
Dynamics of Antibody Responses after Asymptomatic and Mild to Moderate SARS-CoV-2 Infections: Real-World Data in a Resource-Limited Country

 , , , , , , , add
Show full author list
, , , , , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
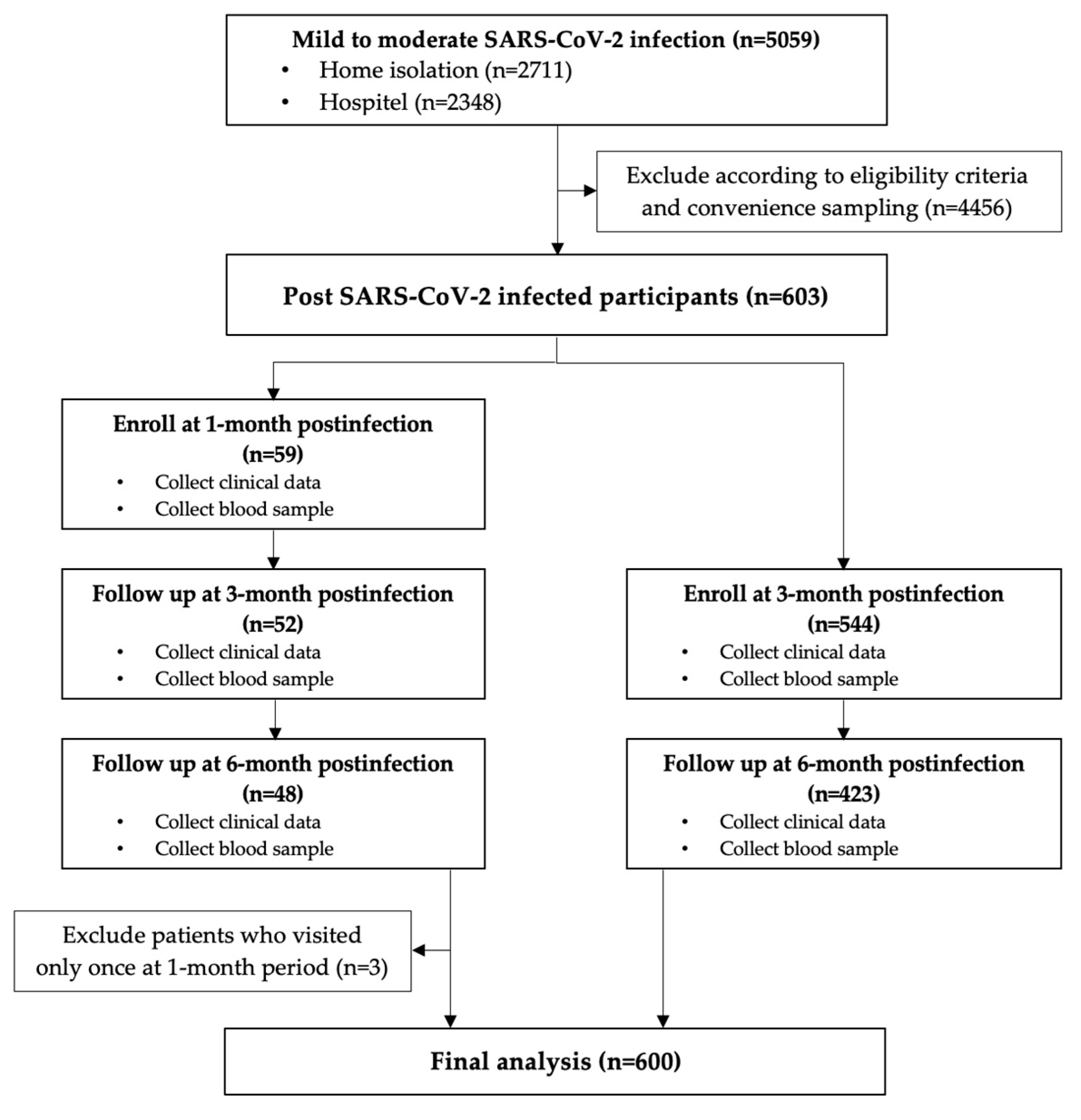
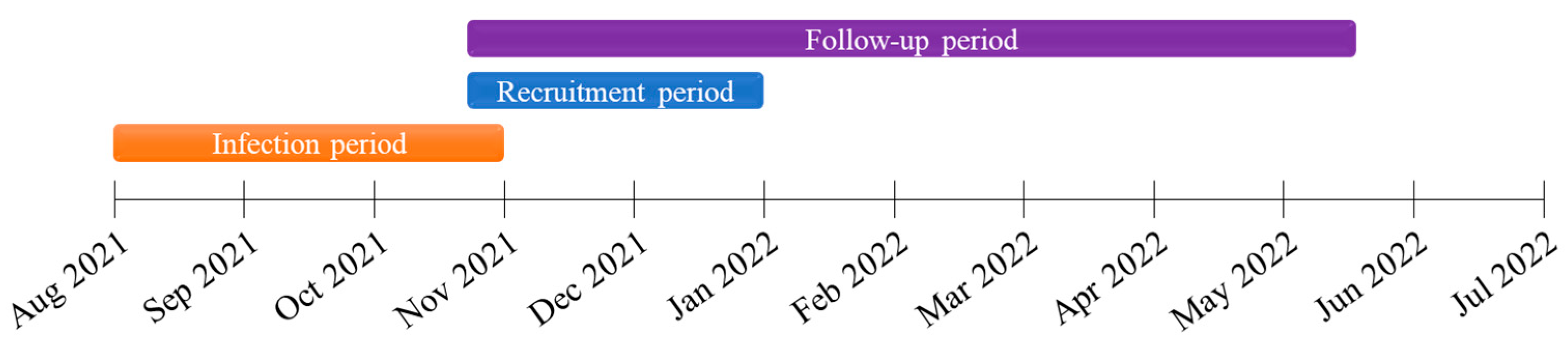
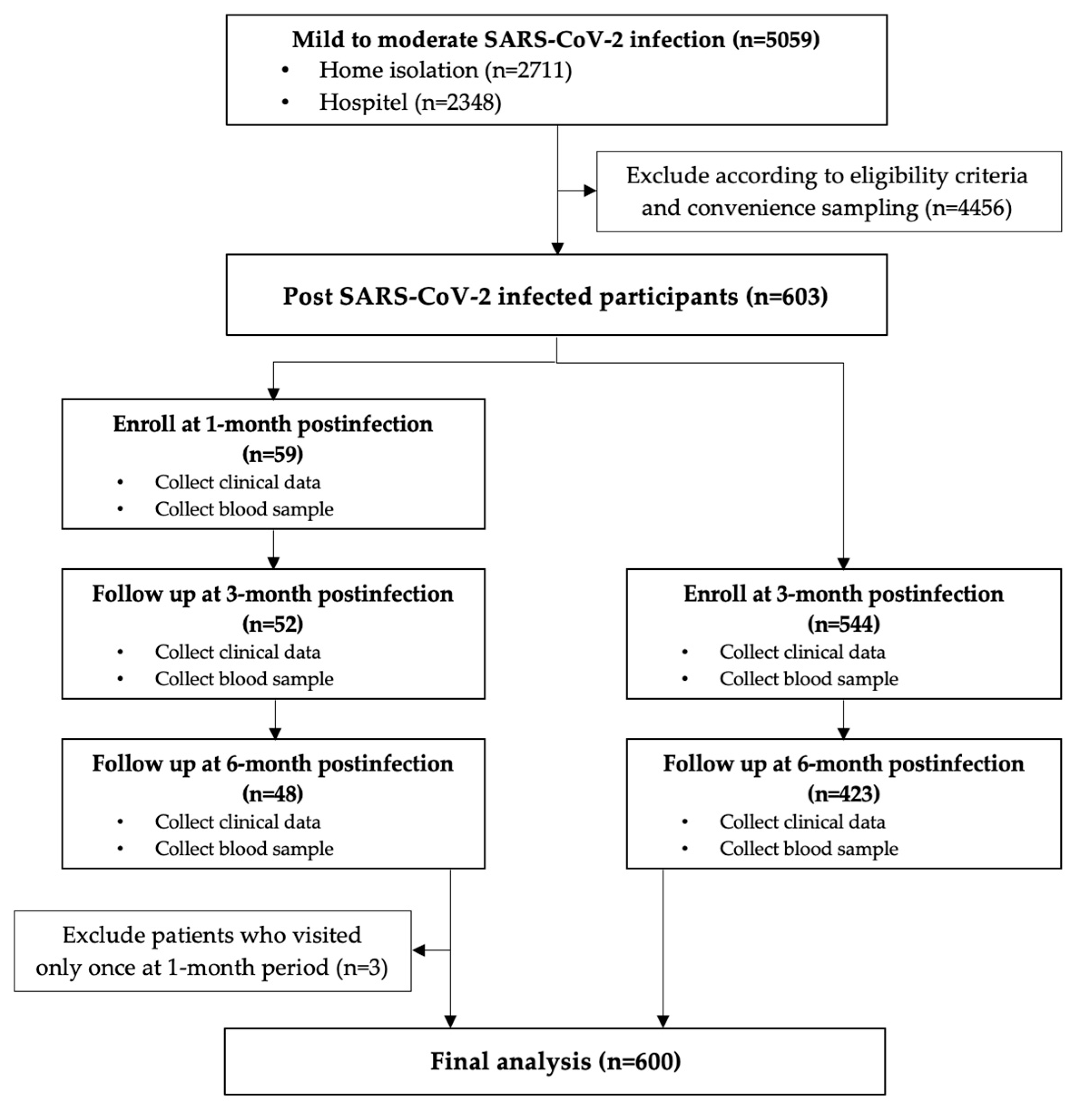
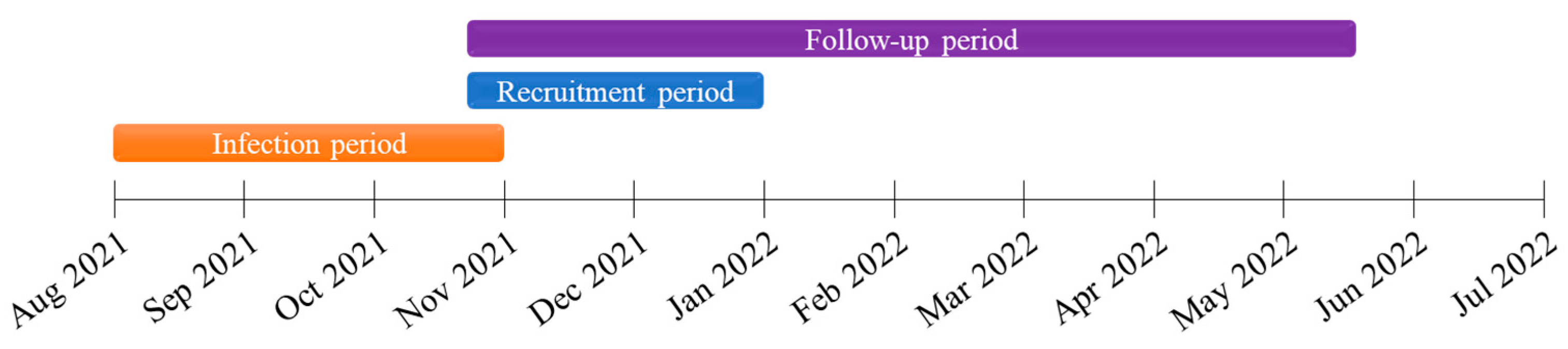
2.1. Study Design and Participants
2.2. Antibody Responses and Clinical Data
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Factors Associated with Antibody Responses
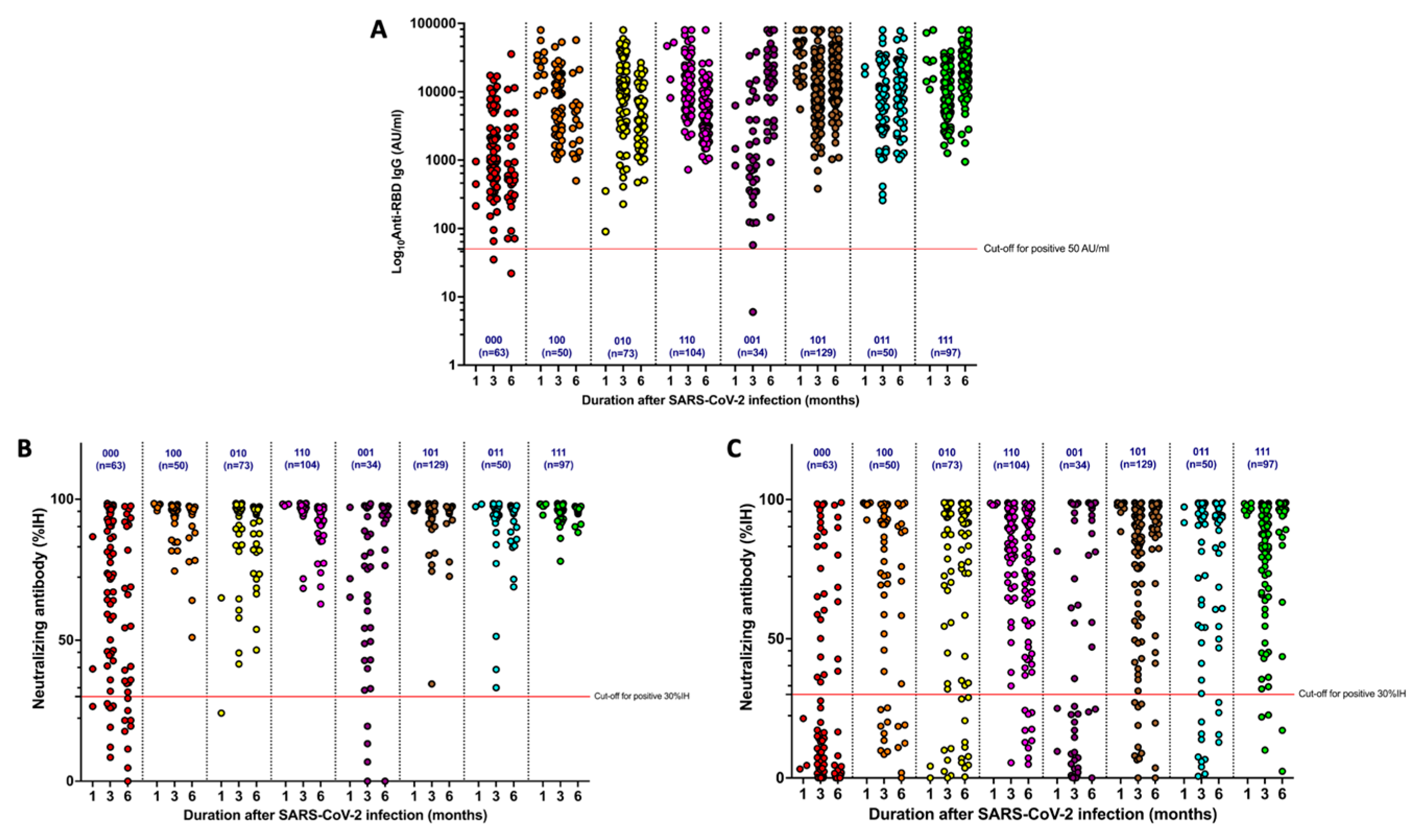
