
Sustained Decline in Hospitalisations for Anogenital Warts in Australia: Analysis of National Hospital Morbidity Data 2003–2020 †



Abstract
1. Introduction
2. Materials and Methods
3. Results
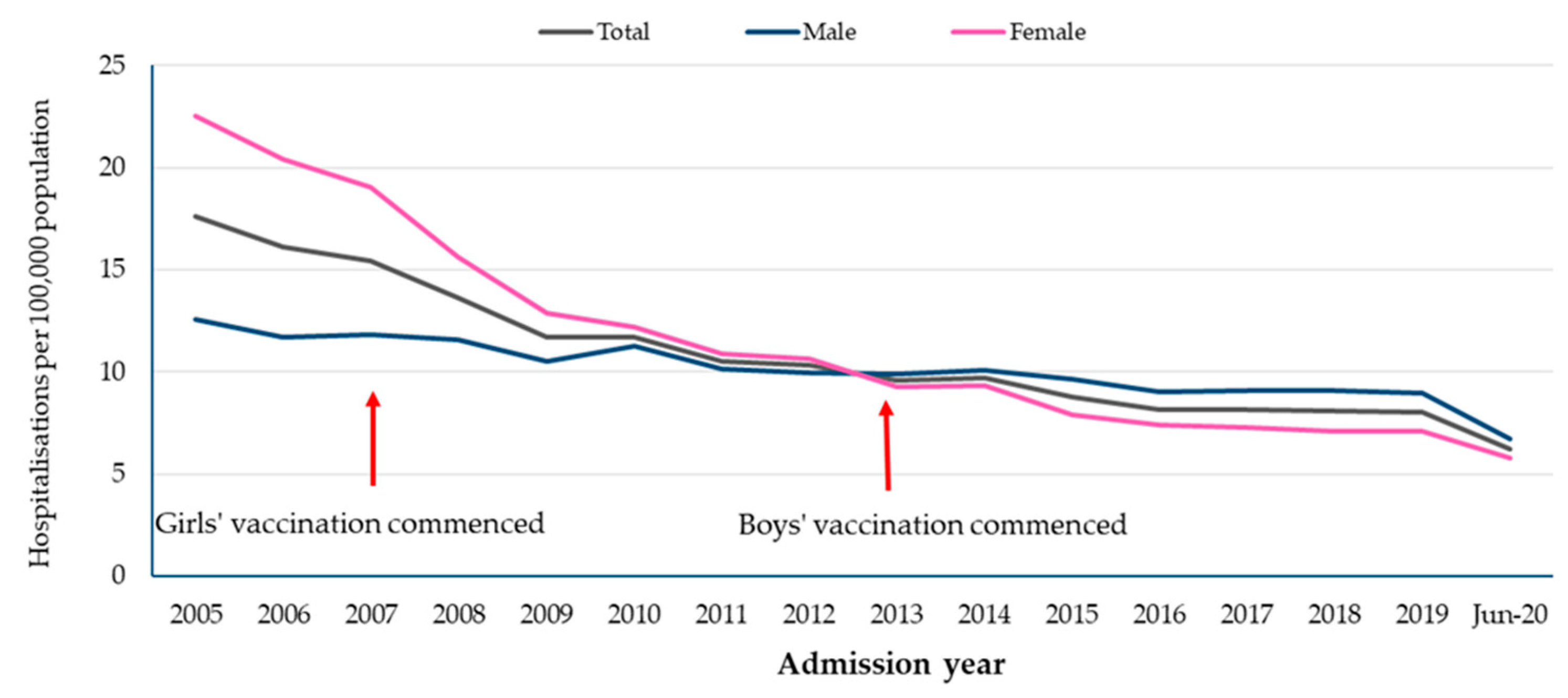
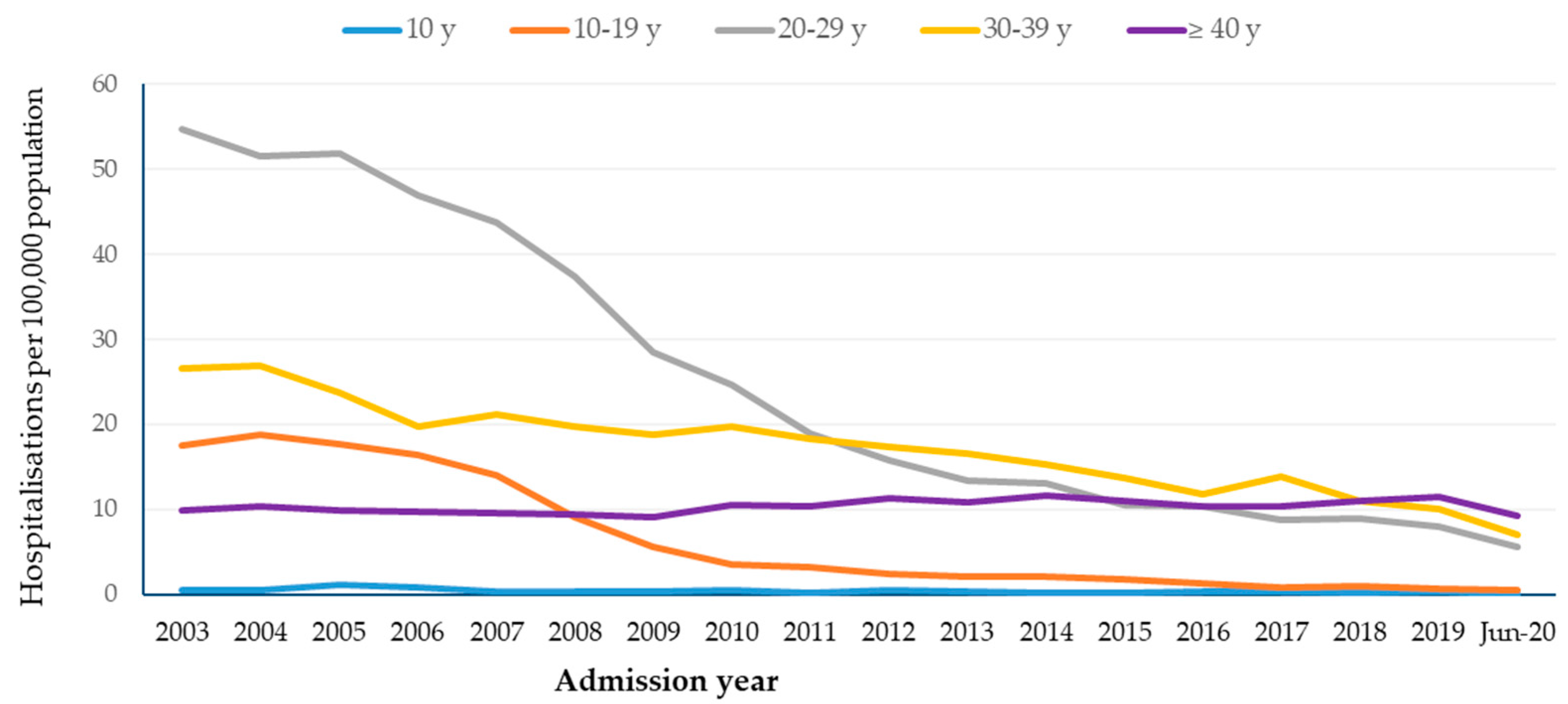
3.1. Hospitalisations by Age and Gender
3.2. Hospitalisations by Indigenous Status
3.3. Hospitalisation Rates by Jurisdiction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brotherton, J.M.L.; Bloem, P.N. Population-based HPV vaccination programmes are safe and effective: 2017 update and the impetus for achieving better global coverage. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 47, 42–58. [Google Scholar] [CrossRef] [PubMed]
- Bouvard, V.; Baan, R.; Straif, K.; Grosse, Y.; Secretan, B.; El Ghissassi, F.; Benbrahim-Tallaa, L.; Guha, N.; Freeman, C.; Galichet, L.; et al. A review of human carcinogens—Part B: Biological agents. Lancet Oncol. 2009, 10, 321–322. [Google Scholar] [CrossRef] [PubMed]
- Garland, S.M.; Steben, M.; Sings, H.L.; James, M.; Lu, S.; Railkar, R.; Railkar, R.; Barr, E.; Haupt, R.M.; Joura, E.A. Natural history of genital warts: Analysis of the placebo arm of 2 randomized phase III trials of a quadrivalent human papillomavirus (types 6, 11, 16, and 18) vaccine. J. Infect. Dis. 2009, 199, 805–814. [Google Scholar] [CrossRef] [PubMed]
- Garland, S.M.; Brotherton, J.M.; Skinner, S.R.; Pitts, M.; Saville, M.; Mola, G.; Jones, R.W. Human papillomavirus and cervical cancer in Australasia and Oceania: Risk-factors, epidemiology and prevention. Vaccine 2008, 26 (Suppl. S12), M80–M88. [Google Scholar] [CrossRef] [PubMed]
- Brotherton, J.; Gertig, D.; Chappell, G.; Rowlands, L.; Saville, M. Catching up with the catch-up: HPV vaccination coverage data for Australian women aged 18–26 years from the National HPV Vaccination Program Register. Commun. Dis. Intell. Q. Rep. 2011, 35, 197–201. [Google Scholar]
- Hull, B.; Dey, A.; Menzies, R.; McIntyre, P. Annual immunisation coverage report, 2010. Commun. Dis. Intell. Q. Rep. 2013, 37, E21–E39. [Google Scholar] [CrossRef] [PubMed]
- Hull, B.; Hendry, A.; Dey, A.; Brotherton, J.; Macartney, K.; Beard, F. Annual immunisation coverage report 2021. Commun. Dis. Intell. 2023, 2018, 47. [Google Scholar] [CrossRef]
