
The Usefulness of Peripheral Blood Cell Counts to Distinguish COVID-19 from Dengue during Acute Infection

 ,
,  ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Definitions
2.4. Statistical Analysis
2.5. Ethics Approval
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weekly Epidemiological Update on COVID-19. 16 March 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update---16-march-2021 (accessed on 23 March 2021).
- Clinical Management of COVID-19. Available online: https://www.who.int/publications-detail-redirect/clinical-management-of-covid-19 (accessed on 28 November 2020).
- Wilder-Smith, A.; Ooi, E.-E.; Horstick, O.; Wills, B. Dengue. Lancet 2019, 393, 350–363. [Google Scholar] [CrossRef]
- Sánchez-De La Cruz, J.P.; Tovilla-Zárate, C.A.; González-Morales, D.L.; González-Castro, T.B. Risk of a Syndemic between COVID-19 and Dengue Fever in Southern Mexico. Gac. Med. Mex. 2020, 156, 460–464. [Google Scholar] [CrossRef]
- Vicente, C.R.; Silva, T.C.C.D.; Pereira, L.D.; Miranda, A.E. Impact of Concurrent Epidemics of Dengue, Chikungunya, Zika, and COVID-19. Rev. Soc. Bras. Med. Trop. 2021, 54. [Google Scholar] [CrossRef]
- Muller, D.A.; Depelsenaire, A.C.I.; Young, P.R. Clinical and Laboratory Diagnosis of Dengue Virus Infection. J. Infect. Dis. 2017, 215, S89–S95. [Google Scholar] [CrossRef]
- Nacher, M.; Douine, M.; Gaillet, M.; Flamand, C.; Rousset, D.; Rousseau, C.; Mahdaoui, C.; Carroll, S.; Valdes, A.; Passard, N.; et al. Simultaneous Dengue and COVID-19 Epidemics: Difficult Days Ahead? PLoS Negl. Trop. Dis. 2020, 14, e0008426. [Google Scholar] [CrossRef]
- Rhee, C.; Kanjilal, S.; Baker, M.; Klompas, M. Duration of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infectivity: When Is It Safe to Discontinue Isolation? Clin. Infect. Dis. 2021, 72, 1467–1474. [Google Scholar] [CrossRef]
- Milby, K.M.; Atallah, A.N.; Rocha-Filho, C.R.; Pinto, A.C.P.N.; Rocha, A.P.D.; Reis, F.S.D.A.; Carvas Junior, N.; Civile, V.T.; Santos, R.R.P.; Ferla, L.J.; et al. SARS-CoV-2 and Arbovirus Infection: A Rapid Systematic Review. Sao Paulo Med. J. 2020, 138, 498–504. [Google Scholar] [CrossRef]
- Yan, G.; Lee, C.K.; Lam, L.T.M.; Yan, B.; Chua, Y.X.; Lim, A.Y.N.; Phang, K.F.; Kew, G.S.; Teng, H.; Ngai, C.H.; et al. Covert COVID-19 and False-Positive Dengue Serology in Singapore. Lancet Infect. Dis. 2020, 20, 536. [Google Scholar] [CrossRef] [Green Version]
- Epidemiological Update: Arboviruses in the Context of COVID-19—2 July 2021—PAHO/WHO|Pan American Health Organization. Available online: https://www.paho.org/en/documents/epidemiological-update-arboviruses-context-covid-19-2-july-2021 (accessed on 1 November 2021).