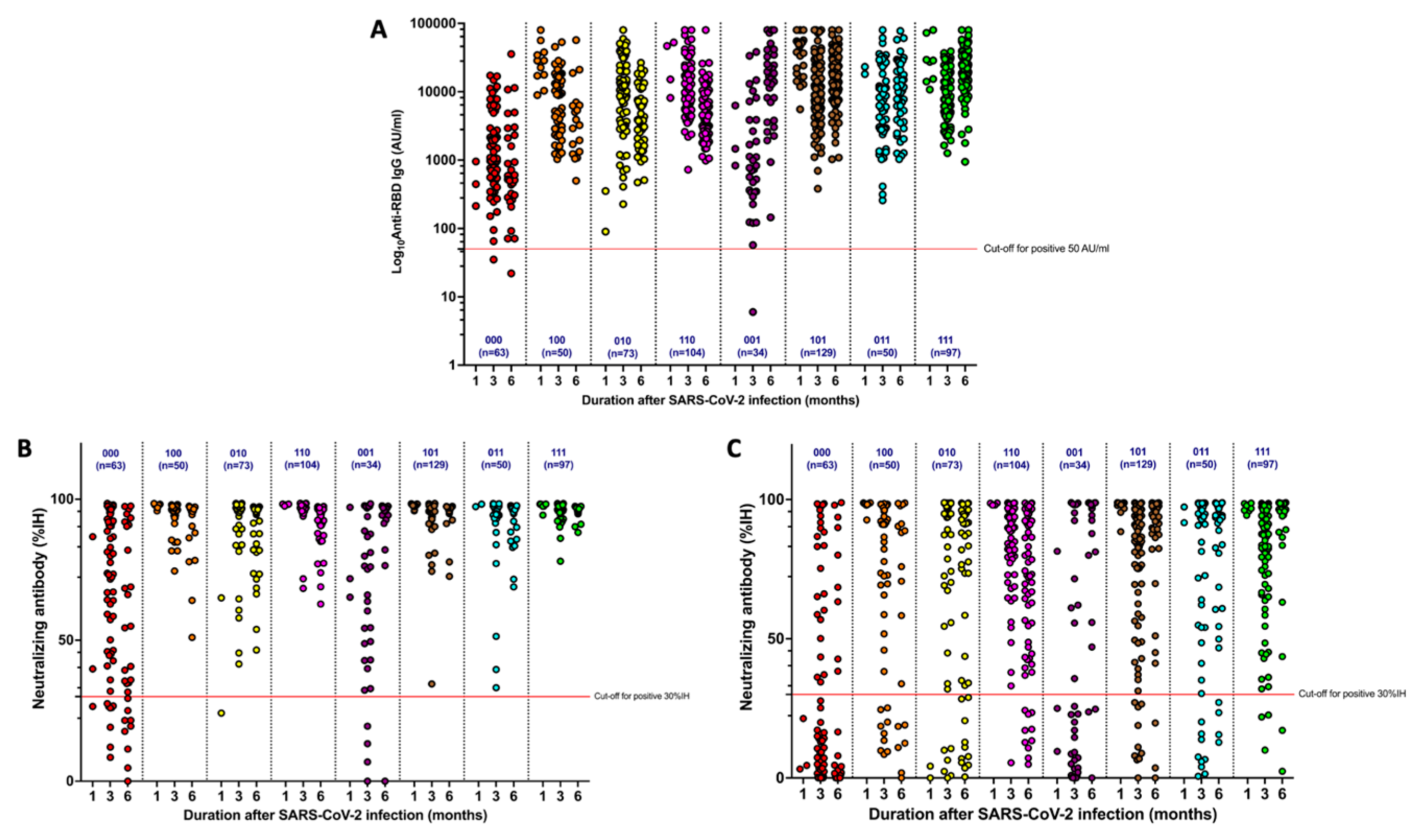
3.3. Dynamics of Antibody Responses
3.4. Reinfection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Worldometer. COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 1 August 2022).
- Tenforde, M.W.; Self, W.H.; Adams, K.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Association Between mRNA Vaccination and COVID-19 Hospitalization and Disease Severity. JAMA 2021, 326, 2043–2054. [Google Scholar] [CrossRef] [PubMed]
- Lauring, A.S.; Tenforde, M.W.; Chappell, J.D.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Clinical severity of, and effectiveness of mRNA vaccines against, covid-19 from omicron, delta, and alpha SARS-CoV-2 variants in the United States: Prospective observational study. BMJ 2022, 376, e069761. [Google Scholar] [CrossRef] [PubMed]
- Eyre, D.W.; Taylor, D.; Purver, M.; Chapman, D.; Fowler, T.; Pouwels, K.B.; Walker, A.S.; Peto, T.E.A. Effect of COVID-19 Vaccination on Transmission of Alpha and Delta Variants. N. Engl. J. Med. 2022, 386, 744–756. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. FDA Approves First COVID-19 Vaccine. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-covid-19-vaccine/ (accessed on 14 July 2022).