- Harrison, C.; Britt, H.; Garland, S.; Conway, L.; Stein, A.; Pirotta, M.; Fairley, C. Decreased management of genital warts in young women in Australian general practice post introduction of national HPV vaccination program: Results from a nationally representative cross-sectional general practice study. PLoS ONE 2014, 9, e105967. [Google Scholar] [CrossRef]
- Liu, B.; Donovan, B.; Brotherton, J.M.; Saville, M.; Kaldor, J.M. Genital warts and chlamydia in Australian women: Comparison of national population-based surveys in 2001 and 2011. Sex. Transm. Infect. 2014, 90, 532–537. [Google Scholar] [CrossRef]
- Smith, M.A.; Liu, B.; McIntyre, P.; Menzies, R.; Dey, A.; Canfell, K. Fall in genital warts diagnoses in the general and indigenous Australian population following implementation of a national human papillomavirus vaccination program: Analysis of routinely collected national hospital data. J. Infect. Dis. 2015, 211, 91–99. [Google Scholar] [CrossRef]
- Wilkinson, E. Australia leads way on HPV vaccination in boys. Lancet Infect. Dis. 2012, 12, 831–832. [Google Scholar] [CrossRef] [PubMed]
- Wnukowski-Mtonga, P.; Jayasinghe, S.; Chiu, C.; Macartney, K.; Brotherton, J.; Donovan, B.; Hall, M.; Smith, D.W.; Peterson, K.; Campbell-Lloyd, S.; et al. Scientific evidence supporting recommendations on the use of the 9-valent HPV vaccine in a 2-dose vaccine schedule in Australia. Commun. Dis. Intell. 2020, 2018, 44. [Google Scholar] [CrossRef]
- Ali, H.; Donovan, B.; Wand, H.; Read, T.R.; Regan, D.G.; Grulich, A.E.; Fairley, C.K.; Guy, R.J. Genital warts in young Australians five years into national human papillomavirus vaccination programme: National surveillance data. BMJ 2013, 346, f2032. [Google Scholar] [CrossRef]
- Ali, H.; Guy, R.J.; Wand, H.; Read, T.R.; Regan, D.G.; Grulich, A.E.; Fairley, C.K.; Donovan, B. Decline in in-patient treatments of genital warts among young Australians following the national HPV vaccination program. BMC Infect. Dis. 2013, 13, 140. [Google Scholar] [CrossRef] [PubMed]
- Ali, H.; McManus, H.; O’Connor, C.C.; Callander, D.; Kong, M.; Graham, S.; Saulo, D.; Fairley, C.K.; Regan, D.G.; Grulich, A.; et al. Human papillomavirus vaccination and genital warts in young Indigenous Australians: National sentinel surveillance data. Med. J. Aust. 2017, 206, 204–209. [Google Scholar] [CrossRef]