- Joob, B.; Wiwanitkit, V. COVID-19 Can Present with a Rash and Be Mistaken for Dengue. J. Am. Acad. Dermatol. 2020, 82, e177. [Google Scholar] [CrossRef]
- Joob, B.; Wiwanitkit, V. COVID-19 in Medical Personnel: Observation from Thailand. J. Hosp. Infect. 2020, 104, 453. [Google Scholar] [CrossRef]
- Wee, L.E.; Cherng, B.P.Z.; Conceicao, E.P.; Goh, K.C.-M.; Wan, W.Y.; Ko, K.K.K.; Aung, M.K.; Sim, X.Y.J.; Wijaya, L.; Ling, M.L.; et al. Experience of a Tertiary Hospital in Singapore with Management of a Dual Outbreak of COVID-19 and Dengue. Am. J. Trop. Med. Hyg. 2020, 103, 2005–2011. [Google Scholar] [CrossRef] [PubMed]
- Lokida, D.; Lukman, N.; Salim, G.; Butar-butar, D.P.; Kosasih, H.; Wulan, W.N.; Naysilla, A.M.; Djajady, Y.; Sari, R.A.; Arlinda, D.; et al. Diagnosis of COVID-19 in a Dengue-Endemic Area. Am. J. Trop. Med. Hyg. 2020, 103, 1220–1222. [Google Scholar] [CrossRef] [PubMed]
- Kularatnam, G.A.M.; Jasinge, E.; Gunasena, S.; Samaranayake, D.; Senanayake, M.P.; Wickramasinghe, V.P. Evaluation of Biochemical and Haematological Changes in Dengue Fever and Dengue Hemorrhagic Fever in Sri Lankan Children: A Prospective Follow up Study. BMC Pediatrics 2019, 19, 87. [Google Scholar] [CrossRef] [Green Version]
- Dussart, P.; Duong, V.; Bleakley, K.; Fortas, C.; Try, P.L.; Kim, K.S.; Choeung, R.; In, S.; Andries, A.-C.; Cantaert, T.; et al. Comparison of Dengue Case Classification Schemes and Evaluation of Biological Changes in Different Dengue Clinical Patterns in a Longitudinal Follow-up of Hospitalized Children in Cambodia. PLoS Negl. Trop. Dis. 2020, 14, e0008603. [Google Scholar] [CrossRef]
- Rafi, A.; Mousumi, A.N.; Ahmed, R.; Chowdhury, R.H.; Wadood, A.; Hossain, G. Dengue Epidemic in a Non-Endemic Zone of Bangladesh: Clinical and Laboratory Profiles of Patients. PLoS Negl. Trop. Dis. 2020, 14, e0008567. [Google Scholar] [CrossRef]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Elalamy, I.; Kastritis, E.; Sergentanis, T.N.; Politou, M.; Psaltopoulou, T.; Gerotziafas, G.; Dimopoulos, M.A. Hematological Findings and Complications of COVID-19. Am. J. Hematol. 2020, 95, 834–847. [Google Scholar] [CrossRef] [Green Version]
