
Temporal Variations and Spatial Clusters of Dengue in Thailand: Longitudinal Study before and during the Coronavirus Disease (COVID-19) Pandemic



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
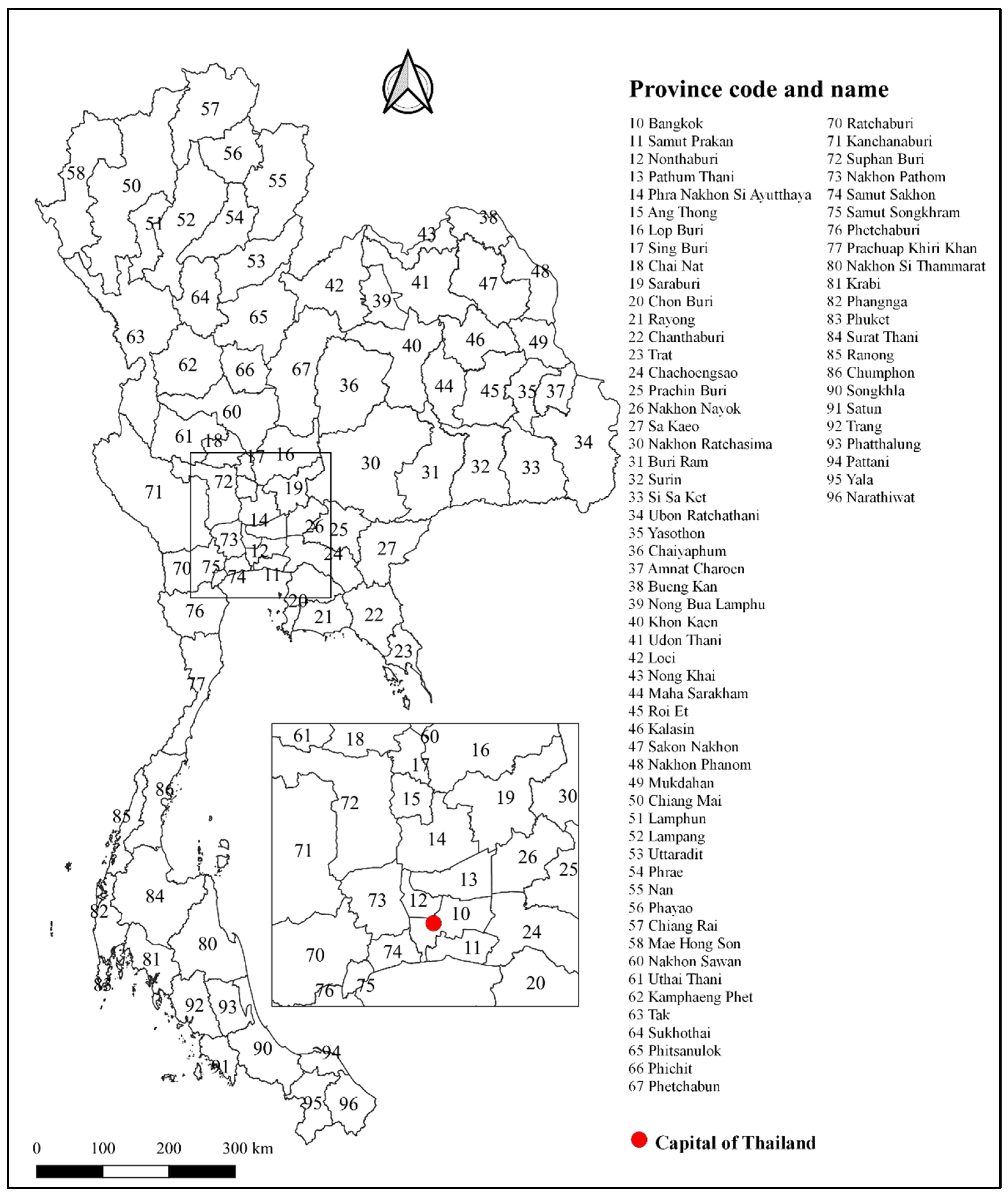
2.1. Study Design and Study Areas
2.2. Dengue Data
2.3. Temporal Analysis