- Angkasekwinai, N.; Sewatanon, J.; Niyomnaitham, S.; Phumiamorn, S.; Sukapirom, K.; Sapsutthipas, S.; Sirijatuphat, R.; Wittawatmongkol, O.; Senawong, S.; Mahasirimongkol, S.; et al. Comparison of safety and immunogenicity of CoronaVac and ChAdOx1 against the SARS-CoV-2 circulating variants of concern (Alpha, Delta, Beta) in Thai healthcare workers. Vaccine X 2022, 10, 100153. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Rodríguez, R.; Terrón-Arcos, V.; Montalbán-Hernández, K.; Casalvilla-Dueñas, J.C.; Bergón-Gutierrez, M.; Pascual-Iglesias, A.; Quiroga, J.V.; Aguirre, L.A.; Pérez de Diego, R.; Vela-Olmo, C.; et al. Prior SARS-CoV-2 infection balances immune responses triggered by four EMA-approved COVID-19 vaccines: An observational study. Clin. Transl. Med. 2022, 12, e869. [Google Scholar] [CrossRef] [PubMed]
- Suthar, M.S.; Zimmerman, M.G.; Kauffman, R.C.; Mantus, G.; Linderman, S.L.; Hudson, W.H.; Vanderheiden, A.; Nyhoff, L.; Davis, C.W.; Adekunle, O.; et al. Rapid Generation of Neutralizing Antibody Responses in COVID-19 Patients. Cell Rep. Med. 2020, 1, 100040. [Google Scholar] [CrossRef]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody Responses to SARS-CoV-2 in Patients with Novel Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 2027–2034. [Google Scholar] [CrossRef]
- Hall, V.J.; Foulkes, S.; Charlett, A.; Atti, A.; Monk, E.J.M.; Simmons, R.; Wellington, E.; Cole, M.J.; Saei, A.; Oguti, B.; et al. SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: A large, multicentre, prospective cohort study (SIREN). Lancet 2021, 397, 1459–1469. [Google Scholar] [CrossRef]
- Hansen, C.H.; Michlmayr, D.; Gubbels, S.M.; Mølbak, K.; Ethelberg, S. Assessment of protection against reinfection with SARS-CoV-2 among 4 million PCR-tested individuals in Denmark in 2020: A population-level observational study. Lancet 2021, 397, 1204–1212. [Google Scholar] [CrossRef]
- Alefishat, E.; Jelinek, H.F.; Mousa, M.; Tay, G.K.; Alsafar, H.S. Immune response to SARS-CoV-2 variants: A focus on severity, susceptibility, and preexisting immunity. J. Infect. Public Health 2022, 15, 277–288. [Google Scholar] [CrossRef]
- Lewis, N.; Chambers, L.C.; Chu, H.T.; Fortnam, T.; De Vito, R.; Gargano, L.M.; Chan, P.A.; McDonald, J.; Hogan, J.W. Effectiveness Associated with Vaccination After COVID-19 Recovery in Preventing Reinfection. JAMA Netw. Open 2022, 5, e2223917. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Wyka, K.; White, T.M.; Picchio, C.A.; Rabin, K.; Ratzan, S.C.; Parsons Leigh, J.; Hu, J.; El-Mohandes, A. Revisiting COVID-19 vaccine hesitancy around the world using data from 23 countries in 2021. Nat. Commun. 2022, 13, 3801. [Google Scholar] [CrossRef]
- Wei, J.; Matthews, P.C.; Stoesser, N.; Maddox, T.; Lorenzi, L.; Studley, R.; Bell, J.I.; Newton, J.N.; Farrar, J.; Diamond, I.; et al. Anti-spike antibody response to natural SARS-CoV-2 infection in the general population. Nat. Commun. 2021, 12, 6250. [Google Scholar] [CrossRef] [PubMed]
- Lumley, S.F.; Wei, J.; O’Donnell, D.; Stoesser, N.E.; Matthews, P.C.; Howarth, A.; Hatch, S.B.; Marsden, B.D.; Cox, S.; James, T.; et al. The Duration, Dynamics, and Determinants of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Antibody Responses in Individual Healthcare Workers. Clin. Infect. Dis. 2021, 73, e699–e709. [Google Scholar] [CrossRef]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 31 December 2022).
- Centers for Disease Control and Prevention. COVID-19: People with Certain Medical Conditions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html#immunocompromised/ (accessed on 10 February 2023).
- Infantino, M.; Pieri, M.; Nuccetelli, M.; Grossi, V.; Lari, B.; Tomassetti, F.; Calugi, G.; Pancani, S.; Benucci, M.; Casprini, P.; et al. The WHO International Standard for COVID-19 serological tests: Towards harmonization of anti-spike assays. Int. Immunopharmacol. 2021, 100, 108095. [Google Scholar] [CrossRef]
- Wang, K.; Long, Q.X.; Deng, H.J.; Hu, J.; Gao, Q.Z.; Zhang, G.J.; He, C.L.; Huang, L.Y.; Hu, J.L.; Chen, J.; et al. Longitudinal Dynamics of the Neutralizing Antibody Response to Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection. Clin. Infect. Dis. 2021, 73, e531–e539. [Google Scholar] [CrossRef] [PubMed]
- Crawford, K.H.D.; Dingens, A.S.; Eguia, R.; Wolf, C.R.; Wilcox, N.; Logue, J.K.; Shuey, K.; Casto, A.M.; Fiala, B.; Wrenn, S.; et al. Dynamics of Neutralizing Antibody Titers in the Months After Severe Acute Respiratory Syndrome Coronavirus 2 Infection. J. Infect. Dis. 2021, 223, 197–205. [Google Scholar] [CrossRef]
- Post, N.; Eddy, D.; Huntley, C.; van Schalkwyk, M.C.I.; Shrotri, M.; Leeman, D.; Rigby, S.; Williams, S.V.; Bermingham, W.H.; Kellam, P.; et al. Antibody response to SARS-CoV-2 infection in humans: A systematic review. PLoS ONE 2020, 15, e0244126. [Google Scholar] [CrossRef]
- Wheatley, A.K.; Juno, J.A.; Wang, J.J.; Selva, K.J.; Reynaldi, A.; Tan, H.X.; Lee, W.S.; Wragg, K.M.; Kelly, H.G.; Esterbauer, R.; et al. Evolution of immune responses to SARS-CoV-2 in mild-moderate COVID-19. Nat. Commun. 2021, 12, 1162. [Google Scholar] [CrossRef]
- Ibarrondo, F.J.; Fulcher, J.A.; Goodman-Meza, D.; Elliott, J.; Hofmann, C.; Hausner, M.A.; Ferbas, K.G.; Tobin, N.H.; Aldrovandi, G.M.; Yang, O.O. Rapid Decay of Anti-SARS-CoV-2 Antibodies in Persons with Mild COVID-19. N. Engl. J. Med. 2020, 383, 1085–1087. [Google Scholar] [CrossRef]
- Di Fusco, M.; Lin, J.; Vaghela, S.; Lingohr-Smith, M.; Nguyen, J.L.; Scassellati Sforzolini, T.; Judy, J.; Cane, A.; Moran, M.M. COVID-19 vaccine effectiveness among immunocompromised populations: A targeted literature review of real-world studies. Expert Rev. Vaccines 2022, 21, 435–451. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, A.M.; Spicer, K.B.; Thoroughman, D.; Glick, C.; Winter, K. Reduced Risk of Reinfection with SARS-CoV-2 After COVID-19 Vaccination—Kentucky, May–June 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1081–1083. [Google Scholar] [CrossRef] [PubMed]
- Barros-Martins, J.; Hammerschmidt, S.I.; Cossmann, A.; Odak, I.; Stankov, M.V.; Morillas Ramos, G.; Dopfer-Jablonka, A.; Heidemann, A.; Ritter, C.; Friedrichsen, M.; et al. Immune responses against SARS-CoV-2 variants after heterologous and homologous ChAdOx1 nCoV-19/BNT162b2 vaccination. Nat. Med. 2021, 27, 1525–1529. [Google Scholar] [CrossRef]
- Hillus, D.; Schwarz, T.; Tober-Lau, P.; Vanshylla, K.; Hastor, H.; Thibeault, C.; Jentzsch, S.; Helbig, E.T.; Lippert, L.J.; Tscheak, P.; et al. Safety, reactogenicity, and immunogenicity of homologous and heterologous prime-boost immunisation with ChAdOx1 nCoV-19 and BNT162b2: A prospective cohort study. Lancet Respir. Med. 2021, 9, 1255–1265. [Google Scholar] [CrossRef]
- Pérez-Then, E.; Lucas, C.; Monteiro, V.S.; Miric, M.; Brache, V.; Cochon, L.; Vogels, C.B.F.; Malik, A.A.; De la Cruz, E.; Jorge, A.; et al. Neutralizing antibodies against the SARS-CoV-2 Delta and Omicron variants following heterologous CoronaVac plus BNT162b2 booster vaccination. Nat. Med. 2022, 28, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Shaw, R.H.; Stuart, A.S.V.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Safety and immunogenicity of heterologous versus homologous prime-boost schedules with an adenoviral vectored and mRNA COVID-19 vaccine (Com-COV): A single-blind, randomised, non-inferiority trial. Lancet 2021, 398, 856–869. [Google Scholar] [CrossRef] [PubMed]
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E.; et al. Homologous and Heterologous COVID-19 Booster Vaccinations. N. Engl. J. Med. 2022, 386, 1046–1057. [Google Scholar] [CrossRef] [PubMed]
- Ho, T.C.; Chen, Y.M.A.; Chan, H.P.; Chang, C.C.; Chuang, K.P.; Lee, C.H.; Yuan, C.H.; Tyan, Y.C.; Yang, M.H. The Effects of Heterologous Immunization with Prime-Boost COVID-19 Vaccination against SARS-CoV-2. Vaccines 2021, 9, 1163. [Google Scholar] [CrossRef]
- Department of Disease Control, Thai Ministry of Public Health. COVID-19 Vaccine Guidance for SARS-CoV-2 Pandemic in Thailand. Available online: https://ddc.moph.go.th/vaccine-covid19/guidelines/ (accessed on 31 December 2022).
