
Capturing Recent Mycobacterium tuberculosis Infection by Tuberculin Skin Test vs. Interferon-Gamma Release Assay


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Population
2.3. Inclusion Criteria for Household Contacts
2.4. Exclusion Criteria for Household Contacts
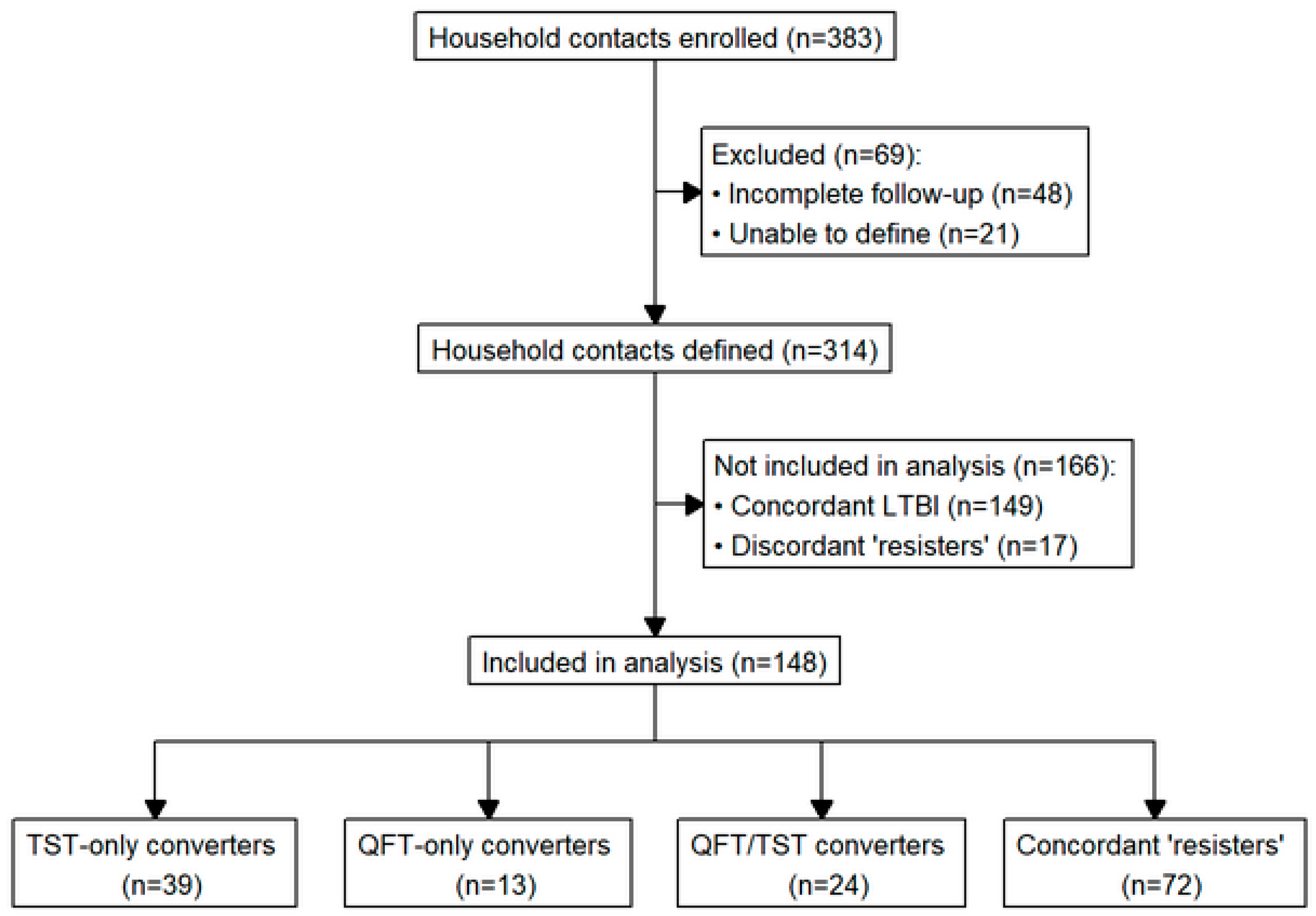
2.5. Study Design
2.6. Definitions
- A person with LTBI was defined as an HHC with all positive QFT and TST results.
- A QFT-only conversion was based on at least three QFT results, requiring a negative QFT at baseline followed by at least one positive QFT result during follow-up, accompanied by TST results that did not change throughout the study.
- A TST-only conversion was based on two TST results (baseline and month 12) and was defined as an original TST of < 10 mm (or < 5 mm for HIV+ individuals) followed by a TST reaction of ≥ 10 mm (or ≥ 5 mm for HIV+ individuals) on subsequent testing with an increase of ≥ 6 mm [33], accompanied by QFT results that remained positive or negative throughout the study.
