
Associations between Bonus and Lottery COVID-19 Vaccine Incentive Policies and Increases in COVID-19 Vaccination Rates: A Social Epidemiologic Analysis


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Associations between COVID-19 Vaccine Incentive Policies and County-Level Vaccination Rates
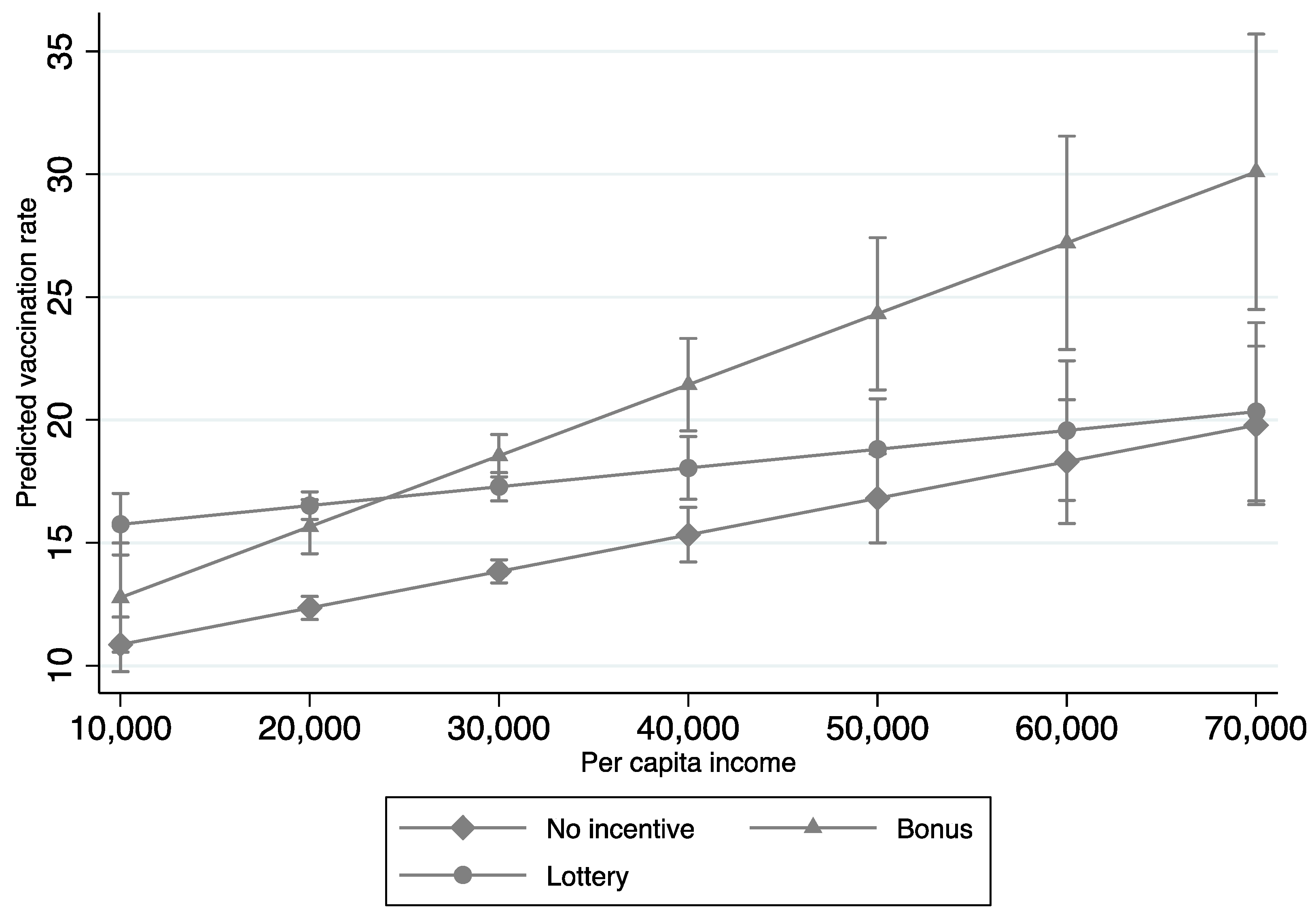
