
Schistosomiasis with a Focus on Africa



Abstract
:1. Introduction
2. Pathogenesis
2.1. Life Cycle of Schistosoma sp.
2.2. Clinical Presentation of Schistosomiasis in Africa
2.2.1. Female Genital Schistosomiasis
2.2.2. Primary and Secondary Infertility in S. haematobium Infections
2.2.3. Male Genital Schistosomiasis
2.2.4. Bladder Cancer in S. haematobium Infections
2.3. Treatment and Control
2.4. Diagnosis
Environmental Monitoring
3. A Brief History of Schistosomiasis in Africa
3.1. Current Status of Schistosomiasis in Africa

| Country | Method | Species | Prevalence % (n/tn) | Ss/sp (%) | Study Type | Age (years) | Intensity of Infection (%) | Study Year | Study Published | Ref | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Light | Mode rate | High | ||||||||||
| Angola | Urine microscopy | S. haematobium | 61.18 (785/1283) | - | Cross-sectional survey | 9–10 | - | - | - | 2013–2014 | 2015 | [190] |
| Urine dipstick | S. haematobium | 65.8 (844/1283) | 96/61 | - | - | - | ||||||
| Haematuria | S. haematobium | 17.1 (219/1283) | 27.1/97.5 | - | - | - | ||||||
| LAMP | S. haematobium | 73.8 (127/172) | - | Evaluation | 5–14 | - | - | - | 2015 | 2018 | [191] | |
| Benin | KK | S. mansoni | 2.45 (472/19250) | - | Surveillance | 8–14 | 59.32 | 25.42 | 15.25 | 2013–2015 | 2019 | [192] |
| Urine microscopy | S. haematobium | 17.60 (3388/19250) | - | 73.99 | - | 20.01 | ||||||
| Burkina Faso | KK | S. mansoni | 5.38 (43/800) | - | Prevalence | 7–11 | - | - | - | 2013 | 2016 | [193] |
| Urine microscopy | S. haematobium | 8.76 (287/3514) | - | - | - | 2.7 | ||||||
| Cameroon | KK | S. mansoni | 61 (381/625) | - | Evaluation | 7–15 | - | - | - | 2010–2011 | 2012 | [110] |
| Urine-CCA | S. mansoni | 66.6 (416/625) | - | - | - | - | ||||||
| Urine microscopy | S. haematobium | 4.6 (29/625) | - | - | - | - | ||||||
| Dipstick | S. haematobium | 9.8 (61/625) | - | - | - | - | ||||||
| Chad | Urine microscopy | S. haematobium | 24.9 (467/1875) | - | Prevalence | 1–14 | - | - | - | 2015–2016 | 2019 | [194] |
| Côte d’Ivoire | Urine microscopy | S. haematobium | 14 (166/1187) | - | Cross-sectional survey | 5–14 | - | - | - | 2018 | 2019 | [195] |
| KK | S. mansoni | 6.1 (66/1089) | - | - | - | - | ||||||
| CCA | S. mansoni | 73.8 (104/141) | - | Cross-sectional survey | 8–12 | - | - | - | 2010 | 2011 | [109] | |
| Dipstick | S. haematobium | 4.1 (6/146) | - | - | - | - | ||||||
| Democratic Republic of the Congo | KK | S. mansoni | 82.7 (277/335) | - | Epidemiology/parasitology | 8–16 | 43.2 | 32 | 24.7 | 2011 | 2014 | [196] |
| KK | S. mansoni | 8.9 (47/526) | - | Cross-sectional survey | 7–13 | 8.8 | - | - | 2016 | 2017 | [197] | |
| Urine microscopy | S. haematobium | 0 (0/526) | - | - | - | - | ||||||
| Urine microscopy | S. haematobium | 17.4 (64/367) | - | Cross-sectional survey | >18 | - | - | 6.3 | 2016–2017 | 2019 | [198] | |
| KK | S. mansoni | 89.3 (176/197) | - | Cross-sectional survey | 11–14 | 11.7 | 22.3 | 55.3 | 2011 | 2018 | [199] | |
| KK | S. mansoni | 57.8 (231/400) | - | Cross-sectional survey | 9–14 | 18.6 | 28.6 | 52.8 | 2010 | 2016 | [200] | |
| KK | S. intercalatum | 48 (24/50) | - | Prevalence | 9–15 | 50 | 20.8 | 29.2 | 2017 | [201] | ||
| KK | S. intercalatum | 3.6 (6/167) | - | Epidemiological/parasitological survey | 8–18 | - | - | - | 1994 | 1997 | [202] | |
| Egypt | KK | S. mansoni | 35.8 (355/993) | - | Cross-sectional survey | - | - | - | - | 1994–1996 | 2020 | [203] |
| KK | S. mansoni | 1.8 (2/110) | - | Prevalence | 6–15 | - | - | - | - | 2016 | [204] | |
| Formol-ether | S. mansoni | 0.9 (1/110) | - | - | - | - | - | |||||
| CCA | S. mansoni | 11.4 (4/110) | - | - | - | - | - | |||||
| Equitorial Guinea | KK | S. intercalatum | 31.9 (114/357) | - | Evaluation | 15–24 * | - | - | 4.7 | 1988 | 1991 | [205] |
| KK | S. intercalatum | 9.6 (27/281) | - | - | - | 0.7 | 1989 | |||||
| KK | S. intercalatum | 6.6 (23/345) | - | - | - | 0.2 | 1990 | |||||
| KK | S. intercalatum | 13 (39/305) | - | Cross-sectional survey | 0–24 | - | - | 9 | 1990 | 1993 | [206] | |
| Ethiopia | KK | S. mansoni | 42.9 (136/317) | - | Cross-sectional survey | 6–15 | 20.5 | 10.7 | 11.7 | 2017 | 2019 | [207] |
| KK | S. mansoni | 76.3 (293/384) | - | 5–19 | 21.6 | 29.4 | 25.5 | 2013 | 2014 | [208] | ||
| KK | S. mansoni | 24 (120/500) | - | 6–18 | 70 | 30 | 20 | 2014 | 2016 | [209] | ||
| KK | S. mansoni | 58.6 (295/503) | - | 5–19 | 34.2 | 35.5 | 30 | 2015 | 2017 | [210] | ||
| Gabon | Urine microscopy | S. haematobium | 77.7 (66/85) | - | Evaluation | 6–39 | - | - | 34.8 | - | 2014 | [211] |
| qPCR | S. haematobium | 98.5 (65/66) | - | - | - | - | ||||||
| Urine microscopy | S. haematobium | 39.9 (103/258) | - | Longitudinal | 6–30 | - | - | - | 2016–2018 | 2019 | [212] | |
| Gambia | POC-CCA | S. haematobium | 23.3 (456/1954) | 47.98/79.44 | Prevalence | 7–14 | - | - | - | 2015 | 2017 | [213] |
| Dipstick | S. haematobium | 17.1 (334/1954) | 47.01/81.54 | - | - | - | ||||||
| Urine microscopy | S. haematobium | 10.1 (198/1954) | - | - | - | 2.7 | ||||||
| KK | S. mansoni | 0.3 (5/1954) | 60/76.76 | - | - | 0 | ||||||
| Ghana | qPCR | S. haematobium | 48.5 (79/163) | 100/59.2 | Prevalence | 2020 | [214] | |||||
| S. mansoni | 28.7 (94/328) | - | Epidemiology/Prevalence | 7–17 | 50 | 35.1 | 11.7 | 2017 | ||||
| S. mansoni | 70.1 (54/77) | - | Longitudinal | 0–4 | - | - | - | 2018 | 2020 | [215] | ||
| 7.9 (9/108) | ||||||||||||
| 13.7 (13/96) | ||||||||||||
| S. mansoni | 80.1 (153/191) | - | 5–16 | - | - | - | ||||||
| 39.9 (89/224) | ||||||||||||
| 35.9 (86/240) | ||||||||||||
| S. mansoni | 79.1 (200/253) | - | >17 | - | - | - | ||||||
| 32.1 (107/332) | ||||||||||||
| 34.8 (100/286) | ||||||||||||
| Urine microscopy | S. haematobium | 5.2 (4/76) | - | 0–4 | - | - | - | |||||
| 0 (0/105) | ||||||||||||
| 13.2 (11/87) | ||||||||||||
| S. haematobium | 23.8 (59/249) | - | 5–16 | - | - | - | ||||||
| 5.8 (14/236) | ||||||||||||
| 27.6 (63/230) | ||||||||||||
| S. haematobium | 10.3 (32/308) | - | >17 | - | - | - | ||||||
| 2.9 (10/346) | ||||||||||||
| 15.1 (41/272) | ||||||||||||
| Guinea | KK | S. mansoni | 66.2 (278/420) | - | Cross-sectional survey | 9–14 | 8.8 | 24 | 33.3 | - | 2011 | [216] |
| Urine microscopy | S. haematobium | 21.0 (88/420) | - | 12.1 | - | 8.8 | ||||||
| Guinea-Bissau | Urine microscopy | S. haematobium | 20 (18/90) | - | Prevalence | 6–15 | - | - | - | 2011 | 2016 | [217] |
| Haematuria | S. haematobium | 61.1 (11/18) | - | |||||||||
| Kenya | Urine microscopy | S. haematobium | 83.3 (95/114) | - | Evaluation | 6–15 | - | - | - | 1996–2010 | 2014 | [218] |
| Hematuria | S. haematobium | 86.0 (98/114) | - | - | - | - | ||||||
| cSEA-ELISA | S. haematobium | 79.8 (91/114) | - | - | - | - | ||||||
| PCR | S. haematobium | 100 (114/114) | - | - | - | - | ||||||
| KK | S. mansoni | 93.9 (1731/1844) | - | Evaluation | 8–12 | 10.2 | 46.9 | 42.9 | 2015 | [219] | ||
| KK | S. mansoni | 60.5 (2458/4064) | - | Prevalence | 5–19 | 49 | 35.8 | 15.2 | 2012 | 2012 | [220] | |
| Liberia | KK | S. mansoni | 87 (333/384) | - | Prevalence | 1–>40 | 25.3 | 29.2 | 31.8 | 1980 | 1985 | [221] |
| Urine microscopy | S. haematobium | 42 (177/423) | - | |||||||||
| KK | S. mansoni | 78 (276/353) | - | Prevalence | - | - | - | - | - | 2018 | [222] | |
| Madagascar | Urine microscopy | S. haematobium | 100 (79/79) | 100/100 | Prevalence | 15–33 | - | - | - | 2010 | 2020 | [223] |
| qPCR | 81 (64/79) | - | - | - | - | |||||||
| KK | S. mansoni | 5 (97/1934) | - | Baseline sentinel study | 7–10 | - | - | 0.9 | 2015 | 2016 | [224] | |
| Urine microscopy | S. haematobium | 30.5 (594/1946) | - | - | - | 15.1 | ||||||
| KK | S. mansoni | 73.6 (215/292) | - | Prevalence | 5–14 | 36.7 | 31.2 | 32.1 | 2015 | 2017 | [225] | |
| Malawi | Urine microscopy | S. haematobium | 13 (18/143) | - | Cross-sectional survey | 0.6–6 | 58 | 33 | 9 | 2012 | 2016 | [226] |
| Urine microscopy | S. haematobium | 12.5 (50/400) | Prevalence | 7–12 | 8.25 | 1.75 | 2.5 | 2012 | 2017 | [227] | ||
| Mali | Urine microscopy | S. haematobium | 51.2 (173/338) | - | Prevalence | 1–4 | 35.5 | - | 15.7 | 2011 | [228] | |
| Urine microscopy | S. haematobium | 88 (570/648) | - | Cross-sectional | 7–14 | - | - | 48.8 | 2004 | 2012 | [229] | |
| KK | S. mansoni | 17.3 (112/648) | - | - | - | 15.6 | ||||||
| KK | S. mansoni | 12.7 (81/640) | - | - | - | 9.4 | 2010 | 2012 | ||||
| Urine microscopy | S. haematobium | 61.7 (395/640) | - | - | - | 13.8 | ||||||
| Mauritania | Urine microscopy | S. haematobium | 4 (86/2162) | - | Cross-sectional survey | - | - | - | - | 2014–2015 | 2017 | [230] |
| KK | S. mansoni | 7.1 (92/1297) | - | Epidemiological survey | 5–12 | - | - | - | - | 1997 | [231] | |
| Urine microscopy | S. haematobium | 15.6 (48/307) | - | Prevalence | 7–17 | - | - | - | - | 2019 | [232] | |
| Mozambique | Urine microscopy | S. haematobium | 60.4 (11492/19039) | - | Cross-sectional survey | 5–55 | - | - | 17.7 | - | 2018 | [233] |
| Urine microscopy | S. haematobium | 59.1 (600/1015) | - | Cross-sectional survey | 5–12 | - | - | - | 2005–2007 | 2014 | [234] | |
| Urine microscopy | S. haematobium | 47 (39166/83331) | - | Prevalence | 7–22 | - | - | 17.9 | - | 2009 | [235] | |
| KK | S. mansoni | 8.7 (7250/83331) | - | - | - | - | ||||||
| Namibia | KK | S. mansoni | 4.4 (913/17896) | - | Mapping | 3–19 | - | - | - | - | 2015 | [236] |
| Dipstick | S. haematobium | 5.0 (895/17896) | - | - | - | - | ||||||
| CCA | S. mansoni | 4.4 (787/17896) | - | - | - | - | ||||||
| Urine microscopy | S. haematobium | 5.1 (913/17896) | - | - | - | - | ||||||
| Niger | Hematuria | S. haematobium | 58.4 (52/89) | - | Evaluation | 10–15 | - | - | - | - | 2011 | [237] |
| Urine microscopy | S. haematobium | 49.4 (44/89) | - | - | - | - | ||||||
| PCR | S. haematobium | 57.3 (51/89) | 100/86 | - | - | - | ||||||
| Nigeria | Urine microscopy | S. haematobium | 21.3% (26/122) | - | Comparative | 31–55 | - | - | - | - | 2018 | [238] |
| Urine microscopy | S. mansoni | 8.9 (49/551) | - | Cross-sectional survey | 1–90 | 80.8 | 15.4 | 3.8 | 2013 | 2016 | [237] | |
| Urine microscopy | S. haematobium | 8.3 (46/551) | - | Cross-sectional survey | 69.4 | 0 | 30.6 | |||||
| Urine microscopy | S. intercalatum | 5.7 (98/1709) | - | Malacological survey | 5–15 | - | - | - | 1987 | 1989 | [184] | |
| Urine microscopy | S. haematobium | 44.1 (64/145) | - | Cross-sectional survey | 5–59 | 2 | 26 | 11 | 2017 | 2019 | [239] | |
| Urine microscopy | S. haematobium | 22.7 (163/718) | - | Cross-sectional survey | 10–23 | 89.57 | - | 10.43 | 2015 | 2016 | [187] | |
| Urine microscopy | S. haematobium | 50.0 (220/443) | - | Cross-sectional survey | 5–14 | 39.5 | 7 | 4.5 | 2003 | 2008 | [240] | |
| Urine microscopy | S. haematobium | 14.5 (55/380) | - | Cross-sectional survey | 5–14 | 11.3 | 1.8 | 1.3 | 2011 | 2017 | [241] | |
| Rwanda | KK | S. mansoni | 2.7 (82/3052) | - | Cross-sectional survey | - | - | - | - | 2007 | 2008 | [242] |
| São Tomé and Príncipe | KK | S. intercalatum | 11 (332/3030) | - | Cross-sectional survey | 5–15 | 54 | 38 | 8 | 1991 | 1994 | [44] |
| Senegal | KK | S. mansoni | 80 (70/88) | - | Evaluation | 2–83 | 54.55 | 15.9 | 9.1 | 2006 | 2008 | [243] |
| Urine microscopy | S. haematobium | 72 (63/88) | - | 50 | - | 21.6 | ||||||
| qPCR | S. mansoni | 73 (64/88) | - | - | - | - | ||||||
| qPCR | S. haematobium | 55 (48/88) | - | - | - | - | ||||||
| South Africa | Urine microscopy | S. haematobium | 19.8 (78/394) | - | Prevalence | 16–23 | - | - | - | 2010–2012 | 2020 | [223] |
| qPCR | 23.1 (91/394) | - | - | - | - | |||||||
| Urine microscopy | S. haematobium | 1.0 (11/1143) | - | Cross-sectional survey | 1–5 | - | - | - | 2018 | 2019 | [244] | |
| KK | S. mansoni | 0.9 (9/998) | - | - | - | - | ||||||
| Urine microscopy | S. haematobium | 40.2 (169/380) | - | Prevalence | 10–15 | 61 | - | - | 2014 | 2018 | [245] | |
| Urine microscopy | S. haematobium | 31.8% (225/708) | - | Cross-sectional survey | 10–12 | - | - | 26.7 | 2009–2010 | 2014 | [246] | |
| qPCR | S. haematobium | 25.4 (180/708) | - | - | - | - | ||||||
| Urine microscopy | S. haematobium | 37.5 (120/320) | - | Prevalence | 10–15 | - | - | - | 2015 | 2017 | [247] | |
| Sudan | KK | S. mansoni | 36 (1020/2832) | - | Cross-sectional | 10–24 | - | - | - | - | 1993 | [248] |
| Urine microscopy | S. haematobium | 38.9 (58/149) | - | Comparative | 5- >20 | - | - | 2 | 2011–2013 | 2018 | [249] | |
| ELISA | S. haematobium | 81.2 (119/149) | - | - | - | - | ||||||
| Swaziland | Urine microscopy | S. haematobium | 5.3 (21/395) | - | Prevalence | 6–12 | - | - | - | 2010 | 2011 | [250] |
| Urine microscopy | S. haematobium | 6.1 (18/295) | - | <5- >19 | - | - | - | - | 2010 | [251] | ||
| Tanzania | KK | S. mansoni | 85.2 (253/297) | 89.7/72.8 | Cross-sectional survey | 7–16 | 30.6 | 39.1 | 15.5 | 2015 | 2018 | [252] |
| qPCR | 92.9 (276/297) | 98.7/81.2 | - | - | - | |||||||
| POC_CCA | 94.9 (282/297) | 99.5/63.4 | - | - | - | |||||||
| KK | S. mansoni | 68.9 (641/930) | - | Cross-sectional survey | 1–95 | 55.2 | 20.4 | 12.9 | 2016 | 2019 | [253] | |
| POC_CCA | S. mansoni | 94.5 (878/929) | - | - | - | - | ||||||
| KK | S. mansoni | 90.6 (752/830) | - | Cross-sectional survey | 5–19 | 24.1 | 38.4 | 28.1 | 2017 | 2020 | [254] | |
| KK | S. mansoni | 15.1 (898/5952) | - | Cross-sectional survey | 7–16 | - | - | - | - | 2015 | [255] | |
| Urine microscopy | S. haematobium | 8.9 (519/5952) | - | - | - | - | - | |||||
| KK | S. mansoni | 84.01 (431/513) | - | Cross-sectional survey | 6–16 | 34.11 | 39.91 | 25.99 | - | 2016 | [256] | |
| Urine microscopy | S. haematobium | 11.6 (13/112) | - | Prevalence | - | - | - | 2009–2010 | 2020 | [223] | ||
| qPCR | S. haematobium | 19.6 (22/112) | - | - | - | - | - | |||||
| KK | S. mansoni | 1.3 (4/310) | - | - | - | - | - | |||||
| Uganda | Urine-CCA Dipstick | S. mansoni | 56.7 (146/258) | 99.1/89.3 | Surveillance | 5–10 | - | - | - | - | 2018 | [257] |
| SEA ELISA | S. mansoni | 75.1 (193/258) | 97.7/49.5 | - | - | - | - | |||||
| KK | S. mansoni | 39.3 (1203/3058) | - | Prevalence | 1–5 | 60.7 | 21.8 | 17.5 | 2012–2013 | 2015 | [258] | |
| KK | S. mansoni | 40.8 (1850/4534) | - | Prevalence | 10–14 | - | - | - | 2009–2010 | 2011 | [259] | |
| KK | S. mansoni | 27.2 (352/1295) | - | Prevalence | 0.4–6.5 | 18.7 | 6 | 2.5 | 2009 | 2010 | [260] | |
| ELISA | S. mansoni | 66 (38/58) | - | - | - | - | ||||||
| KK | S. mansoni | 47.6 (342/719) | - | 15–70 | 29.2 | 12.7 | 5.7 | |||||
| ELISA | S. mansoni | 41.0 (34/83) | - | - | - | - | ||||||
| Urine microscopy | S. haematobium | 2.51 (24/955) | - | 5–17 | - | - | - | 2007–2011 | 2018 | [261] | ||
| Zambia | Urine microscopy | S. haematobium | 61 (90/147) | - | Evaluation | 7–14 | 26 | - | 19 | - | 2020 | [262] |
| KK | S. mansoni | 0.01 (2/147) | - | - | - | - | ||||||
| DDIA | S. haematobium | 51 (75/146) | 60/61 | - | - | - | ||||||
| IHA | 56 (82/146) | 74/72 | - | - | - | |||||||
| Urine microscopy | S. haematobium | 20.7 (328/1583) | - | Prevalence | 5–17 | - | - | - | 2007 | 2010 | [263] | |
| Urine microscopy | S. haematobium | 28.6 (279/975) | - | Prevalence | 9–16 | 84.9 | - | 15.1 | (2007–2015) | 2018 | [264] | |
| Urine microscopy | S. haematobium | 31.5 (494/1570) | - | Prevalence | 9–15 | 75.5 | - | 24.3 | 2011–2015 | |||
| KK | S. mansoni | 42.4 (304/719) | - | Cross-sectional survey | 7–50 | 61.2 | 26 | 12.8 | - | 2014 | [265] | |
| Zimbabwe | KK | S. mansoni | 11.0 (10/91) | - | Comparative | 1–12 | 2.1 | 8.8 | - | 2012 | 2014 | [266] |
| Urine microscopy | S. haematobium | 52.8 (48/91) | - | 41.8 | - | 11 | ||||||
| SmCTF-RDT | Schistosoma spp | 83.5 (76/91) | - | - | - | - | ||||||
| Urine microscopy | S. haematobium | 18.0 (2347/13037) | - | Cross-sectional survey | 10–15 | 12.4 | - | 5.6 | 2010–2011 | 2014 | [267] | |
| KK | S. mansoni | 7.2 (882/12249) | - | 3.6 | 1.4 | 0.3 | ||||||
| Urine microscopy | S. haematobium | 18.7 (61/325) | - | Cross-sectional survey | 17–49 | 93.4 | - | 6.6 | 2016–2017 | 2019 | [268] | |
| Urine microscopy | S. haematobium | 13.3 (71/535) | - | <5 | 93 | - | 7 | |||||
3.2. Stigmatisation Associated with Schistosomiasis, Particularly in Women Is still a Crucial Issue in Africa
3.3. Hybrid Schistosomes
3.4. Control Measures in addition to MDA Utilised in Africa
3.4.1. Mapping Studies and Snail Control
3.4.2. Education and Knowledge
4. Factors That Determine the Distribution of Schistosomiasis in Africa
4.1. Climate Change
4.2. Artificial (Man-Made) Activities
4.3. Human Migration
5. COVID-19
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Schistosomiasis. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/schistosomiasis (accessed on 1 March 2019).