- A QFT/TST conversion was defined as a conversion of both the QFT and TST as described above. There were six QFT converters (five QFT/TST converters and one QFT-only converter) who had only one positive QFT result because it occurred at month 12. These QFT converters were included in the analysis.
2.7. Statistical Analyses
3. Results
3.1. Differences in Classification among All Classified HHCs by Type of Test
3.2. Individual, Household, and TB Index Characteristics of TST-Only, QFT-Only, and TST/QFT Converters
3.3. Identifying Predictors of QFT and TST Conversion

{kind=link}
{kind=link}
{kind=link}
| QFT-Only Converters | TST-Only Converters | QFT/TST Converters | “Resisters” | p-Value (Test) | Relevant Pairwise p-Value | |
|---|---|---|---|---|---|---|
| Sex (female) | 8 (61.5%) | 20 (51.3%) | 17 (70.8%) | 35 (48.6%) | 0.26 (Fisher’s) | NA |
| BCG scar present | 10 (76.9%) | 30 (76.9%) | 17 (73.9%) | 36 (56.3%) | 0.10 (Fisher’s) | NA |
| HIV positive | 1 (10.0%) | 4 (12.9%) | 0 (0%) | 12 (18.8%) | 0.14 (Fisher’s) | NA |
| BMI | 19 [17–21] | 18.5 [17–21] | 18 [17–20] | 19 [18–20] | 0.42 (KW test) | NA |
| Cavitary lesions present | 11 (84.6%) | 32 (82.1%) | 22 (91.7%) | 43 (60.6%) | 0.006 * (Fisher’s) | TST-only vs. “Resister”: 0.03 * QFT/TST vs. “Resister”: 0.005 * |
| Advanced lung disease | 3 (23.1%) | 24 (61.5%) | 14 (58.3%) | 25 (35.2%) | 0.01 * (Fisher’s) | TST-only vs. QFT-only: 0.04 * TST-only vs. “Resister”: 0.01 * |
| Positive Smear | 8 (88.9%) | 29 (100%) | 20 (100%) | 55 (100%) | 0.08 (Fisher’s) | NA |
| Positive GeneXpert | 13 (100%) | 39 (100%) | 24 (100%) | 71 (98.6%) | 1.00 (Fisher’s) | NA |
| Coughing | 13 (100%) | 39 (100%) | 24 (100%) | 71 (100%) | 1.00 (Fisher’s) | NA |
| Cough duration (days) | 60 [60–90] | 90 [60–142.5] | 52.5 [30–60] | 60 [30–90] | 0.03 * (KW test) | TST-only vs. QFT/TST: 0.007 * TST-only vs. “Resister”: 0.017 * |
