Check the Ear. The Importance of Ear Examinations in Assessment of Intracranial Subdural Empyema


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
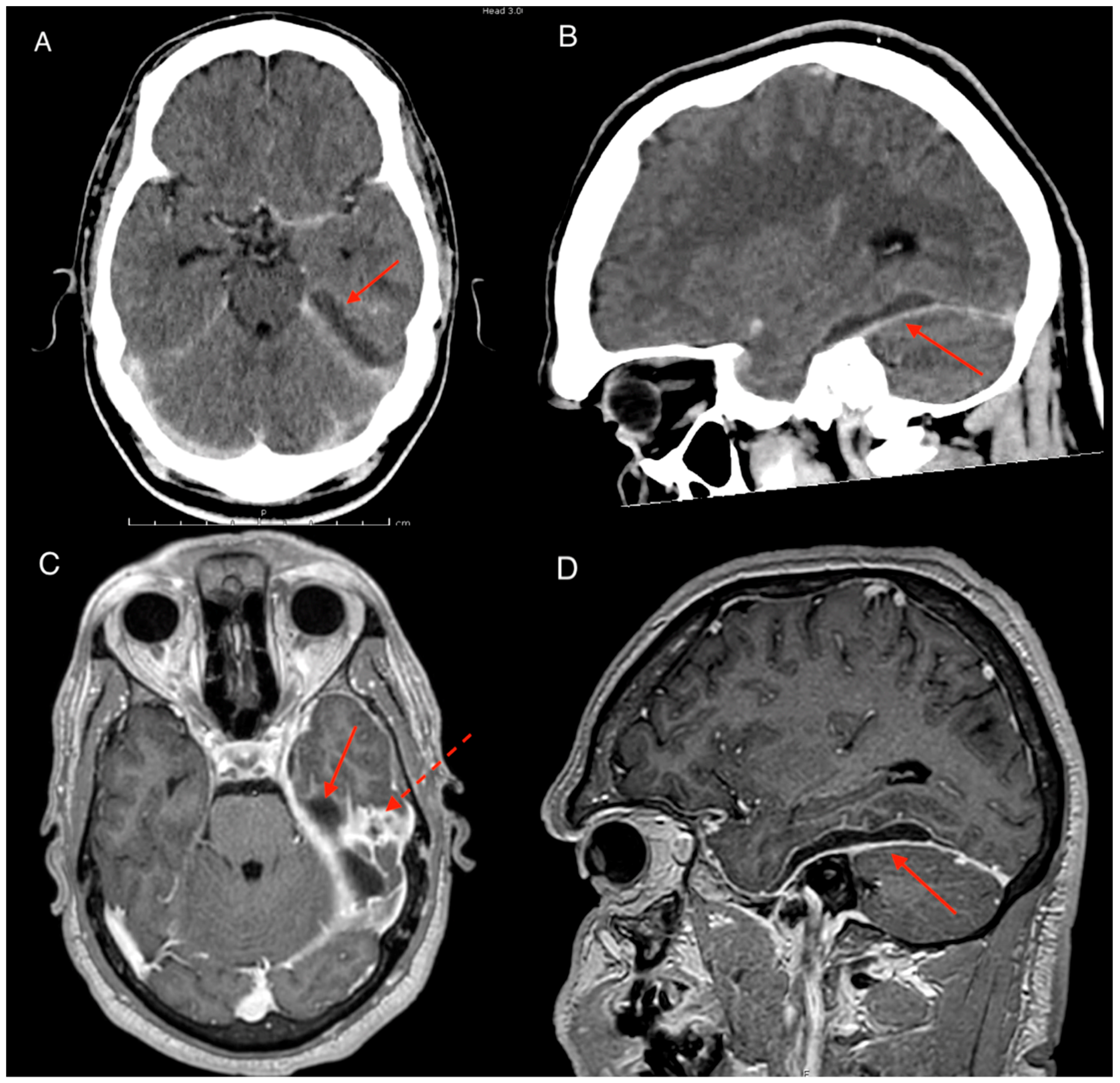
2. Case
3. Discussion
3.1. Epidemiology
3.2. Pathogenesis
3.3. Management
4. Conclusions
Funding
Conflicts of Interest
References
- Bruner, D.; Littlejohn, L.; Pritchard, A. Subdural empyema presenting with seizure, confusion, and focal weakness. West J. Emerg. Med. 2013, 13, 509–511. [Google Scholar] [CrossRef] [PubMed]
- Osma, U.; Cureoglu, S.; Hosoglu, S. The complications of chronic otitis media: Report of 93 cases. J. Laryngol. Otol. 2000, 114, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Penido, N.D.O.; Borin, A.; Iha, L.C.N.; Suguri, V.M.; Onishi, E.; Fukuda, Y.; Laércio, M.C.O. Intracranial complications of otitis media: 15 years of experience in 33 patients. Arch. Otolaryngol. Head Neck Surg. 2005, 132, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Hlavin, M.L.; Kaminski, H.J.; Fenstermaker, R.A.; White, R.J. intracranial suppuration: a modern decade of postoperative subdural empyema and epidural abscess. Neurosurgery 1994, 34, 974–981. [Google Scholar] [CrossRef] [PubMed]
- French, H.; Schaefer, N.; Hons, M.; Keijzers, G.; Barison, D.; Olson, S. Intracranial subdural empyema: A 10-year case series. Ochsner J. 2014, 14, 188–194. [Google Scholar] [PubMed]
- Dill, S.R.; Cobbs, C.G.; McDonald, C.K. Subdural empyema: Analysis of 32 cases and review. Clin. Infect. Dis. 1995, 20, 372–386. [Google Scholar] [CrossRef] [PubMed]
- Goldman, S.A.; Ankerstjerne, J.K.B.; Welker, K.B.; Chen, D.A. Fatal meningitis and brain abscess resulting from foreign body-induced otomastoiditis. Arch. Otolaryngol. Head Neck Surg. 1998, 118, 6–8. [Google Scholar] [CrossRef]
- Madhugiri, V.S.; Sastri, B.V.S.; Bhagavatula, I.D.; Sampath, S.; Chandramouli, B.A.; Pandey, P. Posterior fossa subdural empyema in children-management and outcome. Child’s Nerv. Syst. 2011, 27, 137–144. [Google Scholar] [CrossRef]
- Nathoo, N.; Nadvi, S.S.; van Dellen, J.R.; Gouws, E. Intracranial subdural empyemas in the era of computed tomography: A review of 699 cases. Neurosurgery 1999, 44, 529–535. [Google Scholar] [CrossRef]
- Sharma, N.; Jaiswal, A.A.; Banerjee, P.K.; Garg, A.K. Complications of chronic suppurative otitis media and their management: A single institution 12 years experience. Indian J. Otolaryngol. 2015, 67, 353–360. [Google Scholar] [CrossRef]