- Gallo Marin, B.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 Severity: A Literature Review. Rev. Med. Virol. 2021, 31, e2146. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Ryan, M.; Yohan, B.; Abidin, R.S.; Nainu, F.; Rakib, A.; Jahan, I.; Emran, T.B.; Ullah, I.; Panta, K.; et al. COVID-19 and Dengue: Double Punches for Dengue-Endemic Countries in Asia. Rev. Med. Virol. 2021, 31, e2161. [Google Scholar] [CrossRef]
- Kantri, A.; Ziati, J.; Khalis, M.; Haoudar, A.; Aidaoui, K.E.; Daoudi, Y.; Chikhaoui, I.; Yamani, K.E.; Mouhaoui, M.; Bakkouri, J.E.; et al. Hematological and Biochemical Abnormalities Associated with Severe Forms of COVID-19: A Retrospective Single-Center Study from Morocco. PLoS ONE 2021, 16, e0246295. [Google Scholar] [CrossRef]
- Fois, A.G.; Paliogiannis, P.; Scano, V.; Cau, S.; Babudieri, S.; Perra, R.; Ruzzittu, G.; Zinellu, E.; Pirina, P.; Carru, C.; et al. The Systemic Inflammation Index on Admission Predicts In-Hospital Mortality in COVID-19 Patients. Molecules 2020, 25, 5725. [Google Scholar] [CrossRef]
- Qu, R.; Ling, Y.; Zhang, Y.; Wei, L.; Chen, X.; Li, X.; Liu, X.; Liu, H.; Guo, Z.; Ren, H.; et al. Platelet-to-Lymphocyte Ratio Is Associated with Prognosis in Patients with Coronavirus Disease-19. J. Med. Virol. 2020, 92, 1533–1541. [Google Scholar] [CrossRef]
- Wang, X.; Li, X.; Shang, Y.; Wang, J.; Zhang, X.; Su, D.; Zhao, S.; Wang, Q.; Liu, L.; Li, Y.; et al. Ratios of Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Predict All-Cause Mortality in Inpatients with Coronavirus Disease 2019 (COVID-19): A Retrospective Cohort Study in a Single Medical Centre. Epidemiol. Infect. 2020, 148. [Google Scholar] [CrossRef]
- Yang, A.-P.; Liu, J.; Tao, W.; Li, H. The Diagnostic and Predictive Role of NLR, d-NLR and PLR in COVID-19 Patients. Int. Immunopharmacol. 2020, 84, 106504. [Google Scholar] [CrossRef]
- Diagnosis and Treatment Protocol for Novel Coronavirus Pneumonia (Trial Version 7). Chin. Med. J. 2020, 133, 1087–1095. [CrossRef]
