

CFD Investigation of Ventilation Strategies to Remove Contaminants from a Hospital Room



Abstract
:1. Introduction
2. Methodology
2.1. Governing Equations
2.1.1. Turbulence Model
2.1.2. Contaminant Substance
2.1.3. Removal Effectiveness
- (a)
- Contaminant Removal Efficiency (CRE)
- (b)
- The Local Air Quality Index (LAQI)
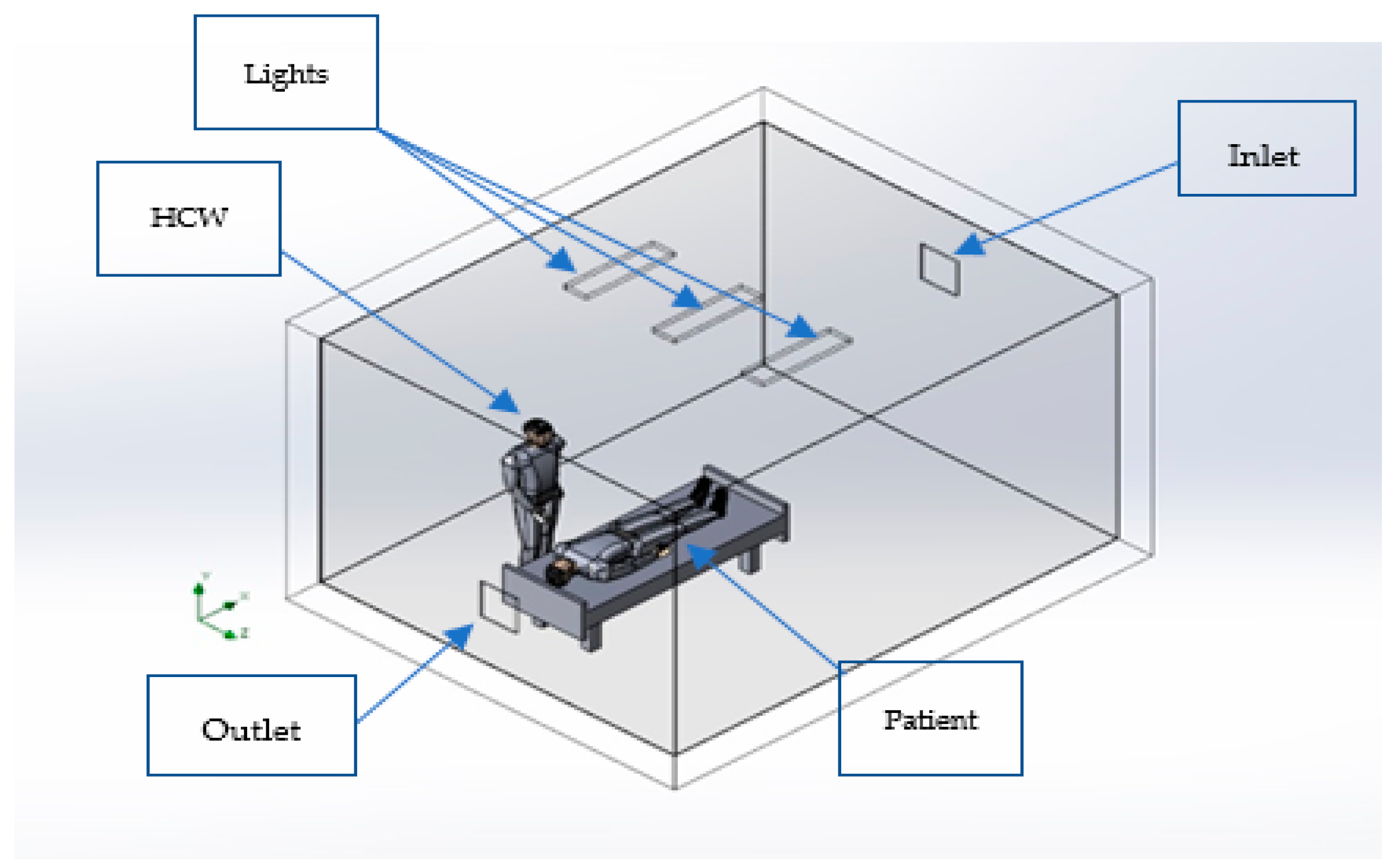
2.2. Model Description
2.3. Boundary Conditions
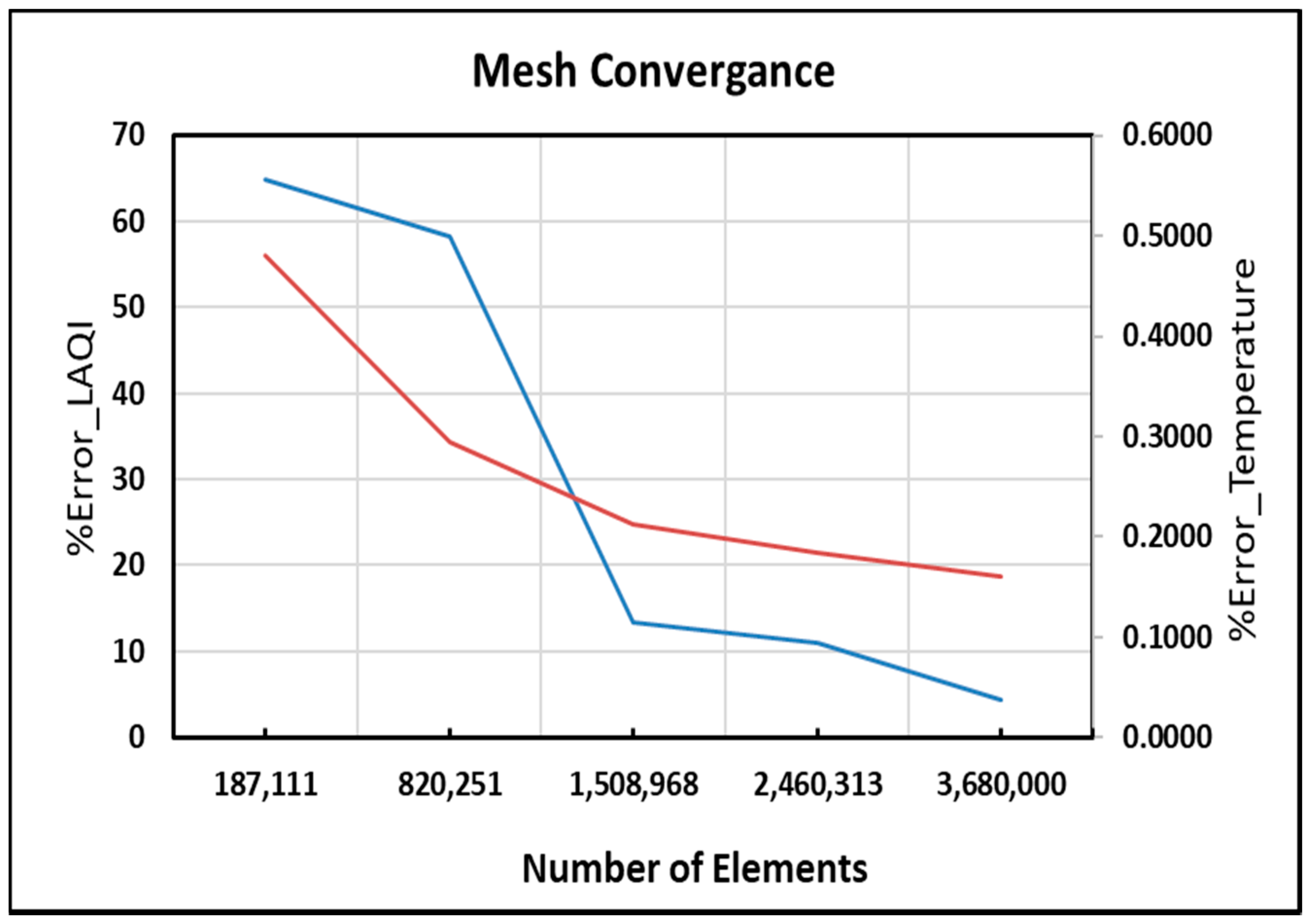
2.4. Mesh Independency Study and Solution Convergence Criteria
3. Results and Discussion
3.1. Cases 1, 2 and 3
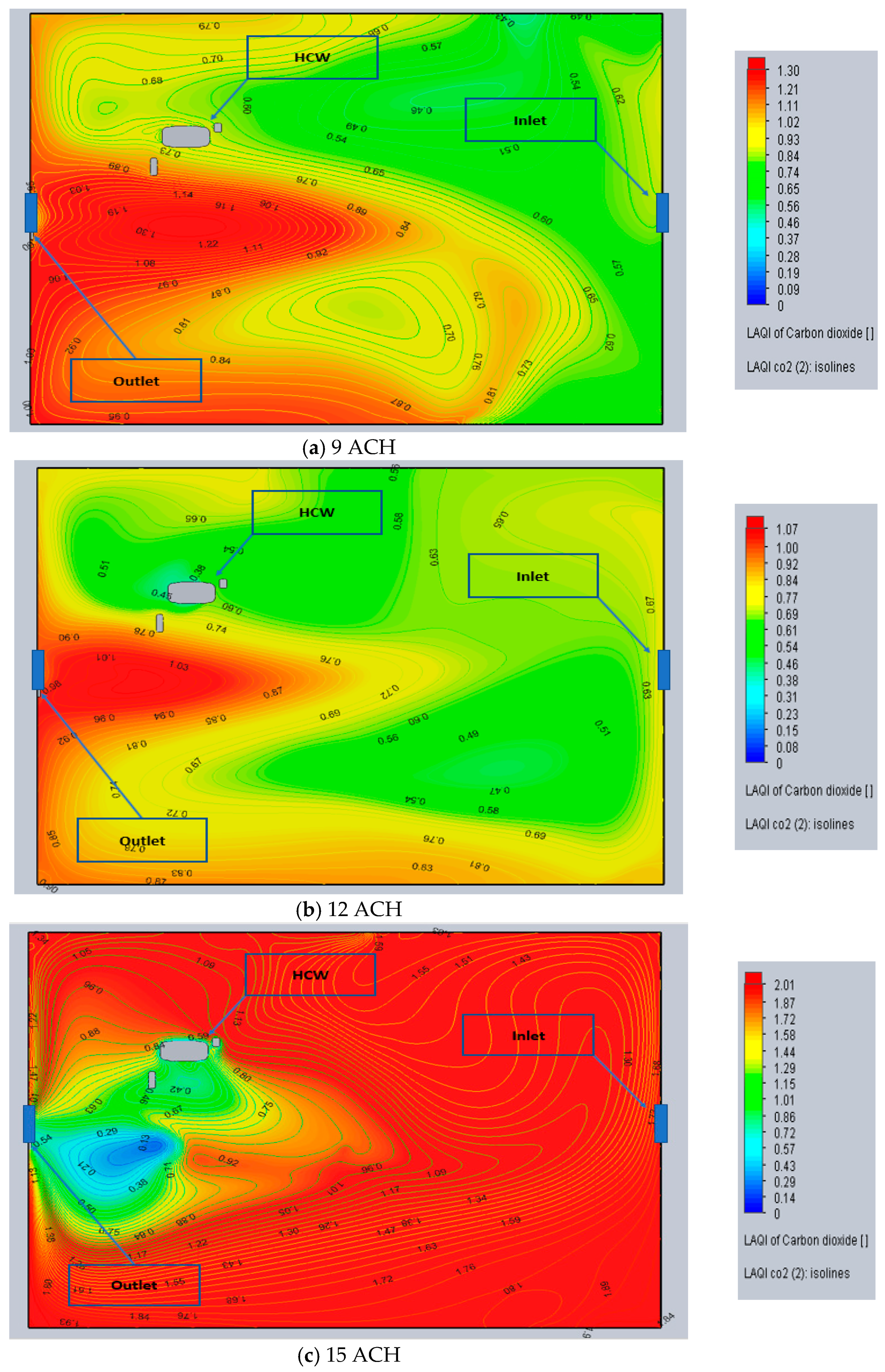
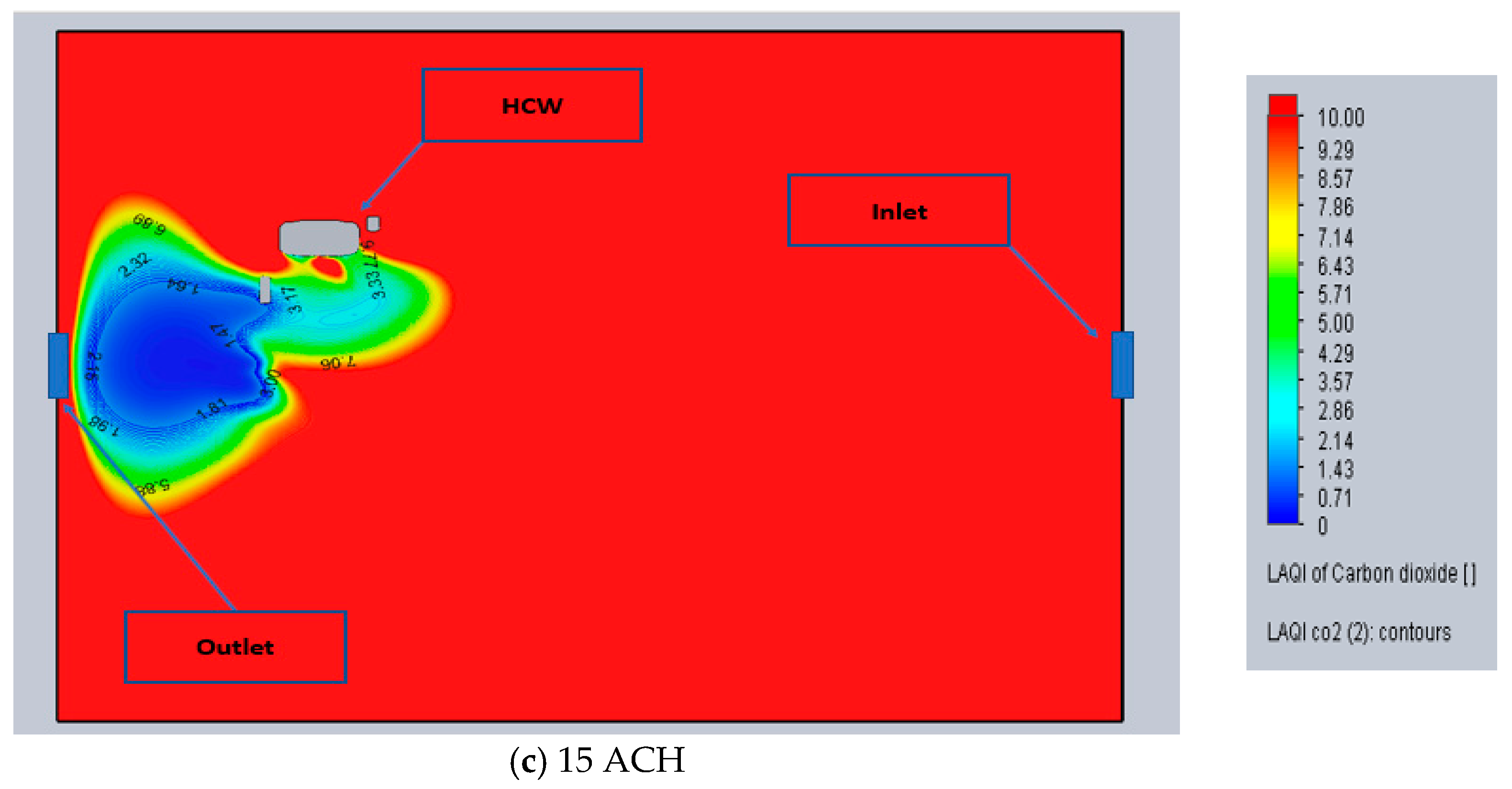
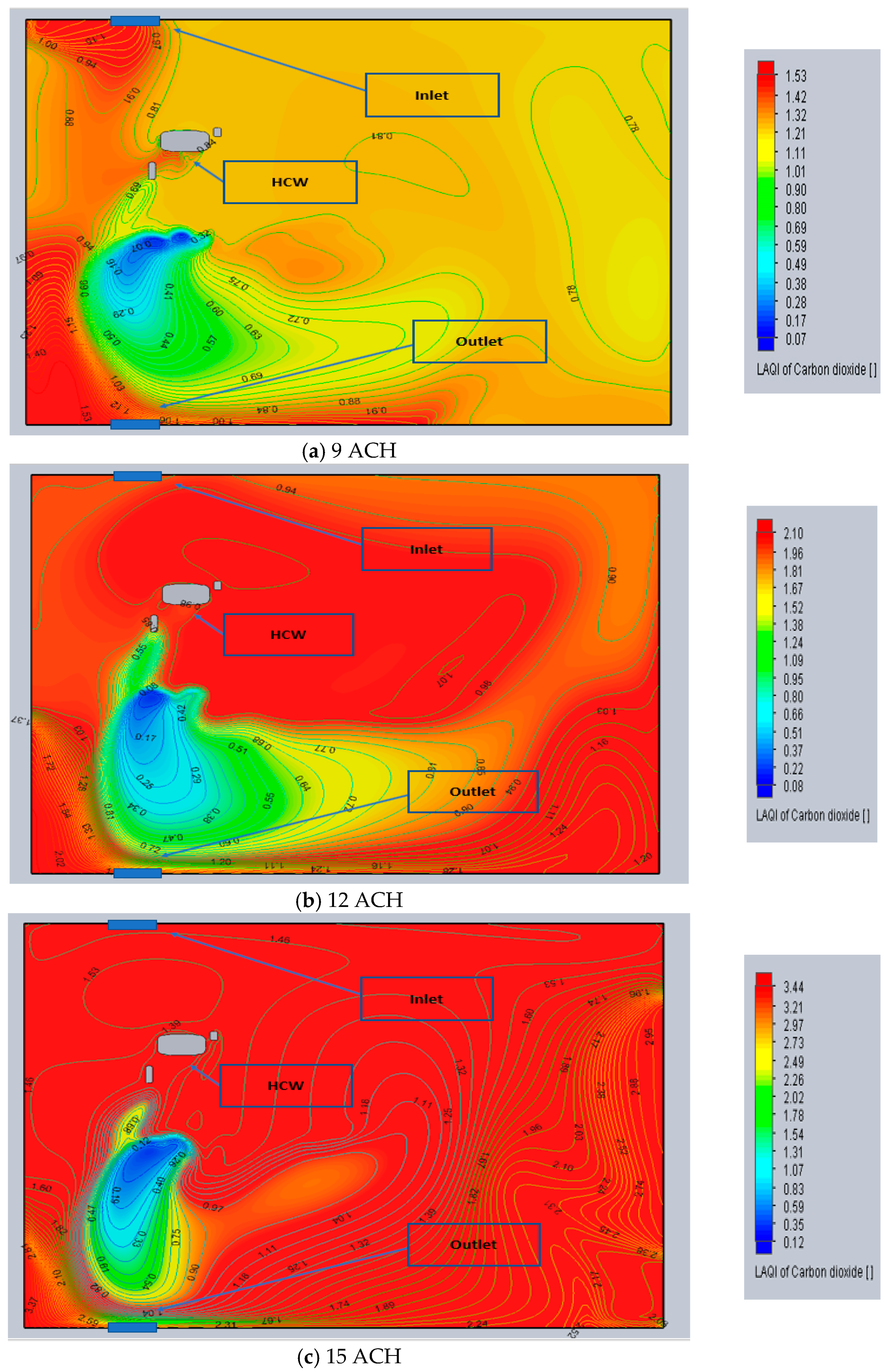
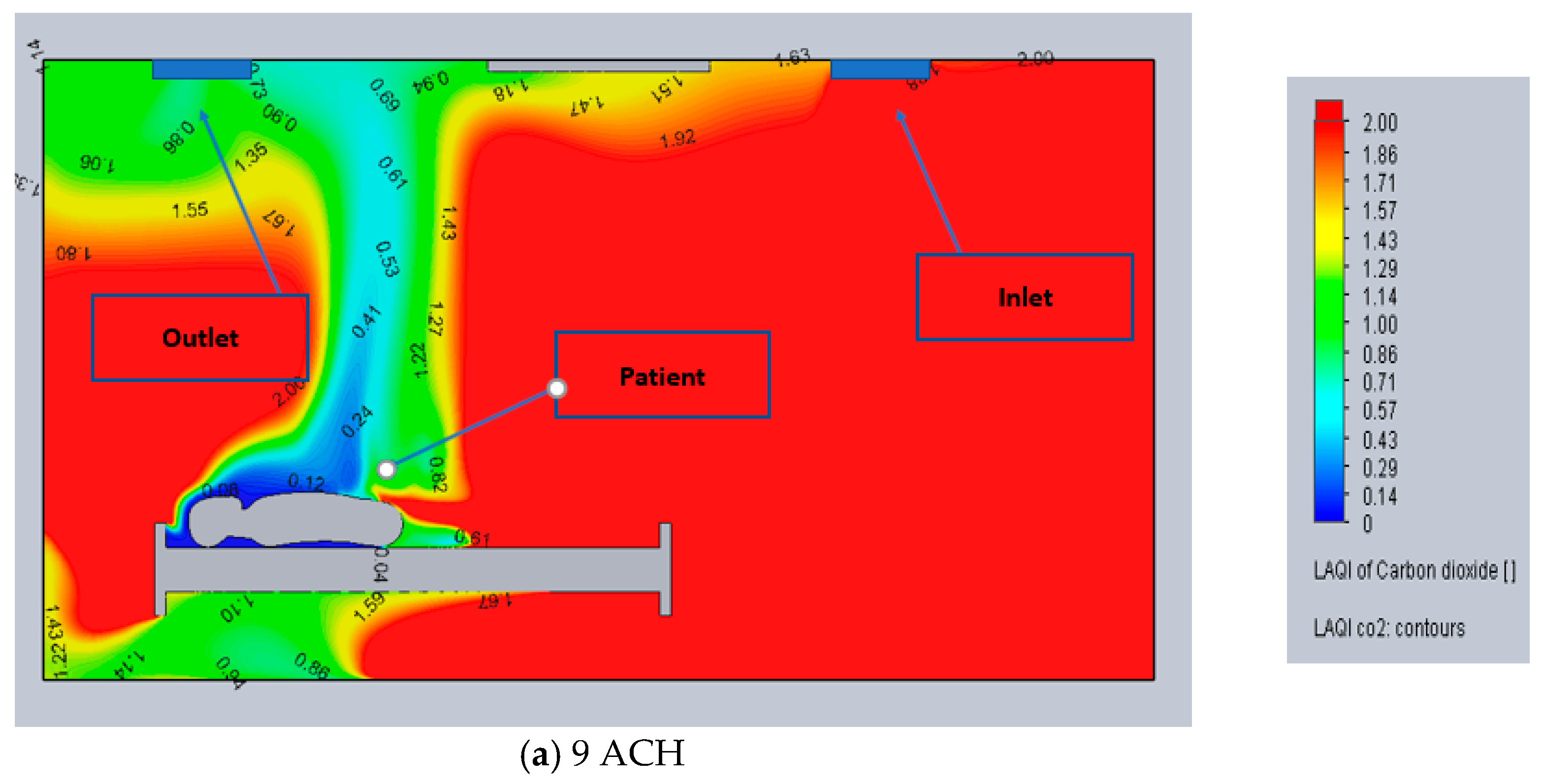
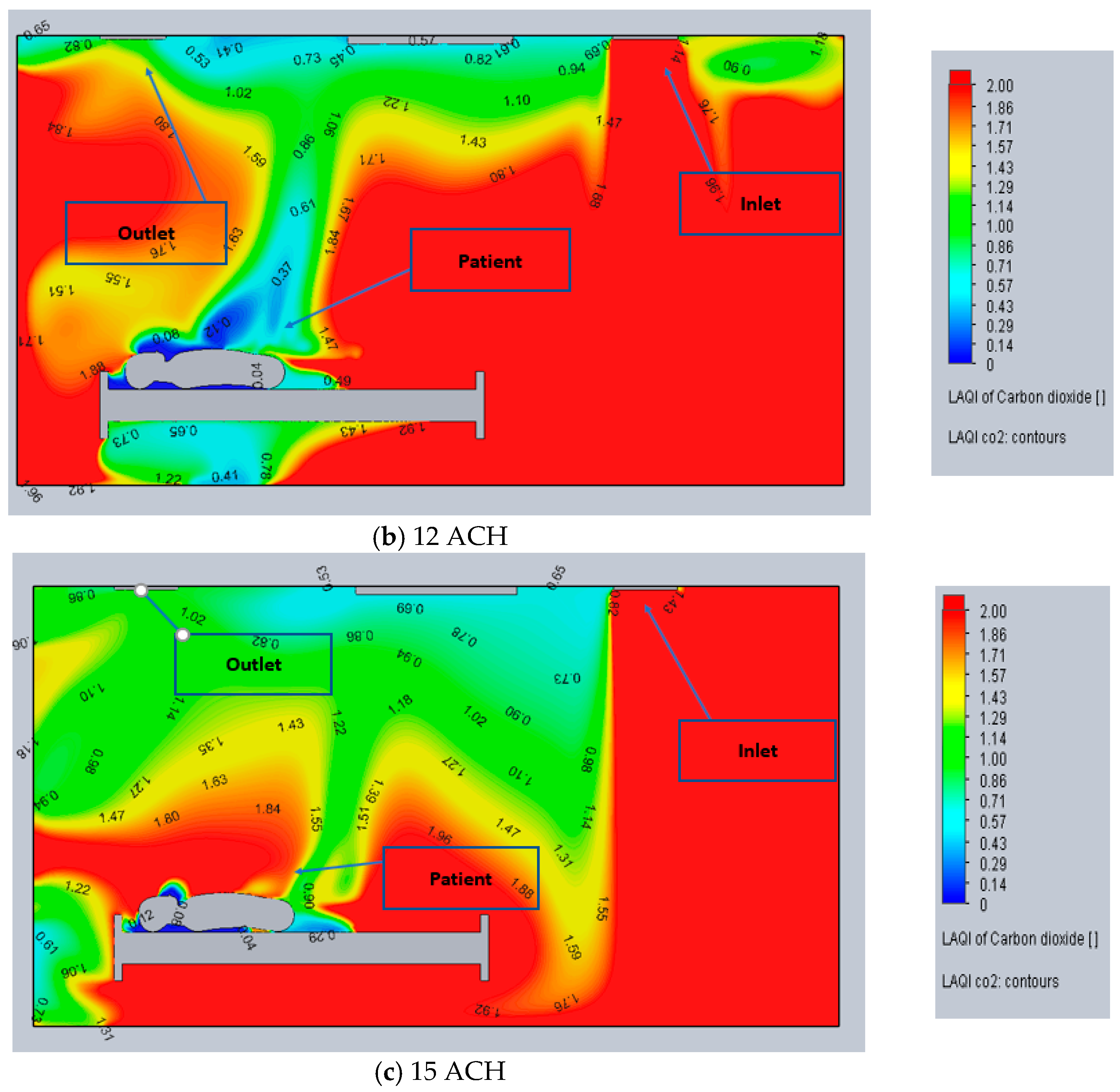
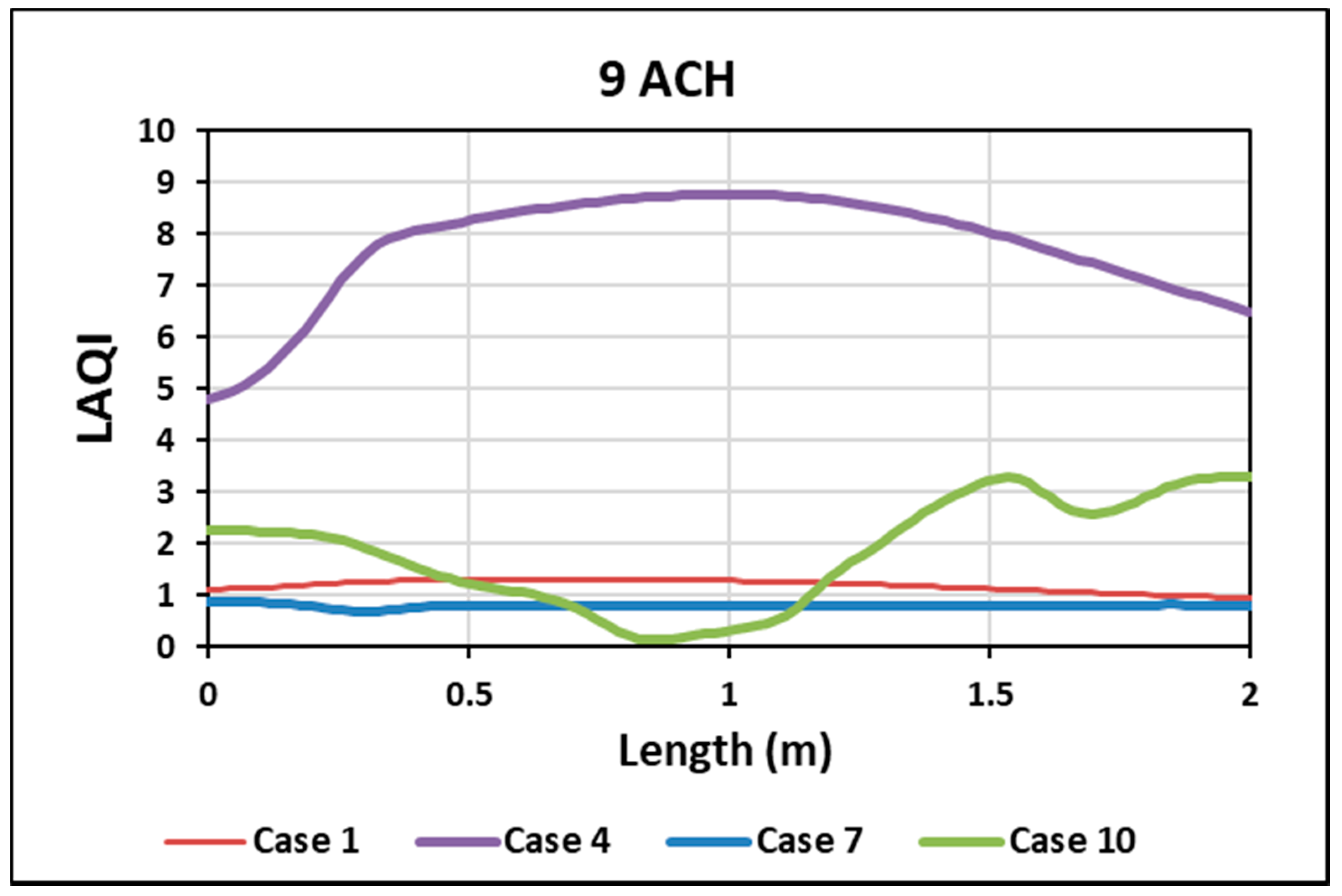
3.1.1. Local Air Quality Index (LAQI)
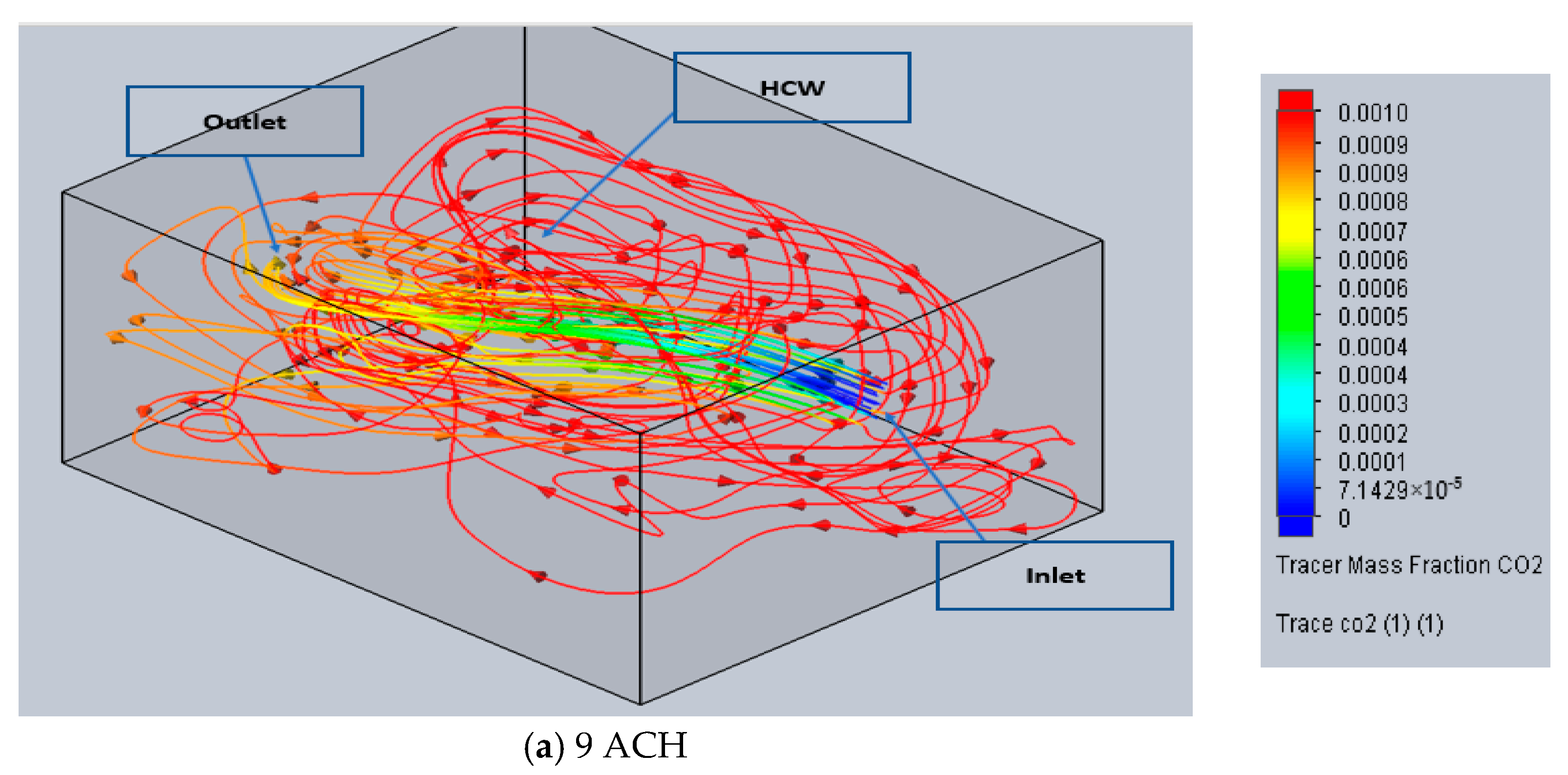
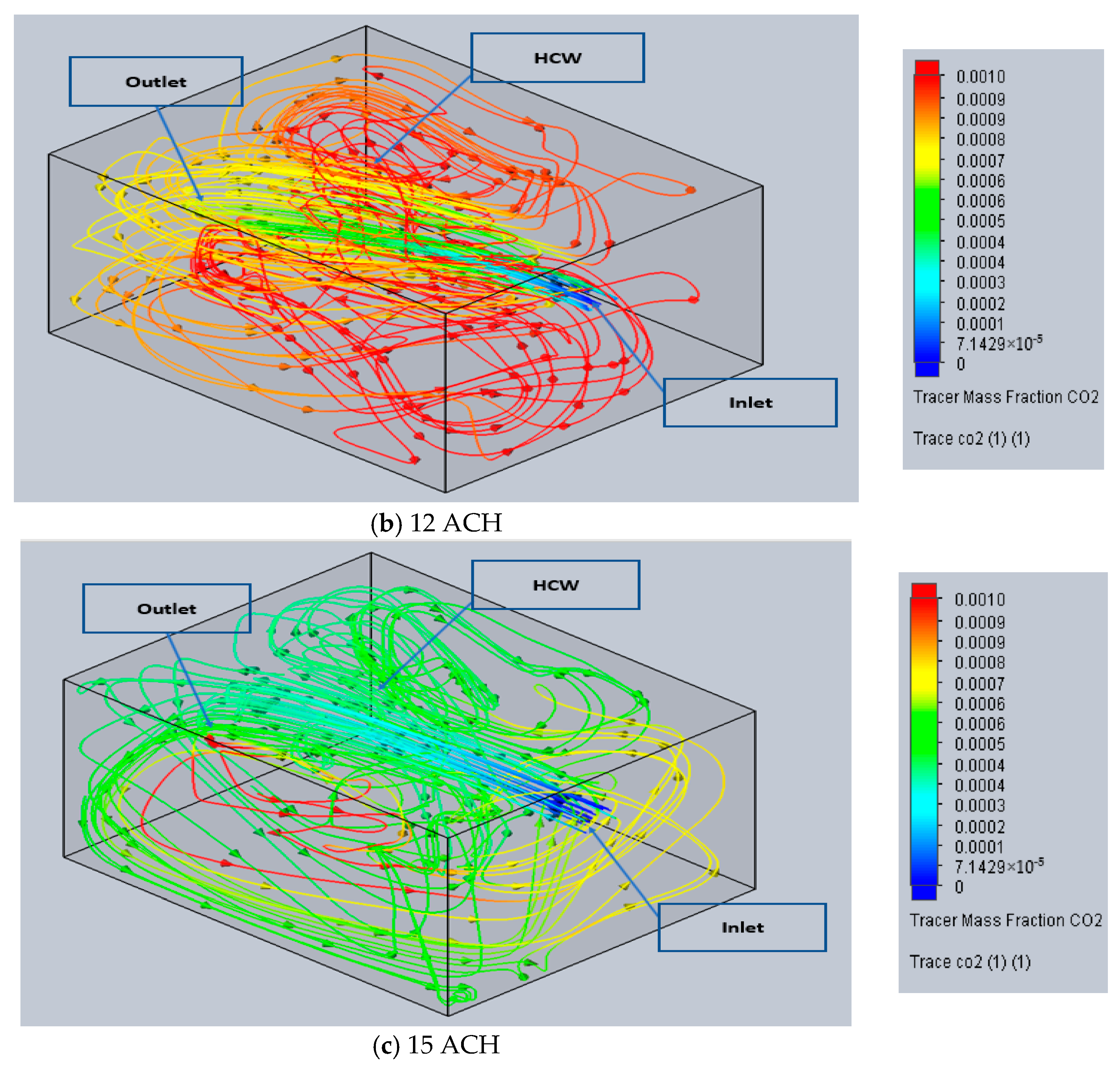
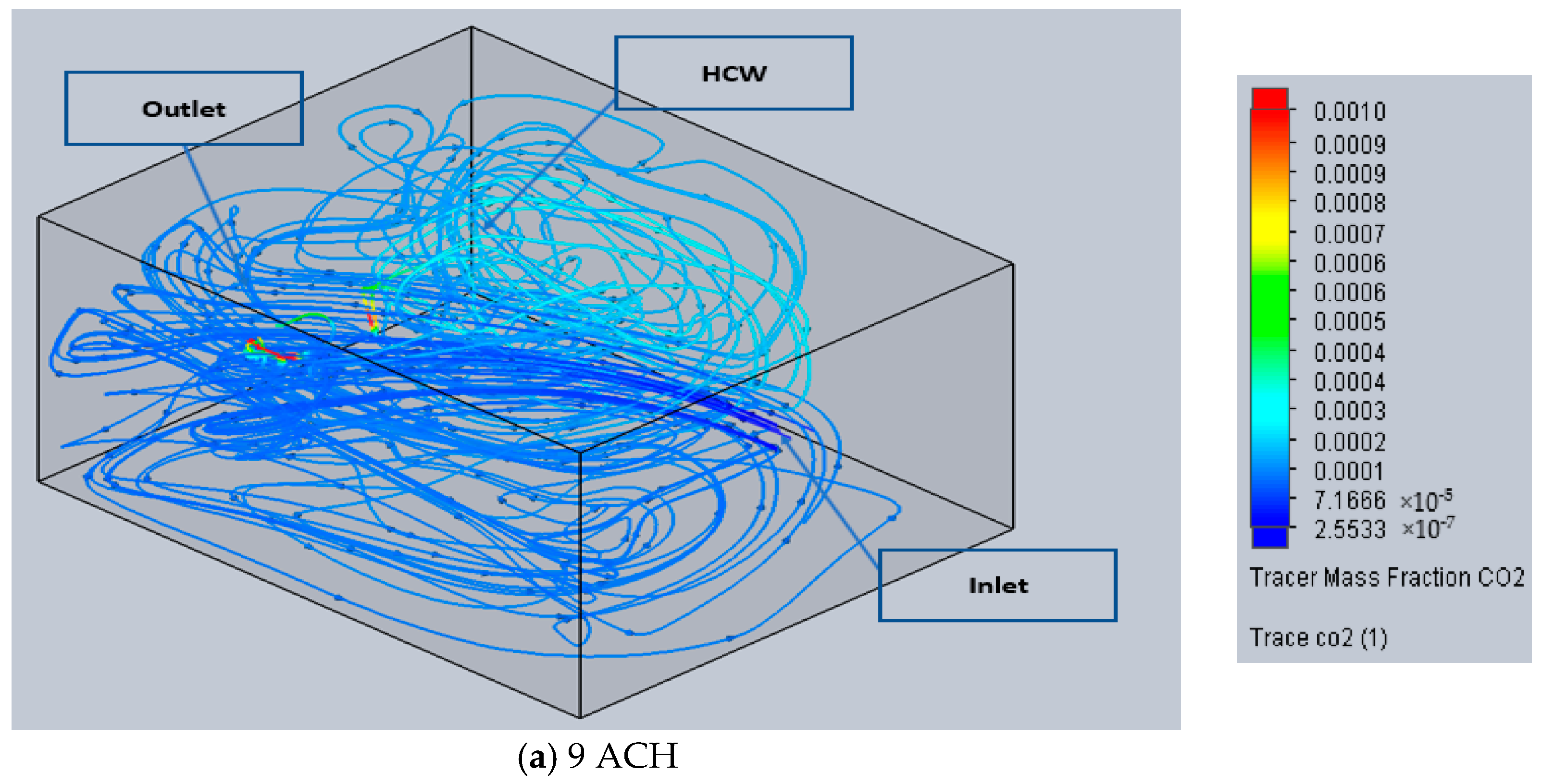
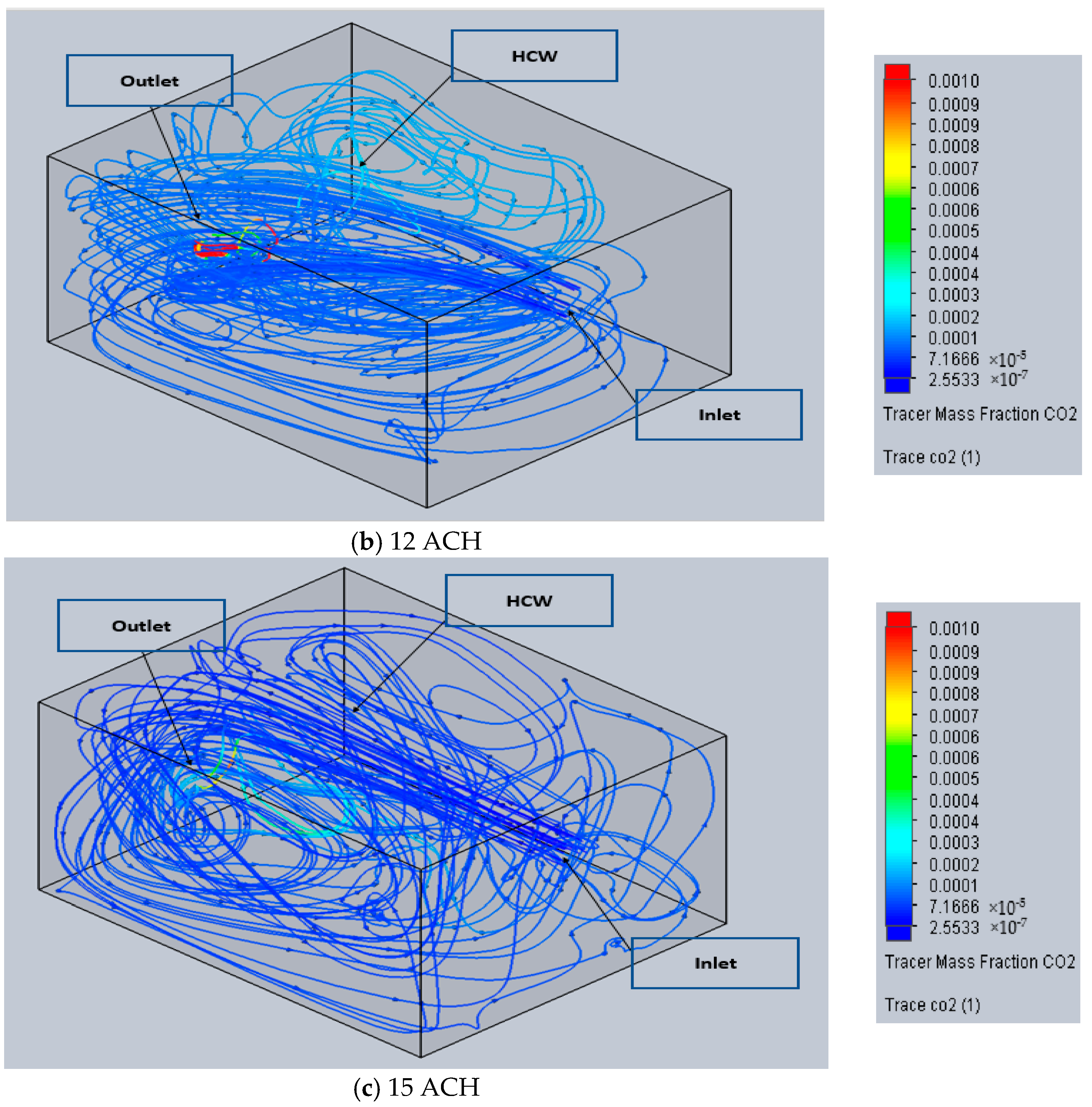
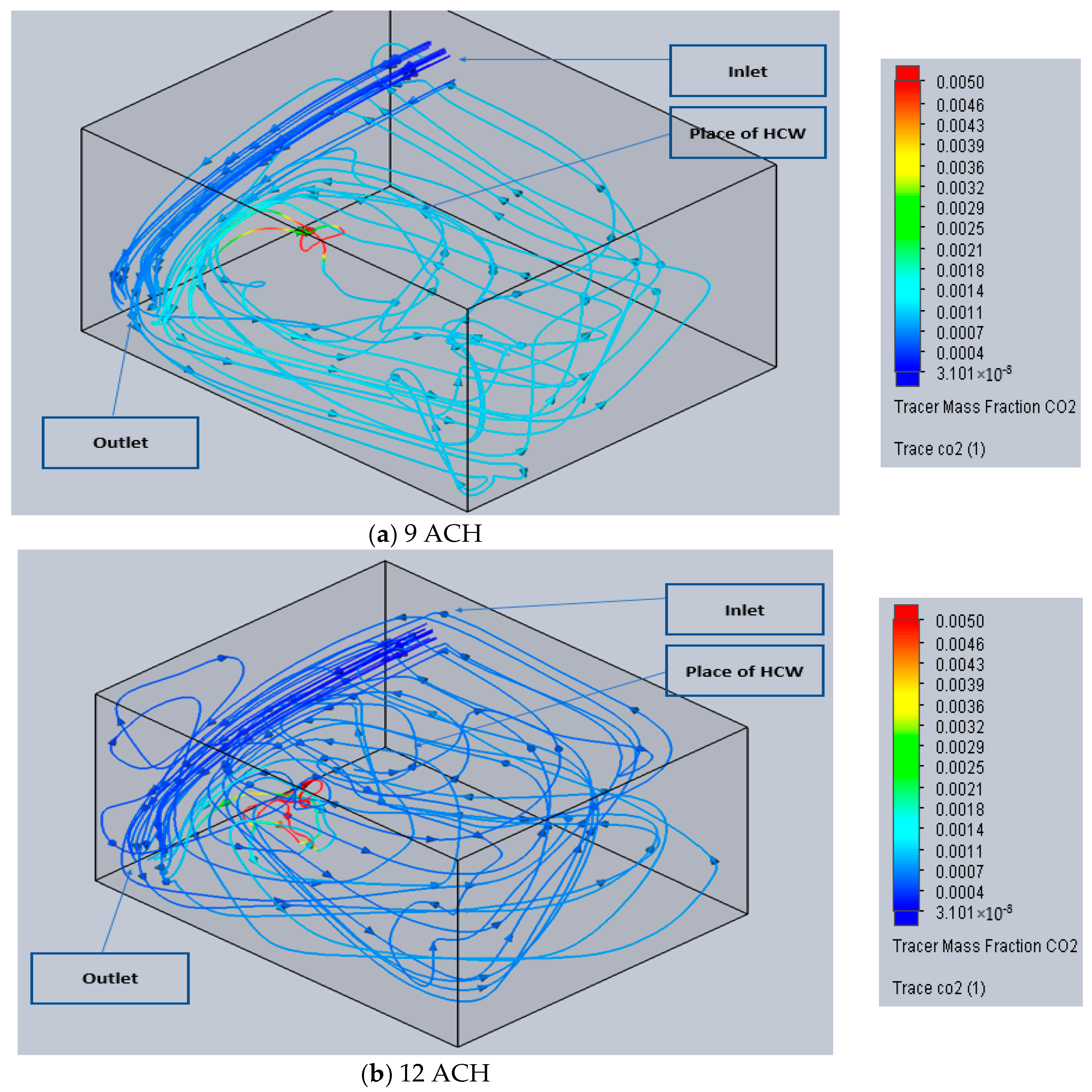
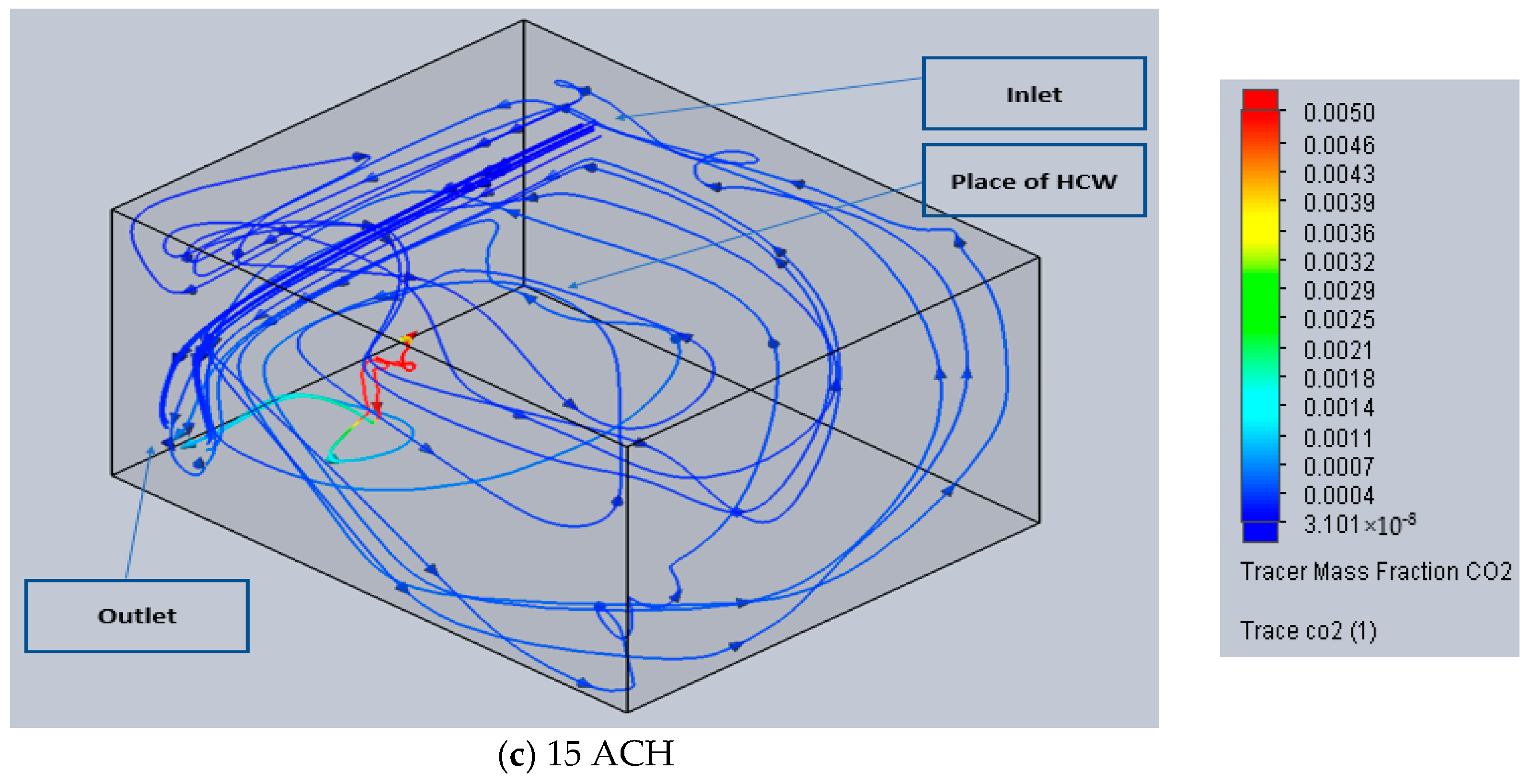
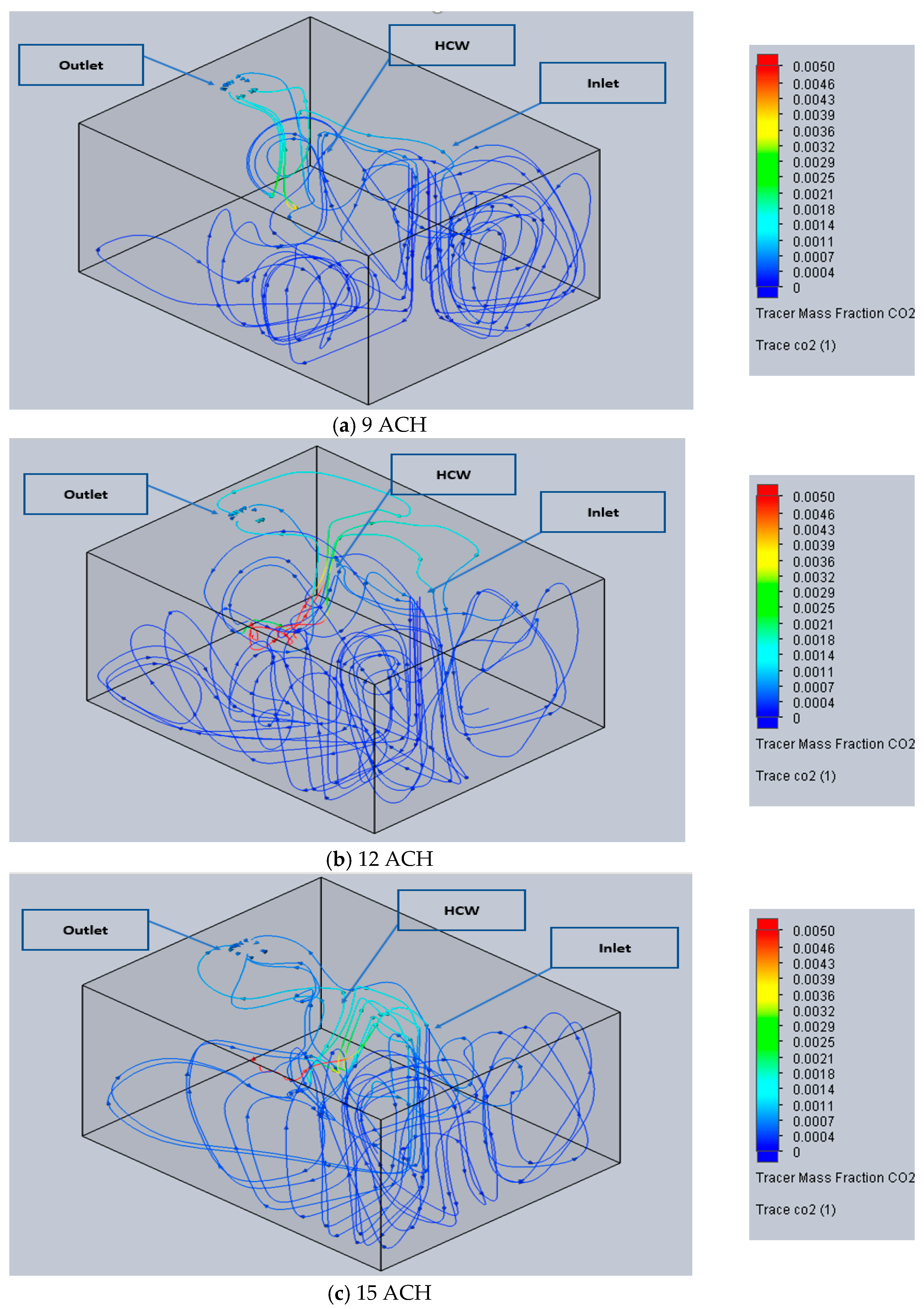
3.1.2. Tracer Study of CO2 (Flow Trajectories) Section of Each Case