- Wu, J.F.; Jin, Z.; Yang, J.M.; Liu, Y.H.; Duan, M.L. Extracranial and intracranial complications of otitis media: 22-year clinical experience and analysis. Acta Otolaryngol. 2012, 132, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Jervis-Bardy, J.; Sanchez, L.; Carney, A.S. Otitis media in indigenous australian children: Review of epidemiology and risk factors. J. Laryngol. Otol. 2014, 128, 16–27. [Google Scholar] [CrossRef]
- Mackenzie, G.A.; Carapetis, J.R.; Leach, A.J.; Morris, P.S. Pneumococcal vaccination and otitis media in Australian Aboriginal infants: Comparison of two birth cohorts before and after introduction of vaccination. BMC Pediatr. 2009, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Chronic Suppurative Otitis Media: Burden of Illness and Management Options; WHO: Geneva, Switzerland, 2004; pp. 1–84. [Google Scholar]
- Bailie, R.; Stevens, M.; McDonald, E.; Brewster, D.; Guthridge, S. Exploring cross-sectional associations between common childhood illness, housing and social conditions in remote Australian Aboriginal communities. BMC Public Health 2010, 10, 147. [Google Scholar] [CrossRef] [PubMed]
- Jacoby, P.A.; Coates, H.L.; Arumugaswamy, A.; Elsbury, D.; Stokes, A.; Monck, R.; Finucane, J.M.; Weeks, S.A.; Lehmann, D. The effect of passive smoking on the risk of otitis media in Aboriginal and non-Aboriginal children in the Kalgoorlie-Boulder region of Western Australia. Med. J. Aust. 2008, 188, 599–603. [Google Scholar] [PubMed]
- de Bonis, P.; Anile, C.; Pompucci, A.; Labonia, M.; Lucantoni, C.; Mangiola, A. Cranial and spinal subdural empyema. Br. J. Neurosurg 2009, 23, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Germiller, J.A.; Monin, D.L.; Sparano, A.M.; Tom, L.W.C. Intracranial complications of sinusitis in children and adolescents and their outcomes. Arch. Otolaryngol. Head Neck Surg. 2006, 132, 969–976. [Google Scholar] [CrossRef] [PubMed]
- Chalishazar, U.K.; Singh, V. Correlation between a foreign body in the external auditory canal and otitis media with effusion. J. Laryngol. Otol. 2007, 121, 850–852. [Google Scholar] [CrossRef]
- Charlton, A.; Janjua, N.; Rejali, D. Cotton bud in external ear canal causing necrotising otitis externa and subdural abscess. BMJ Case Rep. 2019, 12, 1–4. [Google Scholar] [CrossRef]