- Smith, M.A.; Liu, B.; McIntyre, P.; Menzies, R.; Dey, A.; Canfell, K. Trends in genital warts by socioeconomic status after the introduction of the national HPV vaccination program in Australia: Analysis of national hospital data. BMC Infect. Dis. 2016, 16, 52. [Google Scholar] [CrossRef]
- Donovan, B.; Franklin, N.; Guy, R.; Grulich, A.E.; Regan, D.G.; Ali, H.; Wand, H.; Fairley, C.K. Quadrivalent human papillomavirus vaccination and trends in genital warts in Australia: Analysis of national sentinel surveillance data. Lancet Infect. Dis. 2011, 11, 39–44. [Google Scholar] [CrossRef]
- Fairley, C.K.; Hocking, J.S.; Gurrin, L.C.; Chen, M.Y.; Donovan, B.; Bradshaw, C.S. Rapid decline in presentations of genital warts after the implementation of a national quadrivalent human papillomavirus vaccination programme for young women. Sex. Transm. Infect. 2009, 85, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Hull, B.P.; Dey, A.; Beard, F.H.; Menzies, R.I.; Brotherton, J.M.; McIntyre, P.B. Immunisation coverage annual report, 2013. Commun. Dis. Intell. Q. Rep. 2016, 40, E146–E169. [Google Scholar]
- Khawar, L.; McManus, H.; Vickers, T.; Chow, E.P.F.; Fairley, C.K.; Donovan, B.; Machalek, D.A.; Regan, D.G.; Grulich, A.E.; Guy, R.J.; et al. Genital warts trends in Australian and overseas-born people in Australia: A cross-sectional trend analysis to measure progress towards control and elimination. Lancet Reg. Health West. Pac. 2021, 16, 100251. [Google Scholar] [CrossRef]
- Checchi, M.; Mesher, D.; Mohammed, H.; Soldan, K. Declines in anogenital warts diagnoses since the change in 2012 to use the quadrivalent HPV vaccine in England: Data to end 2017. Sex. Transm. Infect. 2019, 95, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Cocchio, S.; Baldovin, T.; Bertoncello, C.; Buja, A.; Furlan, P.; Saia, M.; Baldo, V. Decline in hospitalization for genital warts in the Veneto region after an HPV vaccination program: An observational study. BMC Infect. Dis. 2017, 17, 249. [Google Scholar] [CrossRef][Green Version]
- Di Martino, G.; Cedrone, F.; Di Giovanni, P.; Tognaccini, L.; Trebbi, E.; Romano, F.; Staniscia, T. The Burden of HPV-Related Hospitalizations: Analysis of Hospital Discharge Records from the Years 2015-2021 from a Southern Italian Region. Pathogens 2023, 12, 725. [Google Scholar] [CrossRef]
- Flagg, E.W.; Torrone, E.A. Declines in Anogenital Warts Among Age Groups Most Likely to Be Impacted by Human Papillomavirus Vaccination, United States, 2006–2014. Am. J. Public Health 2018, 108, 112–119. [Google Scholar] [CrossRef]