3.1.3. Tracer Study of CO2 (Flow Trajectories)
3.2. Cases 4, 5 and 6
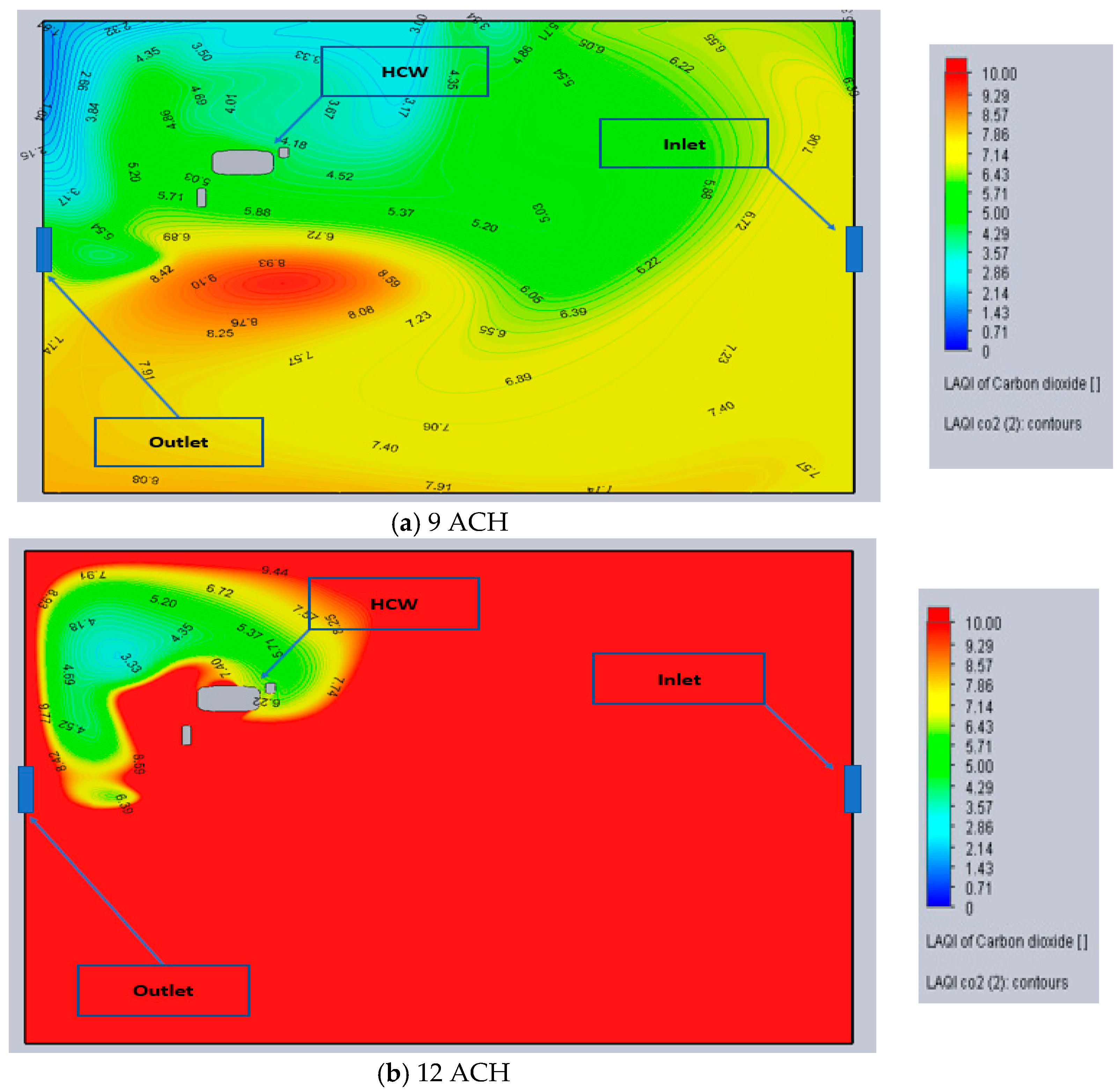
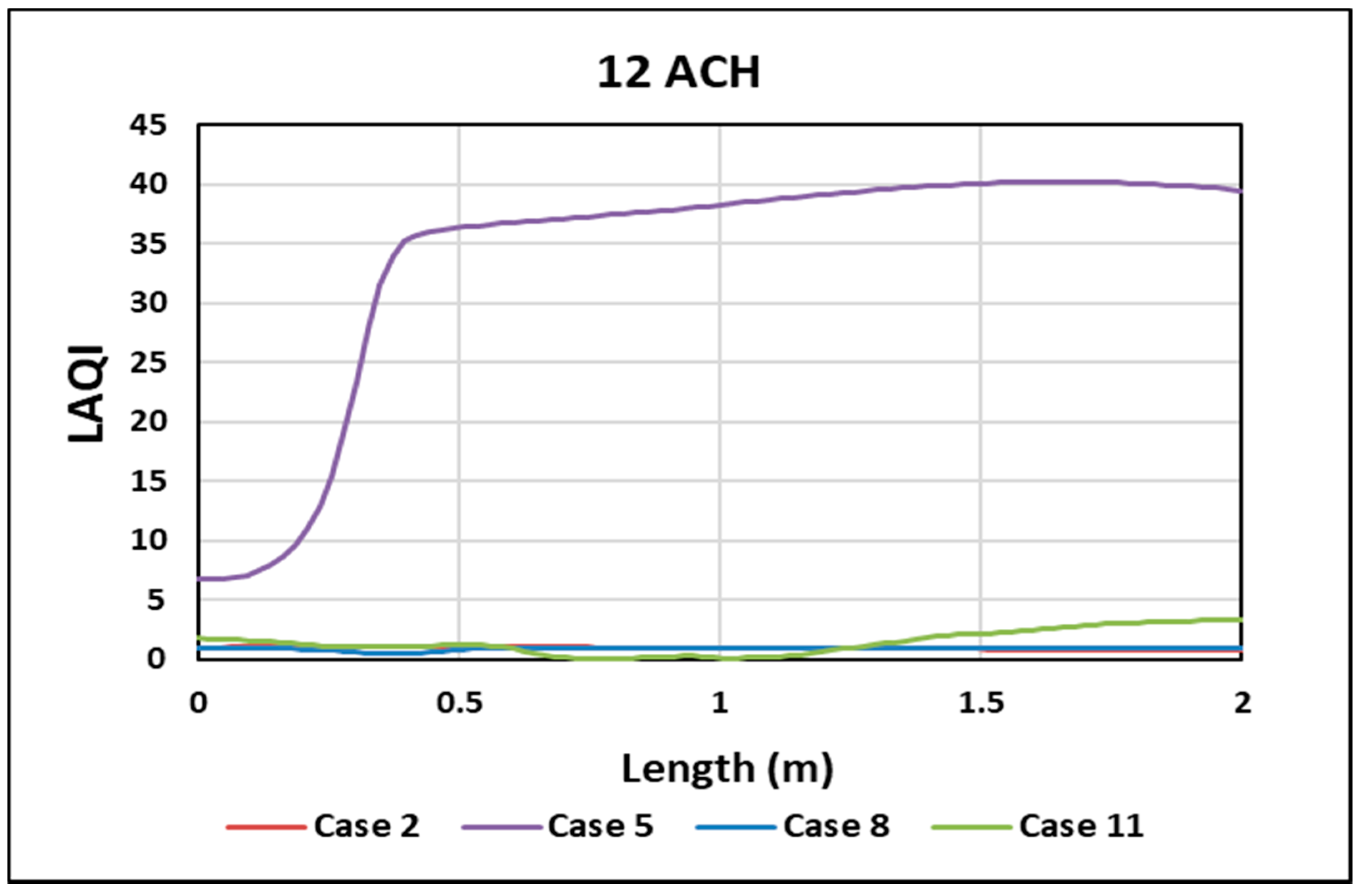
3.2.1. Local Air Quality Index (LAQI)
3.2.2. Tracer Study of CO2 (Flow Trajectories)
3.3. Cases 7, 8 and 9
3.3.1. Local Air Quality Index (LAQI)
3.3.2. Tracer Study of CO2 (Flow Trajectories)
3.4. Cases 10, 11 and 12
3.4.1. Local Air Quality Index (LAQI)
3.4.2. Tracer Study of CO2 (Flow Trajectories)
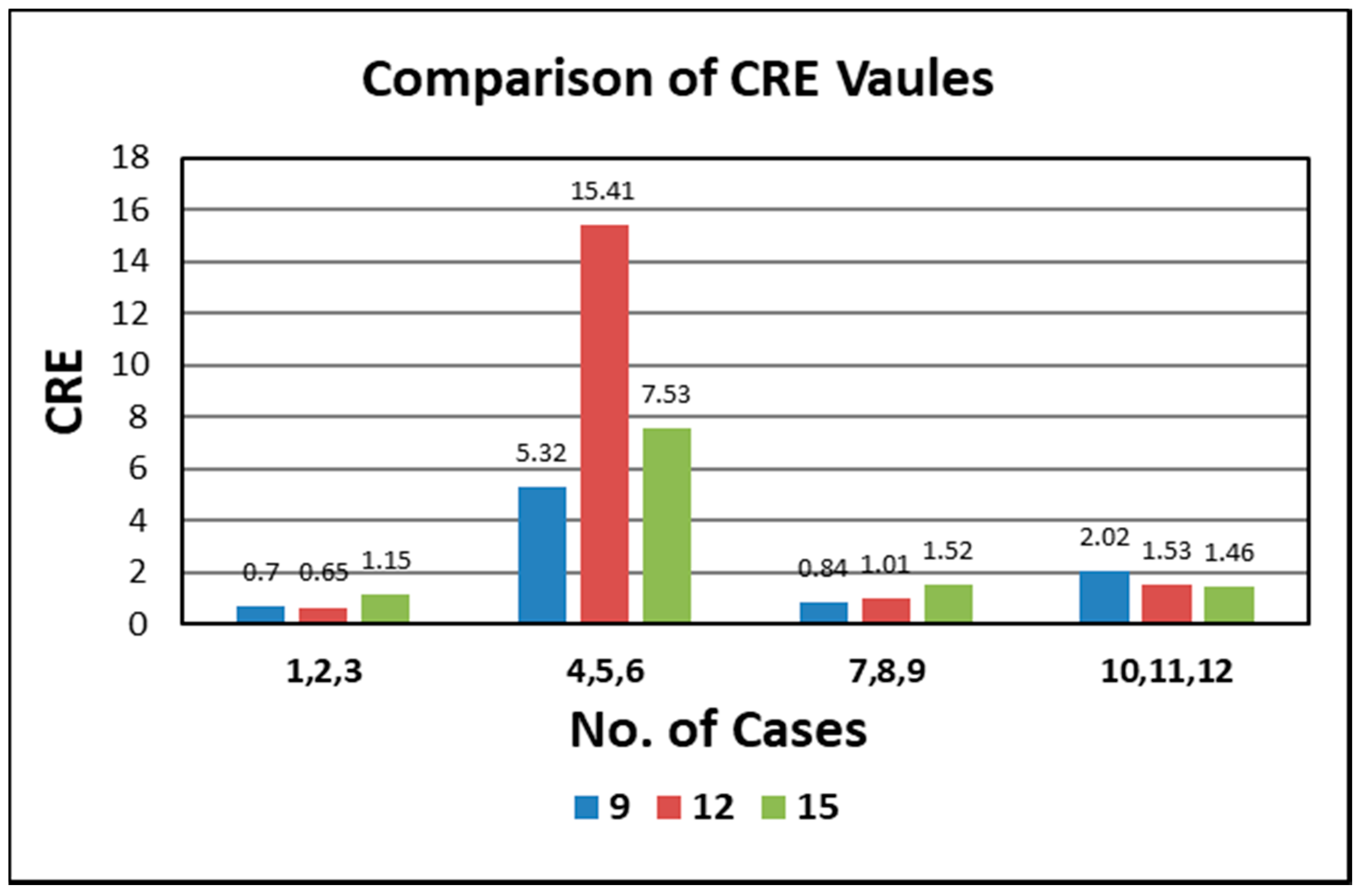
3.5. Contaminant Removal Effectiveness (CRE)
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Borro, L.; Mazzei, L.; Raponi, M.; Piscitelli, P.; Miani, A.; Secinaro, A. The role of air conditioning in the diffusion of Sars-CoV-2 in indoor environments: A first computational fluid dynamic model, based on investigations performed at the Vatican State Children’s hospital. Environ. Res. 2021, 193, 110343. [Google Scholar] [CrossRef] [PubMed]
- Hallé. Prediction of Bioparticles Dispersion and Distribution in a Hospital Isolation Room. Ph.D. Thesis, École De Technologie Supérieure, Montreal, QC, Canada, 2016. [Google Scholar]