2.4. Spatial Analysis
3. Results
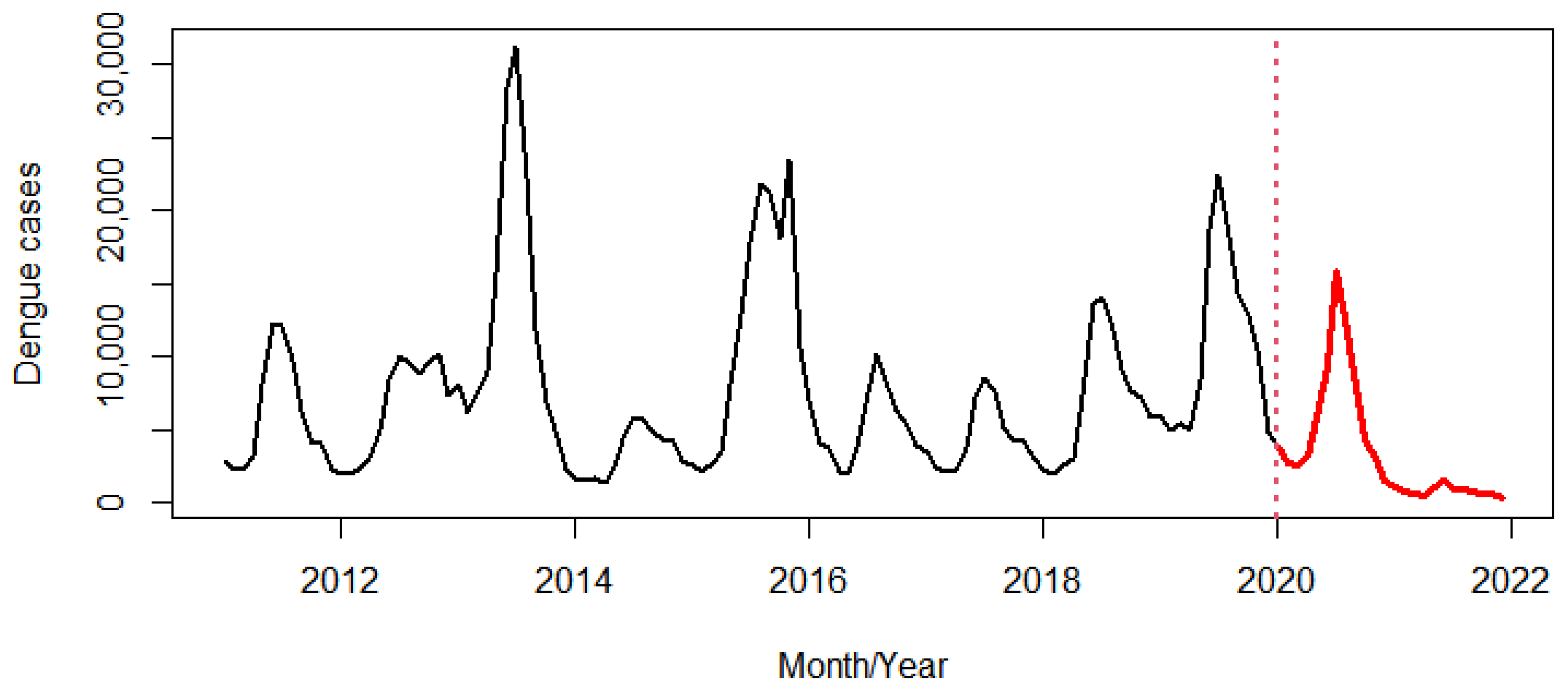
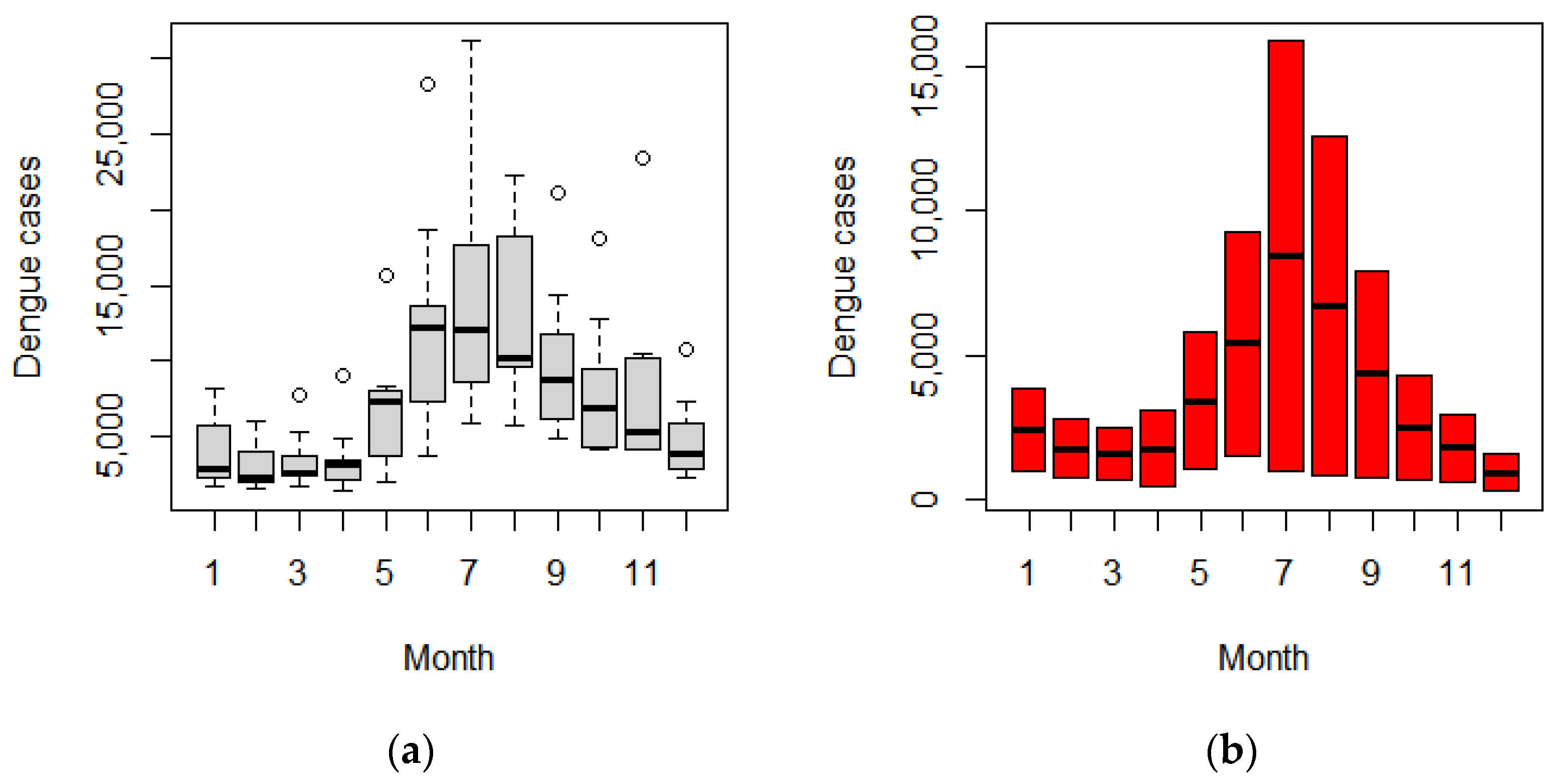
3.1. Temporal Variation
3.1.1. Cyclic, Seasonal, and Trend
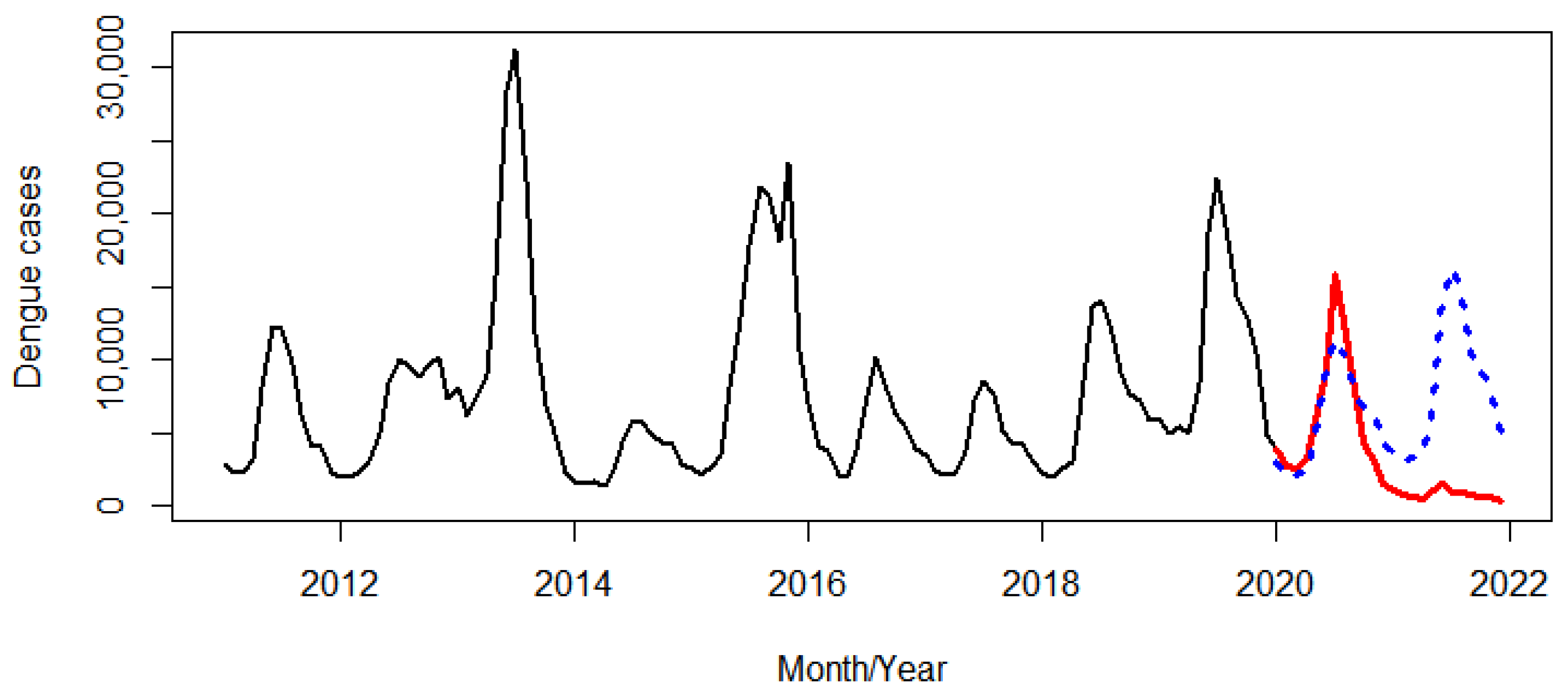
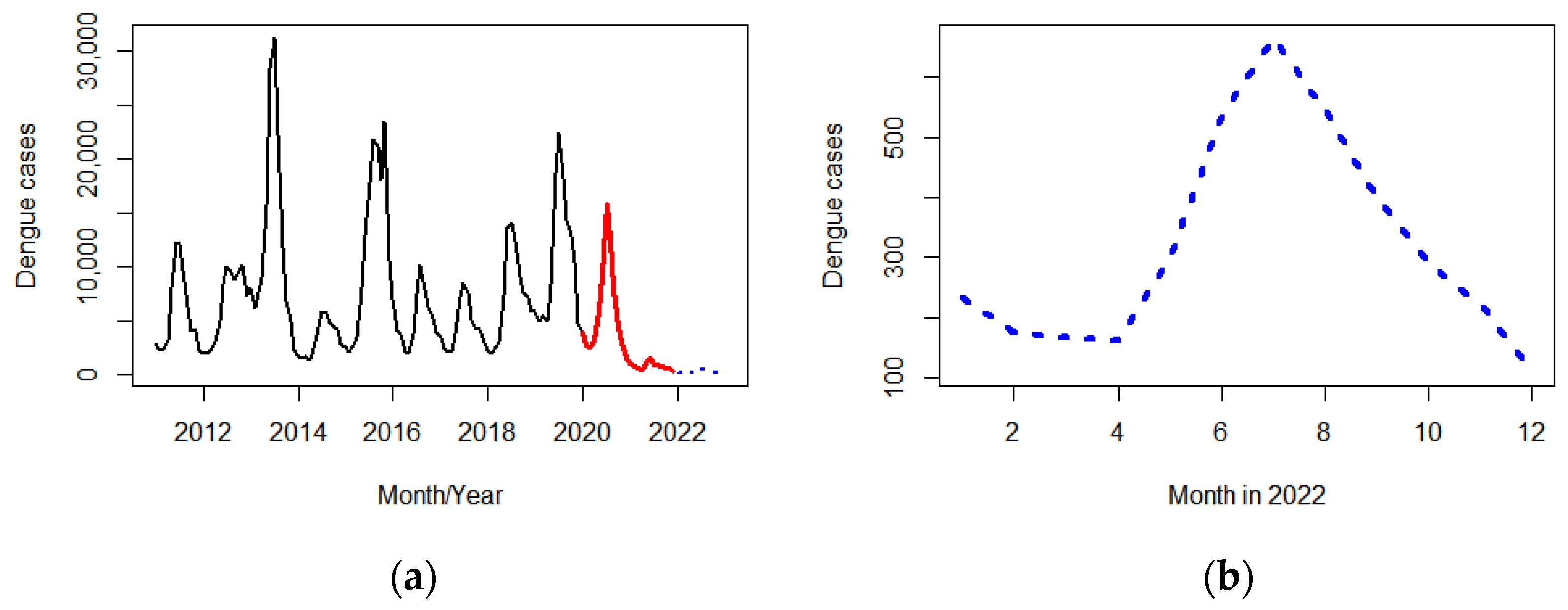
3.1.2. Forecasting Dengue Incidence
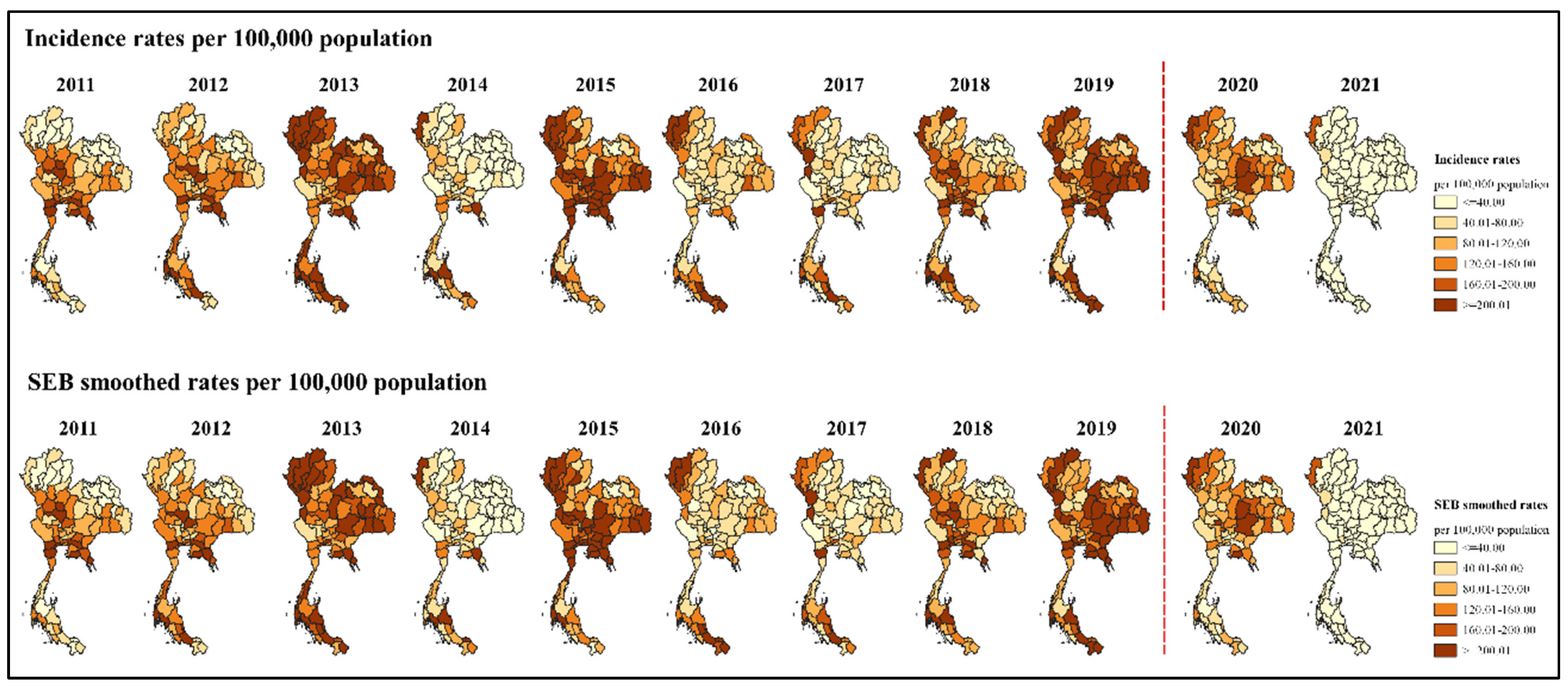