- Nygård, S.; Nygård, M.; Orumaa, M.; Hansen, B.T. Quadrivalent HPV vaccine effectiveness against anogenital warts: A registry-based study of 2,2 million individuals. Vaccine 2023, 41, 5469–5476. [Google Scholar] [CrossRef] [PubMed]
- Drolet, M.; Bénard, É.; Pérez, N.; Brisson, M. Population-level impact and herd effects following the introduction of human papillomavirus vaccination programmes: Updated systematic review and meta-analysis. Lancet 2019, 394, 497–509. [Google Scholar] [CrossRef] [PubMed]
- Steben, M.; Garland, S.M. Genital warts. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 1063–1073. [Google Scholar] [CrossRef]
- Hull, B.; Hendry, A.; Dey, A.; Brotherton, J.; Macartney, K.; Beard, F. Annual Immunisation Coverage Report 2017. Commun. Dis. Intell. 2019, 2018. [Google Scholar] [CrossRef]
- Soares, G.H.; Sethi, S.; Hedges, J.; Jamieson, L. Disparities in Human Papillomavirus vaccination coverage among adolescents in Australia: A geospatial analysis. Vaccine 2022, 40, 4644–4653. [Google Scholar] [CrossRef]
- Chow, E.P.F.; Carter, A.; Vickers, T.; Fairley, C.K.; McNulty, A.; Guy, R.J.; Regan, D.G.; Grulich, A.E.; Callander, D.; Khawar, L.; et al. Effect on genital warts in Australian female and heterosexual male individuals after introduction of the national human papillomavirus gender-neutral vaccination programme: An analysis of national sentinel surveillance data from 2004–2018. Lancet Infect. Dis. 2021, 21, 1747–1756. [Google Scholar] [CrossRef]
- Brotherton, J.M.; Heywood, A.; Heley, S. The incidence of genital warts in Australian women prior to the national vaccination program. Sex Health 2009, 6, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Read, T.R.; Hocking, J.S.; Chen, M.Y.; Donovan, B.; Bradshaw, C.S.; Fairley, C.K. The near disappearance of genital warts in young women 4 years after commencing a national human papillomavirus (HPV) vaccination programme. Sex Transm. Infect. 2011, 87, 544–547. [Google Scholar] [CrossRef] [PubMed]
- Chow, E.P.; Lin, A.C.; Read, T.R.; Bradshaw, C.S.; Chen, M.Y.; Fairley, C.K. Ratio of anogenital warts between different anatomical sites in homosexual and heterosexual individuals in Australia, 2002–2013: Implications for susceptibility of different anatomical sites to genital warts. Epidemiol. Infect. 2015, 143, 1495–1499. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age Group | 2003–2007 (a) | 2008–2020 (b) | Rate Ratio (b/a) | 95%CI |