- Anuraghava, C.; Abhiram, K.; Reddy, V.N.; Rajan, H. CFD modelling of airborne virus diffusion characteristics in a negative pressure room with mixed mode ventilation. Int. J. Simul. Multidiscip. Des. Optim. 2021, 12, 1. [Google Scholar] [CrossRef]
- Novoselac, A.; Srebric, J. Comparison of air exchange efficiency and contaminant removal effectiveness as IAQ indices. Trans.-Am. Soc. Heat. Refrig. Air Cond. Eng. 2003, 109, 339–349. Available online: https://www.caee.utexas.edu/prof/novoselac/Publications/Novoselac_ASHRAE_Transactions_2003.pdf (accessed on 11 July 2003).
- Tian, X.; Zhang, S.; Awbi, H.B.; Liao, C.; Cheng, Y.; Lin, Z. Multi-indicator evaluation on ventilation effectiveness of three ventilation methods: An experimental study. Build Environ. 2020, 1, 180. [Google Scholar] [CrossRef]
- Daisey, J.M.; Angell, W.J.; Apte, M.G. Indoor Air Quality, Ventilation And Health Symptoms In Schools: An Analysis Of Existing Information. Indoor Air Berkeley USA 2003, 13, LBNL-48287. [Google Scholar] [CrossRef] [Green Version]
- American Society of Heating R and ACEngineers. HVAC Design Manual for Hospitals and Clinics. 2012. 301p. Available online: https://www.ashrae.org/technical-resources/bookstore/hvac-design-manual-for-hospitals-and-clinics (accessed on 11 July 2003).