- Sánchez-Leyva, M.; Sánchez-Zazueta, J.G.; Osuna-Ramos, J.F.; Rendón-Aguilar, H.; Félix-Espinoza, R.; Becerra-Loaiza, D.S.; Sánchez-García, D.C.; Romero-Quintana, J.G.; Castillo Ureta, H.; Velarde-Rodríguez, I.; et al. Genetic Polymorphisms of Tumor Necrosis Factor Alpha and Susceptibility to Dengue Virus Infection in a Mexican Population. Viral. Immunol. 2017, 30, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Special Programme for Research and Training in Tropical Diseases, World Health Organization (Ed.) Dengue: Guidelines for Diagnosis, Treatment, Prevention, and Control, New ed.; World Health Organization: Geneva, Switzerland, 2009; ISBN 978-92-4-154787-1.
- Li, Y.; Zou, Z.; Zhang, Y.; Zhu, B.; Ning, Y.; Shen, B.; Wang, C.; Luo, Z.; Xu, J.; Ding, X. Dynamics in Perioperative Neutrophil-to-Lymphocyte*platelet Ratio as a Predictor of Early Acute Kidney Injury Following Cardiovascular Surgery. Ren. Fail. 2021, 43, 1012–1019. [Google Scholar] [CrossRef]
- Sommer, P.; Lukovic, E.; Fagley, E.; Long, D.R.; Sobol, J.B.; Heller, K.; Moitra, V.K.; Pauldine, R.; O’Connor, M.F.; Shahul, S.; et al. Initial Clinical Impressions of the Critical Care of COVID-19 Patients in Seattle, New York City, and Chicago. Anesth. Analg. 2020, 131, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Nasomsong, W.; Luvira, V.; Phiboonbanakit, D. Case Report: Dengue and COVID-19 Coinfection in Thailand. Am. J. Trop. Med. Hyg. 2020, 104, 487–489. [Google Scholar] [CrossRef]
- Hilmy, A.I.; Dey, R.K.; Imad, H.A.; Yoosuf, A.A.; Nazeem, A.; Latheef, A.A. Coronavirus Disease 2019 and Dengue: Two Case Reports. J. Med. Case Rep. 2021, 15, 171. [Google Scholar] [CrossRef]
- Reyes-Ruiz, J.M.; Campuzano-Vences, R.; Osuna-Ramos, J.F.; De Jesús-González, L.A.; Pérez-Méndez, M.J.; González-González, C.; Farfan-Morales, C.N.; Rivas-Tovar, L.; Dávila-González, E.; María Del Ángel, R.; et al. Case Report: Extrapulmonary Manifestations of COVID-19 and Dengue Coinfection. Am. J. Trop. Med. Hyg. 2021, 105. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; Gallego, V.; Escalera-Antezana, J.P.; Méndez, C.A.; Zambrano, L.I.; Franco-Paredes, C.; Suárez, J.A.; Rodriguez-Enciso, H.D.; Balbin-Ramon, G.J.; Savio-Larriera, E.; et al. COVID-19 in Latin America: The Implications of the First Confirmed Case in Brazil. Travel Med. Infect. Dis. 2020, 35, 101613. [Google Scholar] [CrossRef] [PubMed]