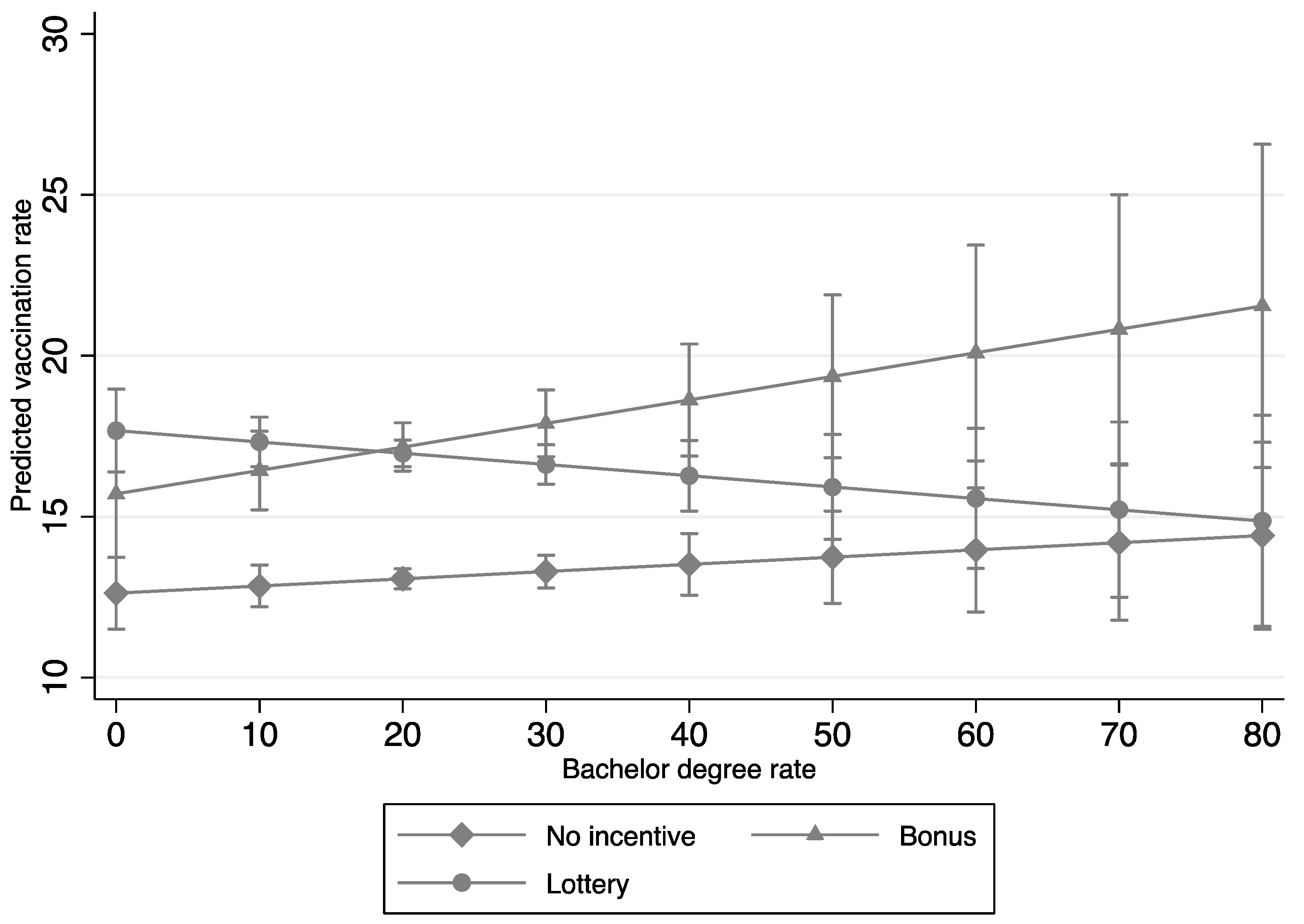
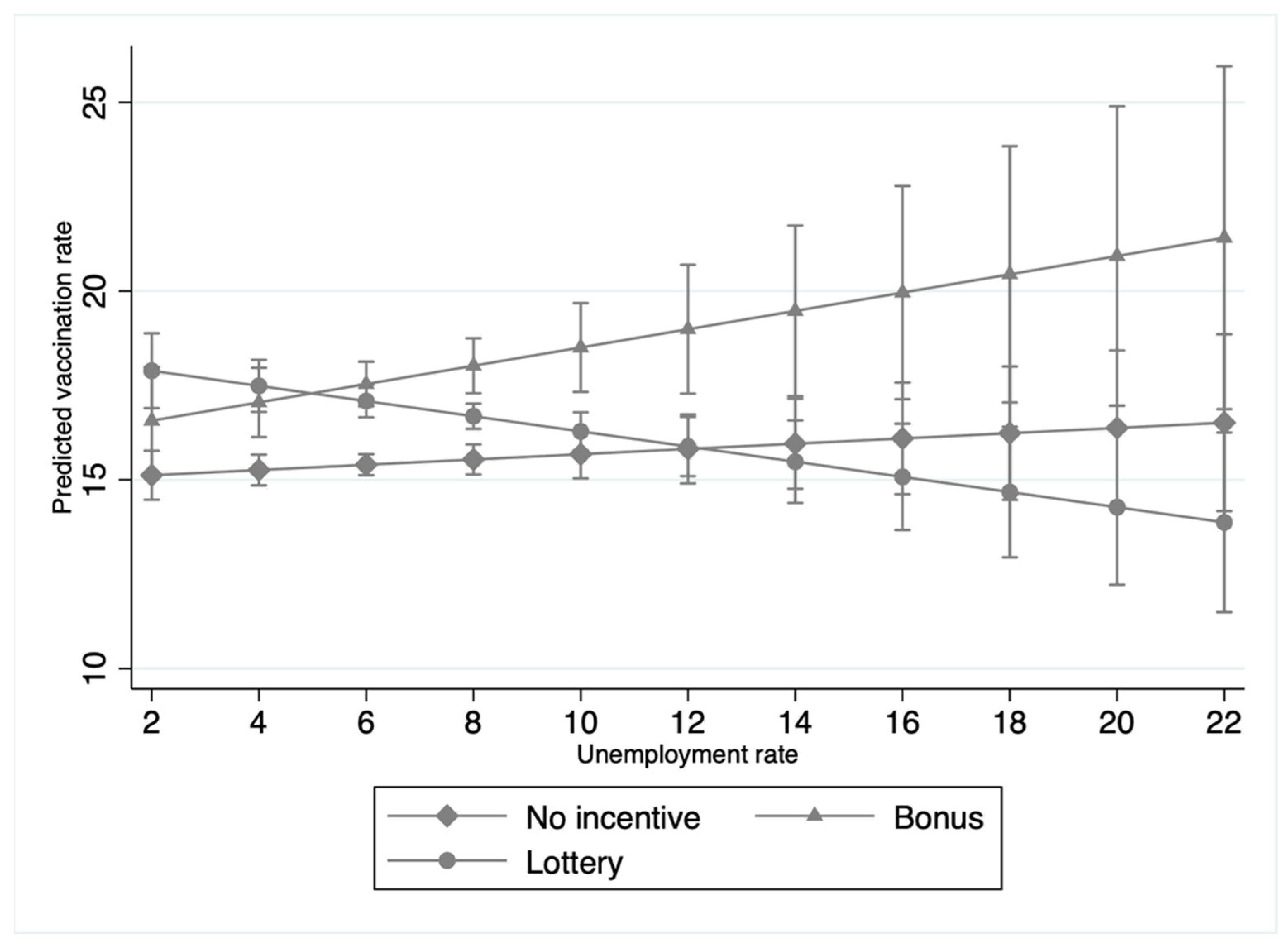
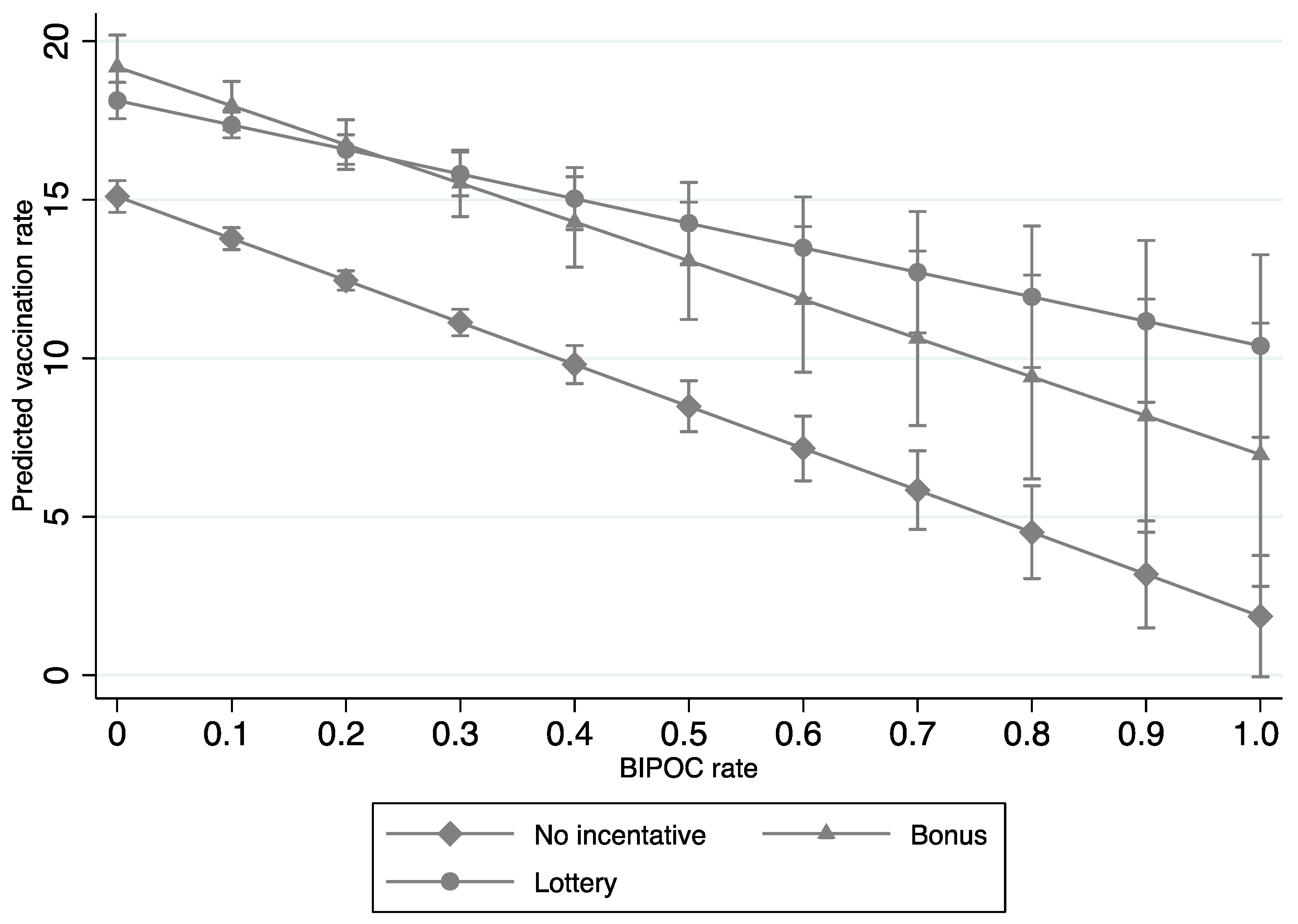
3.2. Interaction Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- CDC. COVID Data Tracker. Available online: https://covid.cdc.gov/covid-data-tracker/#datatracker-home (accessed on 23 March 2022).