- van der Werf, M.J.; de Vlas, S.J.; Brooker, S.; Looman, C.W.; Nagelkerke, N.J.; Habbema, J.D.; Engels, D. Quantification of clinical morbidity associated with schistosome infection in sub-Saharan Africa. Acta Trop. 2003, 86, 125–139. [Google Scholar] [CrossRef]
- McManus, D.P.; Dunne, D.W.; Sacko, M.; Utzinger, J.; Vennervald, B.J.; Zhou, X.N. Schistosomiasis. Nat. Rev. Dis. Primers 2018, 4, 13. [Google Scholar] [CrossRef] [PubMed]
- Gryseels, B.; Polman, K.; Clerinx, J.; Kestens, L. Human schistosomiasis. Lancet 2006, 368, 1106–1118. [Google Scholar] [CrossRef]
- Boissier, J.; Grech-Angelini, S.; Webster, B.L.; Allienne, J.F.; Huyse, T.; Mas-Coma, S.; Toulza, E.; Barre-Cardi, H.; Rollinson, D.; Kincaid-Smith, J.; et al. Outbreak of urogenital schistosomiasis in Corsica (France): An epidemiological case study. Lancet Infect. Dis. 2016, 16, 971–979. [Google Scholar] [CrossRef]
- Boissier, J.; Mone, H.; Mitta, G.; Bargues, M.D.; Molyneux, D.; Mas-Coma, S. Schistosomiasis reaches Europe. Lancet Infect. Dis. 2015, 15, 757–758. [Google Scholar] [CrossRef]
- Stothard, J.R.; Sekeleghe, A.K.; Mohammad, H.A.-H.; Janelisa, M.; Bonnie, L.W. Future schistosome hybridizations: Will all Schistosoma haematobium hybrids please stand-up. PLoS Negl. Trop. Dis. 2020, 14, e0008201. [Google Scholar] [CrossRef]
- Webster, B.L.; Diaw, O.T.; Seye, M.M.; Webster, J.P.; Rollinson, D. Introgressive hybridization of Schistosoma haematobium group species in Senegal: Species barrier break down between ruminant and human schistosomes. PLoS Negl. Trop. Dis. 2013, 7, e2110. [Google Scholar] [CrossRef] [Green Version]
- Webster, B.L. On the Interactions of Schistosoma Haematobium, S. Guineensis and Their Hybrids in the Laboratory and in the Field; University College London: London, UK, 2003. [Google Scholar]
- Kabatereine, N.B.; Vennervald, B.J.; Ouma, J.H.; Kemijumbi, J.; Butterworth, A.E.; Dunne, D.W.; Fulford, A.J. Adult resistance to schistosomiasis mansoni: Age-dependence of reinfection remains constant in communities with diverse exposure patterns. Parasitology 1999, 118, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Steinmann, P.; Keiser, J.; Bos, R.; Tanner, M.; Utzinger, J. Schistosomiasis and water resources development: Systematic review, meta-analysis, and estimates of people at risk. Lancet Infect. Dis. 2006, 6, 411–425. [Google Scholar] [CrossRef]
- De Bont, J.; Vercruysse, J. Schistosomiasis in Cattle. Adv. Parasitol. 1998, 41, 285–364. [Google Scholar] [CrossRef]
- Charlier, J.; van der Voort, M.; Kenyon, F.; Skuce, P.; Vercruysse, J. Chasing helminths and their economic impact on farmed ruminants. Trends Parasitol. 2014, 30, 361–367. [Google Scholar] [CrossRef]
- You, H.; Cai, P.; Tebeje, B.M.; Li, Y.; McManus, D.P. Schistosome Vaccines for Domestic Animals. Trop. Med. Infect. Dis. 2018, 3, 68. [Google Scholar] [CrossRef] [Green Version]
- Vercruysse, J. Schistosomiasis. Available online: https://www.msdvetmanual.com/circulatory-system/blood-parasites/schistosomiasis (accessed on 26 May 2021).
- Hotez, P.J.; Fenwick, A.; Savioli, L.; Molyneux, D.H. Rescuing the bottom billion through control of neglected tropical diseases. Lancet 2009, 373, 1570–1575. [Google Scholar] [CrossRef]
- Hotez, P.J.; Fenwick, A. Schistosomiasis in Africa: An emerging tragedy in our new global health decade. PLoS Negl. Trop. Dis. 2009, 3, e485. [Google Scholar] [CrossRef]
- Lothe, A.; Zulu, N.; Øyhus, A.O.; Kjetland, E.F.; Taylor, M. Treating schistosomiasis among South African high school pupils in an endemic area, a qualitative study. BMC Infect. Dis. 2018, 18, 239. [Google Scholar] [CrossRef] [Green Version]
- Tuhebwe, D.; Bagonza, J.; Kiracho, E.E.; Yeka, A.; Elliott, A.M.; Nuwaha, F. Uptake of mass drug administration programme for schistosomiasis control in Koome Islands, Central Uganda. PLoS ONE 2015, 10, e0123673. [Google Scholar] [CrossRef] [Green Version]
- Akogun, O.B. Urinary schistosomiasis and the coming of age in Nigeria. Parasitol. Today 1991, 7, 62. [Google Scholar] [CrossRef]
- Boko, P.M.; Ibikounle, M.; Onzo-Aboki, A.; Tougoue, J.-J.; Sissinto, Y.; Batcho, W.; Kinde-Gazard, D.; Kabore, A. Schistosomiasis and soil transmitted helminths distribution in Benin: A baseline prevalence survey in 30 districts. PLoS ONE 2016, 11, e0162798. [Google Scholar] [CrossRef] [PubMed]
- WHO. Ending the Neglect to Attain the Sustainable Development Goals—A Road Map for Neglected Tropical Diseases 2021–2030; World Health Organization: Geneva, Swizterland, 2020. [Google Scholar]
- WHO. Accelerating Work to Overcome the Global Impact of Neglected Tropical Diseases: A Roadmap for Implementation. 2012. Available online: https://apps.who.int/iris/handle/10665/70809 (accessed on 7 March 2019).
- Kajihara, N.; Hirayama, K. The War against a Regional Disease in Japan A History of the Eradication of Schistosomiasis japonica. Trop. Med. Health 2011, 39 (Suppl. S1), 3–44. [Google Scholar]
- Hotez, P.J.; Kamath, A. Neglected tropical diseases in sub-saharan Africa: Review of their prevalence, distribution, and disease burden. PLoS Negl. Trop. Dis. 2009, 3, e412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergquist, R.; Zhou, X.-N.; Rollinson, D.; Reinhard-Rupp, J.; Klohe, K. Elimination of schistosomiasis: The tools required. Infect. Dis. Poverty 2017, 6, 158. [Google Scholar] [CrossRef] [Green Version]
- Tchuem Tchuenté, L.-A.; Rollinson, D.; Stothard, J.; Molyneux, D. Moving from control to elimination of schistosomiasis in sub-Saharan Africa: Time to change and adapt strategies. Infect. Dis. Poverty 2017, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Butterworth, A.E. Human immunity to schistosomes: Some questions. Parasitol. Today 1994, 10, 378–380. [Google Scholar] [CrossRef]
- Butterworth, A.E.; Curry, A.J.; Dunne, D.W.; Fulford, A.J.; Kimani, G.; Kariuki, H.C.; Klumpp, R.; Koech, D.; Mbugua, G.; Ouma, J.H.; et al. Immunity and morbidity in human schistosomiasis mansoni. Trop. Geogr. Med. 1994, 46, 197–208. [Google Scholar]
- Colley, D.G.; Bustinduy, A.L.; Secor, W.E.; King, C.H. Human schistosomiasis. Lancet 2014, 383, 2253–2264. [Google Scholar] [CrossRef]
- Chabasse, D.; Bertrand, G.; Leroux, J.P.; Gauthey, N.; Hocquet, P. Developmental bilharziasis caused by Schistosoma mansoni discovered 37 years after infestation. Bull. Soc. Pathol. Exot. Fil. 1985, 78, 643–647. [Google Scholar]
- McCullough, F.S.; Gayral, P.; Duncan, J.; Christie, J.D. Molluscicides in schistosomiasis control. Bull. World Health Organ. 1980, 58, 681–689. [Google Scholar]
- WHO. Field Use of Molluscicides in Schistosomiasis Control Programmes: An Operational Manual for Programme Managers; WHO: Geneva, Swizterland, 2017. [Google Scholar]
- Ekabo, O.A.; Farnsworth, N.R.; Henderson, T.O.; Mao, G.; Mukherjee, R. Antifungal and molluscicidal saponins from Serjania salzmanniana. J. Nat. Prod. 1996, 59, 431–435. [Google Scholar] [CrossRef]
- Rocha-Filho, C.A.; Albuquerque, L.P.; Silva, L.R.; Silva, P.C.; Coelho, L.C.; Navarro, D.M.; Albuquerque, M.C.; Melo, A.M.; Napoleão, T.H.; Pontual, E.V.; et al. Assessment aof toxicity of Moringa oleifera flower extract to Biomphalaria glabrata, Schistosoma mansoni and Artemia salina. Chemosphere 2015, 132, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Gray, D.; Ross, A.; Li, Y.-S.; McManus, D. Diagnosis and management of schistosomiasis. Br. Med. J. 2011, 342, 1138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, A.G.; Vickers, D.; Olds, G.R.; Shah, S.M.; McManus, D.P. Katayama syndrome. Lancet Infect. Dis. 2007, 7, 218–224. [Google Scholar] [CrossRef]
- Ross, A.G.P.; Bartley, P.B.; Sleigh, A.C.; Olds, G.R.; Li, Y.; Williams, G.M.; McManus, D.P. Schistosomiasis. N. Engl. J. Med. 2002, 346, 1212–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, A.G.; McManus, D.P.; Farrar, J.; Hunstman, R.J.; Gray, D.J.; Li, Y.S. Neuroschistosomiasis. J. Neurol. 2012, 259, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Gunn, A.; Pitt, S.J. Parasitology an Integrated Approach; John Wiley & Sons: Chichester, UK, 2012. [Google Scholar]
- Wynn, T.A.; Thompson, R.W.; Cheever, A.W.; Mentink-Kane, M.M. Immunopathogenesis of schistosomiasis. Immunol Rev. 2004, 201, 156–167. [Google Scholar] [CrossRef]
- Burke, M.L.; Jones, M.K.; Gobert, G.N.; Li, Y.S.; Ellis, M.K.; McManus, D.P. Immunopathogenesis of human schistosomiasis. Parasite Immunol. 2009, 31, 163–176. [Google Scholar] [CrossRef]
- Costain, A.H.; MacDonald, A.S.; Smits, H.H. Schistosome egg migration: Mechanisms, pathogenesis and host immune responses. Front. Immunol. 2018, 9, 3042. [Google Scholar] [CrossRef] [Green Version]
- Almeda, J.; Corachan, M.; Sousa, A.; Ascaso, C.; Carvalho, J.M.; Rollinson, D.; Southgate, V.R. Schistosomiasis in the Republic of São Tomé and Principe: Human studies. Trans. R. Soc. Trop. Med. Hyg. 1994, 88, 406–409. [Google Scholar] [CrossRef]
- Poggensee, G.; Feldmeier, H.; Krantz, I. Schistosomiasis of the female genital tract: Public health aspects. Parasitol. Today 1999, 15, 378–381. [Google Scholar] [CrossRef]
- Christinet, V.; Lazdins-Helds, J.K.; Stothard, J.R.; Reinhard-Rupp, J. Female genital schistosomiasis (FGS): From case reports to a call for concerted action against this neglected gynaecological disease. Int. J. Parasitol. 2016, 46, 395–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nour, N.M. Schistosomiasis: Health effects on women. Rev. Obstet. Gynecol. 2010, 3, 28–32. [Google Scholar] [PubMed]
- Friedman, J.F.; Mital, P.; Kanzaria, H.K.; Olds, G.R.; Kurtis, J.D. Schistosomiasis and pregnancy. Trends Parasitol. 2007, 23, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Helling-Giese, G.; Kjetland, E.F.; Gundersen, S.G.; Poggensee, G.; Richter, J.; Krantz, I.; Feldmeier, H. Schistosomiasis in women: Manifestations in the upper reproductive tract. Acta Trop. 1996, 62, 225–238. [Google Scholar] [CrossRef]
- Ajanga, A.; Lwambo, N.J.; Blair, L.; Nyandindi, U.; Fenwick, A.; Brooker, S. Schistosoma mansoni in pregnancy and associations with anaemia in Northwest Tanzania. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 59–63. [Google Scholar] [CrossRef]
- Ben-Chetrit, E.; Lachish, T.; Mørch, K.; Atias, D.; Maguire, C.; Schwartz, E. Schistosomiasis in pregnant travelers: A case series. J. Travel Med. 2015, 22, 94–98. [Google Scholar] [CrossRef] [Green Version]
- Downs, J.A.; Dupnik, K.M.; van Dam, G.J.; Urassa, M.; Lutonja, P.; Kornelis, D.; de Dood, C.J.; Hoekstra, P.; Kanjala, C.; Isingo, R.; et al. Effects of schistosomiasis on susceptibility to HIV-1 infection and HIV-1 viral load at HIV-1 seroconversion: A nested case-control study. PLoS Negl. Trop. Dis. 2017, 11, e0005968. [Google Scholar] [CrossRef] [PubMed]
- Kjetland, E.F.; Leutscher, P.D.C.; Ndhlovu, P.D. A review of female genital schistosomiasis. Trends Parasitol. 2012, 28, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Kjetland, E.F.; Ndhlovu, P.D.; Gomo, E.; Mduluza, T.; Midzi, N.; Gwanzura, L.; Mason, P.R.; Sandvik, L.; Friis, H.; Gundersen, S.G. Association between genital schistosomiasis and HIV in rural Zimbabwean women. Aids 2006, 20, 593–600. [Google Scholar] [CrossRef] [Green Version]
- Olusegun, A.F.; Ehis, O.C.; Richard, O. Proportion of urinary schistosomiasis among HIV-infected subjects in Benin City, Nigeria. Oman Med. J. 2011, 26, 175–177. [Google Scholar] [CrossRef]
- Downs, J.A.; Mguta, C.; Kaatano, G.M.; Mitchell, K.B.; Bang, H.; Simplice, H.; Kalluvya, S.E.; Changalucha, J.M.; Johnson, W.D., Jr.; Fitzgerald, D.W. Urogenital schistosomiasis in women of reproductive age in Tanzania’s Lake Victoria region. Am. J. Trop. Med. Hyg. 2011, 84, 364–369. [Google Scholar] [CrossRef] [Green Version]
- Feldmeier, H.; Krantz, I.; Poggensee, G. Female genital schistosomiasis as a risk-factor for the transmission of HIV. Int. J. STD AIDS 1994, 5, 368–372. [Google Scholar] [CrossRef]
- Ndhlovu, P.D.; Mduluza, T.; Kjetland, E.F.; Midzi, N.; Nyanga, L.; Gundersen, S.G.; Friis, H.; Gomo, E. Prevalence of urinary schistosomiasis and HIV in females living in a rural community of Zimbabwe: Does age matter? Trans. R. Soc. Trop Med. Hyg. 2007, 101, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Leutscher, P.; Ramarokoto, C.E.; Reimert, C.; Feldmeier, H.; Esterre, P.; Vennervald, B.J. Community-based study of genital schistosomiasis in men from Madagascar. Lancet 2000, 355, 117–118. [Google Scholar] [CrossRef]
- Wall, K.M.; Kilembe, W.; Vwalika, B.; Dinh, C.; Livingston, P.; Lee, Y.M.; Lakhi, S.; Boeras, D.; Naw, H.K.; Brill, I.; et al. Schistosomiasis is associated with incident HIV transmission and death in Zambia. PLoS Negl. Trop. Dis. 2018, 12, e0006902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mbabazi, P.S.; Andan, O.; Fitzgerald, D.W.; Chitsulo, L.; Engels, D.; Downs, J.A. Examining the relationship between urogenital schistosomiasis and HIV infection. PLoS Negl. Trop. Dis. 2011, 5, e1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kjetland, E.F.; Hegertun, I.E.; Baay, M.F.; Onsrud, M.; Ndhlovu, P.D.; Taylor, M. Genital schistosomiasis and its unacknowledged role on HIV transmission in the STD intervention studies. Int. J. STD AIDS 2014, 25, 705–715. [Google Scholar] [CrossRef] [PubMed]
- Zegers-Hochschild, F.; Adamson, G.D.; de Mouzon, J.; Ishihara, O.; Mansour, R.; Nygren, K.; Sullivan, E.; Vanderpoel, S. International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) revised glossary of ART terminology, 2009. Fertil. Steril. 2009, 92, 1520–1524. [Google Scholar] [CrossRef]
- Bentefouet, T.L.; Thiam, M.; Gaye, A.M.; El Wardi, A.; Gueye, L.; Cisse, M.L. Case report of tubo-ovarian Bilharziasis presented with pelvic pain and secondary infertility. Case Rep. Images Obstet. Gynecol. 2017, 3, 19–22. [Google Scholar] [CrossRef]
- Ogunniyi, S.O.; Nganwuchu, A.M.; Adenle, M.A.; Dare, F.O. Pregnancy following infertility due to pelvic schistosomiasis—A case report. West. Afr. J. Med. 1994, 13, 132–133. [Google Scholar]
- Aminu, M.B.; Abdullahi, K.; Dattijo, L.M. Tubal ectopic gestation associated with genital schistosomiasis: A case report. Afr. J. Reprod. Health La Rev. Afr. de la St. Reprod. 2014, 18, 144–146. [Google Scholar]