- Rosso, F.; Parra-Lara, L.G.; Agudelo-Rojas, O.L.; Martinez-Ruiz, D.M. Differentiating Dengue from COVID-19: Comparison of Cases in Colombia. Am. J. Trop. Med. Hyg. 2021, 105, 745–750. [Google Scholar] [CrossRef]
- Mandrekar, J.N. Receiver Operating Characteristic Curve in Diagnostic Test Assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [Green Version]
- Cavalcante-Silva, L.H.A.; Carvalho, D.C.M.; de Almeida Lima, É; Galvão, J.G.; da Silva, J.S.D.F.; de Sales-Neto, J.M.; Rodrigues-Mascarenhas, S. Neutrophils and COVID-19: The Road so Far. Int. Immunopharmacol. 2021, 90, 107233. [Google Scholar] [CrossRef] [PubMed]
- Cui, S.-N.; Tan, H.-Y.; Fan, G.-C. Immunopathological Roles of Neutrophils in Virus Infection and COVID-19. Shock 2021, 56, 345. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.D.; Malachowa, N.; DeLeo, F.R. Influence of Microbes on Neutrophil Life and Death. Front. Cell Infect. Microbiol. 2017, 7, 159. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Z.; Ren, L.; Zhang, L.; Zhong, J.; Xiao, Y.; Jia, Z.; Guo, L.; Yang, J.; Wang, C.; Jiang, S.; et al. Heightened Innate Immune Responses in the Respiratory Tract of COVID-19 Patients. Cell Host Microbe 2020, 27, 883–890.e2. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Núñez, I.; Priego-Ranero, Á.A.; García-González, H.B.; Jiménez-Franco, B.; Bonilla-Hernández, R.; Domínguez-Cherit, G.; Merayo-Chalico, J.; Crispín, J.C.; Barrera-Vargas, A.; Valdés-Ferrer, S.I. Common Hematological Values Predict Unfavorable Outcomes in Hospitalized COVID-19 Patients. Clin. Immunol. 2021, 225, 108682. [Google Scholar] [CrossRef]
- Vafadar Moradi, E.; Teimouri, A.; Rezaee, R.; Morovatdar, N.; Foroughian, M.; Layegh, P.; Rezvani Kakhki, B.; Ahmadi Koupaei, S.R.; Ghorani, V. Increased Age, Neutrophil-to-Lymphocyte Ratio (NLR) and White Blood Cells Count Are Associated with Higher COVID-19 Mortality. Am. J. Emerg. Med. 2021, 40, 11–14. [Google Scholar] [CrossRef]
- Liu, Y.; Du, X.; Chen, J.; Jin, Y.; Peng, L.; Wang, H.H.X.; Luo, M.; Chen, L.; Zhao, Y. Neutrophil-to-Lymphocyte Ratio as an Independent Risk Factor for Mortality in Hospitalized Patients with COVID-19. J. Infect. 2020, 81, e6–e12. [Google Scholar] [CrossRef]