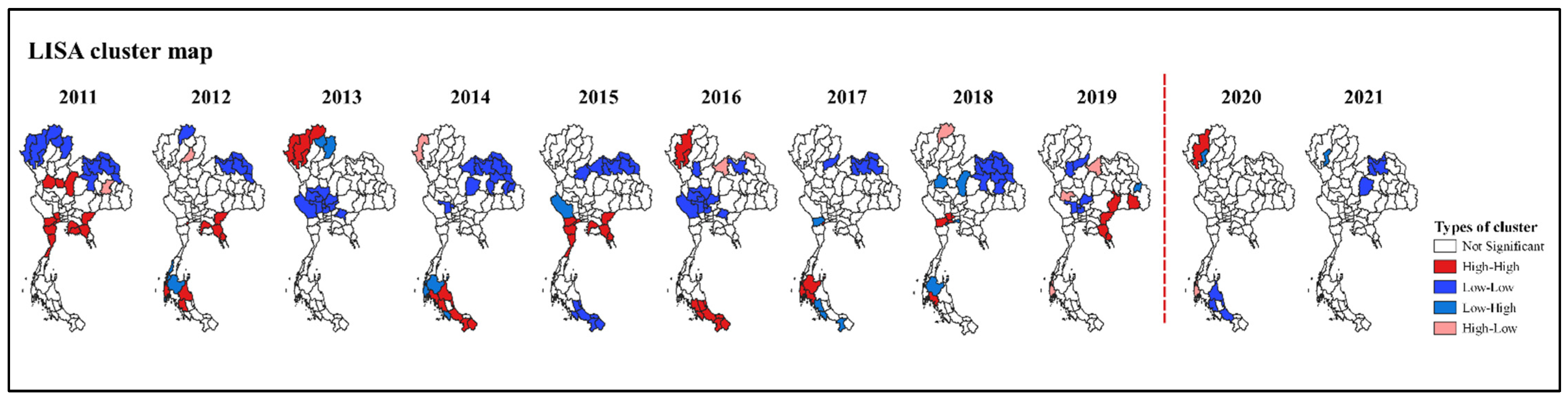
3.2. Spatial Clusters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACF | Autocorrelation function |
| AIC | Akaike information criterion |
| AR | Autoregressive model |
| ARIMA | Autoregressive integrated moving average |
| CI | Confidence interval |
| COVID-19 | Coronavirus disease 2019 |
| DENV | Dengue virus |
| DF | Dengue fever |
| DHF | Dengue hemorrhagic fever |
| DSS | Dengue shock syndrome |
| IRR | Incidence rate ratio |
| LISA | Local indicators of spatial association |
| MA | Moving average model |
| MAPE | Mean absolute percentage error |
| MAUP | Modifiable areal unit problem |
| PACF | Partial autocorrelation function |
| SEB | Spatial empirical Bayesian |
| STL | Seasonal decomposition of time series by Loess |
| WHO | World Health Organization |
References
- World Health Organization. Dengue and Severe Dengue. Available online: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue (accessed on 10 July 2022).
