
Cholera Hot-Spots and Contextual Factors in Burundi, Planning for Elimination

 , ,
, ,
Abstract
:1. Introduction
1.1. Background Information Regarding Burundi
1.2. Study Background Information
2. Materials and Methods
2.1. Cholera Case Data
2.2. Population Data
2.3. Geographic Information Systems (GIS) Data
2.4. Identification of Hotspots
2.5. Definitions in Data Management
3. Results
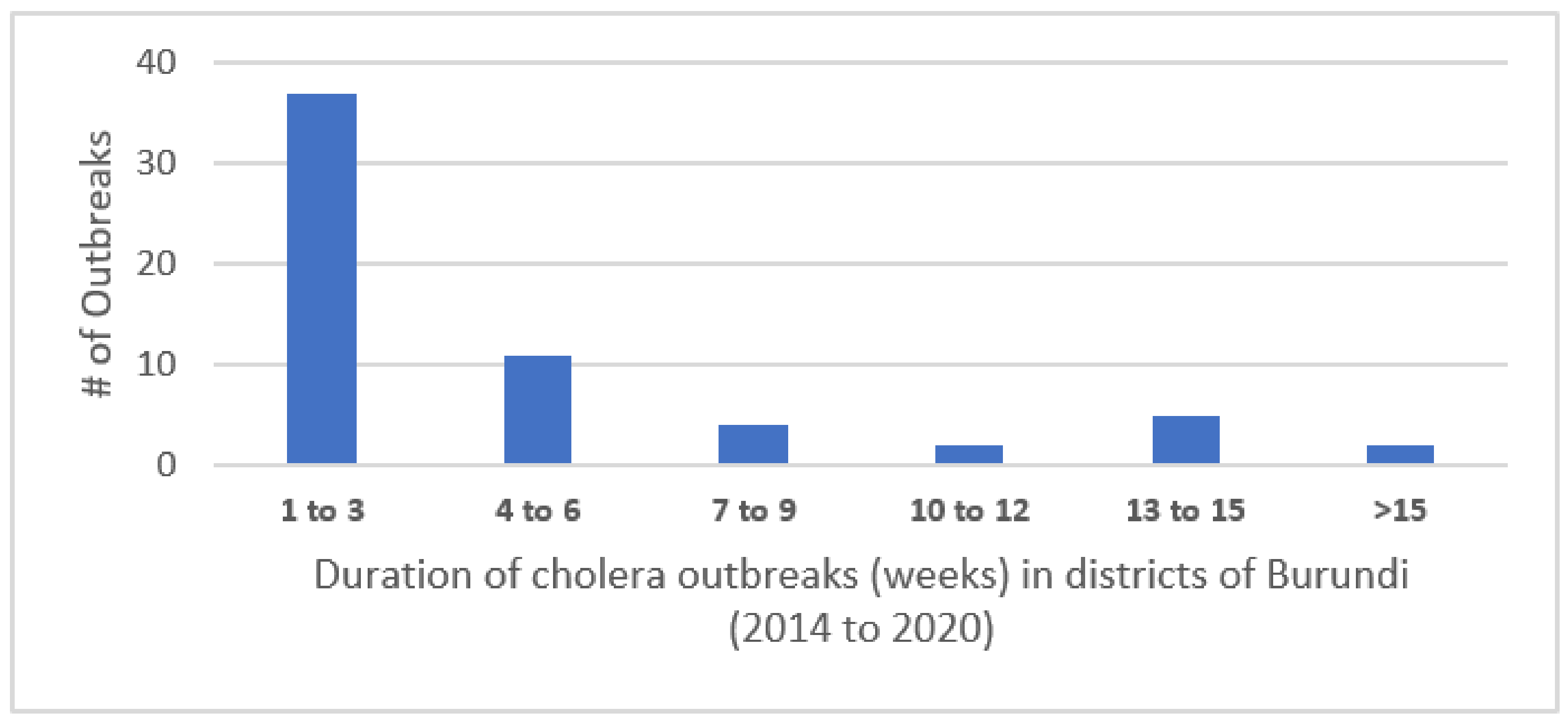
3.1. Weekly Number of Cases
3.2. Hotspot Classification–Mean Annual Incidence and Persistence
4. Discussion
4.1. Hotspots and Contextual Factor Findings
4.2. Planning for Elimination
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Information WWC. Average Monthly Snow And Rainfall In Bujumbura In Millimeter 2019. Available online: https://weather-and-climate.com/average-monthly-precipitation-Rainfall,Bujumbura,Burundi (accessed on 18 March 2021).
- United_Nations_Statistics_Division. UN Data. A World of Informations. 2021. Available online: http://data.un.org/default.aspx (accessed on 1 March 2021).