|---|---|---|---|---|
| All Australians | ||||
| <10 years | 0.6 | 0.3 | 0.46 | 0.22–1.11 |
| 10–19 years | 16.9 | 2.6 | 0.15 | 0.12–0.19 |
| 20–29 years | 49.6 | 15.2 | 0.31 | 0.28–0.34 |
| 30–39 years | 23.6 | 14.6 | 0.62 | 0.55–0.69 |
| ≥40 years | 9.9 | 10.5 | 1.07 | 0.98–1.17 |
| Total | 17.1 | 9.5 | 0.55 | 0.53–0.58 |
| Aboriginal and Torres Strait Islander | ||||
| <10 years | 1.3 | 0.4 | 0.28 | 0.04–4.97 |
| 10–19 years | 20.4 | 3.1 | 0.15 | 0.06–0.39 |
| 20–29 years | 24.8 | 11.0 | 0.45 | 0.23–0.88 |
| 30–39 years | 14.0 | 15.5 | 1.11 | 0.53–2.35 |
| ≥40 years | 6.0 | 12.8 | 2.13 | 0.99–4.87 |
| Total | 11.8 | 7.8 | 0.66 | 0.47–0.93 |
| Non-Indigenous | ||||
| <10 years | 0.6 | 0.3 | 0.49 | 0.21–1.18 |
| 10–19 years | 16.7 | 2.6 | 0.15 | 0.12–0.20 |
| 20–29 years | 50.5 | 15.4 | 0.30 | 0.27–0.34 |
| 30–39 years | 23.9 | 14.6 | 0.61 | 0.54–0.69 |
| ≥40 years | 9.9 | 10.5 | 1.06 | 0.97–1.16 |
| Total | 17.3 | 9.5 | 0.55 | 0.52–0.58 |
| Age Group | 2003–2007 (a) | 2008–2020 (b) | Rate Ratio (b/a) | 95%CI |
|---|---|---|---|---|
| Aboriginal and Torres Strait Islander Male | ||||
| <10 years | 0.7 | 0.3 | 0.46 | 0.01–7.39 |
| 10–19 years | 2.1 | 1.1 | 0.54 | 0.05–13.07 |
| 20–29 years | 10.7 | 8.8 | 0.82 | 0.27–2.85 |
| 30–39 years | 12.7 | 11.1 | 0.87 | 0.24–2.59 |
| ≥40 years | 3.9 | 10.5 | 2.72 | 0.65–8.62 |
| Total | 4.9 | 5.7 | 1.18 | 0.62–2.30 |
| Aboriginal and Torres Strait Islander Female | ||||
| <10 years | 2.0 | 0.4 | 0.22 | 0.01–3.75 |
| 10–19 years | 39.5 | 5.1 | 0.13 | 0.04–0.36 |
| 20–29 years | 38.8 | 13.4 | 0.34 | 0.15–0.77 |
| 30–39 years | 15.2 | 19.8 | 1.30 | 0.47–3.42 |
| ≥40 years | 8.0 | 14.8 | 1.86 | 0.68–4.49 |
| Total | 18.7 | 9.8 | 0.52 | 0.35–0.79 |
| Non-Indigenous Male | ||||
| <10 years | 0.4 | 0.2 | 0.53 | 0.12–2.18 |
| 10–19 years | 2.8 | 1.8 | 0.62 | 0.38–1.04 |
| 20–29 years | 30.3 | 15.4 | 0.51 | 0.44–0.59 |
| 30–39 years | 21.4 | 13.9 | 0.65 | 0.55–0.77 |
| ≥40 years | 10.6 | 11.5 | 1.09 | 0.96–1.23 |
| Total | 12.6 | 9.8 | 0.78 | 0.72–0.84 |
| Non-Indigenous Female | ||||
| <10 years | 0.8 | 0.4 | 0.47 | 0.16–1.44 |
| 10–19 years | 31.3 | 3.4 | 0.11 | 0.08–0.15 |
| 20–29 years | 71.2 | 15.3 | 0.21 | 0.19–0.25 |
| 30–39 years | 26.3 | 15.2 | 0.58 | 0.49–0.68 |