- Lin, H.-A.; Lin, S.-F.; Chang, H.-W.; Lee, Y.-J.; Chen, R.-J.; Hou, S.-K. Clinical Impact of Monocyte Distribution Width and Neutrophil-to-Lymphocyte Ratio for Distinguishing COVID-19 and Influenza from Other Upper Respiratory Tract Infections: A Pilot Study. PLoS ONE 2020, 15, e0241262. [Google Scholar] [CrossRef]
- Wang, J.; Li, Q.; Yin, Y.; Zhang, Y.; Cao, Y.; Lin, X.; Huang, L.; Hoffmann, D.; Lu, M.; Qiu, Y. Excessive Neutrophils and Neutrophil Extracellular Traps in COVID-19. Front. Immunol. 2020, 11, 2063. [Google Scholar] [CrossRef]
- Forget, P.; Khalifa, C.; Defour, J.-P.; Latinne, D.; Van Pel, M.-C.; De Kock, M. What Is the Normal Value of the Neutrophil-to-Lymphocyte Ratio? BMC Res. Notes 2017, 10, 12. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Hou, H.; Diao, J.; Wang, Y.; Yang, H. Neutrophil-to-Lymphocyte Ratio Is Independently Associated with COVID-19 Severity: An Updated Meta-Analysis Based on Adjusted Effect Estimates. Int. J. Lab. Hematol. 2021, 43. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Liu, Y.; Xiang, P.; Pu, L.; Xiong, H.; Li, C.; Zhang, M.; Tan, J.; Xu, Y.; Song, R.; et al. Neutrophil-to-Lymphocyte Ratio Predicts Critical Illness Patients with 2019 Coronavirus Disease in the Early Stage. J. Transl. Med. 2020, 18, 206. [Google Scholar] [CrossRef]
- Ralapanawa, U.; Alawattegama, A.T.M.; Gunrathne, M.; Tennakoon, S.; Kularatne, S.A.M.; Jayalath, T. Value of Peripheral Blood Count for Dengue Severity Prediction. BMC Res. Notes 2018, 11, 400. [Google Scholar] [CrossRef] [PubMed]
- Cox, D. Targeting SARS-CoV-2-Platelet Interactions in COVID-19 and Vaccine-Related Thrombosis. Front Pharm. 2021, 12, 708665. [Google Scholar] [CrossRef]
- Yang, X.; Yang, Q.; Wang, Y.; Wu, Y.; Xu, J.; Yu, Y.; Shang, Y. Thrombocytopenia and Its Association with Mortality in Patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1469–1472. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M.; Henry, B.M. Thrombocytopenia Is Associated with Severe Coronavirus Disease 2019 (COVID-19) Infections: A Meta-Analysis. Clin. Chim. Acta 2020, 506, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Figliozzi, S.; Masci, P.G.; Ahmadi, N.; Tondi, L.; Koutli, E.; Aimo, A.; Stamatelopoulos, K.; Dimopoulos, M.-A.; Caforio, A.L.P.; Georgiopoulos, G. Predictors of Adverse Prognosis in COVID-19: A Systematic Review and Meta-Analysis. Eur. J. Clin. Investig. 2020, 50, e13362. [Google Scholar] [CrossRef] [PubMed]