- Bolashikov, Z.D.; Melikov, A.K.; Kierat, W.; Popioek, Z.; Brand, M. Exposure of health care workers and occupants to coughed airborne pathogens in a double-bed hospital patient room with overhead mixing ventilation. HVAC R Res. 2012, 18, 602–615. [Google Scholar]
- Chow, T.T.; Kwan, A.; Lin, Z.; Bai, W. Conversion of operating theatre from positive to negative pressure environment. J. Hosp. Infect. 2006, 64, 371–378. [Google Scholar] [CrossRef]
- Alhamid, M.I.; Budihardjo Raymond, A. Design of the ventilation system and the simulation of air flow in the negative isolation room using FloVent 8.2. AIP Conf. Proc. 2018, 1984, 020016. [Google Scholar]
- Cho, J. Investigation on the contaminant distribution with improved ventilation system in hospital isolation rooms: Effect of supply and exhaust air diffuser configurations. Appl. Therm. Eng. 2019, 148, 208–218. [Google Scholar] [CrossRef]
- Mousavi. Airborne Infection in Healthcare Environments: Implications to Hospital Corridor Design [Internet]. 2015. Available online: http://digitalcommons.unl.edu/constructiondisshttp://digitalcommons.unl.edu/constructiondiss/21 (accessed on 17 July 2015).