| ≥40 years | 9.3 | 9.5 | 1.03 | 0.90–1.17 |
| Total | 22.0 | 9.3 | 0.42 | 0.39–0.46 |
| Age Group | Aboriginal and Torres Strait Islander (a) | Non-Indigenous (b) | Rate Ratio (a/b) | 95%CI |
|---|---|---|---|---|
| 2003–2007 | ||||
| <10 years | 1.3 | 0.6 | 2.33 | 0.51–10.06 |
| 10–19 years | 20.4 | 16.7 | 1.22 | 0.82–1.78 |
| 20–29 years | 24.8 | 50.5 | 0.49 | 0.32–0.73 |
| 30–39 years | 14.0 | 23.9 | 0.59 | 0.34–1.03 |
| ≥40 years | 6.0 | 9.9 | 0.61 | 0.29–1.16 |
| Total | 11.8 | 17.3 | 0.68 | 0.54–0.86 |
| 2008–2013 | ||||
| <10 years | 0.6 | 0.4 | 1.53 | 0.19–11.57 |
| 10–19 years | 4.7 | 4.3 | 1.08 | 0.49–2.27 |
| 20–29 years | 14.5 | 23.1 | 0.63 | 0.38–1.01 |
| 30–39 years | 14.7 | 18.5 | 0.79 | 0.45–1.36 |
| ≥40 years | 11.7 | 10.3 | 1.14 | 0.75–1.79 |
| Total | 8.2 | 11.3 | 0.72 | 0.56–0.93 |
| 2014–2020 | ||||
| <10 years | 0.2 | 0.2 | 1.10 | 0.07–21.45 |
| 10–19 years | 1.8 | 1.1 | 1.67 | 0.48–5.17 |
| 20–29 years | 8.7 | 9.3 | 0.93 | 0.52–1.64 |
| 30–39 years | 16.2 | 11.6 | 1.40 | 0.86–2.33 |
| ≥40 years | 13.5 | 10.7 | 1.27 | 0.86–1.80 |
| Total | 7.5 | 8.2 | 0.92 | 0.71–1.18 |
| Age group | 2003–2007 (a) | 2008–2020 (b) | RR (b/a) | 95%CI |
|---|---|---|---|---|
| New South Wales | ||||
| <10 years | 0.5 | 0.2 | 0.52 | 0.08–2.47 |
| 10–19 years | 14.9 | 2.2 | 0.15 | 0.10–0.24 |
| 20–29 years | 46.2 | 14.5 | 0.31 | 0.26–0.38 |
| 30–39 years | 22.1 | 13.6 | 0.61 | 0.50–0.76 |
| ≥40 years | 9.7 | 9.9 | 1.02 | 0.87–1.19 |
| Total | 16.0 | 8.9 | 0.56 | 0.50–0.61 |
| Victoria | ||||
| <10 years | 0.7 | 0.4 | 0.48 | 0.12–2.13 |
| 10–19 years | 16.0 | 2.2 | 0.14 | 0.08–0.24 |
| 20–29 years | 59.4 | 16.0 | 0.27 | 0.22–0.33 |
| 30–39 years | 28.6 | 16.3 | 0.57 | 0.46–0.70 |
| ≥40 years | 11.2 | 11.2 | 1.00 | 0.84–1.18 |
| Total | 19.9 | 10.2 | 0.51 | 0.46–0.57 |
| Queensland | ||||
| <10 years | 0.6 | 0.3 | 0.48 | 0.09–3.37 |
| 10–19 years | 18.1 | 2.6 | 0.14 | 0.09–0.24 |
| 20–29 years | 40.9 | 13.0 | 0.32 | 0.25–0.41 |
| 30–39 years | 20.0 | 13.5 | 0.68 | 0.51–0.89 |
| ≥40 years | 7.9 | 11.3 | 1.43 | 1.16–1.77 |
| Total | 14.7 | 9.3 | 0.63 | 0.56–0.71 |
| Australian Capital Territory | ||||
| <10 years | 0.0 | 0.3 | 0.82 | 0.02–41.10 |
| 10–19 years | 11.1 | 0.2 | 0.02 | 0.01–1.63 |
| 20–29 years | 28.5 | 8.0 | 0.28 | 0.10–0.72 |
| 30–39 years | 15.5 | 7.2 | 0.46 | 0.17–1.58 |
| ≥40 years | 6.6 | 6.3 | 0.95 | 0.37–2.26 |
| Total | 11.5 | 5.2 | 0.45 | 0.27–0.80 |