- Kawada, T. Platelet Count in Patients with Severe Coronavirus Disease 2019. EXCLI J. 2021, 20, 17–18. [Google Scholar] [CrossRef] [PubMed]
- Halstead, S.B.; Katzelnick, L. COVID-19 Vaccines: Should We Fear ADE? J. Infect. Dis. 2020, 222, 1946–1950. [Google Scholar] [CrossRef] [PubMed]
- Maemura, T.; Kuroda, M.; Armbrust, T.; Yamayoshi, S.; Halfmann, P.J.; Kawaoka, Y. Antibody-Dependent Enhancement of SARS-CoV-2 Infection Is Mediated by the IgG Receptors FcγRIIA and FcγRIIIA but Does Not Contribute to Aberrant Cytokine Production by Macrophages. mBio 2021, 12, e0198721. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Overall, N = 288 * | COVID-19, n = 105 * | Dengue, n = 183 * | p-Value |
|---|---|---|---|---|
| Gender | <0.001 | |||
| Female | 163 (57) | 41 (39) | 122 (67) | |
| Male | 125 (43) | 64 (61) | 61 (33) | |
| Age | 40.0 (27.2) | 56.0 (22.0) | 33.0 (21.0) | <0.001 |
| Severity | ||||
| Non-Critical | 105 (36) | 105 (100) | 0 (0) | <0.001 |
| Non-Severe | 183 (64) | 0 (0) | 183 (100) | |
| Day after Symptom Onset | 4 (3) | 7 (5.5) | 4 (2) | <0.001 |
| Fever | 267 (93) | 85 (81) | 182 (99) | <0.001 |
| Headache | 210 (73) | 76 (72) | 134 (73) | ns |
| Myalgya | 218 (76) | 57 (54) | 161 (88) | <0.001 |
| Arthralgia | 228 (79) | 59 (56) | 169 (92) | <0.001 |
| Univariate | Multivariate | |||||||
|---|---|---|---|---|---|---|---|---|
| Coeff | OR | 95% CI | p-value | Coeff | OR | 95% CI | p-Value | |
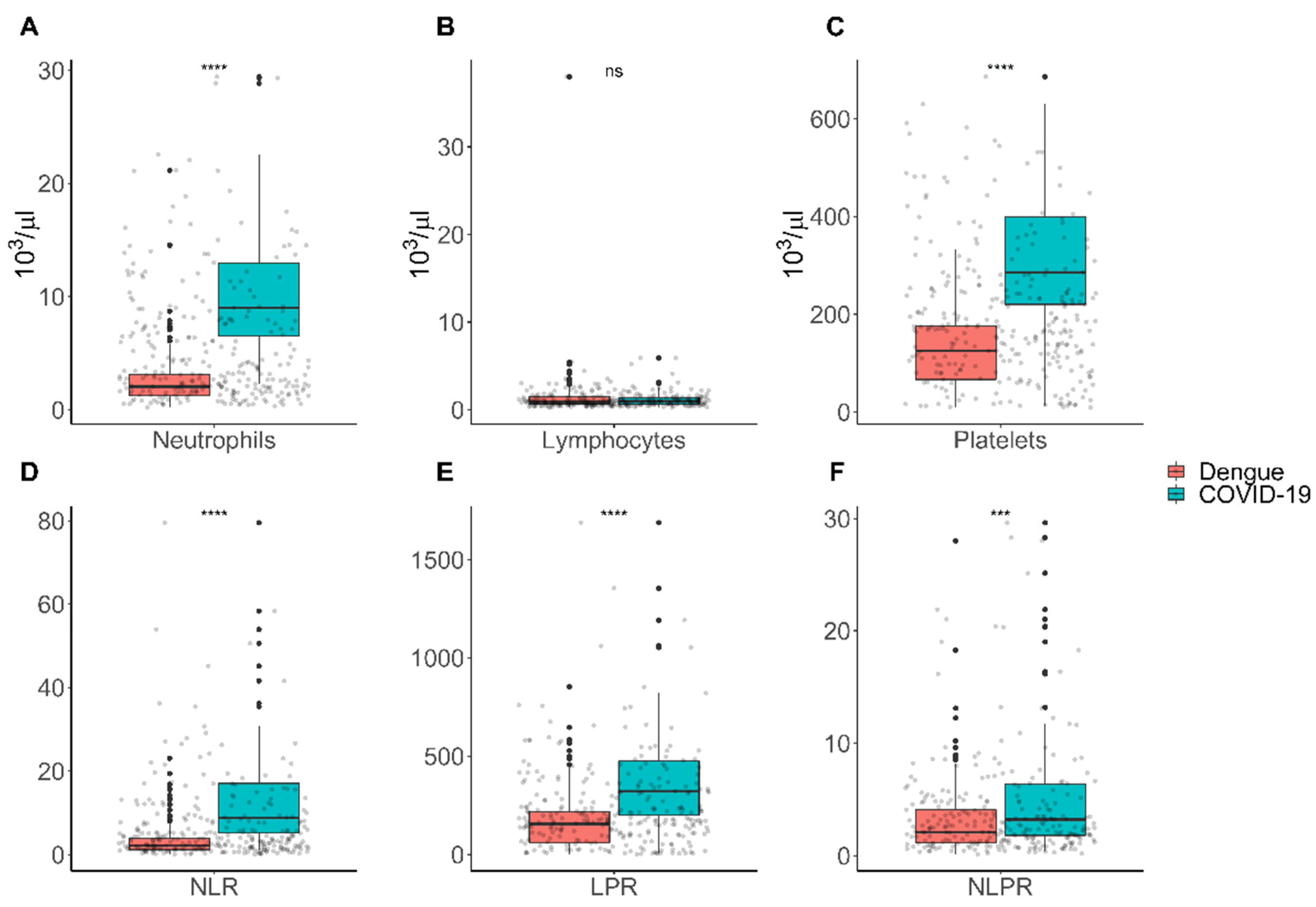
| Neutrophils | 0.54 | 1.72 | 1.50–1.99 | <0.0001 | 0.27 | 1.31 | 1.03–1.67 | 0.0260 |
| Lymphocytes | −0.07 | 0.93 | 0.79–1.09 | 0.3858 | −0.20 | 0.81 | 0.39–1.72 | 0.5904 |
| Platelets | 0.01 | 1.01 | 1.01–1.02 | <0.0001 | 0.02 | 1.02 | 1.01–1.03 | <0.0001 |
| NLR | 0.22 | 1.25 | 1.166–1.34 | <0.0001 | −0.025 | 0.97 | 0.80–1.19 | 0.8051 |
| PLR | 0.006 | 1.00 | 1.00–1.00 | <0.001 | −0.002 | 0.99 | 0.99–1.00 | 0.3579 |
| NLPR | 0.05 | 1.05 | 0.99–1.13 | 0.0895 | 0.192 | 1.21 | 1.05–1.39 | 0.0074 |
| AUC | 95% CI | Cut-Off Point | p-Value | Sens % | Spec % | |