- Okonofua, F.E.; Ojo, O.S.; Odunsi, O.A.; Odesanmi, W.O. Ectopic pregnancy associated with tubal schistosomiasis in a Nigerian woman. Int. J. Gynaecol. Obstet. 1990, 32, 281–284. [Google Scholar] [CrossRef]
- Woodall, P.A.; Kramer, M.R. Schistosomiasis and infertility in East Africa. Am. J. Trop. Med. Hyg. 2018, 98, 1137–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kini, S.; Dayoub, N.; Raja, A.; Pickering, S.; Thong, J. Schistosomiasis-induced male infertility. BMJ Case Rep. 2009, 2009. [Google Scholar] [CrossRef] [Green Version]
- Adisa, J.; Egbujo, E.M.; Yahaya, B.A.; Echejoh, G. Primary infertility associated with Schistosoma mansoni: A case report from the Jos plateau, North-Central Nigeria. Afr. Health Sci. 2012, 12, 563–565. [Google Scholar] [PubMed] [Green Version]
- Madden, F. Two rare manifestations of bilharziosis. Lancet 1911, 178, 754–755. [Google Scholar] [CrossRef]
- Leutscher, P.D.; Ramarokoto, C.E.; Hoffmann, S.; Jensen, J.S.; Ramaniraka, V.; Randrianasolo, B.; Raharisolo, C.; Migliani, R.; Christensen, N. Coexistence of urogenital schistosomiasis and sexually transmitted infection in women and men living in an area where Schistosoma haematobium is endemic. Clin. Infect. Dis. 2008, 47, 775–782. [Google Scholar] [CrossRef] [Green Version]
- Kayuni, S.; Lampiao, F.; Makaula, P.; Juziwelo, L.; Lacourse, E.J.; Reinhard-Rupp, J.; Leutscher, P.D.C.; Stothard, J.R. A systematic review with epidemiological update of male genital schistosomiasis (MGS): A call for integrated case management across the health system in sub-Saharan Africa. Parasite Epidemiol. Control. 2018, 4, e00077. [Google Scholar] [CrossRef]
- Gelfand, M.; Ross, C.M.; Blair, D.M.; Castle, W.M.; Weber, M.C. Schistosomiasis of the male pelvic organs. Severity of infection as determined by digestion of tissue and histologic methods in 300 cadavers. Am. J. Trop. Med. Hyg. 1970, 19, 779–784. [Google Scholar] [CrossRef] [PubMed]
- Vilana, R.; Corachan, M.; Gascon, J.; Valls, E.; Bru, C. Schistosomiasis of the male genital tract: Transrectal sonographic findings. J. Urol. 1997, 158, 1491–1493. [Google Scholar] [CrossRef]
- Kayuni, S.A.; Lacourse, E.J.; Makaula, P.; Lampiao, F.; Juziwelo, L.; Fawcett, J.; Shaw, A.; Alharbi, M.H.; Verweij, J.J.; Stothard, J.R. Case report: Highlighting male genital schistosomiasis (MGS) in fishermen from the southwestern shoreline of Lake Malawi, Mangochi District. Am. J. Trop. Med. Hyg. 2019, 101, 1331. [Google Scholar] [CrossRef]
- Abol-Enein, H. Infection: Is it a cause of bladder cancer? Scand. J. Urol. Nephrol. Suppl. 2008, 79–84. [Google Scholar] [CrossRef]
- Heyns, C.F.; van der Merwe, A. Bladder cancer in Africa. Can. J. Urol. 2008, 15, 3899–3908. [Google Scholar] [PubMed]
- Shiff, C.; Veltri, R.; Naples, J.; Quartey, J.; Otchere, J.; Anyan, W.; Marlow, C.; Wiredu, E.; Adjei, A.; Brakohiapa, E.; et al. Ultrasound verification of bladder damage is associated with known biomarkers of bladder cancer in adults chronically infected with Schistosoma haematobium in Ghana. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 847–854. [Google Scholar] [CrossRef]
- Michaud, D.S. Chronic inflammation and bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2007, 25, 260–268. [Google Scholar] [CrossRef]
- El-Bolkainy, M.N.; Mokhtar, N.M.; Ghoneim, M.A.; Hussein, M.H. The impact of schistosomiasis on the pathology of bladder carcinoma. Cancer 1981, 48, 2643–2648. [Google Scholar] [CrossRef]
- Kitinya, J.N.; Laurèn, P.A.; Eshleman, L.J.; Paljärvi, L.; Tanaka, K. The incidence of squamous and transitional cell carcinomas of the urinary bladder in northern Tanzania in areas of high and low levels of endemic Schistosoma haematobium infection. Trans. R. Soc. Trop. Med. Hyg. 1986, 80, 935–939. [Google Scholar] [CrossRef]
- Botelho, M.C.; Figueiredo, J.; Alves, H. Bladder cancer and urinary schistosomiasis in Angola. J. Nephrol. Res. 2015, 1, 22–24. [Google Scholar] [CrossRef] [Green Version]
- Gouda, I.; Mokhtar, N.; Bilal, D.; El-Bolkainy, T.; El-Bolkainy, N.M. Bilharziasis and bladder cancer: A time trend analysis of 9843 patients. J. Egypt. Natl. Cancer Inst. 2007, 19, 158–162. [Google Scholar]
- Botelho, M.C.; Machado, J.; Da Costa, J. Schistosoma haematobium total antigen induces increased proliferation, migration and invasion, and decreases apoptosis of normal epithelial cells. Virulence 2010, 1, 84–87. [Google Scholar] [CrossRef] [Green Version]
- Vennervald, B.J.; Polman, K. Helminths and malignancy. Parasite Immunol. 2009, 31, 686–696. [Google Scholar] [CrossRef] [PubMed]
- Botelho, M.; Oliveira, P.; Gomes, J.; Gartner, F.; Lopes, C.; da Costa, J.M.C.; Machado, J.C. Tumourigenic effect of Schistosoma haematobium total antigen in mammalian cells. Int. J. Exp. Pathol. 2009, 90, 448–453. [Google Scholar] [CrossRef]
- Doenhoff, M.J.; Cioli, D.; Utzinger, J. Praziquantel: Mechanisms of action, resistance and new derivatives for schistosomiasis. Curr. Opin. Infect. Dis. 2008, 21, 659–667. [Google Scholar] [CrossRef]
- Cioli, D.; Pica-Mattoccia, L. Praziquantel. Parasitol Res. 2003, 90 (Suppl. S1), S3–S9. [Google Scholar] [CrossRef]
- Utzinger, J.; Xiao, S.H.; Tanner, M.; Keiser, J. Artemisinins for schistosomiasis and beyond. Curr. Opin. Investig. Drugs 2007, 8, 105–116. [Google Scholar]
- Harries, A.D.; Cook, G.C. Acute schistosomiasis (Katayama fever): Clinical deterioration after chemotherapy. J. Infect. 1987, 14, 159–161. [Google Scholar] [CrossRef]
- WHO. Preventive Chemotherapy in Human Helminthiasis: Coordinated Use of Anthelminthic Drugs in Control Interventions: A Manual for Health Professionals and Programme Managers. Schistosomiasis, A Major Public Health Problem. 2015. Available online: http://www.who.int/schistosomiasis/en/. (accessed on 22 March 2019).
- WHO. Helminth Control in School Age Children A Guide for Control Managers Second Edition; World Heal Organisation: Geneva, Switzerland, 2011. [Google Scholar]
- WHO. Summary of global update on implementation of preventive chemotherapy against neglected tropical diseases in 2019/Resume des donnees mondiales actualisees sur la mise en oeuvre de la chimioprevention contre les maladies tropicales negligees en 2019. Wkly. Epidemiol. Rec. 2020, 95, 469. [Google Scholar]
- Cioli, D.; Pica-Mattoccia, L.; Basso, A.; Guidi, A. Schistosomiasis control: Praziquantel forever? Mol. Biochem. Parasitol. 2014, 195, 23–29. [Google Scholar] [CrossRef]
- Prüss-Üstün, A.; Bos, R.; Gore, F.; Bartram, J. Safer Water, Better Health: Costs, Benefits and Sustainability of Interventions to Protect and Promote Health; World Health Organization: Geneva, Swizterland, 2008; p. 60. [Google Scholar]
- WHO. Neglected Tropical Diseases, Hidden Successes, Emerging Opportunities; World Health Organization: Geneva, Swizterland; 52p.
- WHO. Regional Strategic Plan for Neglected Tropical Diseases in the African Region 2014–2020; World Health Organization Regional Office for Africa: Brazzaville, Cango, 2013. [Google Scholar]
- Campbell, S.J.; Savage, G.B.; Gray, D.J.; Atkinson, J.A.; Soares Magalhães, R.J.; Nery, S.V.; McCarthy, J.S.; Velleman, Y.; Wicken, J.H.; Traub, R.J.; et al. Water, Sanitation, and Hygiene (WASH): A critical component for sustainable soil-transmitted helminth and schistosomiasis control. PLoS Negl. Trop. Dis. 2014, 8, e2651. [Google Scholar] [CrossRef] [Green Version]
- Alsallaq, R.A.; Gurarie, D.; Ndeffo Mbah, M.; Galvani, A.; King, C. Quantitative assessment of the impact of partially protective anti-schistosomiasis vaccines. PLoS Negl. Trop. Dis. 2017, 11, e0005544. [Google Scholar] [CrossRef] [Green Version]
- Tebeje, B.M.; Harvie, M.; You, H.; Loukas, A.; McManus, D.P. Schistosomiasis vaccines: Where do we stand? Parasites Vectors 2016, 9, 528. [Google Scholar] [CrossRef] [Green Version]
- Mulero, S.; Rey, O.; Arancibia, N.; Mas-Coma, S.; Boissier, J. Persistent establishment of a tropical disease in Europe: The preadaptation of schistosomes to overwinter. Parasites Vectors 2019, 12, 379. [Google Scholar] [CrossRef]
- Dazo, B.C.; Biles, J.E. Two new field techniques for detection and counting of Schistosoma haematobium eggs in urine samples, with an evaluation of both methods. Bull. World Health Organ. 1974, 51, 399–408. [Google Scholar]
- Teesdale, C.H.; Amin, M.A. A simple thick smear technique for the diagnosis of Schistosoma mansoni infection. Bull. World Health Organ. 1976, 54, 703–705. [Google Scholar]
- Lunde, M.N.; Ottesen, E.A. Enzyme-linked immunosorbent assay (ELISA) for detecting IgM and IgE antibodies in human schistosomiasis. Am. J. Trop Med. Hyg. 1980, 29, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Wen, L.Y.; Chen, J.H.; Ding, J.Z.; Zhang, J.F.; Lu, S.H.; Yu, L.L.; Shen, L.Y.; Wu, G.L.; Zhou, X.N.; Zheng, J. Evaluation on the applied value of the dot immunogold filtration assay (DIGFA) for rapid detection of anti-Schistosoma japonicum antibody. Acta Trop. 2005, 96, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Sarhan, R.M.; Aminou, H.A.; Saad, G.A.; Ahmed, O.A. Comparative analysis of the diagnostic performance of adult, cercarial and egg antigens assessed by ELISA, in the diagnosis of chronic human Schistosoma mansoni infection. Parasitol Res. 2014, 113, 3467–3476. [Google Scholar] [CrossRef]
- Corstjens, P.L.; De Dood, C.J.; Kornelis, D.; Fat, E.M.; Wilson, R.A.; Kariuki, T.M.; Nyakundi, R.K.; Loverde, P.T.; Abrams, W.R.; Tanke, H.J.; et al. Tools for diagnosis, monitoring and screening of Schistosoma infections utilizing lateral-flow based assays and upconverting phosphor labels. Parasitology 2014, 141, 1841–1855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coulibaly, J.T.; Knopp, S.; N’Guessan, N.A.; Silué, K.D.; Fürst, T.; Lohourignon, L.K.; Brou, J.K.; N’Gbesso, Y.K.; Vounatsou, P.; N’Goran, E.K.; et al. Accuracy of Urine Circulating Cathodic Antigen (CCA) Test for Schistosoma mansoni Diagnosis in Different Settings of Côte d’Ivoire. PLoS Negl. Trop. Dis. 2011, 5, e1384. [Google Scholar] [CrossRef] [Green Version]
- Tchuem Tchuenté, L.-A.; Kueté Fouodo, C.J.; Kamwa Ngassam, R.I.; Sumo, L.; Dongmo Noumedem, C.; Kenfack, C.M.; Gipwe, N.F.; Nana, E.D.; Stothard, J.R.; Rollinson, D. Evaluation of Circulating Cathodic Antigen (CCA) Urine-Tests for Diagnosis of Schistosoma mansoni Infection in Cameroon. PLoS Negl. Trop. Dis. 2012, 6, e1758. [Google Scholar] [CrossRef]
- Abdel-Fattah, M.; Al-Sherbiny, M.; Osman, A.; Charmy, R.; Tsang, V. Improving the detection limit of quantitative diagnosis of anti-S. haematobium antibodies using Falcon Assay Screening Test (FAST) ELISA by developing a new standard curve. Parasitol. Res. 2011, 108, 1457–1463. [Google Scholar] [CrossRef] [PubMed]
- Gobert, G.N.; Chai, M.; Duke, M.; McManus, D.P. Copro-PCR based detection of Schistosoma eggs using mitochondrial DNA markers. Mol. Cell. Probes 2005, 19, 250–254. [Google Scholar] [CrossRef]
- Lier, T.; Simonsen, T.; Haaheim, T.; Hjelmevoll, T.; Vennervald, T.; Johansen, T. Novel real-time PCR for detection of Schistosoma japonicum in stool. Southeast Asian J. Trop. Med. Public Health 2006, 37, 257–264. [Google Scholar]
- Pontes, L.; Dias-Neto, E.; Rabello, A. Detection by polymerase chain reaction of Schistosoma mansoni DNA in human serum and feces. Am. J. Trop. Med. Hyg. 2002, 66, 157–162. [Google Scholar] [CrossRef]
- Sandoval, N.; Siles-Lucas, M.; Aban, J.L.; Pérez-Arellano, J.L.; Gárate, T.; Muro, A. Schistosoma mansoni: A diagnostic approach to detect acute schistosomiasis infection in a murine model by PCR. Exp. Parasitol. 2006, 114, 84–88. [Google Scholar] [CrossRef]
- Sandoval, N.; Siles-Lucas, M.; Pérez-Arellano, J.L.; Carranza, C.; Puente, S.; López-Abán, J.; Muro, A. A new PCR-based approach for the specific amplification of DNA from different Schistosoma species applicable to human urine samples. Parasitology 2006, 133, 581–587. [Google Scholar] [CrossRef]
- Suzuki, T.; Osada, Y.; Kumagai, T.; Hamada, A.; Okuzawa, E.; Kanazawa, T. Early detection of Schistosoma mansoni infection by touchdown PCR in a mouse model. Parasitol. Int. 2006, 55, 213–218. [Google Scholar] [CrossRef]
- Weerakoon, K.G.; Gordon, C.A.; Williams, G.M.; Cai, P.; Gobert, G.N.; Olveda, R.M.; Ross, A.G.; Olveda, D.U.; McManus, D.P. Droplet digital PCR diagnosis of human schistosomiasis: Parasite cell-free DNA detection in diverse clinical samples. J. Infect. Dis. 2017, 216, 1611–1622. [Google Scholar] [CrossRef]
- Weerakoon, K.G.; Gordon, C.A.; Cai, P.; Gobert, G.N.; Duke, M.; Williams, G.M.; McManus, D.P. A novel duplex ddPCR assay for the diagnosis of schistosomiasis japonica: Proof of concept in an experimental mouse model. Parasitology 2017, 144, 1005–1015. [Google Scholar] [CrossRef]
- Notomi, T.; Okayama, H.; Masubuchi, H.; Yonekawa, T.; Watanabe, K.; Amino, N.; Hase, T. Loop-mediated isothermal amplification of DNA. Nucleic Acids Res. 2000, 28, E63. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Guan, Z.-X.; Zhao, B.; Wang, Y.-Y.; Cao, Y.; Zhang, H.-Q.; Zhu, X.-Q.; He, Y.-K.; Xia, C.-M. DNA detection of Schistosoma japonicum: Diagnostic validity of a lamp assay for low-intensity infection and effects of chemotherapy in humans (diagnostic validity of lamp in humans). PLoS Negl. Trop. Dis. 2015, 9, e0003668. [Google Scholar] [CrossRef]
- Qin, Z.-Q.; Xu, J.; Feng, T.; Lv, S.; Qian, Y.-J.; Zhang, L.-J.; Li, Y.-L.; Lv, C.; Bergquist, R.; Li, S.-Z.; et al. Field Evaluation of a Loop-Mediated Isothermal Amplification (LAMP) Platform for the Detection of Schistosoma japonicum Infection in Oncomelania hupensis Snails. Trop. Med. Infect. Dis. 2018, 15, 124. [Google Scholar] [CrossRef] [Green Version]
- Mwangi, I.N.; Agola, E.L.; Mugambi, R.M.; Shiraho, E.A.; Mkoji, G.M. Development and evaluation of a loop-mediated isothermal amplification assay for diagnosis of Schistosoma mansoni infection in faecal samples. J. Parasitol. Res. 2018, 2018, 1267826. [Google Scholar] [CrossRef]