- Tregoning, J.S.; Flight, K.E.; Higham, S.L.; Wang, Z.; Pierce, B.F. Progress of the COVID-19 vaccine effort: viruses, vaccines and variants versus efficacy, effectiveness and escape. Nat. Rev. Immunol. 2021, 21, 626–636. [Google Scholar] [CrossRef] [PubMed]
- Bernal, J.L.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 Vaccines against the B.1.617.2 Variant. Available online: https://www.medrxiv.org/content/10.1101/2021.05.22.21257658v1 (accessed on 20 June 2022). [CrossRef]
- RRosenberg, E.S.; Dorabawila, V.; Easton, D.; Bauer, U.E.; Kumar, J.; Hoen, R.; Hoefer, D.; Wu, M.; Lutterloh, E.; Conroy, M.B.; et al. COVID-19 Vaccine Effectiveness in New York State. N. Engl. J. Med. 2022, 386, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Nunes, B.; Rodrigues, A.P.; Kislaya, I.; Cruz, C.; Peralta-Santos, A.; Lima, J.; Leite, P.P.; Sequeira, D.; Dias, C.M.; Machado, A. mRNA vaccine effectiveness against COVID-19-related hospitalisations and deaths in older adults: A cohort study based on data linkage of national health registries in Portugal, February to August 2021. Eurosurveillance 2021, 26, 2100833. [Google Scholar] [CrossRef]
- Oliver, S. Updates to the Evidence to Recommendation Framework: Pfizer-BioNTech and Moderna COVID-19 Vaccine Booster Doses. Available online: https://www.cdc.gov/vaccines/acip/meetings/slides-2021-09-22-23.html (accessed on 23 March 2022).
- Brehm, M.E.; Brehm, P.A.; Saavedra, M. The Ohio Vaccine Lottery and Starting Vaccination Rates. Am. Soc. Health Econoomists 2021. Available online: https://www.journals.uchicago.edu/doi/abs/10.1086/718512?journalCode=ajhe (accessed on 25 June 2022). [CrossRef]
- Robertson, C.; Schaefer, K.A.; Scheitrum, D. Are vaccine lotteries worth the money? Econ. Lett. 2021, 209, 110097. [Google Scholar] [CrossRef]
- Lang, D.; Esbenshade, L.; Willer, R. Did Ohio’s Vaccine Lottery Increase Vaccination Rates? A Pre-Registered, Synthetic Control Study. J. Exp. Political Sci. 2022, 1–19. Available online: https://www.cambridge.org/core/journals/journal-of-experimental-political-science/article/did-ohios-vaccine-lottery-increase-vaccination-rates-a-preregistered-synthetic-control-study/07720E0BB974962FE4547FF2BCC71CAC (accessed on 25 June 2022). [CrossRef]
- Barber, A.; West, J. Conditional cash lotteries increase COVID-19 vaccination rates. J. Health Econ. 2022, 81, 102578. [Google Scholar] [CrossRef]
- Sehgal, N.K.R. Impact of Vax-a-Million Lottery on COVID-19 Vaccination Rates in Ohio. Am. J. Med. 2021, 134, 1424–1426. [Google Scholar] [CrossRef]
- Pérez-Stable, E.J. Author Affiliations: National Institute on Minority Health and Health Disparities. Natl. Inst. Health 2021, 109, S16–S20. [Google Scholar] [CrossRef]
- Mallow, P.J.; Enis, A.; Wackler, M.; Hooker, E.A. COVID-19 financial lottery effect on vaccine hesitant areas: Results from Ohio’s Vax-a-million program. Am. J. Emerg. Med. 2022, 56, 316–317. [Google Scholar] [CrossRef]
- Thirumurthy, H.; Milkman, K.L.; Volpp, K.; Buttenheim, A.; Pope, D.G. Association between Statewide Financial Incentive Programs and COVID-19 Vaccination Rates. PLoS ONE 2022, 17, e0263425. [Google Scholar] [CrossRef] [PubMed]
- Bronfenbrenner, U. Ecological systems theory. In Encyclopedia of Psychology; Jessica Kingsley Publishers: London, UK, 2004; Volume 3. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Ecological models of human development. Int. Encycl. Educ. 1994, 3, 37–43. [Google Scholar]