- World_Food_Program. Where We Work/Burundi Italy: World Food Program. 2020. Available online: https://www.wfp.org/countries/burundi (accessed on 2 March 2021).
- Joint_Monitoring_Project_(JMP). WHO/UNICEF. 2021. Available online: https://washdata.org/data/household#!/ (accessed on 16 February 2021).
- UNICEF. UNICEF Burundi Humanitarian Situation Report No. 4 - Reporting Period: 1 January to 31 December 2020 New York: UNICEF. 2021. Available online: https://reliefweb.int/report/burundi/unicef-burundi-humanitarian-situation-report-no-4-reporting-period-01-january-31-0 (accessed on 6 February 2021).
- International_Organization_for_Migration. OM Burundi Emergency Tracking Overview—Natural Disasters: October 2018–June 2019. International Organization for Migration. 2019. Available online: https://reliefweb.int/report/burundi/iom-burundi-emergency-tracking-overview-natural-disasters-october-2018-june-2019 (accessed on 12 June 2019).
- UNHCR. Burundi Situation 2021. Available online: https://data2.unhcr.org/en/situations/burundi (accessed on 16 February 2021).
- De Wever, A.; Muylaert, K.; Van der Gucht, K.; Pirlot, S.; Cocquyt, C.; Descy, J.P. Bacterial community composition in Lake Tanganyika: Vertical and horizontal heterogeneity. Appl. Environ. Microbiol. 2005, 71, 5029–5037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nkoko, D.B.; Giraudoux, P.; Plisnier, P.D.; Tinda, A.M.; Piarroux, M.; Sudre, B. Dynamics of cholera outbreaks in Great Lakes region of Africa, 1978–2008. Emerg. Infect. Dis. 2011, 17, 2026–2034. [Google Scholar] [CrossRef] [PubMed]
- Birmingham, M.; Lee, L.; Ndayimirije, N.; Nkurikiye, S.; Hersh, B.S.; Wells, J.G.; Deming, M.S. Epidemic cholera in Burundi: Patterns of transmission in the Great Rift Valley Lake region. Lancet 1997, 349, 981–985. [Google Scholar] [CrossRef]
- World_Health_Organization. Global Health Observatory, Number of Reported Cholera Cases Geneva: WHO. 2016. Available online: https://www.who.int/gho/epidemic_diseases/cholera/cases/en/ (accessed on 16 February 2021).
- MSF. Cholera Outbreak among Burundian Refugees 2015. Available online: https://www.msf.org/tanzania-cholera-outbreak-among-burundian-refugees (accessed on 8 September 2019).
- AFRO. Status of the Implementation of the IDSR Second Edition in 2010 in the WHO African Region: AFRO. 2016. Available online: https://www.afro.who.int (accessed on 16 September 2019).
- OCHA. Burundi–Subnational Population Statistics New York. 2018. Available online: http://ghdx.healthdata.org/organizations/central-bureau-census-burundi (accessed on 16 February 2021).
- Global Task Force on Cholera Control G. Framework for the Development and Monitoring of a Multisectoral National Cholera Plan; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Humanitarian_Data_Exchange. Burundi–Health District Boundaries (2017) OCHA. 2017. Available online: https://data.humdata.org/dataset/burundi-health-district-boundaries-2017 (accessed on 16 February 2021).
- GTFCC. Guidance and tool for countries to identify priority areas for intervention Geneva: GTFCC. Available online: https://www.gtfcc.org/resources/guidance-and-tool-for-countries-to-identify-priority-areas-for-intervention/ (accessed on 16 February 2021).