- Kumagai, T.; Furushima-Shimogawara, R.; Ohmae, H.; Wang, T.P.; Lu, S.; Chen, R.; Wen, L.; Ohta, N. Detection of early and single infections of Schistosoma japonicum in the intermediate host snail, Oncomelania hupensis, by PCR and loop-mediated isothermal amplification (LAMP) assay. Am. J. Trop. Med. Hyg. 2010, 83, 542–548. [Google Scholar] [CrossRef]
- Hamburger, J.; Abbasi, I.; Kariuki, C.; Wanjala, A.; Mzungu, E.; Mungai, P.; Muchiri, E.; King, C.H. Evaluation of loop-mediated isothermal amplification suitable for molecular monitoring of schistosome-infected snails in field laboratories. Am. J. Trop. Med. Hyg. 2013, 88, 344–351. [Google Scholar] [CrossRef]
- Gandasegui, J.; Fernández-Soto, P.; Muro, A.; Lopes de Melo, F.; Loyo, R.; de Souza Gomes, C. A field survey using LAMP assay for detection of Schistosoma mansoni in a low-transmission area of schistosomiasis in Umbuzeiro, Brazil: Assessment in human and snail samples. PLoS Negl. Trop. Dis. 2018, 12, e0006314. [Google Scholar] [CrossRef]
- Gandasegui, J.; Fernandez-Soto, P.; Hernandez-Goenaga, J.; Lopez-Aban, J.; Vicente, B.; Muro, A. Biompha-lamp: A new rapid loop-mediated isothermal amplification assay for detecting Schistosoma mansoni in Biomphalaria glabrata snail host. PLoS Negl. Trop. Dis. 2016, 10, e0005225. [Google Scholar] [CrossRef]
- Fernández-Soto, P.; Gandasegui Arahuetes, J.; Sánchez Hernández, A.; López Abán, J.; Vicente Santiago, B.; Muro, A. A Loop-Mediated Isothermal Amplification (LAMP) Assay for Early Detection of Schistosoma mansoni in Stool Samples: A Diagnostic Approach in a Murine Model (LAMP Assay for Early Detection of Schistosoma mansoni in Stool Samples). PLoS Negl. Trop. Dis. 2014, 8, e3126. [Google Scholar] [CrossRef] [Green Version]
- Abbasi, I.; King, C.H.; Muchiri, E.M.; Hamburger, J. Detection of Schistosoma mansoni and Schistosoma haematobium DNA by loop-mediated isothermal amplification: Identification of infected snails from early prepatency. Am. J. Trop. Med. Hyg. 2010, 83, 427–432. [Google Scholar] [CrossRef] [Green Version]
- Vincent, M.; Xu, Y.; Kong, H. Helicase-dependent isothermal DNA amplification. EMBO Rep. 2004, 5, 795–800. [Google Scholar] [CrossRef]
- Piepenburg, O.; Williams, C.H.; Stemple, D.L.; Armes, N.A. DNA detection using recombination proteins. PloS Biol. 2006, 4, 1115. [Google Scholar] [CrossRef]
- Compton, J. Nucleic acid sequence-based amplification. Nature 1991, 350, 91. [Google Scholar] [CrossRef]
- Xing, W.; Yu, X.; Feng, J.; Sun, K.; Fu, W.; Wang, Y.; Zou, M.; Xia, W.; Luo, Z.; He, H.; et al. Field evaluation of a recombinase polymerase amplification assay for the diagnosis of Schistosoma japonicum infection in Hunan province of China. BMC Infect. Dis. 2017, 17, 164. [Google Scholar] [CrossRef] [Green Version]
- Sun, K.; Xing, W.; Yu, X.; Fu, W.; Wang, Y.; Zou, M.; Luo, Z.; Xu, D. Recombinase polymerase amplification combined with a lateral flow dipstick for rapid and visual detection of Schistosoma japonicum. Parasit Vectors 2016, 9, 476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rostron, P.; Pennance, T.; Bakar, F.; Rollinson, D.; Knopp, S.; Allan, F.; Kabole, F.; Ali, S.M.; Ame, S.M.; Webster, B.L. Development of a recombinase polymerase amplification (RPA) fluorescence assay for the detection of Schistosoma haematobium. Parasites Vectors 2019, 12, 514. [Google Scholar] [CrossRef]
- Poulton, K.; Webster, B. Development of a lateral flow recombinase polymerase assay for the diagnosis of Schistosoma mansoni infections. Anal. Biochem. 2018, 546, 65–71. [Google Scholar] [CrossRef]
- Kato-Hayashi, N.; Yasuda, M.; Yuasa, J.; Isaka, S.; Haruki, K.; Ohmae, H.; Osada, Y.; Kanazawa, T.; Chigusa, Y. Use of cell-free circulating schistosome DNA in serum, urine, semen, and saliva to monitor a case of refractory imported schistosomiasis hematobia. J. Clin. Microbiol. 2013, 51, 3435–3438. [Google Scholar] [CrossRef] [Green Version]
- van Dam, G.J.; Wichers, J.H.; Ferreira, T.M.F.; Ghati, D.; van Amerongen, A.; Deelder, A.M. Diagnosis of schistosomiasis by reagent strip test for detection of circulating cathodic antigen. J. Clin. Microbiol. 2004, 42, 5458–5461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Dam, G.J.; de Dood, C.J.; Lewis, M.; Deelder, A.M.; van Lieshout, L.; Tanke, H.J.; van Rooyen, L.H.; Corstjens, P.L. A robust dry reagent lateral flow assay for diagnosis of active schistosomiasis by detection of Schistosoma circulating anodic antigen. Exp. Parasitol. 2013, 135, 274–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grenfell, R.F.; Martins, W.; Drummond, S.C.; Antunes, C.M.; Voieta, I.; Otoni, A.; Oliveira, A.A.; Silva-Moraes, V.; Oliveira, E.R.; Oliveira, E.; et al. Acute schistosomiasis diagnosis: A new tool for the diagnosis of schistosomiasis in a group of travelers recently infected in a new focus of Schistosoma mansoni. Rev. Soc. Bras. Med. Trop. 2013, 46, 208–213. [Google Scholar] [CrossRef] [Green Version]
- Marchese, V.; Beltrame, A.; Angheben, A.; Monteiro, G.B.; Giorli, G.; Perandin, F.; Buonfrate, D.; Bisoffi, Z. Schistosomiasis in immigrants, refugees and travellers in an Italian referral centre for tropical diseases. Infect. Dis. Poverty 2018, 7, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beltrame, A.; Zammarchi, L.; Zuglian, G.; Gobbi, F.; Angheben, A.; Marchese, V.; Degani, M.; Mantella, A.; Bianchi, L.; Montagnani, C.; et al. Schistosomiasis screening of travelers from Italy with possible exposure in Corsica, France. Emerg. Infect. Dis. 2015, 21, 1887–1889. [Google Scholar] [CrossRef] [Green Version]
- Tosswill, J.H.; Ridley, D.S. An evaluation of the ELISA for schistosomiasis in a hospital population. Trans. R. Soc. Trop. Med. Hyg. 1986, 80, 435–438. [Google Scholar] [CrossRef]
- Mott, K.E.; Dixon, H.; Osei-Tutu, E.; England, E.C. Relation between intensity of Schistosoma haematobium infection and clinical haematuria and proteinuria. Lancet 1983, 321, 1005–1008. [Google Scholar] [CrossRef]
- Ochodo, E.A.; Gopalakrishna, G.; Spek, B.; Reitsma, J.B.; van Lieshout, L.; Polman, K.; Lamberton, P.; Bossuyt, P.M.; Leeflang, M.M. Circulating antigen tests and urine reagent strips for diagnosis of active schistosomiasis in endemic areas. Cochrane Database Syst. Rev. 2015, 2015, Cd009579. [Google Scholar] [CrossRef] [Green Version]
- Adekiya, T.A.; Aruleba, R.T.; Oyinloye, B.E.; Okosun, K.O.; Kappo, A.P. The effect of climate change and the snail-schistosome cycle in transmission and bio-control of schistosomiasis in sub-Saharan Africa. Int. J. Environ. Research Public Health 2019, 17, 181. [Google Scholar] [CrossRef] [Green Version]
- Rollinson, D.; Knopp, S.; Levitz, S.; Stothard, J.R.; Tchuem Tchuenté, L.-A.; Garba, A.; Mohammed, K.A.; Schur, N.; Person, B.; Colley, D.G.; et al. Time to set the agenda for schistosomiasis elimination. Acta Trop. 2013, 128, 423–440. [Google Scholar] [CrossRef]
- McManus, D.P.; Gordon, C.; Weerakoon, K.G.A.D. Testing of water samples for environmental DNA as a surveillance tool to assess the risk of schistosome infection in a locality. Int. J. Infect. Dis. 2018, 76, 128–129. [Google Scholar] [CrossRef] [Green Version]
- Allan, F.; Ame, S.M.; Tian-Bi, Y.-N.T.; Hofkin, B.V.; Webster, B.L.; Diakité, N.R.; N’Goran, E.K.; Kabole, F.; Khamis, I.S.; Gouvras, A.N.; et al. Snail-related contributions from the schistosomiasis consortium for operational research and evaluation program including xenomonitoring, focal mollusciciding, biological control, and modeling. Am. Soc. Trop. Med. Hyg. 2020, 103 (Suppl. S1), 66–79. [Google Scholar] [CrossRef] [PubMed]
- Sokolow, S.H.; Huttinger, E.; Jouanard, N.; Hsieh, M.H.; Lafferty, K.D.; Kuris, A.M.; Riveau, G.; Senghor, S.; Thiam, C.; N’Diaye, A.; et al. Reduced transmission of human schistosomiasis after restoration of a native river prawn that preys on the snail intermediate host. Proc. Natl. Acad. Sci. USA 2015, 112, 9650–9655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, K.; Sun, L.P.; Liang, Y.S.; Wu, F.; Li, W.; Zhang, J.F.; Huang, Y.X.; Hang, D.R.; Liang, S.; Bergquist, R.; et al. Schistosoma japonicum risk in Jiangsu province, People’s Republic of China: Identification of a spatio-temporal risk pattern along the Yangtze River. Geospat. Health 2013, 8, 133–142. [Google Scholar] [CrossRef] [Green Version]
- Hamburger, J.; Xu, Y.; Ramzy, R.M.; Jourdane, J.; Ruppel, A. Development and laboratory evaluation of a polymerase chain reaction for monitoring Schistosoma mansoni infestation of water. Am. J. Trop. Med. Hyg. 1998, 59, 468–473. [Google Scholar] [CrossRef] [Green Version]
- Hertel, J.; Kedves, K.; Hassan, A.H.M.; Haberl, B.; Haas, W. Detection of Schistosoma mansoni cercariae in plankton samples by PCR. Acta Trop. 2004, 91, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Amarir, F.; Sebti, F.; Abbasi, I.; Sadak, A.; Fellah, H.; Nhammi, H.; Ameur, B.; El Idrissi, A.L.; Rhajaoui, M. Schistosoma haematobium detection in snails by DraI PCR and Sh110/Sm-Sl PCR: Further evidence of the interruption of schistosomiasis transmission in Morocco. Parasites Vectors 2014, 7, 288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbasi, I.; King, C.H.; Sturrock, R.F.; Kariuki, C.; Muchiri, E.; Hamburger, J. Differentiation of Schistosoma haematobium from related schistosomes by PCR amplifying an inter-repeat sequence. Am. J. Trop. Med. Hyg. 2007, 76, 950–955. [Google Scholar] [CrossRef] [PubMed]
- Hamburger, J.; Hoffman, O.; Kariuki, H.C.; Muchiri, E.M.; Ouma, J.H.; Koech, D.K.; Sturrock, R.F.; King, C.H. Large-scale, polymerase chain reaction-based surveillance of Schistosoma haematobium DNA in snails from transmission sites in coastal Kenya: A new tool for studying the dynamics of snail infection. Am. J. Trop. Med. Hyg. 2004, 71, 765–773. [Google Scholar] [CrossRef]
- Melo, F.L.; Gomes, A.L.; Barbosa, C.S.; Werkhauser, R.P.; Abath, F.G. Development of molecular approaches for the identification of transmission sites of schistosomiasis. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 1049–1055. [Google Scholar] [CrossRef]
- Sato, M.O.; Rafalimanantsoa, A.; Ramarokoto, C.; Rahetilahy, A.M.; Ravoniarimbinina, P.; Kawai, S.; Minamoto, T.; Sato, M.; Kirinoki, M.; Rasolofo, V.; et al. Usefulness of environmental DNA for detecting Schistosoma mansoni occurrence sites in Madagascar. Int. J. Infect. Dis. 2018, 76, 130–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schols, R.; Carolus, H.; Hammoud, C.; Mulero, S.; Mudavanhu, A.; Huyse, T. A rapid diagnostic multiplex PCR approach for xenomonitoring of human and animal schistosomiasis in a ‘One Health’ context. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 722–729. [Google Scholar] [CrossRef]
- Pennance, T.; Archer, J.; Lugli, E.B.; Rostron, P.; Llanwarne, F.; Ali, S.M.; Amour, A.K.; Suleiman, K.R.; Li, S.; Rollinson, D.; et al. Development of a Molecular Snail Xenomonitoring Assay to Detect Schistosoma haematobium and Schistosoma bovis Infections in their Bulinus Snail Hosts. Molecules 2020, 25, 4011. [Google Scholar] [CrossRef]
- Mahmoud, A.A. Schistosomiasis; Imperial College Press: London, UK, 2001; Volume 3. [Google Scholar]
- Sarant, L. Egypt: The flatworm’s revenge. Nature 2017, 551, S46–S47. [Google Scholar] [CrossRef] [PubMed]
- Ruffer, M.A. Note on the presence of "bilharzia haematobia" in Egyptian mummies of the twentieth dynasty [1250–1000 b.C.]. Br. Med. J. 1910, 1, 16. [Google Scholar] [CrossRef]
- Cox, F.E.G. History of Human Parasitology. Clin. Microbiol. Rev. 2002, 15, 595. [Google Scholar] [CrossRef] [Green Version]
- Di Bella, S.; Riccardi, N.; Giacobbe, D.R.; Luzzati, R. History of schistosomiasis (bilharziasis) in humans: From Egyptian medical papyri to molecular biology on mummies. Pathog. Glob. Health 2018, 112, 268–273. [Google Scholar] [CrossRef]
- Appleton, C.C.; Naidoo, I. Why did schistosomiasis disappear from the southern part of the Eastern Cape? S. Afr. J. Sci. 2012, 108, 1–11. [Google Scholar] [CrossRef]
- Harley, J. On the endemic haematuria of the Cape of Good Hope. J. R. Soc. Med. 1864, 47, 55–72. [Google Scholar] [CrossRef]
- Bilharz, T.; Siebold, C.T. Ein Beitrag zur Helminhographia humana, aus brieflichen Mitteilungen des Dr. Bilharz in Cairo, nenst Bermerkungen von Prof. C. Th. von Siebold in Breslau. Z. Wiss. Zool. 1852, 4, 53–76. [Google Scholar]
- Porter, A. The Larval Trematoda Found in Certain South African Mollusca with Special Eference to Schistosomiasls; Publications of the South African Institute for Medical Research: Bilharzlasls, Congo, 1938; 492p. [Google Scholar]
- Gear, J.; Pitchford, R.J.; van Eeden, J.A. Atlas of bilharzia in Southern Africa. Joint publication by the South. African Institute for Medical Research; South African Medical Research Council: Johannesburg, South Africa, 1980. [Google Scholar]
- Appleton, C.C.; Kvalsvig, J.D. A school-based helminth control programme successfully implemented in KwaZulu-Natal. S. Afr. J. Epidemiol. Infect. 2006, 21, 55–67. [Google Scholar] [CrossRef] [Green Version]
- Utroska, J.A.; Chen, M.G.; Dixon, H.; Yoon, S.-Y.; Helling-Borda, M.; Hogerzeil, H.V.; Mott, K.E.; World Health Organization. Schistosomiasis Control, U. An Estimate of Global Needs for Praziquantel within Schistosomiasis Control Programmes / by J. A. Utroska; World Health Organization: Geneva, Swizterland, 1990. [Google Scholar]
- Chernin, E. The curious case of the lateral-spined egg: Schistosoma mansoni. Trans. R. Soc. Trop. Med. Hyg. 1983, 77, 847–850. [Google Scholar] [CrossRef]
- WHO. The control of schistosomiasis. Second report of the WHO Expert Committee. Tech. Rep. Ser. 1993, 830, 1–86. [Google Scholar]
- WHO. Current Estimated Total Number of Individuals with Morbidity and Mortality due to Schistosomiasis Haematobium and S. Mansoni infection in Sub-Saharan Africa. Schistosomiasis; Epidemiological situation; World Health Organisation: Pretoria, South Africa, 2020. [Google Scholar]
- WHO. Regional Office for Africa. 03/06/2020 03/06/2020. Available online: https://espen.afro.who.int/regions/who-african-region-afro (accessed on 3 June 2020).
- IAMAT. Travel Health Information. Available online: Iamat.org (accessed on 3 June 2020).