- Downs, J.S.; Bruine De Bruin, W.; Fischhoff, B. Parents’ vaccination comprehension and decisions. Vaccine 2008, 26, 1595–1607. [Google Scholar] [CrossRef] [PubMed]
- Endrich, M.M.; Blank, P.R.; Szucs, T.D. Influenza vaccination uptake and socioeconomic determinants in 11 European countries. Vaccine 2009, 27, 4018–4024. [Google Scholar] [CrossRef] [PubMed]
- Singleton, J.A.; Santibanez, T.A.; Wortley, P.M. Influenza and Pneumococcal Vaccination of Adults Aged >65 Racial/Ethnic Differences. Am. J. Prev. Med. 2005, 29, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Lu, P.J.; O’Halloran, A.; Williams, W.W.; Lindley, M.C.; Farrall, S.; Bridges, C.B. Racial and ethnic disparities in vaccination coverage among adult populations in the U.S. Vaccine 2015, 33, D83–D91. [Google Scholar] [CrossRef]
- Wong, C.A.; Dowler, S.; Moore, A.F.; Sosne, E.F.; Young, H.; Tenenbaum, J.D.; Burns, C.E.; Jones, S.; Smelyanskaya, M.; Kinsley, K.H. COVID-19 Vaccine Administration, by Race and Ethnicity—North Carolina, December 14, 2020–April 6, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 991–996. [Google Scholar] [CrossRef]
- Debus, M.; Tosun, J. Political ideology and vaccination willingness: implications for policy design. Policy Sci. 2021, 54, 477–491. [Google Scholar] [CrossRef]
- Agarwal, R.; Dugas, M.; Ramaprasad, J.; Luo, J.; Li, G.; Gao, G. Socioeconomic privilege and political ideology are associated with racial disparity in COVID-19 vaccination. Proc. Natl. Acad. Sci. USA 2021, 118, 2107873118. [Google Scholar] [CrossRef]
- COVID-19 Vaccine Incentives—National Governors Association. Available online: https://www.nga.org/center/publications/covid-19-vaccine-incentives/ (accessed on 22 April 2022).
- Biden Approval Rating Continues to Slide among Democrats|Pew Research Center. Available online: https://www.pewresearch.org/politics/2022/01/25/views-of-joe-biden/ (accessed on 22 April 2022).
- Census.gov. Available online: https://www.census.gov/en.html (accessed on 22 April 2022).
- ACIP COVID-19 Vaccine Recommendations|CDC. Available online: https://www.cdc.gov/vaccines/hcp/acip-recs/vacc-specific/covid-19.html (accessed on 22 April 2022).
- Fogg, B.J. A Behavior Model for Persuasive Design. 2009. Available online: www.bjfogg.com (accessed on 11 April 2022).
- Salali, G.D.; Uysal, M.S. Psychological Medicine Effective incentives for increasing COVID-19 vaccine uptake. Psychol. Med. 2021, 20, 1–3. [Google Scholar] [CrossRef]
- Law, A.C.; Peterson, D.; Walkey, A.J.; Bosch, N.A. Lottery-Based Incentives and COVID-19 Vaccination Rates in the US. JAMA Intern. Med. 2022, 182, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Walkey, A.J.; Law, A.; Bosch, N.A. Lottery-Based Incentive in Ohio and COVID-19 Vaccination Rates. JAMA 2021, 326, 766–767. [Google Scholar] [CrossRef] [PubMed]
- Acharya, B.; Dhakal, C. Implementation of State Vaccine Incentive Lottery Programs and Uptake of COVID-19 Vaccinations in the United States. JAMA Netw. Open. 2021, 4, e2138238. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency (n) | Percentage (%) | Mean | Std. Dev. | Min | Max |
|---|---|---|---|---|---|---|
| Panel time range | 1 Jan 2021 | 1 Jul 2021 | ||||