- Global Task Force on Cholera Control. Interim Guidance Document on Cholera Surveillance; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- M’Bangombe, M.; Pezzoli, L.; Reeder, B.; Kabuluzi, S.; Msyamboza, K.; Masuku, H.; Ngwira, B.; Cavailler, P.; Grandesso, F.; Palomares, A.; et al. Oral cholera vaccine in cholera prevention and control, Malawi. Bull. World Health Organ. 2018, 96, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Grandesso, F.; Kasambara, W.; Page, A.-L.; Debes, A.K.; M’Bang’Ombe, M.; Palomares, A.; Lechevalier, P.; Pezzoli, L.; Alley, I.; Salumu, L.; et al. Effectiveness of oral cholera vaccine in preventing cholera among fishermen in Lake Chilwa, Malawi: A case-control study. Vaccine 2019, 37, 3668–3676. [Google Scholar] [CrossRef] [PubMed]
- Sauvageot, D.; Saussier, C.; Gobeze, A.; Chipeta, S.; Mhango, I.; Kawalazira, G.; Mengel, M.A.; Legros, D.; Cavailler, P.; M’Bang’Ombe, M. Oral cholera vaccine coverage in hard-to-reach fishermen communities after two mass Campaigns, Malawi, 2016. Vaccine 2017, 35, 5194–5200. [Google Scholar] [CrossRef] [PubMed]
- Bwire, G.; Ali, M.; Sack, D.A.; Nakinsige, A.; Naigaga, M.; Debes, A.K.; Ngwa, M.C.; Brooks, W.A.; Orach, C.G. Identifying cholera “hotspots” in Uganda: An analysis of cholera surveillance data from 2011 to 2016. PLoS Negl. Trop. Dis. 2017, 11, e0006118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bwire, G. Lessons and challenges of implementing an integrated oral cholera vaccine and WaSH response to a cholera epidemic in Hoima district, Uganda. BMJ Open 2019. under review. [Google Scholar]
- Ferreras, E.; Matapo, B.; Chizema-Kawesha, E.; Chewe, O.; Mzyece, H.; Blake, A.; Moonde, L.; Zulu, G.; Poncin, M.; Sinyange, N.; et al. Delayed second dose of oral cholera vaccine administered before high-risk period for cholera transmission: Cholera control strategy in Lusaka, 2016. PLoS ONE 2019, 14, e0219040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iyer, A.S.; Bouhenia, M.; Rumunu, J.; Abubakar, A.; Gruninger, R.J.; Pita, J.; Lino, R.L.; Deng, L.L.; Wamala, J.F.; Ryan, E.T.; et al. Immune Responses to an Oral Cholera Vaccine in Internally Displaced Persons in South Sudan. Sci. Rep. 2016, 6, 35742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouhenia, M. Overview of the OCV Campaigns in 2020. In Proceedings of the 7th Meeting of the GTFCC Working Group on Oral Cholera, Virtual Event, 19 November–10 December 2020. [Google Scholar]
- Azman, A.S.; Luquero, F.J.; Ciglenecki, I.; Grais, R.F.; Sack, D.A.; Lessler, J. Correction: The Impact of a One-Dose versus Two-Dose Oral Cholera Vaccine Regimen in Outbreak Settings: A Modeling Study. PLoS Med. 2015, 12, e1001867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qadri, F.; Ali, M.; Lynch, J.; Chowdhury, F.; Khan, A.I.; Wierzba, T.F.; Excler, J.-L.; Saha, A.; Islam, T.; Begum, Y.; et al. Efficacy of a single-dose regimen of inactivated whole-cell oral cholera vaccine: Results from 2 years of follow-up of a randomised trial. Lancet Infect. Dis. 2018, 18, 666–674. [Google Scholar] [CrossRef] [Green Version]
- Ingelbeen, B.; Hendrickx, D.; Miwanda, B.; Van Der Sande, M.A.; Mossoko, M.; Vochten, H.; Riems, B.; Nyakio, J.-P.; Vanlerberghe, V.; Lunguya, O.; et al. Recurrent Cholera Outbreaks, Democratic Republic of the Congo, 2008–2017. Emerg. Infect. Dis. 2019, 25, 856–864. [Google Scholar] [CrossRef] [PubMed]