- Kraemer, M.U.G.; Reiner, R.C.; Brady, O.J.; Messina, J.P.; Gilbert, M.; Pigott, D.M.; Yi, D.; Johnson, K.; Earl, L.; Marczak, L.B.; et al. Past and future spread of the arbovirus vectors Aedes aegypti and Aedes albopictus. Nat. Microbiol. 2019, 4, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Department of Medical Services, Ministry of Public Health. Guidelines for Diagnosis and Treatment of Dengue in Adults 2020; Ministry of Public Health: Nonthaburi, Thailand, 2020; ISBN 978-974-422-927-4.
- García-Carreras, B.; Yang, B.; Grabowski, M.K.; Sheppard, L.W.; Huang, A.T.; Salje, H.; Clapham, H.E.; Iamsirithaworn, S.; Doung-Ngern, P.; Lessler, J.; et al. Periodic synchronisation of dengue epidemics in Thailand over the last 5 decades driven by temperature and immunity. PLoS Biol. 2022, 20, e3001160. [Google Scholar] [CrossRef]
- Department of Disease Control, Ministry of Public Health. National Disease Surveillance (Report 506). Available online: http://doe.moph.go.th/surdata/index.php (accessed on 10 July 2022).
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Prasertbun, R.; Mori, H.; Mahittikorn, A.; Siri, S.; Naito, T. Pneumonia, influenza, and dengue cases decreased after the COVID-19 pandemic in Thailand. Trop. Med. Health 2022, 50, 27. [Google Scholar] [CrossRef] [PubMed]
- Liyanage, P.; Rocklöv, J.; Tissera, H.A. The impact of COVID-19 lockdown on dengue transmission in Sri Lanka; a natural experiment for understanding the influence of human mobility. PLoS Negl. Trop. Dis. 2021, 15, e0009420. [Google Scholar] [CrossRef] [PubMed]
- Department of Disease Control, Ministry of Public Health. Thailand COVID-19 Situation Update on 14 December 2020. Available online: https://ddc.moph.go.th/viralpneumonia/eng/file/situation/situation-no344-141263.pdf (accessed on 10 July 2022).
- Centre for COVID-19 Situation Administration. Thailand COVID-19 Situation Report on 8 June 2022. Available online: https://www.moicovid.com/08/07/2022/uncategorized/7967/ (accessed on 10 July 2022).
- Rajatanavin, N.; Tuangratananon, T.; Suphanchaimat, R.; Tangcharoensathien, V. Responding to the COVID-19 second wave in Thailand by diversifying and adapting lessons from the first wave. BMJ Glob. Health 2021, 6, e006178. [Google Scholar] [CrossRef]
- Marome, W.; Shaw, R. COVID-19 response in Thailand and its implications on future preparedness. Int. J. Environ. 2021, 18, 1089. [Google Scholar] [CrossRef]
- Wilder-Smith, A. Dengue during the COVID-19 pandemic. J. Travel Med. 2021, 28, taab183. [Google Scholar] [CrossRef]
- Ong, J.; Soh, S.; Ho, S.H.; Seah, A.; Dickens, B.S.; Tan, K.W.; Koo, J.R.; Cook, A.R.; Richards, D.R.; Gaw, L.Y.-F.; et al. Fine-scale estimation of effective reproduction numbers for dengue surveillance. PLoS Comput. Biol. 2022, 18, e1009791. [Google Scholar] [CrossRef]
- Plasencia-Dueñas, R.; Failoc-Rojas, V.E.; Rodriguez-Morales, A.J. Impact of the COVID-19 pandemic on the incidence of dengue fever in Peru. J. Med. Virol. 2022, 94, 393–398. [Google Scholar] [CrossRef]
- Chen, Y.; Li, N.; Lourenço, J.; Wang, L.; Cazelles, B.; Dong, L.; Li, B.; Liu, Y.; Jit, M.; Bosse, N.I.; et al. Measuring the effects of COVID-19-related disruption on dengue transmission in Southeast Asia and Latin America: A statistical modelling study. Lancet Infect. Dis. 2022, 22, 657–667. [Google Scholar] [CrossRef]
- Imlach, F.; McKinlay, E.; Kennedy, J.; Pledger, M.; Middleton, L.; Cumming, J.; McBride-Henry, K. Seeking healthcare during lockdown: Challenges, opportunities and lessons for the future. Int. J. Health Policy Manag. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sheng, Z.Y.; Li, M.; Yang, R.; Liu, Y.H.; Yin, X.X.; Mao, J.R.; Brown, H.E.; An, J.; Zhou, H.N.; Wang, P.G. COVID-19 prevention measures reduce dengue spread in Yunnan Province, China, but do not reduce established outbreak. Microbes Infect. 2022, 11, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Surendran, S.N.; Nagulan, R.; Sivabalakrishnan, K.; Arthiyan, S.; Tharsan, A.; Jayadas, T.T.P.; Raveendran, S.; Kumanan, T.; Ramasamy, R. Reduced dengue incidence during the COVID-19 movement restrictions in Sri Lanka from March 2020 to April 2021. BMC Public Health 2022, 22, 388. [Google Scholar] [CrossRef] [PubMed]
- Paz-Bailey, G.; Adams, L.; Wong, J.M.; Poehling, K.A.; Chen, W.H.; McNally, V.; Atmar, R.L.; Waterman, S.H. Dengue vaccine: Recommendations of the advisory committee on immunization practices, United States, 2021. MMWR Recomm. Rep. 2021, 70, 1–16. [Google Scholar] [CrossRef]
- Statistical Forecasting Division, National Statistical Office, Ministry of Digital Economy and Society. Statistical Yearbook Thailand 2020; National Statistical Office: Bangkok, Thailand, 2020.