| Rate of vaccinated population per county | 16.14 | 15.20 | 0.00 | 99.90 | ||
| Incentive policies: | ||||||
| No incentives | 10,367 | 51.84 | ||||
| Bonus incentives | 2233 | 11.17 | ||||
| Lottery incentives | 7399 | 37.00 | ||||
| Number of days of implementation of incentive policies | 2.46 | 8.90 | 0.00 | 55.00 | ||
| ACIP VRS Phasing: | ||||||
| Followed the ACIP VRS | 13,972 | 64.16 | ||||
| Slowly expanded the ACIP VRS | 448 | 2.06 | ||||
| Quickly expanded the ACIP VRS | 7357 | 33.78 | ||||
| Number of days that COVID-19 vaccines were available to the general population | 25.07 | 33.18 | 0.00 | 107.00 | ||
| Biden support rate | 0.34 | 0.16 | 0.05 | 0.92.00 | ||
| Number of nurse practitioners | 54.29 | 15,45.66 | 0.23 | 3937.77 | ||
| Unemployment rate | 6.71 | 2.23 | 1.70 | 22.50 | ||
| Per capita income | 25,074.69 | 5999.78 | 9688.43 | 66,518.36 | ||
| Percentage of adults with a bachelor’s degree | 21.82 | 9.55 | 5.40 | 78.50 | ||
| Rate of BIPOC | 0.15 | 0.16 | 0.01 | 0.94 | ||
| Percentage of people aged 65 and above | 0.19 | 0.05 | 0.00 | 0.58 |
| Variables | Mean | Std. Dev. | Min | Max | Observations | |
|---|---|---|---|---|---|---|
| Rate of COVID-19 vaccination | overall | 16.14 | 15.20 | 0.00 | 99.90 | N = 19,999 |
| between | 6.00 | 0.00 | 61.14 | n = 2857 | ||
| within | 13.97 | −45.01 | 62.94 | T = 7 | ||
| Number of days that COVID-19 vaccines were available to the general population | overall | 25.07 | 33.18 | 0.00 | 107.00 | N = 19,999 |
| between | 3.57 | 18.29 | 35.14 | n = 2857 | ||
| within | 32.99 | −10.07 | 96.93 | T = 7 | ||
| Number of days of implementation of incentive policies | overall | 2.46 | 8.90 | 0.00 | 55.00 | N = 19,999 |
| between | 3.45 | 0.00 | 11.43 | n = 2857 | ||
| within | 8.20 | −8.97 | 46.03 | T = 7 | ||
| ACIP VRS phasing | overall | 0.76 | 0.96 | 0.00 | 2.00 | N = 19,999 |
| between | 0.96 | 0.00 | 2.00 | n = 2857 | ||
| within | 0 | 0.76 | 0.76 | T = 7 | ||
| Biden support rate | overall | 0.34 | 0.16 | 0.05 | 0.92 | N = 19,999 |
| between | 0.16 | 0.05 | 0.92 | n = 2857 | ||
| within | 0.00 | 0.34 | 0.34 | T = 7 | ||
| Number of nurse practitioners | overall | 54.29 | 155.66 | 0.23 | 3937.77 | N = 19,999 |
| between | 155.68 | 0.23 | 3937.77 | n = 2857 | ||
| within | 0.00 | 54.29 | 54.29 | T = 7 | ||
| Unemployment rate | overall | 6.71 | 2.23 | 1.70 | 22.5 | N = 19,999 |
| between | 2.23 | 1.70 | 22.5 | n = 2857 | ||
| within | 0.00 | 6.71 | 6.71 | T = 7 | ||
| Per capita income | overall | 25,074.69 | 5999.80 | 9688.43 | 66,518.36 | N = 19,999 |
| between | 6000.70 | 9688.43 | 66,518.36 | n = 2857 | ||
| within | 0.00 | 25,074.69 | 25,074.69 | T = 7 | ||
| Percentage of adults with a bachelor’s degree | overall | 21.82 | 9.55 | 5.40 | 78.50 | N = 19,999 |
| between | 9.55 | 5.40 | 78.50 | n = 2857 | ||
| within | 0.00 | 21.82 | 21.81 | T = 7 | ||
| Rate of BIPOC populations | overall | 0.16 | 0.16 | 0.01 | 0.94 | N = 19,992 |
| between | 0.16 | 0.01 | 0.94 | n = 2856 | ||
| within | 0.00 | 0.16 | 0.15 | T = 7 | ||
| Percentage of people aged 65 and above | overall | 0.19 | 0.05 | 0.00 | 0.58 | N = 19,999 |
| between | 0.05 | 0.00 | 0.58 | n = 2857 | ||
| within | 0.00 | 0.19 | 0.19 | T = 7 |
| Random Effects | ||||||
|---|---|---|---|---|---|---|
