6 for lobular cancer) [
22]. Since the numerator of the lesion SNR varies approximately proportionally with the LBR,
Figure 6 suggests that at a depth of 10 mm even the smallest (0.8 mm diameter) lesion tested would, with an LBR of 6.5, have an SNR of approximately 6.2, making it readily visible.
To our knowledge, neither high contrast nor SNR-based analysis of the posterior extent of the usable VoV of other dbPET scanners is available in the literature, making direct comparison difficult. In a study of 230 subjects undergoing both whole body PET (WBPET) and MAMMI, with WBPET findings used as ground truth, the MAMMI system had a lesion detection sensitivity of 88.9%. However, when tumors outside the scanner’s VoV near the chest wall were excluded from the analysis, the sensitivity increased to 98.6% [
26]. A more recent study of MAMMI also concluded that lack of visualization of posterior breast tissue degraded BIRADS-4 lesion sensitivity [
27]. Investigators at the Mayo Clinic reported significant gains in the volume of posterior breast tissue imaged by MAMMI via modification of its standard table to provide a larger breast aperture and thinner table sections [
28].
In a study including 69 subjects, WBPET was compared to both Shimadzu’s full-ring O scanner and to their C-shaped scanner. The overall lesion sensitivities of the O and C scanners were 82 and 83%, respectively. However, excluding lesions outside of their VoVs their sensitivities increased to 93 and 90%, respectively [
11]. The authors of this study noted that all tumors outside of the field of view were located close to the chest wall in the posterior breast tissue [
11].
It should be noted that the conical recess of the prone table breast aperture produces a natural convex flexing downward of the chest wall region, with the result that some posterior breast tissue extends lower than the plane defined by the edges of the breast aperture.
Participants in the pilot human study comparing BRPET to CEMRI were primarily women with recently diagnosed breast cancer (
n = 8) and high-risk women undergoing breast cancer screening with CEMRI (
n = 2). Among this cohort, the sensitivity of BRPET was comparable to that of CEMRI while the specificity was ~4-fold higher and the overall accuracy was ~25% higher (see
Table 5). The lower specificity for CEMRI was due to a large number of false positives. These results suggest that BRPET might have a role in reducing the false positive rate of CEMRI without unacceptably increasing the false negative rate.
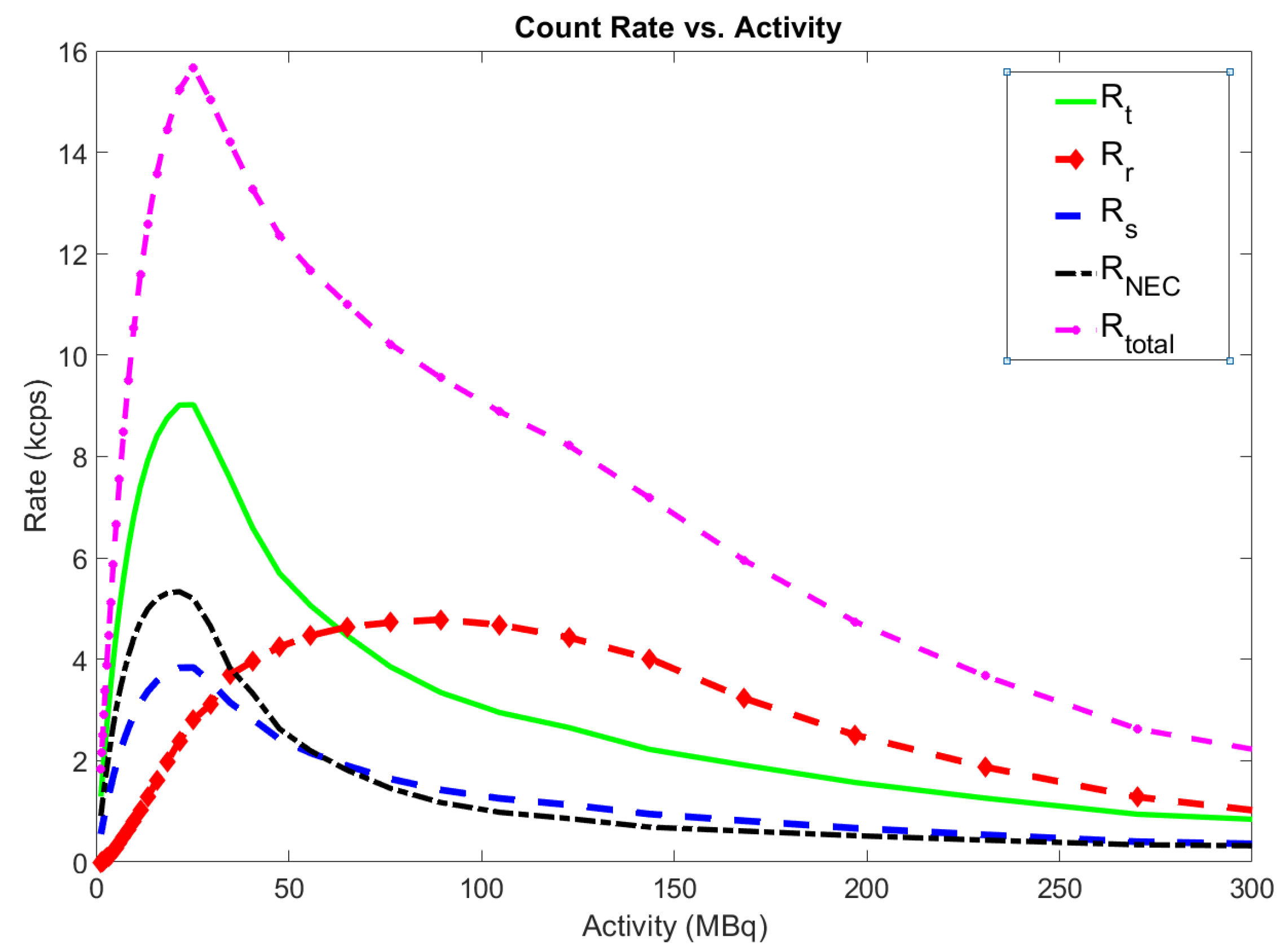
Although the performance of the BRPET scanner was encouraging, there is room for improvement. Most importantly, the NECR of 5.3 kcps at 21 MBq, although adequate for the human study described here, is lower than desirable. It is limited primarily by inefficiencies and overhead in the data acquisition software, which must be replaced in order to increase count rate capability, and thus improve photon sensitivity and image SNR. Also, the addition of a second detector ring could increase the axial FoV sufficiently to permit the majority of breasts to be imaged with only one or two vertical detector positions, thereby decreasing scan time and improving overall scanner sensitivity.


 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}