- Thompson, M.G.; Stenehjem, E.; Grannis, S.; Ball, S.W.; Naleway, A.L.; Ong, T.C.; DeSilva, M.B.; Natarajan, K.; Bozio, C.H.; Lewis, N.; et al. Effectiveness of COVID-19 Vaccines in Ambulatory and Inpatient Care Settings. N. Engl. J. Med. 2021, 385, 1355–1371. [Google Scholar] [CrossRef]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef]
- Iketani, S.; Liu, L.; Guo, Y.; Liu, L.; Chan, J.F.W.; Huang, Y.; Wang, M.; Luo, Y.; Yu, J.; Chu, H.; et al. Antibody evasion properties of SARS-CoV-2 Omicron sublineages. Nature 2022, 604, 553–556. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, C.J.; Pade, C.; Gibbons, J.M.; Otter, A.D.; Lin, K.M.; Muñoz Sandoval, D.; Pieper, F.P.; Butler, D.K.; Liu, S.; Joy, G.; et al. Immune boosting by B.1.1.529 (Omicron) depends on previous SARS-CoV-2 exposure. Science 2022, 377, eabq1841. [Google Scholar] [CrossRef] [PubMed]
- Külper-Schiek, W.; Piechotta, V.; Pilic, A.; Batke, M.; Dreveton, L.S.; Geurts, B.; Koch, J.; Köppe, S.; Treskova, M.; Vygen-Bonnet, S.; et al. Facing the Omicron variant-how well do vaccines protect against mild and severe COVID-19? Third interim analysis of a living systematic review. Front. Immunol. 2022, 13, 940562. [Google Scholar] [CrossRef] [PubMed]
- Altarawneh, H.N.; Chemaitelly, H.; Ayoub, H.H.; Tang, P.; Hasan, M.R.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Coyle, P.; Al-Kanaani, Z.; et al. Effects of Previous Infection and Vaccination on Symptomatic Omicron Infections. N. Engl. J. Med. 2022, 387, 21–34. [Google Scholar] [CrossRef]
- Link-Gelles, R.; Ciesla, A.A.; Fleming-Dutra, K.E.; Smith, Z.R.; Britton, A.; Wiegand, R.E.; Miller, J.D.; Accorsi, E.K.; Schrag, S.J.; Verani, J.R.; et al. Effectiveness of Bivalent mRNA Vaccines in Preventing Symptomatic SARS-CoV-2 Infection—Increasing Community Access to Testing Program, United States, September–November 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1526–1530. [Google Scholar] [CrossRef]
- Ou, J.; Tan, M.; He, H.; Tan, H.; Mai, J.; Long, Y.; Jiang, X.; He, Q.; Huang, Y.; Li, Y.; et al. SARS-CoV-2 Antibodies and Associated Factors at Different Hospitalization Time Points in 192 COVID-19 Cases. J. Appl. Lab. Med. 2021, 6, 1133–1142. [Google Scholar] [CrossRef]
- Luchsinger, L.L.; Ransegnola, B.P.; Jin, D.K.; Muecksch, F.; Weisblum, Y.; Bao, W.; George, P.J.; Rodriguez, M.; Tricoche, N.; Schmidt, F.; et al. Serological Assays Estimate Highly Variable SARS-CoV-2 Neutralizing Antibody Activity in Recovered COVID-19 Patients. J. Clin. Microbiol. 2020, 58, e02005–e02020. [Google Scholar] [CrossRef]
- Brochot, E.; Demey, B.; Touzé, A.; Belouzard, S.; Dubuisson, J.; Schmit, J.L.; Duverlie, G.; Francois, C.; Castelain, S.; Helle, F. Anti-spike, Anti-nucleocapsid and Neutralizing Antibodies in SARS-CoV-2 Inpatients and Asymptomatic Individuals. Front. Microbiol. 2020, 11, 584251. [Google Scholar] [CrossRef]
- Frasca, D.; Reidy, L.; Cray, C.; Diaz, A.; Romero, M.; Kahl, K.; Blomberg, B.B. Influence of obesity on serum levels of SARS-CoV-2-specific antibodies in COVID-19 patients. PLoS ONE 2021, 16, e0245424. [Google Scholar] [CrossRef]
- Al-Otaiby, M.; Krissaane, I.; Al Seraihi, A.; Alshenaifi, J.; Qahtani, M.H.; Aljeri, T.; Zaatari, E.; Hassanain, M.; Algwizani, A.; Albarrag, A.; et al. SARS-CoV-2 Reinfection Rate and Outcomes in Saudi Arabia: A National Retrospective Study. Int J. Infect. Dis. 2022, 122, 758–766. [Google Scholar] [CrossRef]
- Shah, V.P.; Farah, W.H.; Hill, J.C.; Hassett, L.C.; Binnicker, M.J.; Yao, J.D.; Murad, M.H. Association Between SARS-CoV-2 Cycle Threshold Values and Clinical Outcomes in Patients With COVID-19: A Systematic Review and Meta-analysis. Open Forum Infect. Dis. 2021, 8, ofab453. [Google Scholar] [CrossRef]
- Lee, B.; Ko, J.H.; Park, J.; Moon, H.W.; Baek, J.Y.; Jung, S.; Lim, H.Y.; Kim, K.C.; Huh, K.; Cho, S.Y.; et al. Estimating the Neutralizing Effect and Titer Correlation of Semi-Quantitative Anti-SARS-CoV-2 Antibody Immunoassays. Front. Cell Infect. Microbiol. 2022, 12, 822599. [Google Scholar] [CrossRef] [PubMed]
- Dolscheid-Pommerich, R.; Bartok, E.; Renn, M.; Kümmerer, B.M.; Schulte, B.; Schmithausen, R.M.; Stoffel-Wagner, B.; Streeck, H.; Saschenbrecker, S.; Steinhagen, K.; et al. Correlation between a quantitative anti-SARS-CoV-2 IgG ELISA and neutralization activity. J. Med. Virol. 2022, 94, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Guiomar, R.; Santos, A.J.; Melo, A.M.; Costa, I.; Matos, R.; Rodrigues, A.P.; Kislaya, I.; Silva, A.S.; Roque, C.; Nunes, C.; et al. Monitoring of SARS-CoV-2 Specific Antibodies after Vaccination. Vaccines 2022, 10, 154. [Google Scholar] [CrossRef] [PubMed]