- Bwire, G.; Sack, D.A.; Almeida, M.; Li, S.; Voeglein, J.B.; Debes, A.K.; Kagirita, A.; Buyinza, A.W.; Orach, C.G.; Stine, O.C. Molecular characterization of Vibrio cholerae responsible for cholera epidemics in Uganda by PCR, MLVA and WGS. PLoS Negl. Trop. Dis. 2018, 12, e0006492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bwire, G.; Mwesawina, M.; Baluku, Y.; Kanyanda, S.S.E.; Orach, C.G. Cross-Border Cholera Outbreaks in Sub-Saharan Africa, the Mystery behind the Silent Illness: What Needs to Be Done? PLoS ONE 2016, 11, e0156674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bwire, G.; Munier, A.; Ouedraogo, I.; Heyerdahl, L.; Komakech, H.; Kagirita, A.; Wood, R.; Mhlanga, R.; Njanpop-Lafourcade, B.; Malimbo, M.; et al. Epidemiology of cholera outbreaks and socio-economic characteristics of the communities in the fishing villages of Uganda: 2011–2015. PLoS Negl. Trop. Dis. 2017, 11, e0005407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khonje, A.; Metcalf, C.A.; Diggle, E.; Mlozowa, D.; Jere, C.; Akesson, A.; Corbet, T.; Chimanga, Z. Cholera outbreak in districts around Lake Chilwa, Malawi: Lessons learned. Malawi Med. J. 2012, 24, 29–33. [Google Scholar] [PubMed]
- Sack, R.B.; Siddique, A.K.; Longini, I.M., Jr.; Nizam, A.; Yunus, M.; Islam, M.S. A 4-year study of the epidemiology of Vibrio cholerae in four rural areas of Bangladesh. J. Infect. Dis. 2003, 187, 96–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Burundi | 234 | 355 | 333 | 1072 | 214 | 1557 | 582 | 442 | 434 | 300 | 92 |
| Tanzania | 2911 | 7700 | 4469 | 942 | 286 | 270 | 0 | 11,563 | 11,360 | 4895 | 4777 |
| Uganda | 3726 | 1095 | 2341 | 0 | 6326 | 748 | 309 | 1461 | 516 | 292 | 4440 |
| DRC | 30,150 | 22,899 | 13,884 | 21,700 | 33,661 | 26,944 | 22,203 | 19,182 | 28,093 | 56,190 | 30,768 |
| Rwanda | 23 | 0 | 0 | 0 | 9 | 0 | 0 | 0 | 355 | 0 | 0 |
| All Africa | 179,323 | 217,333 | 115,106 | 188,678 | 117,570 | 0 | 105,287 | 71,176 | 71,058 | 179,385 | 120,652 |
| World | 190,130 | 221,226 | 317,106 | 589,854 | 245,393 | 129,064 | 190,549 | 172,454 | 132,121 | 1,227,391 | 499,447 |
| Type of Hotspots | Mean Annual Incidence Per 100,000 Population (70th percentile value) | Proportion of Weeks with Cholera Reported (60th Percentile Value) | ||
|---|---|---|---|---|
| 2014–2018 | 2016–2020 | 2014–2018 | 2016–2020 | |
| High | >23 | >13 | >8% | >5% |
| Medium | >23 | >13 | ≤8% | ≤5% |
| Medium | ≤23 | ≤13 | >8% | >5% |
| Lower | ≤23 | ≤13 | ≤8% | ≤5% |
| Type of Hotspot | District | 2014–2018 | 2016–2020 | Population (Refers to Groups 2016–2020) | ||
|---|---|---|---|---|---|---|
| Mean Annual Incidence/100,000 | Proportion of Weeks with Cholera Reported (%) | Mean Annual Incidence/100,000 | Proportion of Weeks with Cholera Reported (%) | |||
| High | Bujumbura centre | 57.37 | 16.92 | 142.12 | 21.92 | 123,415 |
| Cibitoke | 30.89 | 14.23 | 42.20 | 16.15 | 229,867 | |
| Kabezi | 37.05 | 10.38 | 31.22 | 6.54 | 171,665 | |
| Total high | 524,947 | |||||
| Medium | Mpanda | 15.57 | 8.08 | 8.02 | 5.38 | 172,138 |
| Bujumbura nord * | - | - | 12.70 | 3.92 | 248,915 | |
| Rumonge Φ | 29.55 | 10 | 18.85 | 4.62 | 203,744 | |
| Total Medium | 624,797 | |||||
| Lower | Bubanza | 6.1 | 3.1 | 5.55 | 1.92 | 165,885 |
| Bujumbura sud | 5.3 | 4.2 | 5.93 | 4.23 | 124,836 | |
| Nyanza-Lac Ψ | 5.77 | 4.51 | 4.51 | 2.31 | 203,811 | |
| Mabayi δ | 6.2 | 0.4 | - | - | 230568 | |
| Total Lower | 494,532 | |||||
| Total Hotspots | 1,644,276 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Debes, A.K.; Shaffer, A.M.; Ndikumana, T.; Liesse, I.; Ribaira, E.; Djumo, C.; Ali, M.; Sack, D.A. Cholera Hot-Spots and Contextual Factors in Burundi, Planning for Elimination. Trop. Med. Infect. Dis. 2021, 6, 76. https://doi.org/10.3390/tropicalmed6020076
Debes AK, Shaffer AM, Ndikumana T, Liesse I, Ribaira E, Djumo C, Ali M, Sack DA. Cholera Hot-Spots and Contextual Factors in Burundi, Planning for Elimination. Tropical Medicine and Infectious Disease. 2021; 6(2):76. https://doi.org/10.3390/tropicalmed6020076
Chicago/Turabian StyleDebes, Amanda K., Allison M. Shaffer, Thaddee Ndikumana, Iteka Liesse, Eric Ribaira, Clement Djumo, Mohammad Ali, and David A. Sack. 2021. "Cholera Hot-Spots and Contextual Factors in Burundi, Planning for Elimination" Tropical Medicine and Infectious Disease 6, no. 2: 76. https://doi.org/10.3390/tropicalmed6020076