- Abhinav, R.; Sunder, P.B.S.; Gowrishankar, A.; Vignesh, S.; Vivek, M.; Kishore, V.R. Numerical study on effect of vent locations on natural convection in an enclosure with an internal heat source. Int. Commun. Heat Mass Transf. 2013, 49, 69–77. [Google Scholar] [CrossRef]
- Abdel, K.; Saadeddin, R. The Effects of Diffuser Exit Velocity and Distance Between Supply The Effects of Diffuser Exit Velocity and Distance Between Supply and Return Apertures on the Efficiency of an Air Distribution and Return Apertures on the Efficiency of an Air Distribution System in an Office Space System in an Office Space [Internet]. 2016. Available online: https://openprairie.sdstate.edu/etd (accessed on 5 February 2016).
- Kokkonen, A.; Hyttinen, M.; Holopainen, R.; Salmi, K.; Pasanen, P. Performance testing of engineering controls of airborne infection isolation rooms by tracer gas techniques—Enhanced Reader. Indoor Built Environ. 2014, 23, 994–1001. [Google Scholar] [CrossRef]
- Villafruela, J.M.; Olmedo, I.; Berlanga, F.A.; Ruiz de Adana, M. Assessment of displacement ventilation systems in airborne infection risk in hospital rooms. PLoS ONE 2019, 1, 14. [Google Scholar] [CrossRef] [PubMed]