- Salwa, D.; Hesham, M.A.-M.; Init, I.; Jamaiah, I.; Awatif, M.A.; Abdulhamid, A.; Hany, S.; Nabil, A.N.; Wahib, M.A. The menace of schistosomiasis in Nigeria: Knowledge, attitude, and practices regarding schistosomiasis among rural communities in Kano State. PLoS ONE 2015, 10, e0143667. [Google Scholar]
- Cowper, S.G. Schistosomiasis in Nigeria. Ann. Trop. Med. Parasitol. 1963, 57, 307–322. [Google Scholar] [CrossRef]
- Ezeh, C.O.; Onyekwelu, K.C.; Akinwale, O.P.; Shan, L.; Wei, H. Urinary schistosomiasis in Nigeria: A 50 year review of prevalence, distribution and disease burden. Parasite 2019, 26, 19. [Google Scholar] [CrossRef] [Green Version]
- WHO. Atlas of Global Distribution of Schistosomiasis. Available online: https://www.who.int/schistosomiasis/epidemiology/en/nigeria.pdf. (accessed on 10 January 2020).
- World Bank. World Development Report; World Bank: Washington, DC, USA, 1997. [Google Scholar]
- Adenowo, A.F.; Oyinloye, B.E.; Ogunyinka, B.I.; Kappo, A.P. Impact of human schistosomiasis in sub-Saharan Africa. Braz. J. Infect. Dis. 2015, 19, 196–205. [Google Scholar] [CrossRef] [Green Version]
- Arene, F.; Ukpeibo, E.; Nwanze, E. Studies on schistosomiasis in the Niger Delta: Schistosoma intercalatum in the urban city of Port Harcourt, Nigeria. Public Heal. 1989, 103, 295–301. [Google Scholar] [CrossRef]
- Ndukwe, Y.E.; Obiezue, R.N.; Aguzie, I.O.N.; Anunobi, J.T.; Okafor, F.C. Corrigendum: Mapping of Urinary Schistosomiasis in Anambra State, Nigeria. Ann. Glob. Heal. 2019, 85, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, J.D.; Endeshaw, T.; Escher, E.; Alemtaye, G.; Melaku, S.; Gelaye, W.; Worku, A.; Adugna, M.; Melak, B.; Teferi, T.; et al. Intestinal Parasite Prevalence in an Area of Ethiopia after Implementing the SAFE Strategy, Enhanced Outreach Services, and Health Extension Program. PLoS Negl. Trop. Dis. 2013, 7, e2223. [Google Scholar] [CrossRef] [Green Version]
- Atalabi, T.E.; Lawal, U.; Ipinlaye, S.J. Prevalence and intensity of genito-urinary schistosomiasis and associated risk factors among junior high school students in two local government areas around Zobe Dam in Katsina State, Nigeria. Parasites Vectors 2016, 9, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atalabi, T.E.; Adoh, S.D.; Eze, K.M. The current epidemiological status of urogenital schistosomiasis among primary school pupils in Katsina State, Nigeria: An imperative for a scale up of water and sanitation initiative and mass administration of medicines with Praziquantel. PLOS Negl. Trop. Dis. 2018, 12, e0006636. [Google Scholar] [CrossRef] [Green Version]
- Okoli, C.; Iwuala, M. The prevalence, intensity and clinical signs of urinary schistosomiasis in Imo state, Nigeria. J. Helminthol. 2004, 78, 337–342. [Google Scholar] [CrossRef]
- Bocanegra, C.; Gallego, S.; Mendioroz, J.; Moreno, M.; Sulleiro, E.; Salvador, F.; Sikaleta, N.; Nindia, A.; Tchipita, D.; Joromba, M.; et al. Epidemiology of schistosomiasis and usefulness of indirect diagnostic tests in school-age children in Cubal, Central Angola (schistosomiasis in Cubal, Angola). PLoS Negl. Trop. Dis. 2015, 9, e0004055. [Google Scholar] [CrossRef] [Green Version]
- Gandasegui, J.; Fernández-Soto, P.; Dacal, E.; Rodríguez, E.; Saugar, J.M.; Yepes, E.; Aznar-Ruiz-De-Alegría, M.L.; Espasa, M.; Ninda, A.; Bocanegra, C.; et al. Field and laboratory comparative evaluation of a LAMP assay for the diagnosis of urogenital schistosomiasis in Cubal, Central Angola. Trop. Med. Int. Health 2018, 23, 992–1001. [Google Scholar] [CrossRef]
- Onzo-Aboki, A.; Ibikounlé, M.; Boko, P.M.; Savassi, B.S.; Doritchamou, J.; Siko, E.J.; Daré, A.; Batcho, W.; Massougbodji, A.; Tougoue, J.J.; et al. Human schistosomiasis in Benin: Countrywide evidence of Schistosoma haematobium predominance. Acta Trop. 2019, 191, 185–197. [Google Scholar] [CrossRef]
- Ouedraogo, H.; Drabo, F.; Zongo, D.; Bagayan, M.; Bamba, I.; Pima, T.; Yago-Wienne, F.; Toubali, E.; Zhang, Y. Schistosomiasis in school-age children in Burkina Faso after a decade of preventive chemotherapy. Bull. World Heal. Organ. 2015, 94, 37–45. [Google Scholar] [CrossRef]
- Lalaye, D.; Bruijn, M.; De Jong, T. Prevalence of Schistosoma haematobium in an unexplored endemic region in the sub-prefecture of Torrock, Chad (Preprint). JMIR Public Health Surveill. 2019, 5. [Google Scholar] [CrossRef] [PubMed]
- Angora, E.K.; Boissier, J.; Menan, H.; Rey, O.; Tuo, K.; Touré, A.O.; Coulibaly, J.T.; Méité, A.; Raso, G.; N’Goran, E.K.; et al. Prevalence and risk factors for schistosomiasis among school children in two settings of Côte d’Ivoire. Trop. Med. Infect. Dis. 2019, 4, 110. [Google Scholar] [CrossRef] [Green Version]
- Linsuke, S.; Nundu, S.; Mupoyi, S.; Mukele, R.; Mukunda, F.; Kabongo, M.M.; Da Luz, R.I.; Van Geertruyden, J.-P.; Van Sprundel, M.; Boelaert, M.; et al. High Prevalence of Schistosoma mansoni in Six Health Areas of – Kasansa Health Zone, Democratic Republic of the Congo: Short Report. PLoS Negl. Trop. Dis. 2014, 8, e3387. [Google Scholar] [CrossRef] [Green Version]
- Da Luz, R.I.; Linsuke, S.; Lutumba, P.; Hasker, E.; Boelaert, M. Assessment of schistosomiasis and soil-transmitted helminths prevalence in school-aged children and opportunities for integration of control in local health services in Kwilu Province, the Democratic Republic of the Congo. Trop. Med. Int. Heal. 2017, 22, 1442–1450. [Google Scholar] [CrossRef] [Green Version]
- Gadoth, A.; Mvumbi, G.; Hoff, N.A.; Musene, K.; Mukadi, P.; Ashbaugh, H.R.; Doshi, R.H.; Javanbakht, M.; Gorbach, P.; Okitolonda-Wemakoy, E.; et al. Urogenital Schistosomiasis and Sexually Transmitted Coinfections among Pregnant Women in a Schistosome-Endemic Region of the Democratic Republic of Congo. Am. J. Trop. Med. Hyg. 2019, 101, 828–836. [Google Scholar] [CrossRef]
- Kabongo, M.M.; Linsuke, S.; Baloji, S.; Mukunda, F.; Raquel, I.D.L.; Stauber, C.; Van Geertruyden, J.-P.; Lutumba, P. Schistosoma mansoni infection and its association with nutrition and health outcomes: A household survey in school-aged children living in Kasansa, Democratic Republic of the Congo. Pan. Afr. Med. J. 2018, 31, 197. [Google Scholar] [CrossRef]
- Knoblauch, A.; Archer, C.; Owuor, M.; Schmidlin, S.; Divall, M.J.; Utzinger, J.; Winkler, M.S. Schistosomiasis and soil-transmitted helminth infections in schoolchildren in north-eastern Democratic Republic of the Congo. Trans. R. Soc. Trop. Med. Hyg. 2016, 110, 424–426. [Google Scholar] [CrossRef]
- Kabore, A.; Ibikounle, M.; Tougoue, J.J.; Mupoyi, S.; Ndombe, M.; Shannon, S.; Ottesen, E.A.; Mukunda, F.; Awaca, N. Initiating NTD programs targeting schistosomiasis and soil-transmitted helminthiasis in two provinces of the Democratic Republic of the Congo: Establishment of baseline prevalence for mass drug administration. Acta Trop. 2017, 166, 177–185. [Google Scholar] [CrossRef]
- Tchuenté, L.A.T.; Southgate, V.; Vercruysse, J.; Kaukas, A.; Kane, R.; Mulumba, M.; Pagés, J.; Jourdane, J. Epidemiological and genetic observations on human schistosomiasis in Kinshasa, Zaire. Trans. R. Soc. Trop. Med. Hyg. 1997, 91, 263–269. [Google Scholar] [CrossRef]
- Elmorshedy, H.; Bergquist, R.; Fayed, A.; Guirguis, W.; Abdel-Gawwad, E.; Eissa, S.; Barakat, R. Elimination of schistosomiasis requires multifactorial diagnostics: Evidence from high- and low-prevalence areas in the Nile Delta, Egypt. Infect. Dis. Poverty 2020, 9, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Sharazly, B.; Abou Rayia, D.; Antonios, S.; Eissa, S.H. Current status of Schistosoma mansoni infection and its snail host in three rural areas in Gharbia governorate, Egypt. Tanta Med. J. 2016, 44, 141–150. [Google Scholar] [CrossRef]
- Simarro, P.P.; Sima, F.; Mir, M.; Ndong, P. Effect of repeated targeted mass treatment with praziquantel on the prevalence, intensity of infection and morbidity due to Schistosoma intercalatum in an urban community in equatorial Guinea. Trop. Med. Parasitol Off. Organ Dtsch. Tropenmedizinische Ges. Dtsch. Ges. fur Tech. Zusammenarbeit (GTZ) 1991, 42, 167–171. [Google Scholar]
- Simarroi, P.P.; Noong, P.; Mir, M.; Nguema, E. Urban schistosomiasis in Equitorial Guinea. Research and Reviews in Parasitology. Res. Rev. Parasitol. 1993, 53, 93–95. [Google Scholar]
- Bekana, T.; Hu, W.; Liang, S.; Erko, B. Transmission of Schistosoma mansoni in Yachi areas, southwestern Ethiopia: New foci. Infect. Dis. Poverty 2019, 8, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Alebie, G.; Erko, B.; Aemero, M.; Petros, B. Epidemiological study on Schistosoma mansoni infection in Sanja area, Amhara region, Ethiopia. Parasites Vectors 2014, 7, 15. [Google Scholar] [CrossRef] [Green Version]
- Bajiro, M.; Dana, D.; Ayana, M.; Emana, D.; Mekonnen, Z.; Zawdie, B.; Garbi, A.; Kure, A.; Zeynudin, A. Prevalence of Schistosoma mansoni infection and the therapeutic efficacy of praziquantel among school children in Manna District, Jimma Zone, southwest Ethiopia. Parasites Vectors 2016, 9, 560. [Google Scholar] [CrossRef] [Green Version]
- Alemayehu, B.; Tomass, Z.; Wadilo, F.; Leja, D.; Liang, S.; Erko, B. Epidemiology of intestinal helminthiasis among school children with emphasis on Schistosoma mansoni infection in Wolaita zone, Southern Ethiopia. BMC Public Heal. 2017, 17, 1–10. [Google Scholar] [CrossRef]
- Kenguele, H.M.; Adegnika, A.A.; Nkoma, A.-M.; Ateba-Ngoa, U.; Mbong, M.; Zinsou, J.F.; Lell, B.; Verweij, J.J.; Gabon, S. Short report: Impact of short-time urine freezing on the sensitivity of an established Schistosoma real-time PCR assay. Am. J. Trop. Med. Hyg. 2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dejon-Agobé, J.C.; Edoa, J.R.; Honkpehedji, Y.J.; Zinsou, J.F.; Adegbite, B.R.; Ngwese, M.M.; Mangaboula, A.; Lell, B.; Grobusch, M.P.; Mordmüller, B.; et al. Schistosoma haematobium infection morbidity, praziquantel effectiveness and reinfection rate among children and young adults in Gabon. Parasites Vectors 2019, 12, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Sanneh, B.; Joof, E.; Sanyang, A.M.; Renneker, K.; Camara, Y.; Sey, A.P.; Jagne, S.; Baldeh, I.; Ceesay, S.J.; Sambou, S.M.; et al. Field evaluation of a schistosome circulating cathodic antigen rapid test kit at point-of-care for mapping of schistosomiasis endemic districts in The Gambia. PLoS ONE 2017, 12, e0182003. [Google Scholar] [CrossRef] [Green Version]
- Anyan, W.K.; Pulkkila, B.R.; Dyra, C.E.; Price, M.; Naples, J.M.; Quartey, J.K.; Anang, A.K.; Lodh, N. Assessment of dual schistosome infection prevalence from urine in an endemic community of Ghana by molecular diagnostic approach. Parasite Epidemiol. Control 2020, 9, e00130. [Google Scholar] [CrossRef]
- Cunningham, L.J.; Campbell, S.J.; Armoo, S.; Koukounari, A.; Watson, V.; Selormey, P.; Stothard, J.R.; Idun, B.; Asiedu, M.; Ashong, Y.; et al. Assessing expanded community wide treatment for schistosomiasis: Baseline infection status and self-reported risk factors in three communities from the Greater Accra region, Ghana. PLoS Negl. Trop. Dis. 2020, 14, e0007973. [Google Scholar] [CrossRef]
- Hodges, M.; Koroma, M.M.; Baldé, M.S.; Turay, H.; Fofanah, I.; Divall, M.J.; Winkler, M.S.; Zhang, Y. Current status of schistosomiasis and soil-transmitted helminthiasis in Beyla and Macenta Prefectures, Forest Guinea. Trans. R. Soc. Trop. Med. Hyg. 2011, 105, 672–674. [Google Scholar] [CrossRef] [Green Version]
- Botelho, M.C.; Machado, A.; de Carvalho, A.F.C.; Vilaça, M.; Conceição, O.; Rosa, F.; Alves, H.; Richter, J.; Bordalo, A.A. Schistosoma haematobium in Guinea-Bissau: Unacknowledged morbidity due to a particularly neglected parasite in a particularly neglected country. Parasitol. Res. 2016, 115, 1567–1572. [Google Scholar] [CrossRef]
- Vinkeles Melchers, N.V.S.; van Dam, G.J.; Shaproski, D.; Kahama, A.I.; Brienen, E.A.T.; Vennervald, B.J.; van Lieshout, L. Diagnostic performance of Schistosoma Real-Time PCR in urine samples from Kenyan children infected with Schistosoma haematobium: Day-to-day variation and follow-up after praziquantel treatment (Diagnostic Accuracy of Urine Schistosoma PCR). PLoS Negl. Trop. Dis. 2014, 8, e2807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foo, K.T.; Matete, D.O.; Karanja, D.M.S.; Mwinzi, P.N.M.; Secor, W.E.; Montgomery, S.P.; Blackstock, A.J.; Ochola, E.A. Evaluation of Point-of-Contact Circulating Cathodic Antigen Assays for the Detection of Schistosoma mansoni Infection in Low-, Moderate-, and High-Prevalence Schools in Western Kenya. Am. J. Trop. Med. Hyg. 2015, 92, 1227–1232. [Google Scholar] [CrossRef] [Green Version]
- Odiere, M.R.; Rawago, F.; Ombok, M.; Secor, W.E.; Karanja, D.M.S.; Mwinzi, P.N.M.; Lammie, P.J.; Won, K. High prevalence of schistosomiasis in Mbita and its adjacent islands of Lake Victoria, western Kenya. Parasites Vectors 2012, 5, 278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazura, J.W.; Dennis, E.; Neill, M.; Peters, P.A.S. Swamp Rice Farming: Possible Effects on Endemicity of Schistosomiasis Mansoni and Haematobia in a Population in Liberia. Am. J. Trop. Med. Hyg. 1985, 34, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.; Gankpala, A.; Gankpala, L.; Bolay, F.K.; Curtis, K.C.; Weil, G.J.; Fischer, P.U. Capillaria Ova and Diagnosis of Trichuris trichiura Infection in Humans by Kato-Katz Smear, Liberia. Emerg. Infect. Dis. 2018, 24, 1551–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pillay, P.; Downs, J.; Changalucha, J.; Brienen, E.; Ramarokoto, C.; Leutscher, P.; Vennervald, B.; Taylor, M.; Kjetland, E.; Van Lieshout, L. Detection of Schistosoma DNA in genital specimens and urine: A comparison between five female African study populations originating from S. haematobium and/or S. mansoni endemic areas. Acta Trop. 2020, 204, 105363. [Google Scholar] [CrossRef]
- Rasoamanamihaja, C.F.; Rahetilahy, A.M.; Ranjatoarivony, B.; Dhanani, N.; Andriamaro, L.; Andrianarisoa, S.H.; Jourdan, P.M. Baseline prevalence and intensity of schistosomiasis at sentinel sites in Madagascar: Informing a national control strategy. Parasites Vectors 2016, 9, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spencer, S.A.; Penney, J.M.S.J.; Russell, H.J.; Howe, A.P.; Linder, C.; Rakotomampianina, A.L.D.; Nandimbiniaina, A.M.; Squire, S.B.; Stothard, J.R.; Bustinduy, A.L.; et al. High burden of Schistosoma mansoni infection in school-aged children in Marolambo District, Madagascar. Parasites Vectors 2017, 10, 307. [Google Scholar] [CrossRef] [Green Version]
- Moyo, V.; Changadeya, W.; Chiotha, S.; Sikawa, D. Urinary schistosomiasis among preschool children in Malengachanzi, Nkhotakota District, Malawi: Prevalence and risk factors. Malawi Med. J. 2016, 28, 10–14. [Google Scholar] [CrossRef] [Green Version]
- Kayuni, S.; Peeling, R.; Makaula, P. Prevalence and distribution of Schistosoma haematobium infection among school children living in southwestern shores of Lake Malawi. Malawi Med. J. 2017, 29, 16–23. [Google Scholar] [CrossRef] [Green Version]
- Dabo, A.; Badawi, H.M.; Bary, B.; Doumbo, O.K. Urinary schistosomiasis among preschool-aged children in Sahelian rural communities in Mali. Parasites Vectors 2011, 4, 21. [Google Scholar] [CrossRef] [Green Version]
- Landouré, A.; Dembélé, R.; Goita, S.; Kané, M.; Tuinsma, M.; Sacko, M.; Toubali, E.; French, M.D.; Keita, A.D.; Fenwick, A.; et al. Significantly reduced intensity of infection but persistent prevalence of schistosomiasis in a highly endemic region in Mali after repeated treatment. PLoS Negl. Trop. Dis. 2012, 6, e1774. [Google Scholar] [CrossRef] [Green Version]
- Gbalégba, N.G.C.; Silué, K.D.; Ba, O.; Ba, H.; Tian-Bi, N.T.Y.; Yapi, G.Y.; Kaba, A.; Koné, B.; Utzinger, J.; Koudou, B.G. Prevalence and seasonal transmission of Schistosoma haematobium infection among school-aged children in Kaedi town, southern Mauritania. Parasites Vectors 2017, 10, 353. [Google Scholar] [CrossRef] [Green Version]
- Urbani, C.; Touré, A.; O Hamed, A.; Albonico, M.; Kane, I.; Cheikna, D.; Hamed, N.; Montresor, A.; Savioli, L. Intestinal parasitic infections and schistosomiasis in the valley of the Senegal river in the Islamic Republic of Mauritania. Med. Trop. Rev. Du Corps De Sante Colon. 1997, 57, 157–160. [Google Scholar]
- Salem, C.B.O.A.; Boussery, A.; Hafid, J. Study of prevalence and parasite load of Schistosoma haematobium in schoolchildren in the Rosso region, Mauritania. Med. Sante Trop. 2019, 29, 268–272. [Google Scholar]
- Phillips, A.E.; Gazzinelli-Guimarães, P.H.; Aurelio, H.O.; Dhanani, N.; Ferro, J.; Nala, R.; Deol, A.; Fenwick, A. Urogenital schistosomiasis in Cabo Delgado, northern Mozambique: Baseline findings from the SCORE study. Parasites Vectors 2018, 11, 30. [Google Scholar] [CrossRef] [Green Version]
- Casmo, V.; Augusto, G.; Nala, R.; Sabonete, A. and Carvalho-Costa, F.A. The effect of hookworm infection and urinary schistosomiasis on blood hemoglobin concentration of schoolchildren living in northern Mozambique. Rev. Do Inst. De Med. Trop. De Sao Paulo 2014, 56, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Augusto, G.; Nala, R.; Casmo, V.; Sabonete, A.; Mapaco, L.; Monteiro, J. Geographic distribution and prevalence of schistosomiasis and soil-transmitted hhelminths among schoolchildren in Mozambique. Am. J. Trop. Med. Hyg. 2009, 81, 799–803. [Google Scholar] [CrossRef] [Green Version]