- Morinaga, Y.; Tani, H.; Terasaki, Y.; Nomura, S.; Kawasuji, H.; Shimada, T.; Igarashi, E.; Saga, Y.; Yoshida, Y.; Yasukochi, R.; et al. Correlation of the Commercial Anti-SARS-CoV-2 Receptor Binding Domain Antibody Test with the Chemiluminescent Reduction Neutralizing Test and Possible Detection of Antibodies to Emerging Variants. Microbiol. Spectr. 2021, 9, e0056021. [Google Scholar] [CrossRef] [PubMed]
- Poon, R.W.S.; Lu, L.; Fong, C.H.Y.; Ip, T.C.; Chen, L.L.; Zhang, R.R.Q.; Yip, C.C.; Cheng, V.C.; Chan, K.H.; Yuen, K.Y.; et al. Correlation between Commercial Anti-RBD IgG Titer and Neutralization Titer against SARS-CoV-2 Beta Variant. Diagnostics 2021, 11, 2216. [Google Scholar] [CrossRef] [PubMed]
- Takheaw, N.; Liwsrisakun, C.; Chaiwong, W.; Laopajon, W.; Pata, S.; Inchai, J.; Duangjit, P.; Pothirat, C.; Bumroongkit, C.; Deesomchok, A.; et al. Correlation Analysis of Anti-SARS-CoV-2 RBD IgG and Neutralizing Antibody against SARS-CoV-2 Omicron Variants after Vaccination. Diagnostics 2022, 12, 1315. [Google Scholar] [CrossRef]
- Benner, S.E.; Patel, E.U.; Laeyendecker, O.; Pekosz, A.; Littlefield, K.; Eby, Y.; Fernandez, R.E.; Miller, J.; Kirby, C.S.; Keruly, M.; et al. SARS-CoV-2 Antibody Avidity Responses in COVID-19 Patients and Convalescent Plasma Donors. J. Infect. Dis. 2020, 222, 1974–1984. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Immunocompetent (n = 566) | Immunocompromised (n = 14) | Reinfected (n = 20) | p Value |
|---|---|---|---|---|
| Age—years (mean ± SD) | 45.8 ± 14.6 | 44.3 ± 10.3 | 37.1 ± 10.7 | 0.029 |
| Sex (female)—n (%) | 348 (61.5%) | 9 (64.3%) | 13 (65.0%) | 0.961 |
| BW at onset—kg (mean ± SD) | 66.7 ± 15.5 | 60.5 ± 13.4 | 74.4 ± 17.7 | 0.029 |
| BMI at onset—kg/m2 (mean ± SD) | 25.4 ± 5.0 | 22.3 4.8 | 27.1 ± 5.1 | 0.022 |
| BW at M3—kg (mean ± SD) | 67.5 ± 16.1 | 62.5 ± 14.4 | 75.3 ± 17.8 | 0.050 |
| BMI at M3—kg/m2 (mean ± SD) | 25.7 ± 5.2 | 23.0 ± 5.1 | 27.5 ± 5.0 | 0.048 |
| Risk factors at onset—n (%) | ||||
| Age ≥ 60 years | 103 (18.2%) | 1 (7.1%) | 1 (5.0%) | 0.255 |
| BMI ≥ 30 kg/m2 | 87 (15.4%) | 1 (7.1%) | 8 (40.0%) | 0.015 |
| Comorbidities | 254 (44.9%) | 14 (100%) | 9 (45.0%) | <0.001 |
| DM | 65 (11.5%) | 1 (7.1%) | 3 (15.0%) | 0.827 |
| HT | 145 (25.6%) | 4 (28.6%) | 4 (20.0%) | 0.860 |
| DLP | 93 (16.4%) | 6 (42.9%) | 2 (10.0%) | 0.038 |
| CKD | 12 (2.1%) | 2 (14.3%) | 0 (0.0%) | 0.063 |
| Chronic lung disease/asthma | 11 (1.9%) | 0 (0.0%) | 0 (0.0%) | 1.000 |
| Cirrhosis | 1 (0.2%) | 0 (0.0%) | 0 (0.0%) | 1.000 |
| ASCVD | 14 (2.5%) | 0 (0.0%) | 0 (0.0%) | 1.000 |
| Number of comorbidities—median (IQR) | 0 (0–1) | 2 (1–3) | 1 (0–1) | <0.001 |
| Symptomatic infection—n (%) | 507 (89.6%) | 14 (100.0%) | 19 (95.0%) | 0.518 |
| Vaccination status before infection—n (%) | <0.001 | |||
| Unvaccinated | 206 (36.4%) | 8 (57.1%) | 6 (30.0%) | |
| Partially vaccinated | 211 (37.3%) | 6 (42.9%) | 2 (10.0%) | |
| Fully vaccinated | 149 (26.3%) | 0 (0.0%) | 12 (60.0%) | |
| Interval between last vaccination and infection—days, median (IQR) | 36.5 (16.8, 58.3) | 35.5 (3.3, 61.8) | 32.0 (17.0, 73.0) | 0.968 |
| Interval between onset and test—days, median (IQR) | 2 (1, 4) | 2 (1, 3) | 2 (1, 3) | 0.438 |
| Ct value (N gene)—mean SD | 21.5 ± 5.8 | 18.8 ± 3.4 | 21.9 ± 5.5 | 0.205 |
| Favipiravir use—n (%) | 543 (95.9%) | 14 (100.0%) | 20 (100.0%) | 1.000 |
| Dexamethasone use—n (%) | 44 (8.0%) | 3 (21.4%) | 1 (5.3%) | 0.156 |
| Fully vaccinated at M3—n (%) | 473 (83.6%) | 12 (85.7%) | 17 (85.0%) | 1.000 |
| Received any booster dose within 3 months postinfection—n (%) | 307 (56.7%) | 11 (78.6%) | 6 (30.0%) | 0.016 |
| Received any booster dose between 3 and 6 months postinfection—n (%) | 291 (65.2%) | 7 (50.0%) | 12 (66.7%) | 0.492 |
| Parameters | Fully Vaccinated (n = 473) | Partially Vaccinated and Unvaccinated (n = 93) | p Value |
|---|---|---|---|
| Age—years (mean ± SD) | 46.0 ± 14.6 | 44.7 ± 15.0 | 0.435 |
| Gender (female)—n (%) | 296 (62.6%) | 52 (55.9%) | 0.227 |
| BW at onset—kg (mean ± SD) | 66.8 ± 15.7 | 65.8 ± 14.7 | 0.562 |
| BMI at onset—kg/m2 (mean ± SD) | 25.5 ± 5.0 | 24.7 ± 5.0 | 0.162 |
| BW at M3—kg (mean ± SD) | 67.6 ± 16.2 | 67.2 ± 15.2 | 0.819 |
| BMI at M3—kg/m2 (mean ± SD) | 25.8 ± 5.2 | 25.2 ± 5.1 | 0.323 |
| Risk factors at onset—n (%) | |||
| Age ≥ 60 yr | 88 (18.6%) | 15 (16.1%) | 0.572 |
| BMI ≥ 30 kg/m2 | 40 (8.5%) | 5 (5.4%) | 0.315 |