- Gupta, S.; Vachhrajani, S.; Kulkarni, A.V.; Taylor, M.D.; Dirks, P.; Drake, J.M.; Rutka, J.T. Neurosurgical management of extraaxial central nervous system infections in children. J. Neurosurg Pediatr. PED 2011, 7, 441–451. [Google Scholar] [CrossRef]
- Hendaus, M.A. Subdural empyema in children. Glob. J. Health Sci. 2013, 5, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Osborn, M.K.; Steinberg, J.P. Subdural empyema and other suppurative complications of paranasal sinusitis. Lancet. Infect. Dis. 2007, 7, 62–67. [Google Scholar] [CrossRef]
- Mauser, H.W.; Ravijst, R.A.; Elderson, A.; van Gijn, J.; Tulleken, C.A. Nonsurgical treatment of subdural empyema: Case report. J. Neurosurg. 1985, 63, 128–130. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Chen, N.; Tu, P.; Lee, S.; Wu, C. The treatment and outcome of postmeningitic subdural empyema in infants. J. Neurosurg. Pediatr. 2010, 6, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Bannister, G.; Williams, B.; Smith, S. Treatment of subdural empyema. J. Neurosurg. 1981, 55, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Maharaj, T.J. Radical mastoidectomy: Its place in otitic intracranial complications. J. Laryngol. Otol. 1993, 107, 1113–1118. [Google Scholar] [CrossRef] [PubMed]
- Kurien, M.; Job, A.; Mathew, J.; Chandy, M. Otogenic intracranial abscess: concurrent craniotomy and mastoidectomy—changing trends in a developing country. Arch. Otolaryngol. Head Neck Surg. 1998, 124, 1353–1356. [Google Scholar] [CrossRef] [PubMed]



© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, J.; Redmond, M. Check the Ear. The Importance of Ear Examinations in Assessment of Intracranial Subdural Empyema. Trop. Med. Infect. Dis. 2019, 4, 120. https://doi.org/10.3390/tropicalmed4030120
Yoon J, Redmond M. Check the Ear. The Importance of Ear Examinations in Assessment of Intracranial Subdural Empyema. Tropical Medicine and Infectious Disease. 2019; 4(3):120. https://doi.org/10.3390/tropicalmed4030120
Chicago/Turabian StyleYoon, Joseph, and Michael Redmond. 2019. "Check the Ear. The Importance of Ear Examinations in Assessment of Intracranial Subdural Empyema" Tropical Medicine and Infectious Disease 4, no. 3: 120. https://doi.org/10.3390/tropicalmed4030120
APA StyleYoon, J., & Redmond, M. (2019). Check the Ear. The Importance of Ear Examinations in Assessment of Intracranial Subdural Empyema. Tropical Medicine and Infectious Disease, 4(3), 120. https://doi.org/10.3390/tropicalmed4030120