- Yam, R.; Yuen, P.L.; Yung, R.; Choy, T. Rethinking hospital general ward ventilation design using computational fluid dynamics. J. Hosp. Infect. 2011, 77, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, E.S.; Grosskopf, K.R. Ventilation Rates and Airflow Pathways in Patient Rooms: A Case Study of Bioaerosol Containment and Removal. Ann. Occup. Hyg. 2014, 59, 1190–1199. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Oladokun, M.; Lin, Z. Reducing the exposure risk in hospital wards by applying stratum ventilation system. Build Environ. 2020, 183, 107204. [Google Scholar] [CrossRef]
- Fan, M.; Fu, Z.; Wang, J.; Wang, Z.; Suo, H.; Kong, X.; Li, H. A review of different ventilation modes on thermal comfort, air quality and virus spread control. Build. Environ. 2022, 212, 108831. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, T. Performance Investigation of Building Ventilation System by Calculating Comfort Criteria through HVAC Simulation. IOSR J. Mech. Civ. Eng. 2012, 3, 7–12. [Google Scholar] [CrossRef]
- Risberg, D. Daniel Risberg Analysis of the Thermal Indoor Climate with Computational Fluid Dynamics for Buildings in Sub-arctic Regions. Ph.D. Thesis, Luleå University of Technology, Luleå, Sweden, 2018. [Google Scholar]