| South Australia | ||||
| <10 years | 0.3 | 0.2 | 0.59 | 0.01–7.59 |
| 10–19 years | 17.0 | 3.1 | 0.18 | 0.07–0.41 |
| 20–29 years | 52.0 | 13.8 | 0.27 | 0.18–0.40 |
| 30–39 years | 21.8 | 14.4 | 0.66 | 0.41–1.02 |
| ≥40 years | 9.4 | 8.6 | 0.91 | 0.66–1.27 |
| Total | 16.5 | 8.4 | 0.51 | 0.41–0.62 |
| Tasmania | ||||
| <10 years | 0.8 | 0.2 | 0.20 | 0.01–8.56 |
| 10–19 years | 34.7 | 5.6 | 0.16 | 0.05–0.58 |
| 20–29 years | 78.0 | 25.3 | 0.32 | 0.17–0.62 |
| 30–39 years | 21.1 | 24.1 | 1.15 | 0.47–2.51 |
| ≥40 years | 9.5 | 14.7 | 1.55 | 0.88–2.80 |
| Total | 21.6 | 14.3 | 0.66 | 0.47–0.93 |
| Northern Territory | ||||
| <10 years | 1.2 | 0.4 | 0.36 | 0.01–7.76 |
| 10–19 years | 10.1 | 2.6 | 0.26 | 0.03–3.18 |
| 20–29 years | 32.7 | 11.7 | 0.36 | 0.13–1.08 |
| 30–39 years | 24.8 | 11.7 | 0.47 | 0.16–1.46 |
| ≥40 years | 12.5 | 11.6 | 0.93 | 0.36–2.18 |
| Total | 15.7 | 8.7 | 0.56 | 0.33–0.98 |
| Western Australia | ||||
| <10 years | 1.0 | 0.3 | 0.29 | 0.03–2.61 |
| 10–19 years | 21.7 | 4.0 | 0.18 | 0.10–0.33 |
| 20–29 years | 53.2 | 20.0 | 0.38 | 0.28–0.50 |
| 30–39 years | 25.7 | 15.7 | 0.61 | 0.43–0.86 |
| ≥40 years | 11.8 | 11.1 | 0.94 | 0.72–1.22 |
| Total | 19.6 | 10.8 | 0.55 | 0.47–0.64 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rashid, H.; Dey, A.; Wang, H.; Beard, F. Sustained Decline in Hospitalisations for Anogenital Warts in Australia: Analysis of National Hospital Morbidity Data 2003–2020. Trop. Med. Infect. Dis. 2024, 9, 79. https://doi.org/10.3390/tropicalmed9040079
Rashid H, Dey A, Wang H, Beard F. Sustained Decline in Hospitalisations for Anogenital Warts in Australia: Analysis of National Hospital Morbidity Data 2003–2020. Tropical Medicine and Infectious Disease. 2024; 9(4):79. https://doi.org/10.3390/tropicalmed9040079
Chicago/Turabian StyleRashid, Harunor, Aditi Dey, Han Wang, and Frank Beard. 2024. "Sustained Decline in Hospitalisations for Anogenital Warts in Australia: Analysis of National Hospital Morbidity Data 2003–2020" Tropical Medicine and Infectious Disease 9, no. 4: 79. https://doi.org/10.3390/tropicalmed9040079
APA StyleRashid, H., Dey, A., Wang, H., & Beard, F. (2024). Sustained Decline in Hospitalisations for Anogenital Warts in Australia: Analysis of National Hospital Morbidity Data 2003–2020. Tropical Medicine and Infectious Disease, 9(4), 79. https://doi.org/10.3390/tropicalmed9040079