| Comorbidities | 80 (16.9%) | 11 (11.8%) | 0.222 |
| DM | 212 (44.8%) | 42 (45.2%) | 0.952 |
| HT | 54 (11.4%) | 11 (11.8%) | 0.909 |
| DLP | 123 (26.0%) | 22 (23.7%) | 0.635 |
| CKD | 83 (17.5%) | 10 (10.8%) | 0.106 |
| Chronic lung disease/asthma | 10 (2.1%) | 2 (2.2%) | 1.000 |
| Cirrhosis | 8 (1.7%) | 3 (3.2%) | 0.401 |
| ASCVD | 1 (0.2%) | 0 (0.0%) | 1.000 |
| Symptomatic infection—n (%) | 422 (89.2%) | 85 (91.4%) | 0.529 |
| Ct ratio (N gene)—mean ± SD | 21.3 ± 5.8 | 22.5 ± 5.7 | 0.071 |
| Favipiravir use—n (%) | 455 (96.2%) | 88 (94.6%) | 0.563 |
| Dexamethasone use—n (%) | 37 (7.9%) | 7 (8.2%) | 0.926 |
| Vaccine Combination before Infection | Anti-RBD IgG (AU/mL) | Nab—Wuhan (%Inhibition) | NAb—Delta (%Inhibition) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| No Booster Dose within 3 Months Postinfection | Booster Dose * within 3 Months Postinfection | p Value | No Booster Dose within 3 Months Postinfection | Booster Dose * within 3 Months Postinfection | p Value | No Booster Dose within 3 Months Postinfection | Booster Dose * within 3 Months Postinfection | p Value | |
| SV or SP for 2 doses (n = 74) | 12.038 (4521, 37.339) | 14.542 (7579, 23,816) | 0.462 | 96.9 (96.0, 97.6) | 97.6 (97.1, 98.1) | 0.004 | 96.6 (76.3, 98.2) | 97.0 (92.5, 98.6) | 0.344 |
| AZ for 2 doses (n = 27) | 9042 (5793, 15,558) | 36,871 (19,183, 36,871) | 0.051 | 97.4 (96.4, 97.6) | 97.6 (97.5, 97.6) | 0.570 | 94.6 (88.4, 98.3) | 96.2 (93.7, 96.2) | 0.462 |
| SV or SP + AZ (n = 39) | 7860 (4370, 15.072) | 17,053 (11,350, 17.053) | 0.219 | 96.2 (95.7, 97.2) | 97.4 (97.1, 97.4) | 0.113 | 91.8 (84.7, 97.7) | 98.1 (97.3, 98.1) | 0.097 |
| SV or SP + PZ (n = 13) | 7000 (4987, 12.343) | N/A | N/A | 96.4 (96.0, 97.6) | N/A | N/A | 84.2 (75.6, 97.5) | N/A | N/A |
| AZ + PZ (n = 4) | 29.639 (9134, 29.639) | 67,495 (67,495, 67.495) | 0.500 | 97.5 (97.5, 97.5) | 96.3 (96.3, 96.3) | 0.500 | 98.1 (93.9, 98.1) | 98.8 (98.8, 98.8) | 0.500 |
| PZ for 2 doses (n = 1) | 3140 (3140, 3140) | N/A | N/A | 91.4 (91.4, 91.4) | N/A | N/A | 58.7 (58.7, 58.7) | N/A | N/A |
| Parameters | Anti-RBD IgG not Decreased | NAb (Wuhan) not Decreased | NAb (Delta) not Decreased | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| cOR | p Value | aOR | p Value | cOR | p Value | aOR | p Value | cOR | p Value | aOR | p Value | |
| Age | 0.99 | 0.062 | 0.97 | 0.005 | 1 | 0.843 | 1.01 | 0.231 | 1 | 0.604 | 0.99 | 0.441 |
| (0.97, 1.00) | (0.95, 0.99) | (0.99, 1.02) | (0.99, 1.03) | (0.98, 1.01) | (0.98, 1.01) | |||||||
| Sex (female) | 1.19 | 0.378 | 0.96 | 0.84 | 1.3 | 0.18 | ||||||
| (0.81, 1.74) | (0.65, 1.43) | (0.89, 1.91) | ||||||||||
| BMI at 3 months | 1.02 | 0.359 | 1 | 0.998 | 1.01 | 0.62 | ||||||
| (0.98, 1.06) | (0.96, 1.04) | (0.97, 1.05) | ||||||||||
| DM | 1.13 | 0.7 | 1.54 | 0.386 | 0.6 | 0.152 | 0.6 | 0.223 | 1.01 | 0.986 | 0.94 | 0.894 |
| (0.61, 2.11) | (0.58, 4.08) | (0.30, 1.21) | (0.27, 1.36) | (0.54, 1.88) | (0.39, 2.29) | |||||||
| HT | 0.95 | 0.827 | 0.87 | 0.535 | 1.03 | 0.912 | ||||||
| (0.62, 1.46) | (0.56, 1.36) | (0.67, 1.58) | ||||||||||
| DLP | 1.23 | 0.414 | 1.83 | 0.141 | 0.74 | 0.266 | 0.66 | 0.238 | 1.37 | 0.235 | 1.57 | 0.254 |
| (0.75, 2.05) | (0.82, 4.07) | (0.43, 1.26) | (0.44, 1.31) | (0.82, 2.29) | (0.72, 3.40) | |||||||
| CKD | 0.46 | 0.274 | 0.27 | 0.17 | 0.84 | 0.805 | 1.58 | 0.575 | 0.95 | 0.944 | 0.94 | 0.945 |
| (0.11, 1.86) | (0.04, 1.76) | (0.21, 3.40) | (0.32, 7.78) | (0.25, 3.60) | (0.16, 5.53) | |||||||
| Chronic lung disease/asthma | 1.88 | 0.47 | 0.84 | 0.841 | 1.54 | 0.622 | ||||||
| (0.34, 10.35) | (0.15, 4.63) | (0.28, 8.47) | ||||||||||
| ASCVD | 1.89 | 0.303 | 1.21 | 0.75 | 1.55 | 0.483 | ||||||
| (0.56, 6.38) | (0.38, 3.87) | (0.46, 5.21) | ||||||||||
| Immunocompromised | 0.51 | 0.23 | 0.61 | 0.523 | 0.93 | 0.902 | 1.32 | 0.652 | 1.02 | 0.973 | 1.79 | 0.417 |
| (0.17, 1.54) | (0.13, 2.77) | (0.31, 2.83) | (0.39, 4.46) | (0.35, 2.99) | (0.44, 7.34) | |||||||
| Reinfection | 1.9 | 0.248 | 2.39 | 0.299 | 1.49 | 0.447 | 1.68 | 0.361 | 1.55 | 0.431 | 1.76 | 0.414 |
| (0.64, 5.65) | (0.46, 12.44) | (0.53, 4.19) | (0.55, 5.12) | (0.52, 4.61) | (0.46, 6.77) | |||||||
| Symptomatic infection | 0.39 | 0.005 | 0.71 | 0.445 | 0.85 | 0.587 | 1.08 | 0.827 | 0.6 | 0.114 | 1.15 | 0.734 |
| (0.20, 0.75) | (0.29, 1.72) | (0.46, 1.55) | (0.54, 2.17) | (0.32, 1.13) | (0.51, 2.59) | |||||||
| Ct ratio (N gene) | 1.03 | 0.108 | 1.04 | 0.122 | 1.01 | 0.772 | 1.01 | 0.729 | 1.01 | 0.7 | 1.01 | 0.727 |