|---|---|---|---|---|---|---|
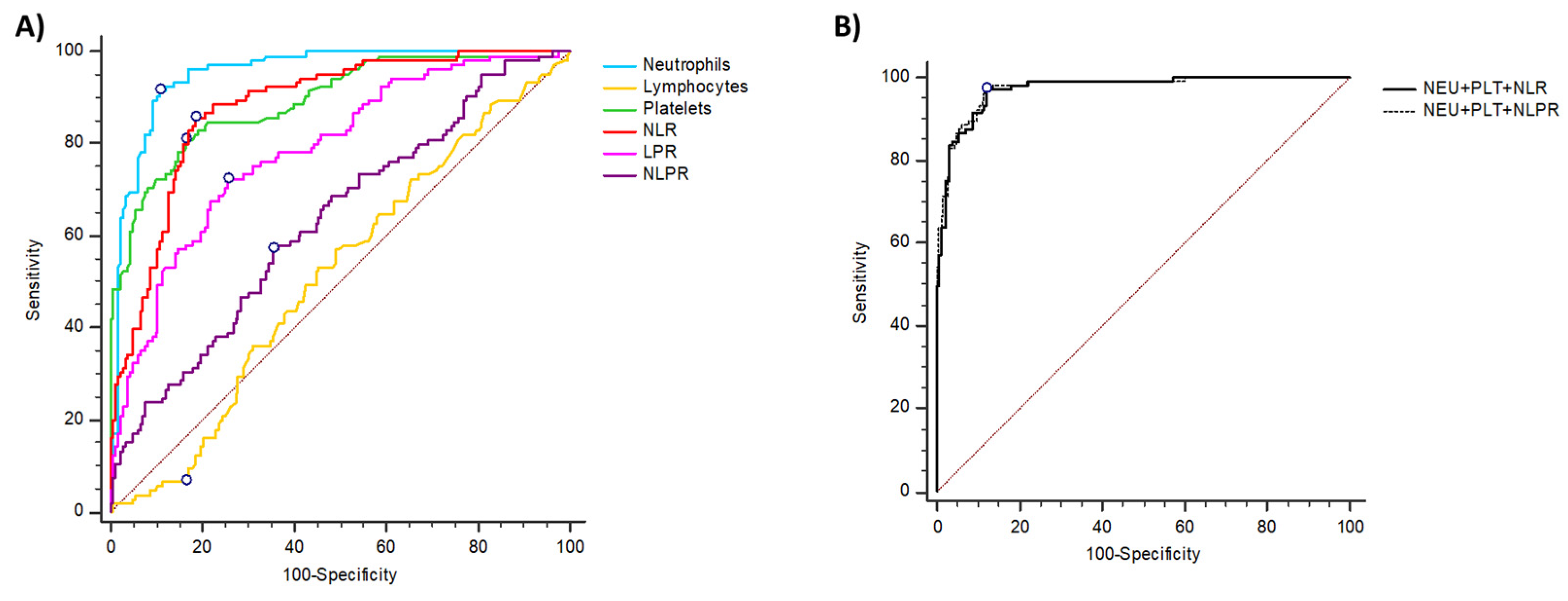
| Neutrophils | 0.95 | 0.92–0.97 | 4.39 | <0.0001 | 91.4 | 89.1 |
| Lymphocytes | 0.51 | 0.45–0.57 | 2.14 | 0.6740 | 6.7 | 83.6 |
| Platelets | 0.89 | 0.85–0.93 | 198 | <0.0001 | 81 | 83.6 |
| NLR | 0.88 | 0.84–0.91 | 4.42 | <0.0001 | 85.71 | 81.42 |
| PLR | 0.78 | 0.73–0.83 | 213.46 | <0.0001 | 72.4 | 74.3 |
| NLPR | 0.63 | 0.57–0.69 | 2.91 | 0.0001 | 57.14 | 64.48 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osuna-Ramos, J.F.; Reyes-Ruiz, J.M.; Ochoa-Ramírez, L.A.; De Jesús-González, L.A.; Ramos-Payán, R.; Farfan-Morales, C.N.; Romero-Utrilla, A.; Ríos-Burgueño, E.R.; Rodríguez-Millán, J.; del Ángel, R.M.; et al. The Usefulness of Peripheral Blood Cell Counts to Distinguish COVID-19 from Dengue during Acute Infection. Trop. Med. Infect. Dis. 2022, 7, 20. https://doi.org/10.3390/tropicalmed7020020
Osuna-Ramos JF, Reyes-Ruiz JM, Ochoa-Ramírez LA, De Jesús-González LA, Ramos-Payán R, Farfan-Morales CN, Romero-Utrilla A, Ríos-Burgueño ER, Rodríguez-Millán J, del Ángel RM, et al. The Usefulness of Peripheral Blood Cell Counts to Distinguish COVID-19 from Dengue during Acute Infection. Tropical Medicine and Infectious Disease. 2022; 7(2):20. https://doi.org/10.3390/tropicalmed7020020
Chicago/Turabian StyleOsuna-Ramos, Juan Fidel, José Manuel Reyes-Ruiz, Luis Antonio Ochoa-Ramírez, Luis Adrián De Jesús-González, Rosalío Ramos-Payán, Carlos Noe Farfan-Morales, Alejandra Romero-Utrilla, Efrén Rafael Ríos-Burgueño, José Rodríguez-Millán, Rosa María del Ángel, and et al. 2022. "The Usefulness of Peripheral Blood Cell Counts to Distinguish COVID-19 from Dengue during Acute Infection" Tropical Medicine and Infectious Disease 7, no. 2: 20. https://doi.org/10.3390/tropicalmed7020020
APA StyleOsuna-Ramos, J. F., Reyes-Ruiz, J. M., Ochoa-Ramírez, L. A., De Jesús-González, L. A., Ramos-Payán, R., Farfan-Morales, C. N., Romero-Utrilla, A., Ríos-Burgueño, E. R., Rodríguez-Millán, J., del Ángel, R. M., & Velarde-Félix, J. S. (2022). The Usefulness of Peripheral Blood Cell Counts to Distinguish COVID-19 from Dengue during Acute Infection. Tropical Medicine and Infectious Disease, 7(2), 20. https://doi.org/10.3390/tropicalmed7020020