- Thai Meteorological Department. The Climate of Thailand. Available online: https://www.tmd.go.th/en/archive/thailand_climate.pdf (accessed on 10 July 2022).
- World Health Organization. Dengue Haemorrhagic Fever: Diagnosis, Treatment, Prevention and Control. 1997. Available online: https://apps.who.int/iris/bitstream/handle/10665/41988/9241545003_eng.pdf?sequence=1&isAllowed=y (accessed on 15 July 2022).
- World Health Organization. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control. 2009. Available online: https://www.who.int/publications/i/item/9789241547871 (accessed on 15 July 2022).
- RStudio Team. RStudio: Integrated Development for R. 2020. Available online: http://www.rstudio.com (accessed on 5 June 2022).
- Box, G.E.P.; Jenkins, G.M. Time series analysis, forecasting and control. In A Very British Affair: Six Britons and the Development of Time Series Analysis during the 20th Century; Mills, T.C., Ed.; Palgrave Macmillan UK: London, UK, 2013; pp. 161–215. [Google Scholar]
- QGIS Development Team. QGIS Geographic Information System 2022. Available online: https://www.qgis.org/en/site/index.html (accessed on 10 June 2022).
- Anselin, L.; Syabri, I.; Kho, Y. GeoDa: An introduction to spatial data analysis. Geogr. Anal. 2006, 38, 5–22. [Google Scholar] [CrossRef]
- Morris, C.N.; Kostal, H. An Empirical Bayes Approach to Spatial Analysis. 1983. Available online: https://ntrs.nasa.gov/citations/19840004489 (accessed on 28 June 2022).
- Anselin, L. Local Indicators of Spatial Association—LISA. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Chumpu, R.; Khamsemanan, N.; Nattee, C. The association between dengue incidences and provincial-level weather variables in Thailand from 2001 to 2014. PLoS ONE 2019, 14, e0226945. [Google Scholar] [CrossRef] [Green Version]
- Yuan, B.; Lee, H.; Nishiura, H. Analysis of international traveler mobility patterns in Tokyo to identify geographic foci of dengue fever risk. Theor. Biol. Med. Model 2021, 18, 17. [Google Scholar] [CrossRef]
- Oo, N.; Hanboonkunupakarn, B.; Piyaphanee, W.; Phumratanaprapin, W.; Luvira, V.; Wichainprasat, P.; Chotivanich, K.; Tantawichien, T. Review of health problems among foreign travelers presenting to the hospital for tropical diseases, Bangkok, Thailand between 2009 and 2014. J. Med. Assoc. Thail. 2019, 102, 918–926. [Google Scholar]
- Gossner, C.M.; Fournet, N.; Frank, C.; Fernández-Martínez, B.; Manso, M.D.; Dias, J.G.; Valk, H. Dengue virus infections among European travellers, 2015 to 2019. Eurosurveillance 2022, 27, 2001937. [Google Scholar] [CrossRef] [PubMed]
- Wongkoon, S.; Jaroensutasinee, M.; Jaroensutasinee, K. Development of temporal modeling for prediction of dengue infection in northeastern Thailand. Asian Pac. J. Trop. Med. 2012, 5, 249–252. [Google Scholar] [CrossRef]
- Gyawali, N.; Johnson, B.J.; Dixit, S.M.; Devine, G.J. Patterns of dengue in Nepal from 2010–2019 in relation to elevation and climate. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 741–749. [Google Scholar] [CrossRef]
- NOAA Climate.gov. November 2017 La Niña Update: She’s Back! Available online: https://www.climate.gov/news-features/blogs/enso/november-2017-la-ni%C3%B1a-update-she%E2%80%99s-back (accessed on 13 July 2022).