| Variables (DV = County Level COVID-19 Vaccination Rate) | (1) Pooled OLS | (2) Initial | (3) Per Capita Income | (4) Percentage of Adults with a Bachelor’s Degree | (5) Unemployment Rate 2020 | (6) Percentage of BIPOC |
| Bonus incentive policies | 2.230 *** | 2.281 *** | −0.798 | 0.764 | 1.101 | 1.641 *** |
| Lottery incentive policies | 1.343 *** | 1.376 *** | 1.497 | 1.284 * | 3.310 *** | −0.116 |
| Slowly expanded the ACIP VRS | 0.324 | 0.300 | 0.257 | 0.298 | 0.349 | −1.385 |
| Quickly expanded the ACIP VRS | −1.084 *** | −1.078 *** | −1.068 *** | −1.062 *** | −1.168 *** | −0.986 *** |
| Number of nurse practitioners | 0.00279 *** | 0.00279 *** | 0.00277 *** | 0.00276 *** | 0.00297 *** | 0.00196 ** |
| Unemployment rates | −0.0160 | −0.0169 | −0.0287 | −0.0245 | 0.0696 | 0.0251 |
| Per capita income | 0.000159 *** | 0.000159 *** | 0.000146 *** | 0.000156 *** | 0.000159 *** | 0.000144 *** |
| Percentage of adults with bachelor’s degrees | −0.0153 | −0.0155 | −0.0154 | −0.0247 | −0.0165 | −0.0121 |
| Rate of BIPOC | −15.04 *** | −15.04 *** | −15.01 *** | −15.13 *** | −15.38 *** | −18.23 *** |
| Percentage of people aged 65 and above | 17.73 *** | 17.73 *** | 17.87 *** | 17.81 *** | 17.60 *** | 16.89 *** |
| Biden support rate | 19.66 *** | 19.67 *** | 19.71 *** | 19.79 *** | 19.59 *** | 19.63 *** |
| Bonus × Per capita income | 0.000120 * | |||||
| Lottery × Per capita income | −0.0000001 | |||||
| Bonus × Percentage of adults with a bachelor’s degree | 0.0691 * | |||||
| Lottery × Percentage of adults with a bachelor’s degree | 0.00465 | |||||
| Bonus × Unemployment rates | 0.173 | |||||
| Lottery × Unemployment rates | −0.270 * | |||||
| Bonus × Rate of BIPOC populations | 4.168 * | |||||
| Lottery × Rate of BIPOC populations | 10.44 *** | |||||
| Constant | −4.363 *** | −4.418 *** | −4.063 *** | −4.147 *** | −4.790 *** | −3.663 *** |
| Observations | 19,992 | 19,992 | 19,992 | 19,992 | 19,992 | 19,992 |
| R2 | 0.604 | |||||
| R2—within | 0.667 | 0.667 | 0.667 | 0.667 | 0.667 | |
| R2—between | 0.261 | 0.263 | 0.262 | 0.264 | 0.273 | |
| R2—overall | 0.604 | 0.604 | 0.604 | 0.604 | 0.606 | |
| Number of counties | 2856 | 2856 | 2856 | 2856 | 2856 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, Y.; Gao, J.; Sims, O.T. Associations between Bonus and Lottery COVID-19 Vaccine Incentive Policies and Increases in COVID-19 Vaccination Rates: A Social Epidemiologic Analysis. Trop. Med. Infect. Dis. 2022, 7, 118. https://doi.org/10.3390/tropicalmed7070118
Guo Y, Gao J, Sims OT. Associations between Bonus and Lottery COVID-19 Vaccine Incentive Policies and Increases in COVID-19 Vaccination Rates: A Social Epidemiologic Analysis. Tropical Medicine and Infectious Disease. 2022; 7(7):118. https://doi.org/10.3390/tropicalmed7070118
Chicago/Turabian StyleGuo, Yuqi, Jingjing Gao, and Omar T. Sims. 2022. "Associations between Bonus and Lottery COVID-19 Vaccine Incentive Policies and Increases in COVID-19 Vaccination Rates: A Social Epidemiologic Analysis" Tropical Medicine and Infectious Disease 7, no. 7: 118. https://doi.org/10.3390/tropicalmed7070118
APA StyleGuo, Y., Gao, J., & Sims, O. T. (2022). Associations between Bonus and Lottery COVID-19 Vaccine Incentive Policies and Increases in COVID-19 Vaccination Rates: A Social Epidemiologic Analysis. Tropical Medicine and Infectious Disease, 7(7), 118. https://doi.org/10.3390/tropicalmed7070118