- Sousa-Figueiredo, J.C.; Stanton, M.C.; Katokele, S.; Arinaitwe, M.; Adriko, M.; Balfour, L.; Reiff, M.; Lancaster, W.; Noden, B.H.; Bock, R.; et al. Mapping of Schistosomiasis and Soil-Transmitted Helminths in Namibia: The First Large-Scale Protocol to Formally Include Rapid Diagnostic Tests. PLoS Negl. Trop. Dis. 2015, 9, e0003831. [Google Scholar] [CrossRef] [Green Version]
- Ibironke, O.A.; Shiff, C.; Garba, A.; Phillips, A.E.; Lamine, S.M. Diagnosis of Schistosoma haematobium by Detection of Specific DNA Fragments from Filtered Urine Samples. Am. J. Trop. Med. Hyg. 2011, 84, 998–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakare, S.; Adebayo, A.; Awobode, H.; Onile, O.; Agunloye, A.; Isokpehi, R.; Anumudu, C. Arsenicosis in bladder pathology and schistosomiasis in Eggua, Nigeria. Trans. R. Soc. Trop. Med. Hyg. 2018, 112, 230–237. [Google Scholar] [CrossRef]
- Otuneme, O.G.; O Obebe, O.; Sajobi, T.T.; Akinleye, W.; Faloye, T.G. Prevalence of Schistosomiasis in a neglected community, South western Nigeria at two points in time, spaced three years apart. Afr. Heal. Sci. 2019, 19, 1338–1345. [Google Scholar] [CrossRef] [Green Version]
- Eyong, M.; E Ikepeme, E.; Ekanem, E. Relationship between Schistosoma haematobium infection and urinary tract infection among children in South Eastern, Nigeria. Niger. Postgrad. Med. J. 2008, 15, 89–93. [Google Scholar]
- Ekanem, E.E.; Akapan, F.M.; Eyong, M.E. Urinary schistosomiasis in school children of a southern nigerian community 8 years after the provision of potable water. Niger. Postgrad. Med. J. 2017, 24, 201. [Google Scholar] [CrossRef] [PubMed]
- Josh, R.; Blaise, K.; Denise, M.; Eugene, R.; Nadine, R.; Gaspard, K.; Corine, K.; Deville, M.; Fenwick, A. School Prevalence Surveys on Soil Transmitted Helminths and Schistosomiasis, Rwanda. Int. J. Infect. Dis. 2008, 12, e376. [Google Scholar] [CrossRef] [Green Version]
- Hove, R.J.T.; Verweij, J.J.; Vereecken, K.; Polman, K.; Dieye, L.; Van Lieshout, L. Multiplex real-time PCR for the detection and quantification of Schistosoma mansoni and S. haematobium infection in stool samples collected in northern Senegal. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 179–185. [Google Scholar] [CrossRef]
- Sacolo-Gwebu, H.; Chimbari, M.; Kalinda, C. Prevalence and risk factors of schistosomiasis and soil-transmitted helminthiases among preschool aged children (1–5 years) in rural KwaZulu-Natal, South Africa: A cross-sectional study. Infect. Dis. Poverty 2019, 8, 47. [Google Scholar] [CrossRef] [Green Version]
- Rubaba, O.; Chimbari, M.; Soko, W.; Manyangadze, T.; Mukaratirwa, S. Validation of a urine circulating cathodic antigen cassette test for detection of Schistosoma haematobiumin uMkhanyakude district of South Africa. Acta Trop. 2018, 182, 161–165. [Google Scholar] [CrossRef]
- Pillay, P.; Kjetland, E.F.; Brienen, E.A.T.; Taylor, M.; Van Lieshout, L.; Gundersen, S.G.; Hoekstra, P.; Zulu, S.G.; Verweij, J.J.; Kleppa, E. Real-Time Polymerase Chain Reaction for Detection of Schistosoma DNA in Small-Volume Urine Samples Reflects Focal Distribution of Urogenital Schistosomiasis in Primary School Girls in KwaZulu Natal, South Africa. Am. J. Trop. Med. Hyg. 2014, 90, 546–552. [Google Scholar] [CrossRef] [Green Version]
- Kabuyaya, M.; Chimbari, M.J.; Manyangadze, T.; Mukaratirwa, S. Schistosomiasis risk factors based on the infection status among school-going children in the Ndumo area, Umkhanyakude district. S. Afr. J. Infect. Dis. 2017, 32, 67–72. [Google Scholar]
- Eltoum, I.A.; Sulaiman, S.M.; Elturabi, H.; Mahgoub, E.; Homeida, M.M. Infection with Schistosoma mansoni in two different endemic areas: a comparative population-based study in Elziedab and Gezira-Managil irrigation schemes, Sudan. J. Trop. Med. Hyg. 1993, 96, 100–106. [Google Scholar] [PubMed]
- Song, H.B.; Kim, J.; Jin, Y.; Lee, J.S.; Jeoung, H.G.; Lee, Y.H.; Saeed, A.A.W.; Hong, S.-T. Comparison of ELISA and Urine Microscopy for Diagnosis ofSchistosoma haematobiumInfection. J. Korean Med. Sci. 2018, 33, e238. [Google Scholar] [CrossRef]
- Liao, C.W.; Sukati, H.; Nara, T.; Tsubouchi, A.; Chou, C.-M.; Jian, J.-Y.; Huang, Y.-C.; Chang, P.W.-S.; Chiu, W.-T.; Huang, Y.-H.; et al. Prevalence of Schistosoma haematobium infection among schoolchildren in remote areas devoid of sanitation in northwestern Swaziland, Southern Africa. JPN. J. Infect. Dis. 2011, 64, 322–326. [Google Scholar]
- Chu, T.B.; Liao, C.W.; D’Lamini, P.; Chang, P.W.S.; Chiu, W.T.; Du, W.Y.; Fan, C.K. Prevalence of Schistosoma haematobium infection among inhabitants of Lowveld, Swaziland, an endemic area for the disease. Trop. Biomed. 2010, 27, 337–342. [Google Scholar]
- Fuss, A.; Mazigo, H.D.; Tappe, D.; Kasang, C.; Mueller, A. Comparison of sensitivity and specificity of three diagnostic tests to detect Schistosoma mansoni infections in school children in Mwanza region, Tanzania. PLoS ONE 2018, 13, e0202499. [Google Scholar] [CrossRef]
- Mueller, A.; Fuss, A.; Ziegler, U.; Kaatano, G.M.; Mazigo, H.D. Intestinal schistosomiasis of Ijinga Island, north-western Tanzania: Prevalence, intensity of infection, hepatosplenic morbidities and their associated factors. BMC Infect. Dis. 2019, 19, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Mnkugwe, R.H.; Minzi, O.S.; Kinung’hi, S.M.; Kamuhabwa, A.A.; Aklillu, E. Prevalence and correlates of intestinal schistosomiasis infection among school-aged children in North-Western Tanzania. PLoS ONE 2020, 15, e0228770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siza, J.E.; Kaatano, G.M.; Chai, J.-Y.; Eom, K.S.; Rim, H.-J.; Yong, T.-S.; Min, D.-Y.; Chang, S.Y.; Ko, Y.; Changalucha, J.M. Prevalence of schistosomes and soil-transmitted Helminths among school children in Lake Victoria Basin, Tanzania. Korean J. Parasitol. 2015, 53, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Munisi, D.Z.; Buza, J.; Mpolya, E.A.; Kinung’hi, S.M. Intestinal schistosomiasis among primary schoolchildren in two on-shore communities in Rorya District, Northwestern Tanzania: Prevalence, intensity of infection and associated risk factors. J. Parasitol. Res. 2016, 2016, 1859737. [Google Scholar] [CrossRef] [Green Version]
- Al-Shehri, H.; Koukounari, A.; Stanton, M.C.; Adriko, M.; Arinaitwe, M.; Atuhaire, A.; Kabatereine, N.B.; Stothard, J.R. Surveillance of intestinal schistosomiasis during control: a comparison of four diagnostic tests across five Ugandan primary schools in the Lake Albert region. Parasitology 2018, 145, 1715–1722. [Google Scholar] [CrossRef] [Green Version]
- Nalugwa, A.; Olsen, A.; Tukahebwa, M.; Nuwaha, F. Intestinal schistosomiasis among preschool children along the shores of Lake Victoria in Uganda. Acta Trop. 2015, 142, 115–121. [Google Scholar] [CrossRef]
- Kabatereine, N.B.; Standley, C.J.; Sousa-Figueiredo, J.C.; Fleming, F.M.; Stothard, J.R.; Talisuna, A.; Fenwick, A. Integrated prevalence mapping of schistosomiasis, soil-transmitted helminthiasis and malaria in lakeside and island communities in Lake Victoria, Uganda. Parasites Vectors 2011, 4, 232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Betson, M.; Sousa-Figueiredo, J.C.; Rowell, C.; Kabatereine, N.B.; Stothard, J.R. Intestinal Schistosomiasis in Mothers and Young Children in Uganda: Investigation of Field-Applicable Markers of Bowel Morbidity. Am. J. Trop. Med. Hyg. 2010, 83, 1048–1055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adriko, M.; Tinkitina, B.; Tukahebw, E.; Standley, C.; Stothard, J.; Kabatereine, N. The epidemiology of schistosomiasis in Lango region Uganda 60 years after Schwetz 1951: Can schistosomiasis be eliminated through mass drug administration without other supportive control measures? Acta Trop. 2018, 185, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.-J.; Mwanakasale, V.; Xu, J.; Sun, L.-P.; Yin, X.-M.; Zhang, J.-F.; Hu, M.-C.; Si, W.-M.; Zhou, X.-N. Diagnostic performance of two specific schistosoma japonicum immunological tests for screening schistosoma haematobium in school children in Zambia. Acta Trop. 2020, 202, 105285. [Google Scholar] [CrossRef]
- Agnew-Blais, J.; Carnevale, J.; Gropper, A.; Shilika, E.; Bail, R.; Ngoma, M. Schistosomiasis Haematobium Prevalence and Risk Factors in a School-age Population of Peri-urban Lusaka, Zambia. J. Trop. Pediatr. 2009, 56, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Chama, M.F.; Shehata, M.A.; Funjika, E. Prevalence and intensity of Schistosoma haematobium infection among schoolchildren in central Zambia before and after mass treatment with a single dose of praziquantel. Trop. Parasitol. 2018, 8, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Mutengo, M.M.; Mduluza, T.; Chipeta, J.; Sianongo, S.; Mwansa, J.C.L. High Schistosoma mansoni Disease Burden in a Rural District of Western Zambia. Am. J. Trop. Med. Hyg. 2014, 91, 965–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nausch, N.; Dawson, E.M.; Midzi, N.; Mduluza, T.; Mutapi, F.; Doenhoff, M.J. Field evaluation of a new antibody-based diagnostic for Schistosoma haematobium and S. mansoniat the point-of-care in northeast Zimbabwe. BMC Infect. Dis. 2014, 14, 165. [Google Scholar] [CrossRef] [Green Version]
- Midzi, N.; Mduluza, T.; Chimbari, M.J.; Tshuma, C.; Charimari, L.; Mhlanga, G.; Manangazira, P.; Munyati, S.M.; Phiri, I.; Mutambu, S.L.; et al. Distribution of Schistosomiasis and Soil Transmitted Helminthiasis in Zimbabwe: Towards a National Plan of Action for Control and Elimination. PLoS Negl. Trop. Dis. 2014, 8, e3014. [Google Scholar] [CrossRef]
- Mutsaka-Makuvaza, M.J.; Matsena-Zingoni, Z.; Katsidzira, A.; Tshuma, C.; Chin’Ombe, N.; Zhou, X.-N.; Webster, B.; Midzi, N. Urogenital schistosomiasis and risk factors of infection in mothers and preschool children in an endemic district in Zimbabwe. Parasites Vectors 2019, 12, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Mazigo, H.D.; Nuwaha, F.; Kinung’hi, S.M.; Morona, D.; Pinot de Moira, A.; Wilson, S.; Heukelbach, J.; Dunne, D.W. Epidemiology and control of human schistosomiasis in Tanzania. Parasites Vectors 2012, 5, 274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooker, S.; Clements, A.C. Spatial heterogeneity of parasite co-infection: Determinants and geostatistical prediction at regional scales. Int. J. Parasitol. 2009, 39, 591–597. [Google Scholar] [CrossRef] [Green Version]
- McCullough, F.S. The distribution of Schistosoma mansoni and S. haematobium in East Africa. Trop. Geogr. Med. 1972, 24, 199–207. [Google Scholar]
- Clements, A.C.; Lwambo, N.J.; Blair, L.; Nyandindi, U.; Kaatano, G.; Kinung’hi, S.; Webster, J.P.; Fenwick, A.; Brooker, S. Bayesian spatial analysis and disease mapping: Tools to enhance planning and implementation of a schistosomiasis control programme in Tanzania. Trop. Med. Int. Health 2006, 11, 490–503. [Google Scholar] [CrossRef] [Green Version]
- Brooker, S.; Kabatereine, N.B.; Gyapong, J.O.; Stothard, J.R.; Utzinger, J. Rapid mapping of schistosomiasis and other neglected tropical diseases in the context of integrated control programmes in Africa. Parasitology 2009, 136, 1707–1718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rimoin, A.W.; Hotez, P.J. NTDs in the Heart of Darkness: The Democratic Republic of Congo’s Unknown Burden of Neglected Tropical Diseases. PLoS Negl. Trop. Dis. 2013, 7, e2118. [Google Scholar] [CrossRef] [PubMed]
- Madinga, J.; Linsuke, S.; Mpabanzi, L.; Meurs, L.; Kanobana, K.; Speybroeck, N.; Lutumba, P.; Polman, K. Schistosomiasis in the Democratic Republic of Congo: a literature review. Parasites Vectors 2015, 8, 601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumbu, R.K.; Makola, K.M.; Bin, L. Prevalence of Schistosoma mansoni Infection in Four Health Areas of Kisantu Health Zone, Democratic Republic of the Congo. Adv. Med. 2016, 2016, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Gyasi, S.F.; Boateng, A.A.; Awuah, E.; Antwi, E.O. Ellucidating the incidence and the prevalence of Schistosomiasis spp infection in riparian communities of the Bui dam. J. Parasit. Dis. 2019, 43, 276–288. [Google Scholar] [CrossRef]
- Hotez, P.J.; Savioli, L.; Fenwick, A. Neglected tropical diseases of the Middle East and North Africa: Review of their prevalence, distribution, and opportunities for control. PLoS Negl. Trop. Dis. 2012, 6, e1475. [Google Scholar] [CrossRef] [Green Version]
- Abou-El-Naga, I.F. Towards elimination of schistosomiasis after 5000 years of endemicity in Egypt. Acta Trop. 2018, 181, 112–121. [Google Scholar] [CrossRef]
- Fatima, A.; Abdelaali, B.; Corstjens, P.L.A.M.; Abderrahim, S.; El Bachir, A.; Mohamed, R. Survey and Diagnostic Challenges after Transmission-Stop: Confirming Elimination of Schistosomiasis haematobium in Morocco. J. Parasitol. Res. 2020, 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Amarir, F.; Fellah, H.; El Mansouri, B.; Wilkins, P.; Rhajaoui, M.; Handali, S.; Mohammed, L.; Sebti, F.; Sadak, A.; El Idrissi, A.L. National Serologic Survey of Haematobium Schistosomiasis in Morocco: Evidence for Elimination. Am. J. Trop. Med. Hyg. 2011, 84, 15–19. [Google Scholar] [CrossRef]
- Hedfi, M.; Debaibi, M.; Ben Iahouel, S.; Chouchen, A. Gallbladder schistosomiasis: Rare but possible, a case report and review of the literature. Pan Afr. Med. J. 2019, 32, 91. [Google Scholar] [PubMed]
- Horstick, O. Guide National d’Epidémiologie d’Intervention; République Tunisienne Ministère De La Santé Direction des Soins de Santé de Base: Tunisia, North Africa, 2015. [Google Scholar]
- WHO. Schistosomiasis: Progress Report 2001–2011 and Strategic Plan 2012–2020; WHO: Geneva, Swizterland, 2012. [Google Scholar]
- Emmanuel, I.O.A.; Ekkehard, D. Epidemiology, of bilharzias (schistosomiasis) in Uganda from 1902 until 2005. Afr. Heal. Sci. 2008, 8, 239–243. [Google Scholar]
- Nelson, G.S. Schistosoma mansoni infection in the West Nile District of Uganda. I. The incidence of S. mansoni infection. East Afr. Med. J. 1958, 35, 311–319. [Google Scholar]
- Rawson, P.A.G.B. Appendix, Annual Report-Uganda Medical Department; Uganda Medical Department: Uganda, East Africa, 1923. [Google Scholar]
- Schwetz, J. On vesical Bilharzia in the lango district (Uganda). Trans. R. Soc. Trop. Med. Hyg. 1951, 44, 501–514. [Google Scholar] [CrossRef]
- WHO. Atlas of Global Distribution of Schistosomiasis: 30-Uganda; World Health Organisation: Geneva, Swizterland, 1987; pp. 243–247. [Google Scholar]
- Ongom, V.L. The earliest age of infection with S. mansoni in West Nile District of Uganda. East Afr. Med. J. 1973, 50, 581–585. [Google Scholar] [PubMed]
- Sacolo, H.; Chimbari, M.; Kalinda, C. Knowledge, attitudes and practices on Schistosomiasis in sub-Saharan Africa: A systematic review. BMC Infect. Dis. 2018, 18, 46. [Google Scholar] [CrossRef] [Green Version]
- Kalinda, C.; Mutengo, M.; Chimbari, M. A meta-analysis of changes in schistosomiasis prevalence in Zambia: Implications on the 2020 elimination target. Parasitol. Res. 2019, 119, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Liese, B.; Rosenberg, M.; Schratz, A. Programmes, partnerships, and governance for elimination and control of neglected tropical diseases. Lancet 2010, 375, 67–76. [Google Scholar] [CrossRef]
- Fenwick, A.; Webster, J.P.; Bosque-Oliva, E.; Blair, L.; Fleming, F.M.; Zhang, Y.; Garba, A.; Stothard, R.; Gabrielli, A.F.; Clements, A.C.A.; et al. The Schistosomiasis Control Initiative (SCI): Rationale, development and implementation from 2002–2008. Parasitology 2009, 136, 1719–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borlase, A.; Webster, J.P.; Rudge, J.W. Opportunities and challenges for modelling epidemiological and evolutionary dynamics in a multihost, multiparasite system: Zoonotic hybrid schistosomiasis in West Africa. Evol. Appl. 2017, 11, 501–515. [Google Scholar] [CrossRef]
- Wharton-Smith, A.; Rassi, C.; Batisso, E.; Ortu, G.; King, R.; Endriyas, M.; Counihan, H.; Hamade, P.; Getachew, D. Gender-related factors affecting health seeking for neglected tropical diseases: Findings from a qualitative study in Ethiopia. PLoS Negl. Trop. Dis. 2019, 13, e0007840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubell, H. Gender, Behavior, and Health: Schistosomiasis Transmission and Control in Rural Egypt (Book Review); The University of Chicago Press: Cairo, Egypt, 2005; pp. 1005–1009. [Google Scholar]
- Aagaard-Hansen, J.; Mwanga, J.R.; Bruun, B. Social science perspectives on schistosomiasis control in Africa: Past trends and future directions. Parasitology 2009, 136, 1747–1758. [Google Scholar] [CrossRef] [PubMed]
- Uniting to Combat Neglected Tropical Diseases. Neglected Tropical Diseases: Women and Girls in Focus. Available online: https://unitingtocombatntds.org/wp-content/uploads/2017/11/women_and_girls_in_focus_english.pdf. (accessed on 2 November 2020).