| (0.99, 1.06) | (0.99, 1.10) | (0.97, 1.04) | (0.97, 1.05) | (0.97, 1.04) | (0.96, 1.05) | |||||||
| Favipiravir use | 0.19 | 0.031 | 0.27 | 0.263 | 0.5 | 0.218 | 0.66 | 0.495 | 0.1 | 0.031 | 0.11 | 0.054 |
| (0.04, 0.86) | (0.03, 2.68) | (0.17, 1.51) | (0.19, 2.21) | (0.01, 0.81) | (0.01, 1.04) | |||||||
| Dexamethasone use | 0.67 | 0.226 | 1.27 | 0.602 | 0.57 | 0.122 | 0.66 | 0.279 | 0.54 | 0.06 | 0.7 | 0.374 |
| (0.35, 1.28) | (0.52, 3.12) | (0.28, 1.16) | (0.30, 1.41) | (0.28, 1.03) | (0.31, 1.55) | |||||||
| Booster vaccine within 3 months but no booster vaccine between 3 and 6 months | 0.5 | 0.247 | 0.49 | 0.239 | 0.31 | 0.008 | 0.29 | 0.005 | 0.45 | 0.058 | 0.42 | 0.046 |
| (0.16, 1.61) | (0.15, 1.62) | (0.13, 0.74) | (0.12, 0.68) | (0.20, 1.03) | (0.18, 0.99) | |||||||
| No booster vaccine within 3 months but booster vaccine between 3 and 6 months | 27.36 | <0.001 | 29.89 | <0.001 | 2.64 | 0.001 | 2.53 | 0.003 | 11.47 | <0.001 | 10.83 | <0.001 |
| (12.07, 62.02) | (12.55, 71.15) | (1.45, 4.79) | (1.37, 4.68) | (5.99, 21.95) | (5.56, 21.09) | |||||||
| Booster vaccine at 0–3 months and 3–6 months | 25.3 | <0.001 | 34.05 | <0.001 | 2.29 | 0.009 | 2.26 | 0.012 | 10.95 | <0.001 | 11.55 | <0.001 |
| (10.91, 58.69) | (13.88, 83.55) | (1.23, 4.28) | (1.20, 4.27) | (5.54, 21.64) | (5.74, 23.22) | |||||||
| Vaccine Regimen | Anti-RBD IgG Difference (AU/mL) | NAb (Wuhan) Difference (%Inhibition) | NAb (Delta) Difference (%Inhibition) |
|---|---|---|---|
| 2 inactivated vaccines + 1 AZ + 1 AZ (n = 3) | −1576 (−9668, −1576) | −0.91 (−2.95, −0.91) | −1.13 (−27.23, −1.13) |
| 2 inactivated vaccines + 1 AZ + 1 mRNA (n = 7) | 15.761 (11.323, 30.458) | −0.43 (−1.98, 0.63) | 1.86 (1.52, 15.49) |
| 2 inactivated vaccines + 1 mRNA + 1 mRNA (n = 8) | 10.947 (−6674, 25.067) | −0.90 (−1.44, −0.28) | 1.91 (−0.19, 6.92) |
| p value | 0.117 | 0.788 | 0.788 |
| Antibody Response | Anti-RBD IgG (AU/mL) | NAb—Wuhan (%Inhibition) | NAb—Delta (%Inhibition) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Prior Reinfection | Post Reinfection | p Value | Prior Reinfection | Post Reinfection | p Value | Prior Reinfection | Post Reinfection | p Value | |
| No vaccination within 3 months postinfection (n = 6) | 18.782 (1586, 42.055) | 11.452 (5660, 16.749) | 0.688 | 96.4 (79.2, 98.1) | 96.4 (95.0, 97.1) | 1.000 | 97.8 (18.9, 98.8) | 98.2 (95.7, 98.6) | 1.000 |
| Vaccination within 3 months postinfection (n = 10) * | 5177 (1460, 8062) | 12.039 (5712, 21.486) | 0.021 | 96.3 (92.6, 97.6) | 96.9 (94.7, 97.3) | 1.000 | 83.9 (23.4, 87.3) | 98.0 (80.4, 98.5) | 0.109 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sayabovorn, N.; Phisalprapa, P.; Srivanichakorn, W.; Chaisathaphol, T.; Washirasaksiri, C.; Sitasuwan, T.; Tinmanee, R.; Kositamongkol, C.; Nimitpunya, P.; Mepramoon, E.; et al. Dynamics of Antibody Responses after Asymptomatic and Mild to Moderate SARS-CoV-2 Infections: Real-World Data in a Resource-Limited Country. Trop. Med. Infect. Dis. 2023, 8, 185. https://doi.org/10.3390/tropicalmed8040185
Sayabovorn N, Phisalprapa P, Srivanichakorn W, Chaisathaphol T, Washirasaksiri C, Sitasuwan T, Tinmanee R, Kositamongkol C, Nimitpunya P, Mepramoon E, et al. Dynamics of Antibody Responses after Asymptomatic and Mild to Moderate SARS-CoV-2 Infections: Real-World Data in a Resource-Limited Country. Tropical Medicine and Infectious Disease. 2023; 8(4):185. https://doi.org/10.3390/tropicalmed8040185
Chicago/Turabian StyleSayabovorn, Naruemit, Pochamana Phisalprapa, Weerachai Srivanichakorn, Thanet Chaisathaphol, Chaiwat Washirasaksiri, Tullaya Sitasuwan, Rungsima Tinmanee, Chayanis Kositamongkol, Pongpol Nimitpunya, Euarat Mepramoon, and et al. 2023. "Dynamics of Antibody Responses after Asymptomatic and Mild to Moderate SARS-CoV-2 Infections: Real-World Data in a Resource-Limited Country" Tropical Medicine and Infectious Disease 8, no. 4: 185. https://doi.org/10.3390/tropicalmed8040185
APA StyleSayabovorn, N., Phisalprapa, P., Srivanichakorn, W., Chaisathaphol, T., Washirasaksiri, C., Sitasuwan, T., Tinmanee, R., Kositamongkol, C., Nimitpunya, P., Mepramoon, E., Ariyakunaphan, P., Woradetsittichai, D., Chayakulkeeree, M., Phoompoung, P., Mayurasakorn, K., Sookrung, N., Tungtrongchitr, A., Wanitphakdeedecha, R., Muangman, S., ... Auesomwang, C. (2023). Dynamics of Antibody Responses after Asymptomatic and Mild to Moderate SARS-CoV-2 Infections: Real-World Data in a Resource-Limited Country. Tropical Medicine and Infectious Disease, 8(4), 185. https://doi.org/10.3390/tropicalmed8040185