- Ghanta, N. Meta-Modeling and Optimization of Computational Fluid Dynamics (CFD) Analysis in Thermal Comfort for Energy-Efficient Chilled Beams-Based Heating, Ventilation and Air-Conditioning (HVAC) Systems. Ph.D. Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, May 2020. [Google Scholar]
- Solidworks Flow Simulation. Technical Reference Solidworks Flow Simulation. 2021. Available online: https://www.solidworks.com/product/solidworks-flow-simulation (accessed on 5 February 2021).
- Mekbib Kifle, P. CFD Simulation of Heavily Insulated Office Cubicle Heated by Ventilation Air Done in Collaboration with [Internet]. 2018. Available online: https://www.oslomet.no (accessed on 23 May 2018).
- Azmi, M.A.; Hassan, N.N.; Salleh, Z.M. Investigation of Airflow in A Restaurant to Prevent COVID-19 Transmission Using CFD Software. Prog. Eng. Appl. Technol. 2021, 3, 977–991. [Google Scholar]
- Çuhadaroğlu, B.; Sungurlu, C. ID 8-A CFD analysis of air distributing performance of a New Type HVAC Diffuser. 2015. Available online: https://www.researchgate.net/publication/288324226_ID_8_-A_CFD_analysis_of_air_distributing_performance_of_a_New_Type_HVAC_Diffuser. (accessed on 27 December 2015).