- Bangert, M.; Molyneux, D.H.; Lindsay, S.W.; Fitzpatrick, C.; Engels, D. The cross-cutting contribution of the end of neglected tropical diseases to the sustainable development goals. Infect. Dis. Poverty 2017, 6, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Amazigo, U.O.; Anago-Amanze, C.I. and Okeibunor, J.C. Urinary schistosomiasis among school children in Nigeria: Consequences of indigenous beliefs and water contact activities. J. Biosoc. Sci. 1997, 29, 9–18. [Google Scholar] [CrossRef]
- Hegertun, I.E.A.; Gundersen, K.M.S.; Kleppa, E.; Zulu, S.G.; Gundersen, S.G.; Taylor, M.; Kvalsvig, J.D.; Kjetland, E.F. S. haematobium as a Common Cause of Genital Morbidity in Girls: A Cross-sectional Study of Children in South Africa. PLoS Negl. Trop. Dis. 2013, 7, e2104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kukula, V.A.; MacPherson, E.E.; Tsey, I.H.; Stothard, J.R.; Theobald, S.; Gyapong, M. A major hurdle in the elimination of urogenital schistosomiasis revealed: Identifying key gaps in knowledge and understanding of female genital schistosomiasis within communities and local health workers. PLoS Negl. Trop. Dis. 2019, 13, e0007207. [Google Scholar] [CrossRef]
- Arnold, M.L. Natural Hybridization and Evolution; Oxford University Press: New York, NY, USA, 1997. [Google Scholar]
- Arnold, M.L. Natural hybridization and the evolution of domesticated, pest and disease organisms. Mol. Ecol. 2004, 13, 997–1007. [Google Scholar] [CrossRef]
- Huyse, T.; Webster, B.; Geldof, S.; Stothard, R.; Diaw, O.T.; Polman, K.; Rollinson, D. Bidirectional Introgressive Hybridization between a Cattle and Human Schistosome Species. PLoS Pathog. 2009, 5, e1000571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tchuenté, L.A.T.; Southgate, V.; Njiokou, F.; Njiné, T.; Kouemeni, L.; Jourdane, J. The evolution of schistosomiasis at Loum, Cameroon: Replacement of Schistosoma intercalatum by S. haematobium through introgressive hybridization. Trans. R. Soc. Trop. Med. Hyg. 1997, 91, 664–665. [Google Scholar] [CrossRef]
- Moné, H.; Holtfreter, M.C.; Allienne, J.-F.; Mintsa-Nguéma, R.; Ibikounle, M.; Boissier, J.; Berry, A.; Mitta, G.; Richter, J.; Mouahid, G. Introgressive hybridizations of Schistosoma haematobium by Schistosoma bovis at the origin of the first case report of schistosomiasis in Corsica (France, Europe). Parasitol. Res. 2015, 114, 4127–4133. [Google Scholar] [CrossRef]
- Southgate, V.R.; Jourdane, J.; Tchuenté, L.A. Recent studies on the reproductive biology of the schistosomes and their relevance to speciation in the Digenea. Int. J. Parasitol. 1998, 28, 1159–1172. [Google Scholar] [CrossRef]
- Wright, C.; Southgate, V.; Knowles, R. What is Schistosoma intercalatum fisher, 1934? Trans. R. Soc. Trop. Med. Hyg. 1972, 66, 28–56. [Google Scholar] [CrossRef]
- Bjørneboe, A.; Frandsen, F. A comparison of the characteristics of two strains of Schistosoma intercalatum Fisher, 1934 in mice. J. Helminthol. 1979, 53, 195–203. [Google Scholar] [CrossRef]
- Frandsen, F. Hybridization between different strains of Schistosoma intercalatum Fisher, 1934 from Cameroun and Zaïre. J. Helminthol. 1978, 52, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.; Southgate, V.; Ross, G. Enzymes in Schistosoma intercalatum and the relative status of the Lower Guinea and Zaire strains of the parasite. Int. J. Parasitol. 1979, 9, 523–528. [Google Scholar] [CrossRef]
- Brown, D.S.; Sarfati, C.; Southgate, V.R.; Ross, G.C.; Knowles, R.J. Observations onSchistosoma intercalatum in south-east gabon. Parasitol. Res. 1984, 70, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Kane, R.A.; Southgate, V.R.; Rollinson, D.; Littlewood, D.T.J.; Lockyer, A.; Pags, J.R.; Tchuent, L.A.T.; Jourdane, J. A phylogeny based on three mitochondrial genes supports the division of Schistosoma intercalatum into two separate species. Parasitology 2003, 127, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Pagès, J.R.; Durand, P.; Southgate, V.R.; Tchuenté, L.A.T.; Jourdane, J. Molecular arguments for splitting of Schistosoma intercalatum, into two distinct species. Parasitol. Res. 2001, 87, 57–62. [Google Scholar] [CrossRef]
- Moné, H.; Minguez, S.; Ibikounlé, M.; Allienne, J.-F.; Massougbodji, A.; Mouahid, G. Natural Interactions between S. haematobium and S. guineensis in the Republic of Benin. Sci. World J. 2012, 2012, 793420. [Google Scholar] [CrossRef] [Green Version]
- Schur, N.; Hürlimann, E.; Stensgaard, A.-S.; Chimfwembe, K.; Mushinge, G.; Simoonga, C.; Kabatereine, N.B.; Kristensen, T.K.; Utzinger, J.; Vounatsou, P. Spatially explicit Schistosoma infection risk in eastern Africa using Bayesian geostatistical modelling. Acta Trop. 2013, 128, 365–377. [Google Scholar] [CrossRef]
- Ekpo, U.F.; Hürlimann, E.; Schur, N.; Oluwole, A.S.; Abe, E.M.; Mafe, M.A.; Nebe, O.J.; Isiyaku, S.; Olamiju, F.; Kadiri, M.; et al. Mapping and prediction of schistosomiasis in Nigeria using compiled survey data and Bayesian geospatial modelling. Geospat. Heal. 2013, 7, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Nguema, R.M.; Mavoungou, J.F.; Ngou-Milama, K.M.M.; Mamfoumbi, M.M.; Koumba, A.A.; Lamine, M.S.; Diarra, A.; Asseko, G.N.; Mourou, J.R.; Akotet, M.K.B.; et al. Baseline Mapping of Schistosomiasis and Soil Transmitted Helminthiasis in the Northern and Eastern Health Regions of Gabon, Central Africa: Recommendations for Preventive Chemotherapy. Trop. Med. Infect. Dis. 2018, 3, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ndukwe, Y.E.; Obiezue, R.N.N.; Aguzie, I.O.N.; Anunobi, J.T.; Okafor, F.C. Mapping of urinary schistosomiasis in Anambra State, Nigeria. Ann. Glob. Health 2019, 85, 52. [Google Scholar] [CrossRef] [Green Version]
- Kabore, A.; Biritwum, N.-K.; Downs, P.W.; Magalhaes, R.J.S.; Zhang, Y.; Ottesen, E.A. Predictive vs. Empiric Assessment of Schistosomiasis: Implications for Treatment Projections in Ghana. PLoS Negl. Trop. Dis. 2013, 7, e2051. [Google Scholar] [CrossRef] [Green Version]
- Ekpo, U.F.; Oluwole, A.S.; Abe, E.M.; Etta, H.E.; Olamiju, F.; Mafiana, C.F.; Ekpo, U. Schistosomiasis in infants and pre-school-aged children in sub-Saharan Africa: Implication for control. Parasitology 2012, 139, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Stothard, J.R.; Gabrielli, A.-F. Schistosomiasis in African infants and preschool children: To treat or not to treat? Trends Parasitol. 2007, 23, 83–86. [Google Scholar] [CrossRef]
- McManus, D.P. Defeating Schistosomiasis. N. Engl. J. Med. 2019, 381, 2567–2568. [Google Scholar] [CrossRef]
- Gray, D.J.; McManus, D.P.; Li, Y.; Williams, G.; Bergquist, R.; Ross, A.G. Schistosomiasis elimination: Lessons from the past guide the future. Lancet Infect. Dis. 2010, 10, 733–736. [Google Scholar] [CrossRef]
- Williams, G.M.; Li, Y.-S.; Gray, D.J.; Zhao, Z.-Y.; Harn, D.A.; Shollenberger, L.M.; Li, S.-M.; Yu, X.; Feng, Z.; Guo, J.-G.; et al. Field Testing Integrated Interventions for Schistosomiasis Elimination in the People’s Republic of China: Outcomes of a Multifactorial Cluster-Randomized Controlled Trial. Front. Immunol. 2019, 10, 645. [Google Scholar] [CrossRef] [Green Version]
- Bergquist, R.; Utzinger, J.; McManus, N.P. Trick or Treat: The Role of Vaccines in Integrated Schistosomiasis Control. PLoS Negl. Trop. Dis. 2008, 2, e244. [Google Scholar] [CrossRef]
- Simoonga, C.; Utzinger, J.; Brooker, S.; Vounatsou, P.; Appleton, C.C.; Stensgaard, A.-S.; Olsen, A.; Kristensen, T.K. Remote sensing, geographical information system and spatial analysis for schistosomiasis epidemiology and ecology in Africa. Parasitology 2009, 136, 1683–1693. [Google Scholar] [CrossRef] [Green Version]
- Walz, Y.; Wegmann, M.; Dech, S.; Raso, G.; Utzinger, J. Risk profiling of schistosomiasis using remote sensing: Approaches, challenges and outlook. Parasites Vectors 2015, 8, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Kulinkina, A.V.; Walz, Y.; Koch, M.; Biritwum, N.-K.; Utzinger, J.; Naumova, E.N. Improving spatial prediction of Schistosoma haematobium prevalence in southern Ghana through new remote sensors and local water access profiles. PLoS Negl. Trop. Dis. 2018, 12, e0006517. [Google Scholar] [CrossRef]
- Schur, N.; Hürlimann, E.; Garba, A.; Traore, M.S.; Ndir, O.; Ratard, R.C.; Tchuenté, L.-A.T.; Kristensen, T.K.; Utzinger, J.; Vounatsou, P. Geostatistical Model-Based Estimates of Schistosomiasis Prevalence among Individuals Aged ≤20 Years in West Africa. PLoS Negl. Trop. Dis. 2011, 5, e1194. [Google Scholar] [CrossRef] [Green Version]
- Wrable, M.; Kulinkina, A.; Liss, A.; Koch, M.; Cruz, M.S.; Biritwum, N.-K.; Ofosu, A.; Gute, D.; Kosinski, K.C.; Naumova, E.N. The use of remotely sensed environmental parameters for spatial and temporal schistosomiasis prediction across climate zones in Ghana. Environ. Monit. Assess. 2019, 191, 301. [Google Scholar] [CrossRef] [Green Version]
- King, C.H.; Bertsch, D. Historical Perspective: Snail Control to Prevent Schistosomiasis. PLoS Negl. Trop. Dis. 2015, 9, e0003657. [Google Scholar] [CrossRef] [Green Version]
- King, C.; Sutherland, L.J.; Bertsch, D. Systematic Review and Meta-analysis of the Impact of Chemical-Based Mollusciciding for Control of Schistosoma mansoni and S. haematobium Transmission. PLoS Negl. Trop. Dis. 2015, 9, e0004290. [Google Scholar] [CrossRef]
- King, C.H.; Sturrock, R.F.; Kariuki, H.C.; Hamburger, J. Transmission control for schistosomiasis – why it matters now. Trends Parasitol. 2006, 22, 575–582. [Google Scholar] [CrossRef]
- Yang, G.-J.; Sun, L.-P.; Hong, Q.-B.; Zhu, H.-R.; Yang, K.; Gao, Q.; Zhou, X.-N. Optimizing molluscicide treatment strategies in different control stages of schistosomiasis in the People’s Republic of China. Parasites Vectors 2012, 5, 260. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, H.; Tsuji, M. From discovery to eradication of schistosomiasis in Japan: 1847–1996. Int. J. Parasitol. 1997, 27, 1465–1480. [Google Scholar] [CrossRef]
- WHO. Molluscicide screening and evaluation. Bull. World Health Organ. 1965, 33, 567–581. [Google Scholar]
- Woolhouse, M.E.J.; Etard, J.-F.; Dietz, K.; Ndhlovu, P.D.; Chandiwana, S.K. Heterogeneities in schistosome transmission dynamics and control. Parasitology 1998, 117, 475–482. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.N.; Bergquist, R.; Leonardo, L.; Yang, G.J.; Yang, K.; Sudomo, M.; Olveda, R. Schistosomiasis japonica control and research needs. Adv. Parasitol. 2010, 72, 145–178. [Google Scholar]
- Minggang, C.; Zheng, F. Schistosomiasis control in China. Parasitol. Int. 1999, 48, 11–19. [Google Scholar] [CrossRef]
- Knopp, S.; Ame, S.M.; Person, B.; Hattendorf, J.; Rabone, M.; Juma, S.; Muhsin, J.; Khamis, I.S.; Hollenberg, E.; Mohammed, K.A.; et al. A 5-Year intervention study on elimination of urogenital schistosomiasis in Zanzibar: Parasitological results of annual cross-sectional surveys. PLoS Negl. Trop. Dis. 2019, 13, e0007268. [Google Scholar] [CrossRef] [Green Version]
- Lo, N.C.; Gurarie, D.; Yoon, N.; Coulibaly, J.T.; Bendavid, E.; Andrews, J.R.; King, C. Impact and cost-effectiveness of snail control to achieve disease control targets for schistosomiasis. Proc. Natl. Acad. Sci. 2018, 115, E584–E591. [Google Scholar] [CrossRef] [Green Version]
- Person, B.; Ali, S.M.; A’Kadir, F.M.; Ali, J.N.; Mohammed, U.A.; Mohammed, K.A.; Rollinson, D.; Knopp, S. Community Knowledge, Perceptions, and Practices Associated with Urogenital Schistosomiasis among School-Aged Children in Zanzibar, United Republic of Tanzania. PLoS Negl. Trop. Dis. 2016, 10, e0004814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stothard, R.; French, M.D.; Khamis, I.S.; Basáñez, M.-G.; Rollinson, D. The epidemiology and control of urinary schistosomiasis and soil-transmitted helminthiasis in schoolchildren on Unguja Island, Zanzibar. Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 1031–1044. [Google Scholar] [CrossRef] [PubMed]
- Stothard, J.R.; Mook, P.; Mgeni, A.F.; Khamis, I.S.; Khamis, A.N.; Rollinson, D. Control of urinary schistosomiasis on Zanzibar (Unguja Island): A pilot evaluation of the educational impact of the Juma na Kichocho health booklet within primary schools. Memórias Do Instituto Oswaldo Cruz 2006, 101, 119–124. [Google Scholar] [CrossRef]
- Savioli, L.; Dixon, H.; Kisumku, U.M.; E Mott, K. Control of morbidity due to Schistosoma haematobium on Pemba Island: Programme organization and management. Trop. Med. Parasitol. Off. Organ Dtsch. Tropenmedizinische Ges. Dtsch. Ges. fur Tech. Zusammenarbeit (GTZ) 1989, 40, 189–194. [Google Scholar]