- Li, N.; Feng, Y.; Vrancken, B.; Chen, Y.; Dong, L.; Yang, Q.; Kraemer, M.U.G.; Pybus, O.G.; Zhang, H.; Brady, O.J.; et al. Assessing the impact of COVID-19 border restrictions on dengue transmission in Yunnan Province, China: An observational epidemiological and phylogenetic analysis. Lancet Reg. Health West. Pac. 2021, 14, 100259. [Google Scholar] [CrossRef] [PubMed]
- Yek, C.; Nam, V.S.; Leang, R.; Parker, D.M.; Heng, S.; Souv, K.; Sovannaroth, S.; Mayxay, M.; AbuBakar, S.; Sasmono, R.T.; et al. The pandemic experience in Southeast Asia: Interface between SARS-CoV-2, malaria, and dengue. Front. Trop. Dis. 2021, 2, 788590. [Google Scholar] [CrossRef] [PubMed]
- Lam, L.T.M.; Chua, Y.X.; Tan, D.H.Y. Roles and challenges of primary care physicians facing a dual outbreak of COVID-19 and dengue in Singapore. Fam. Pract. 2020, 37, 578–579. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Gendriz, I.; de Souza, G.F.; de Andrade, I.G.M.; Neto, A.D.D.; de Medeiros Tavares, A.; Barros, D.M.S.; de Morais, A.H.F.; Galvão-Lima, L.J.; de Medeiros Valentim, R.A. Data-driven computational intelligence applied to dengue outbreak forecasting: A case study at the scale of the city of Natal, RN-Brazil. Sci. Rep. 2022, 12, 6550. [Google Scholar] [CrossRef]
- Lorenz, C.; Bocewicz, A.C.D.; de Azevedo Marques, C.C.; Santana, L.M.R.; Chiaravalloti-Neto, F.; Gomes, A.H.A.; Barbosa, G.L. Have measures against COVID-19 helped to reduce dengue cases in Brazil? Travel Med. Infect. Dis. 2020, 37, 101827. [Google Scholar] [CrossRef]
- Kaweenuttayanon, N.; Pattanarattanamolee, R.; Sorncha, N.; Nakahara, S. Community surveillance of COVID-19 by village health volunteers, Thailand. Bull. World Health Organ. 2021, 99, 393–397. [Google Scholar] [CrossRef]
- Wiyono, L.; Rocha, I.C.N.; Cedeño, T.D.D.; Miranda, A.V.; Lucero-Prisno, D.E., III. Dengue and COVID-19 Infections in the ASEAN Region: A concurrent outbreak of viral diseases. Epidemiol. Health 2021, 43, e2021070. [Google Scholar] [CrossRef]
- Thai Meteorological Department. Monthly and Yearly Rainfall of Thailand 2021. Available online: http://climate.tmd.go.th/gge/R-dev21.pdf (accessed on 31 July 2022).
- Thai Meteorological Department. Monthly and Yearly Rainfall of Thailand 2020. Available online: http://climate.tmd.go.th/gge/R-dev20.pdf (accessed on 31 July 2022).
- Thai Meteorological Department. Monthly and Yearly Rainfall of Thailand 2019. Available online: http://climate.tmd.go.th/gge/R-dev19.pdf (accessed on 31 July 2022).
- Thai Meteorological Department. Monthly and Yearly Rainfall of Thailand 2018. Available online: http://climate.tmd.go.th/gge/R-dev18.pdf (accessed on 31 July 2022).
- Kitphati, R.; Seangkeao, K.; Muangyim, K.; Nak-ai, W. Participatory development in community health for the Pgazkoenyau Ethnic: A case study in an ethnic community in Thailand. Open Public Health J. 2022, 15, 1–10. [Google Scholar] [CrossRef]
- Northern Meteorological Center. Highest-Lowest Temperature and Rainfall of the North. Available online: http://www.cmmet.tmd.go.th/forecast/pt/Max_Min_Rainfall.php (accessed on 31 July 2022).
- Weather Spark. Past Weather at Sanam Bin Mae Hong Son, Thailand. Available online: https://weatherspark.com/h/y/149056/2021/Historical-Weather-during-2021-at-Sanam-Bin-Mae-Hong-Son-Thailand (accessed on 31 July 2022).
- Van Benthem, B.H.B.; Khantikul, N.; Panart, K.; Kessels, P.J.; Somboon, P.; Oskam, L. Knowledge and use of prevention measures related to dengue in Northern Thailand. Trop. Med. Int. Health 2002, 7, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A. Risk of dengue in travelers: Implications for dengue vaccination. Curr. Infect. Dis. Rep. 2018, 20, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saita, S.; Maeakhian, S.; Silawan, T. Temporal Variations and Spatial Clusters of Dengue in Thailand: Longitudinal Study before and during the Coronavirus Disease (COVID-19) Pandemic. Trop. Med. Infect. Dis. 2022, 7, 171. https://doi.org/10.3390/tropicalmed7080171
Saita S, Maeakhian S, Silawan T. Temporal Variations and Spatial Clusters of Dengue in Thailand: Longitudinal Study before and during the Coronavirus Disease (COVID-19) Pandemic. Tropical Medicine and Infectious Disease. 2022; 7(8):171. https://doi.org/10.3390/tropicalmed7080171
Chicago/Turabian StyleSaita, Sayambhu, Sasithan Maeakhian, and Tassanee Silawan. 2022. "Temporal Variations and Spatial Clusters of Dengue in Thailand: Longitudinal Study before and during the Coronavirus Disease (COVID-19) Pandemic" Tropical Medicine and Infectious Disease 7, no. 8: 171. https://doi.org/10.3390/tropicalmed7080171
APA StyleSaita, S., Maeakhian, S., & Silawan, T. (2022). Temporal Variations and Spatial Clusters of Dengue in Thailand: Longitudinal Study before and during the Coronavirus Disease (COVID-19) Pandemic. Tropical Medicine and Infectious Disease, 7(8), 171. https://doi.org/10.3390/tropicalmed7080171