- Thatiparti, D.S.; Ghia, U.; Mead, K.R. Computational fluid dynamics study on the influence of an alternate ventilation configuration on the possible flow path of infectious cough aerosols in a mock airborne infection isolation room. Sci. Technol. Built. Environ. 2017, 23, 355–366. [Google Scholar] [CrossRef] [Green Version]
- Solidworks Flow Simulation 201. 2021. Available online: https://www.solidworks.com/media/solidworks-2021-flow-simulation (accessed on 5 February 2021).
- Berlanga, F.A.; Olmedo, I.; de Adana, M.R.; Villafruela, J.M.; José, J.F.S.; Castro, F. Experimental assessment of different mixing air ventilation systems on ventilation performance and exposure to exhaled contaminants in hospital rooms. Energy Build. 2018, 177, 207–219. [Google Scholar] [CrossRef] [Green Version]
- Ventilation of Health Care Facilities [Internet]. 2020. Available online: https://www.ashrae.org (accessed on 5 February 2020).
- Yoon, S.H.; Ahn, H.S.; Choi, Y.H. Numerical Study To Evaluate The Characteristics Of Hvac-Related Parameters To Reduce CO2 Concentrations In Cars. Int. J. Automot. Technol. 2016, 17, 959–966. [Google Scholar] [CrossRef]
- Cehlin, M.; Moshfegh, B. Numerical modeling of a complex diffuser in a room with displacement ventilation. Build. Environ. 2010, 45, 2240–2252. [Google Scholar] [CrossRef]
- Cao, G.; Ruponen, M.; Paavilainen, R.; Kurnitski, J. Modelling and simulation of the near-wall velocity of a turbulent ceiling attached plane jet after its impingement with the corner. Build. Environ. 2011, 46, 489–500. [Google Scholar] [CrossRef]
- Gao, N.; Niu, J. Transient CFD simulation of the respiration process and inter-person exposure assessment. Build. Environ. 2006, 41, 1214–1222. [Google Scholar] [CrossRef]
- Vasilopoulos, K.; Sarris, I.E.; Tsoutsanis, P. Assessment of air flow distribution and hazardous release dispersion around a single obstacle using Reynolds-averaged Navier-Stokes equations. Heliyon 2019, 5, e01482. [Google Scholar] [CrossRef] [Green Version]
- Georges, L. CFD Simulation of Active Displacement Ventilation Tollef Hjermann. 2017. Available online: http://hdl.handle.net/11250/2454912org (accessed on 15 June 2017).
- Kong, X.; Guo, C.; Lin, Z.; Duan, S.; He, J.; Ren, Y.; Ren, J. Experimental study on the control effect of different ventilation systems on fine particles in a simulated hospital ward. Sustain. Cities Soc. 2021, 73, 103102. [Google Scholar] [CrossRef]






















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Length (m) | Width (m) | Height (m) | |
|---|---|---|---|
| Room | 5.00 | 4.00 | 2.8 |
| Diffusers | 0.4 | 0.4 | - |
| Bed | 2.2 | 0.9 | 0.4 |
| Mannequin | 1.75 | 0.6 | - |
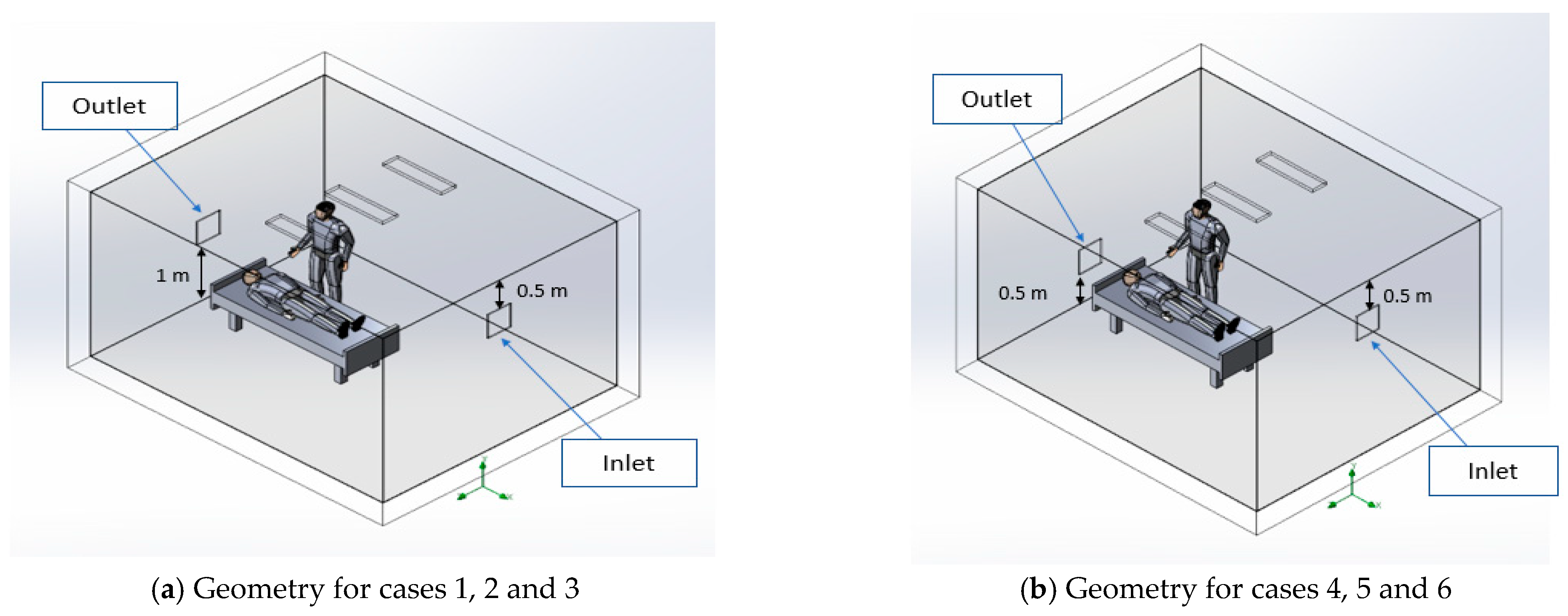
| Case No. | Air Inlet (AI) | Air Outlet (AO) | Distance | Ventilation |
|---|---|---|---|---|
| 1, 2, 3 | Sidewall | Sidewall | AI = 0.5 roof, AO = 1 floor | 0.14, 0.18, 0.23 for ACH 9, 12 and 15 |
| 4, 5, 6 | Sidewall | Sidewall | AI = 0.5 roof, AO = 0.5 floor | 0.14, 0.18, 0.23 for ACH 9, 12 and 15 |
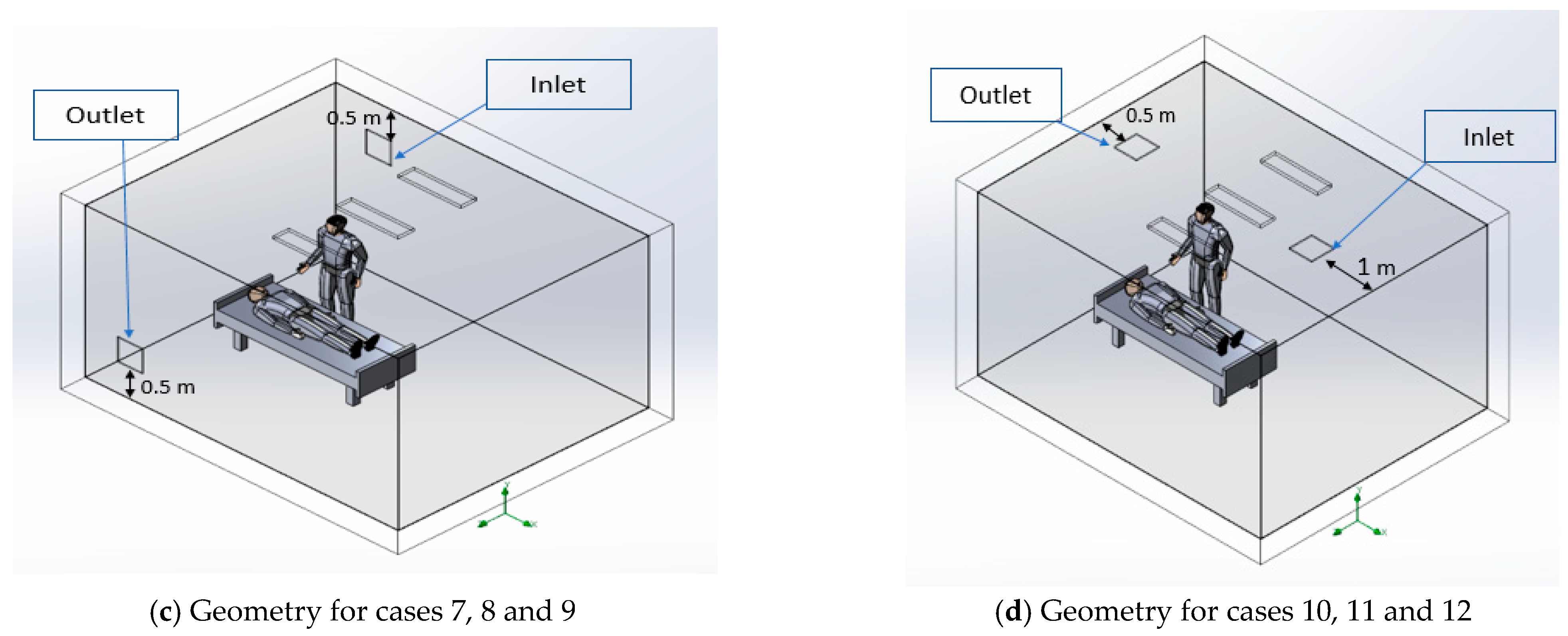
| 7, 8, 9 | Behind the HCW | In front of HCW | AI = AO = 0.5 roof & floor | 0.14, 0.18, 0.23 for ACH 9, 12 and 15 |
| 10, 11, 12 | Roof | Roof | AI = 1 SW AO = 0.5 SW | 0.14, 0.18, 0.23 for ACH 9, 12 and 15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alkhalaf, M.; Ilinca, A.; Hayyani, M.Y. CFD Investigation of Ventilation Strategies to Remove Contaminants from a Hospital Room. Designs 2023, 7, 5. https://doi.org/10.3390/designs7010005
Alkhalaf M, Ilinca A, Hayyani MY. CFD Investigation of Ventilation Strategies to Remove Contaminants from a Hospital Room. Designs. 2023; 7(1):5. https://doi.org/10.3390/designs7010005
Chicago/Turabian StyleAlkhalaf, Mustafa, Adrian Ilinca, and Mohamed Yasser Hayyani. 2023. "CFD Investigation of Ventilation Strategies to Remove Contaminants from a Hospital Room" Designs 7, no. 1: 5. https://doi.org/10.3390/designs7010005
APA StyleAlkhalaf, M., Ilinca, A., & Hayyani, M. Y. (2023). CFD Investigation of Ventilation Strategies to Remove Contaminants from a Hospital Room. Designs, 7(1), 5. https://doi.org/10.3390/designs7010005