- Ejike, C.U.; Oluwole, A.S.; Mogaji, H.O.; Adeniran, A.A.; Alabi, O.M.; Ekpo, U.F. Development and testing of Schisto and Ladders™, an innovative health educational game for control of schistosomiasis in schoolchildren. BMC Res. Notes 2017, 10, 1–9. [Google Scholar] [CrossRef]
- Adeneye, A.; Akinwale, O.; Idowu, E.; Adewale, B.; Manafa, O.; Sulyman, M.; Omotola, B.; Akande, D.; Mafe, M.; Appelt, B. Sociocultural aspects of mass delivery of praziquantel in schistosomiasis control: The Abeokuta experience. Res. Soc. Adm. Pharm. 2007, 3, 183–198. [Google Scholar] [CrossRef] [PubMed]
- John, R.; Ezekiel, M.; Philbert, C.; Andrew, A. Schistosomiasis transmission at high altitude crater lakes in Western Uganda. BMC Infect. Dis. 2008, 8, 110. [Google Scholar] [CrossRef] [Green Version]
- Hewlett, B.S.; Cline, B.L. Anthropological contributions to a community-based schistosomiasis control project in northern Cameroun. Trop. Med. Int. Health 1997, 2, 25–36. [Google Scholar]
- Mangal, T.D.; Paterson, S.; Fenton, A. Predicting the Impact of Long-Term Temperature Changes on the Epidemiology and Control of Schistosomiasis: A Mechanistic Model. PLoS ONE 2008, 3, e1438. [Google Scholar] [CrossRef] [Green Version]
- Stensgaard, A.-S.; Utzinger, J.; Vounatsou, P.; Hürlimann, E.; Schur, N.; Saarnak, C.F.L.; Simoonga, C.; Mubita, P.; Kabatereine, N.B.; Tchuenté, L.-A.T.; et al. Large-scale determinants of intestinal schistosomiasis and intermediate host snail distribution across Africa: Does climate matter? Acta Trop. 2013, 128, 378–390. [Google Scholar] [CrossRef]
- Monde, C.; Syampungani, S.; Brink, P.J.V.D. Natural and human induced factors influencing the abundance of Schistosoma host snails in Zambia. Environ. Monit. Assess. 2016, 188, 370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCreesh, N.; Nikulin, G.; Booth, M. Predicting the effects of climate change on Schistosoma mansoni transmission in eastern Africa. Parasites Vectors 2015, 8, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCreesh, N.; Arinaitwe, M.; Arineitwe, W.; Tukahebwa, E.M.; Booth, M. Effect of water temperature and population density on the population dynamics of Schistosoma mansoni intermediate host snails. Parasites Vectors 2014, 7, 503. [Google Scholar] [CrossRef] [PubMed]
- McCreesh, N.; Booth, M. The Effect of Simulating Different Intermediate Host Snail Species on the Link between Water Temperature and Schistosomiasis Risk. PLoS ONE 2014, 9, e87892. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, U.B.; Karagiannis-Voules, D.-A.; Midzi, N.; Mduluza, T.; Mukaratirwa, S.; Fensholt, R.; Vennervald, B.J.; Kristensen, T.K.; Vounatsou, P.; Stensgaard, A.-S. Comparison of the spatial patterns of schistosomiasis in Zimbabwe at two points in time, spaced twenty-nine years apart: Is climate variability of importance? Geospat. Health 2017, 12, 505. [Google Scholar] [CrossRef] [Green Version]
- Midzi, N.; Mtapuri-Zinyowera, S.; Mapingure, M.P.; Paul, N.H.; Sangweme, D.; Hlerema, G.; Mutsaka, M.J.; Tongogara, F.; Makware, G.; Chadukura, V.; et al. Knowledge attitudes and practices of grade three primary schoolchildren in relation to schistosomiasis, soil transmitted helminthiasis and malaria in Zimbabwe. BMC Infect. Dis. 2011, 11, 169. [Google Scholar] [CrossRef] [Green Version]
- Mekonnen, A.; Legesse, M.; Belay, M.; Tadesse, K.; Torben, W.; Teklemariam, Z.; Erko, B. Efficacy of Praziquantel against Schistosoma haematobium in Dulshatalo village, western Ethiopia. BMC Res. Notes 2013, 6, 392. [Google Scholar] [CrossRef] [Green Version]
- Kabatereine, N.B.; Brooker, S.; Tukahebwa, E.M.; Kazibwe, F.; Onapa, A.W. Epidemiology and geography of Schistosoma mansoni in Uganda: Implications for planning control. Trop. Med. Int. Heal. 2004, 9, 372–380. [Google Scholar] [CrossRef] [Green Version]
- Olivier, T.J.; Handy, K.Q.; Bauer, R.T. Effects of river control structures on the juvenile migration ofMacrobrachium ohione. Freshw. Biol. 2013, 58, 1603–1613. [Google Scholar] [CrossRef]
- Hunter, J.M. Parasitic Diseases in Water Resources Development: The Need for Intersectoral Negotiation; World Health Organization: Geneva, Swizterland, 1993. [Google Scholar]
- Jobin, W.R. Dams and Disease: Ecological Design and Health Impacts of Large Dams, Canals, and Irrigation Systems; E & FN Spon.: London, UK; New York, NY, USA, 1999. [Google Scholar]
- Swartz, S.J.; De Leo, G.A.; Wood, C.L.; Sokolow, S.H. Infection with schistosome parasites in snails leads to increased predation by prawns: Implications for human schistosomiasis control. J. Exp. Biol. 2015, 218, 3962–3967. [Google Scholar] [CrossRef] [Green Version]
- Sokolow, S.H.; Lafferty, K.D.; Kuris, A.M. Regulation of laboratory populations of snails (Biomphalaria and Bulinus spp.) by river prawns, Macrobrachium spp. (Decapoda, Palaemonidae): Implications for control of schistosomiasis. Acta Trop. 2014, 132, 64–74. [Google Scholar] [CrossRef] [Green Version]
- Diakité, N.R.; Winkler, M.S.; Coulibaly, J.T.; Guindo-Coulibaly, N.; Utzinger, J.; N’Goran, E.K. Dynamics of freshwater snails and Schistosoma infection prevalence in schoolchildren during the construction and operation of a multipurpose dam in central Côte d’Ivoire. Infect. Dis. Poverty 2017, 6, 1–9. [Google Scholar] [CrossRef]
- Martínez, B.B.; Talavera, J.R.; Robayna, A.A.; Valencia, A.C.; Morales, N.O.; García, L.G.; Pérez, M.S.C.; Pisaca, M.F.R. Parasitic Hematuria: Six Cases in a Row in a Single Centre in Spain. Urol. Int. 2017, 102, 360–363. [Google Scholar] [CrossRef]
- Cetron, M.S.; Chitsulo, L.; Sullivan, J.J.; Pilcher, J.; Wilson, M.; Noh, J.; Tsang, V.C.; Hightower, A.W.; Addiss, D.G. Schistosomiasis in Lake Malawi. Lancet 1996, 348, 1274–1278. [Google Scholar] [CrossRef]
- Visser, L.G.; Polderman, A.M.; Stuiver, P.C. Outbreak of Schistosomiasis Among Travelers Returning from Mali, West Africa. Clin. Infect. Dis. 1995, 20, 280–285. [Google Scholar] [CrossRef]
- Zuidema, P.J. The Katayama syndrome; an outbreak in Dutch tourists to the Omo National Park, Ethiopia. Trop. Geogr. Med. 1981, 33, 30–35. [Google Scholar]
- Istre, G.R.; Fontaine, R.E.; Tarr, J.; Hopkins, R.S. Acute Schistosomiasis Among Americans Rafting the Omo River, Ethiopia. JAMA 1984, 251, 508–510. [Google Scholar] [CrossRef]
- Elcuaz, R.; Armas, M.; Ramírez, M.; Noguera, F.J.; Bolaños, M.; Quiñones, I.; Lafarga, B. Outbreak of schistosomiasis in a group a travellers returning from Burkina Faso. Enferm. Infecc. Microbiol. Clin. 1998, 16, 367–369. [Google Scholar]
- Luque, A.; Díaz, L.; Martos, S.; Sánchez, L.; Fernández, A.; Chamorro, M. Imported diseases in Spain: Difficulties in health care. Enfermería Global 2019, 18, 595–607. [Google Scholar]
- Berry, A.; Moné, H.; Iriart, X.; Mouahid, G.; Abbo, O.; Boissier, J.; Fillaux, J.; Cassaing, S.; Debuisson, C.; Valentin, A.; et al. Schistosomiasis Haematobium, Corsica, France. Emerg. Infect. Dis. 2014, 20, 1595–1597. [Google Scholar] [CrossRef]
- Holtfreter, M.C.; Moné, H.; Müller-Stöver, I.; Mouahid, G.; Richter, J. Schistosoma haematobium infections acquired in Corsica, France, August 2013. Eurosurveillance 2014, 19, 20821. [Google Scholar] [CrossRef] [Green Version]
- Calvo-Cano, A.; Cnops, L.; Huyse, T.; Van Lieshout, L.; Pardos, J.; Valls, M.E.; Franco, A.; Rollinson, D.; Gascon, J. A Case of Urogenital Human Schistosomiasis from a Non-endemic Area. PLoS Negl. Trop. Dis. 2015, 9, e0004053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roure, S.; Valerio, L.; Pérez-Quílez, O.; Fernández-Rivas, G.; Martínez-Cuevas, O.; Alcántara-Román, A.; Viasus, D.; Pedro-Botet, M.L.; Sabrià, M.; Clotet, B. Epidemiological, clinical, diagnostic and economic features of an immigrant population of chronic schistosomiasis sufferers with long-term residence in a non-endemic country (North Metropolitan area of Barcelona, 2002–2016). PLoS ONE 2017, 12, e0185245. [Google Scholar] [CrossRef] [Green Version]
- WHO. COID-19: WHO Issues Interim Guidance for Implementation of NTD Programmes. Available online: https://www.who.int/neglected_diseases/news/COVID19-WHO-interim-guidance-implementation-NTD-programmes/en/ (accessed on 7 September 2020).
- Mackee, N. COVID Fears Drive Patients to Avoid Doctors, Hospitals. Available online: https://insightplus.mja.com.au/2020/17/covid-19-avoiding-doctors-clinicians-brace-for-wave-of-severe-illnesses/ (accessed on 7 September 2020).
- Solomon, M.D.; McNulty, E.J.; Rana, J.S.; Leong, T.K.; Lee, C.; Sung, S.-H.; Ambrosy, A.P.; Sidney, S.; Go, A.S. The Covid-19 Pandemic and the Incidence of Acute Myocardial Infarction. N. Engl. J. Med. 2020, 383, 691–693. [Google Scholar] [CrossRef]
- Hafner, K. Fear of Covid-19 Leads Other Patients to Decline Critical Treatment, in New York Times; PPSNet: New York, NY, USA, 2020. [Google Scholar]
- Siripanthong, B.; Hanff, T.C.; Levin, M.G.; Vidula, M.K.; Khanji, M.Y.; Nazarian, S.; A Chahal, C.A. Coronavirus disease 2019 is delaying the diagnosis and management of chest pain, acute coronary syndromes, myocarditis and heart failure. Futur. Cardiol. 2021, 17, 3–6. [Google Scholar] [CrossRef]
- Oyeyemi, O.T.; Okunlola, O.A.; Adebayo, A.D. Assessment of schistosomiasis endemicity and preventive treatment on coronavirus disease 2019 outcomes in Africa. New Microbes New Infect. 2020, 38, 100821. [Google Scholar] [CrossRef]
- Kayuni, S.A.; O’Ferrall, A.M.; Baxter, H.; Hesketh, J.; Mainga, B.; Lally, D.; Al-Harbi, M.H.; LaCourse, E.J.; Juziwelo, L.; Musaya, J.; et al. An outbreak of intestinal schistosomiasis, alongside increasing urogenital schistosomiasis prevalence, in primary school children on the shoreline of Lake Malawi, Mangochi District, Malawi. Infect. Dis. Poverty 2020, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Hillyer, J.F. Parasites and Parasitology in this SARS-CoV-2, COVID-19 World: An American Society of Parasitologists Presidential Address. J. Parasitol. 2020, 106, 859–868. [Google Scholar] [CrossRef] [PubMed]
- Gutman, J.R.; Lucchi, N.W.; Cantey, P.T.; Steinhardt, L.C.; Samuels, A.M.; Kamb, M.L.; Kapella, B.K.; McElroy, P.D.; Udhayakumar, V.; Lindblade, K.A. Malaria and Parasitic Neglected Tropical Diseases: Potential Syndemics with COVID-19? Am. J. Trop. Med. Hyg. 2020, 103, 572–577. [Google Scholar] [CrossRef] [PubMed]
- King, C.H.; Dickman, K.; Tisch, D.J. Reassessment of the cost of chronic helmintic infection: A meta-analysis of disability-related outcomes in endemic schistosomiasis. Lancet 2005, 365, 1561–1569. [Google Scholar] [CrossRef]


{kind=link}
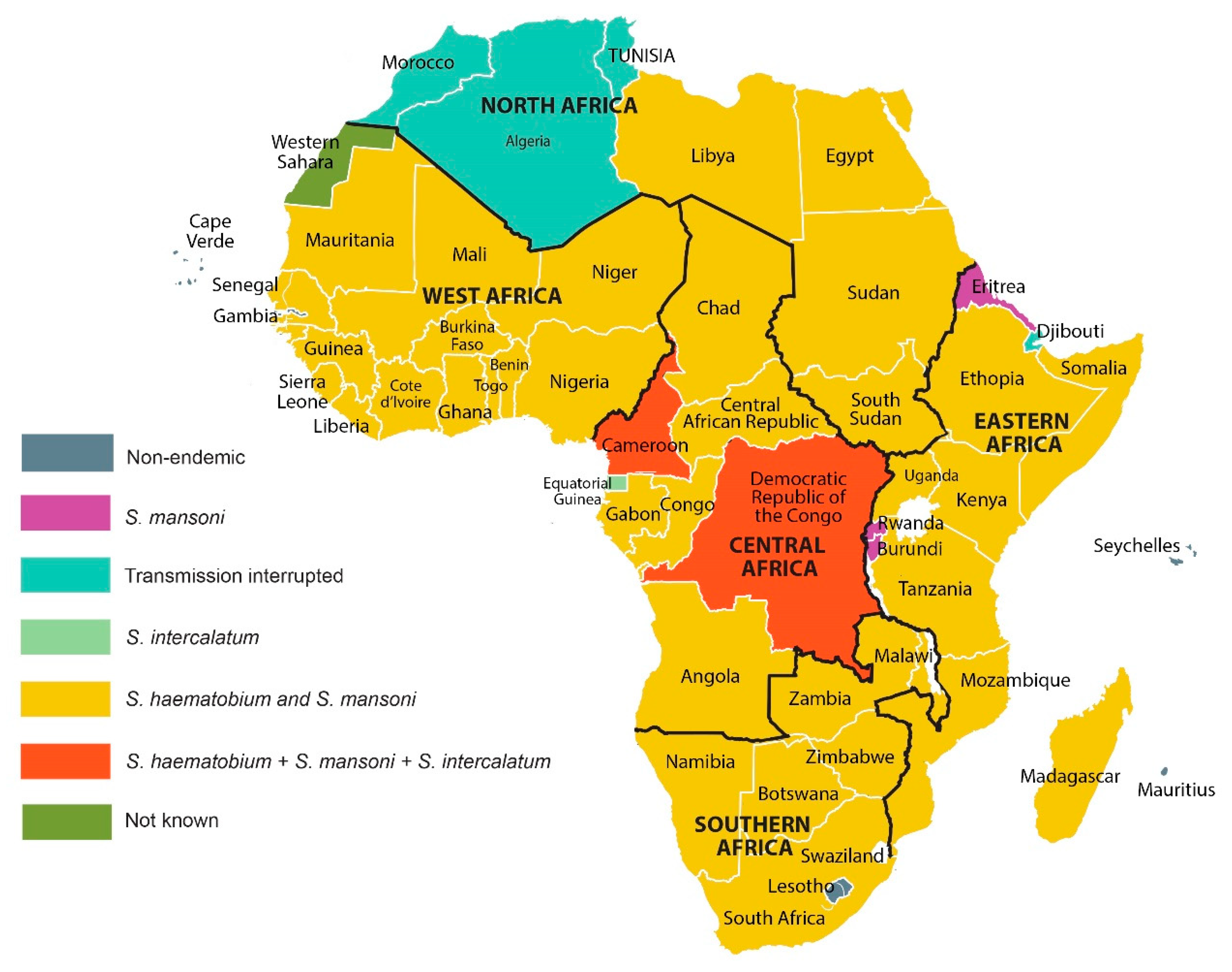{kind=link}
| Species | Intermediate Host | Definitive Hosts | Site of Infection | Geographical Distribution | References | |
|---|---|---|---|---|---|---|
| Intestinal schistosomiasis | S. mansoni | Biomphalari spp. | Humans, rodents | Intestinal mesenteric veins | Sub-Saharan Africa, Madagascar, the Middle East, the Caribbean, South America | [1,10] |
| S. intercalatum and S. guineensis | Bulinus spp. | Humans, non-human primates (excluding apes) | Intestinal mesenteric veins | Central Africa, West Africa, Madagascar | [1,10,11] | |
| Urogenital schistosomiasis | S. haematobium | Bulinus spp. | Humans, non-human primates (excluding apes) | Urogenital veins | Sub-Saharan Africa, the Middle East, Corsica (France) | [1,10] |
| Animal intestinal schistosomiasis | S. mattheei | Bulinus spp. | Cattle, sheep, goats | Intestinal mesenteric veins | Southeastern and Central Africa | [12,13,14,15] |
| S. curassoni | Bulinus spp. | Cattle, sheep, goats | Intestinal mesenteric veins | West Africa | [12,13,14,15] | |
| S. bovis | Bulinus spp. | Cattle, goats, sheep, horses, camels, pigs | Intestinal mesenteric veins | North, East, West and Central Africa, the Middle East and Mediterranean (Europe) region | [12,13,14,15] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aula, O.P.; McManus, D.P.; Jones, M.K.; Gordon, C.A. Schistosomiasis with a Focus on Africa. Trop. Med. Infect. Dis. 2021, 6, 109. https://doi.org/10.3390/tropicalmed6030109
Aula OP, McManus DP, Jones MK, Gordon CA. Schistosomiasis with a Focus on Africa. Tropical Medicine and Infectious Disease. 2021; 6(3):109. https://doi.org/10.3390/tropicalmed6030109
Chicago/Turabian StyleAula, Oyime Poise, Donald P. McManus, Malcolm K. Jones, and Catherine A. Gordon. 2021. "Schistosomiasis with a Focus on Africa" Tropical Medicine and Infectious Disease 6, no. 3: 109. https://doi.org/10.3390/tropicalmed6030109
APA StyleAula, O. P., McManus, D. P., Jones, M. K., & Gordon, C. A. (2021). Schistosomiasis with a Focus on Africa. Tropical Medicine and Infectious Disease, 6(3), 109. https://doi.org/10.3390/tropicalmed6030109