| Fever | 9 (69.2%) | 30 (76.9%) | 19 (79.2%) | 54 (76.1%) | 0.92 (Χ2) | NA |
| Fever duration (days) | 42 [14–75] | 60 [30–90] | 30 [27.8–60] | 30 [14–56.3] | 0.10 (KW test) | NA |
| Productive sputum | 13 (100%) | 36 (92.3%) | 24 (100%) | 68 (95.8%) | 0.55 (Fisher’s) | NA |
| Productive sputum duration (days) | 30 [30–90] | 60 [30–120] | 30 [27.8–60] | 30 [30–60] | 0.11 (KW test) | NA |
| Purulent sputum | 6 (46.2%) | 22 (56.4%) | 14 (58.3%) | 37 (52.9%) | 0.89 (Χ2) | NA |
| Purulent sputum duration (days) | 45 [30–60] | 52.5 [30–120] | 30 [23.3–60] | 30 [15–90] | 0.25 (KW test) | NA |
| Hemoptysis | 1 (7.7%) | 4 (10.3%) | 8 (33.3%) | 7 (10.0%) | 0.04 * (Fisher’s) | QFT/TST vs. “Resisters”: 0.02 * QFT/TST vs. TST-only: 0.04 * |
| Hemoptysis duration (days) | 14 [14–14] | 5 [2.5–12.8] | 2 [1.5–5] | 7 [2.5–10.5] | 0.58 (KW test) | NA |
| Dyspnea | 6 (46.2%) | 20 (52.6%) | 10 (41.7%) | 38 (53.5%) | 0.77 (Fisher’s) | NA |
| Dyspnea duration (days) | 60 [37.5–60] | 90 [30–160] | 60 [37.5–90] | 30 [30–82.5] | 0.18 (KW test) | NA |
| Weight loss | 12 (92.3%) | 33 (84.6%) | 18 (75%) | 59 (83.1%) | 0.62 (Fisher’s) | NA |
| Weight loss duration (days) | 60 [27.8–78.8] | 60 [30–90] | 52.5 [30–71.3] | 30 [30–82.5] | 0.20 (KW test) | NA |
| Covariates | N | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|---|
| Age (years) | NA | 1.05 | 1.01–1.10 | 0.020 * |
| Presence of cavitary lesions | ||||
| No | 11 | (Ref.) | (Ref.) | (Ref.) |
| Yes | 65 | 0.29 | 0.055–1.310 | 0.118 |
| Index cough duration (days) | NA | 1.01 | 1.000–1.018 | 0.099 |
| Epidemiologic risk score | NA | 0.61 | 0.375–0.956 | 0.038 * |
| People per room | NA | 1.559 | 1.085–2.404 | 0.025 * |
| Advanced lung disease | ||||
| Not far advanced | 35 | (Ref.) | (Ref.) | (Ref.) |
| Far advanced | 41 | 2.58 | 0.818–8.866 | 0.115 |
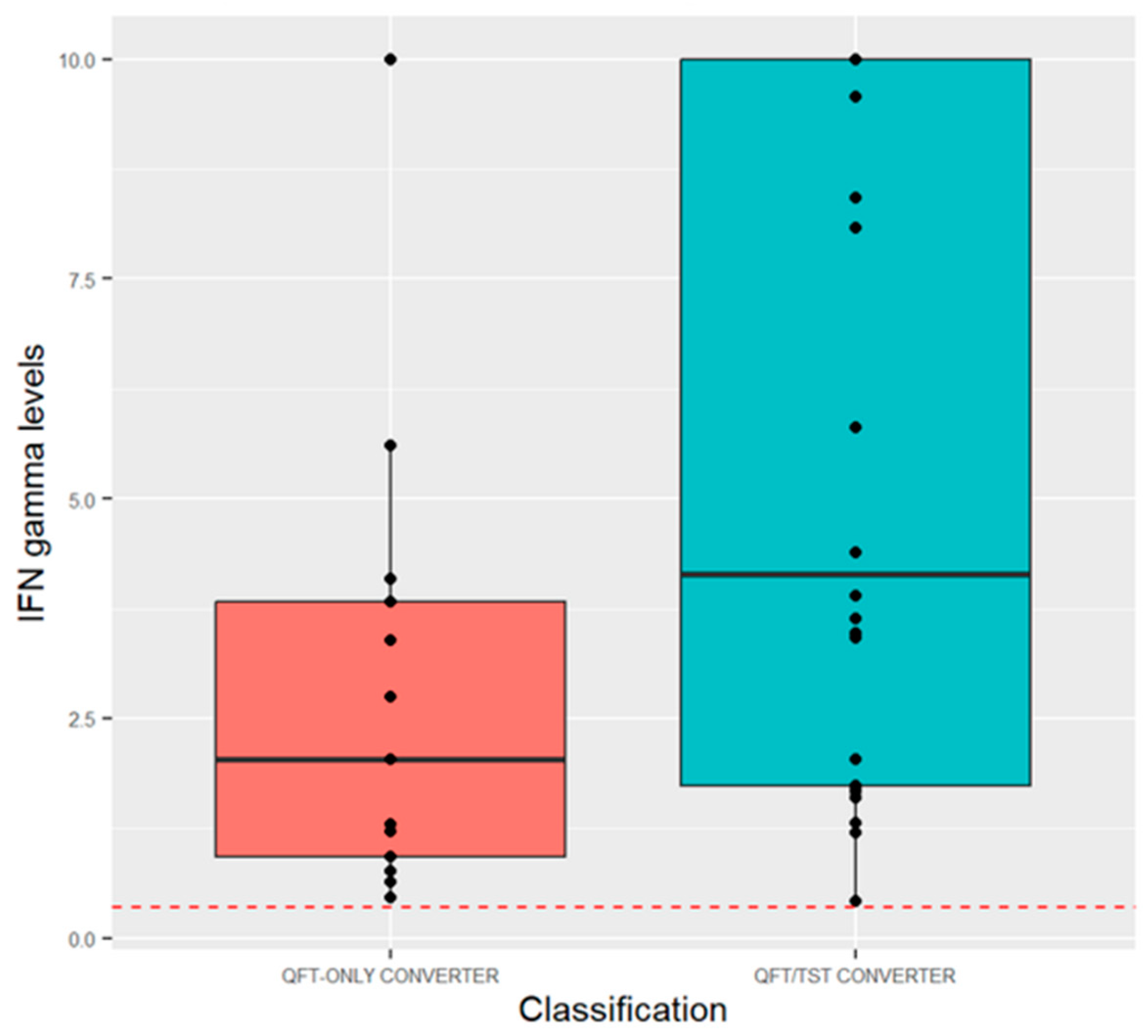
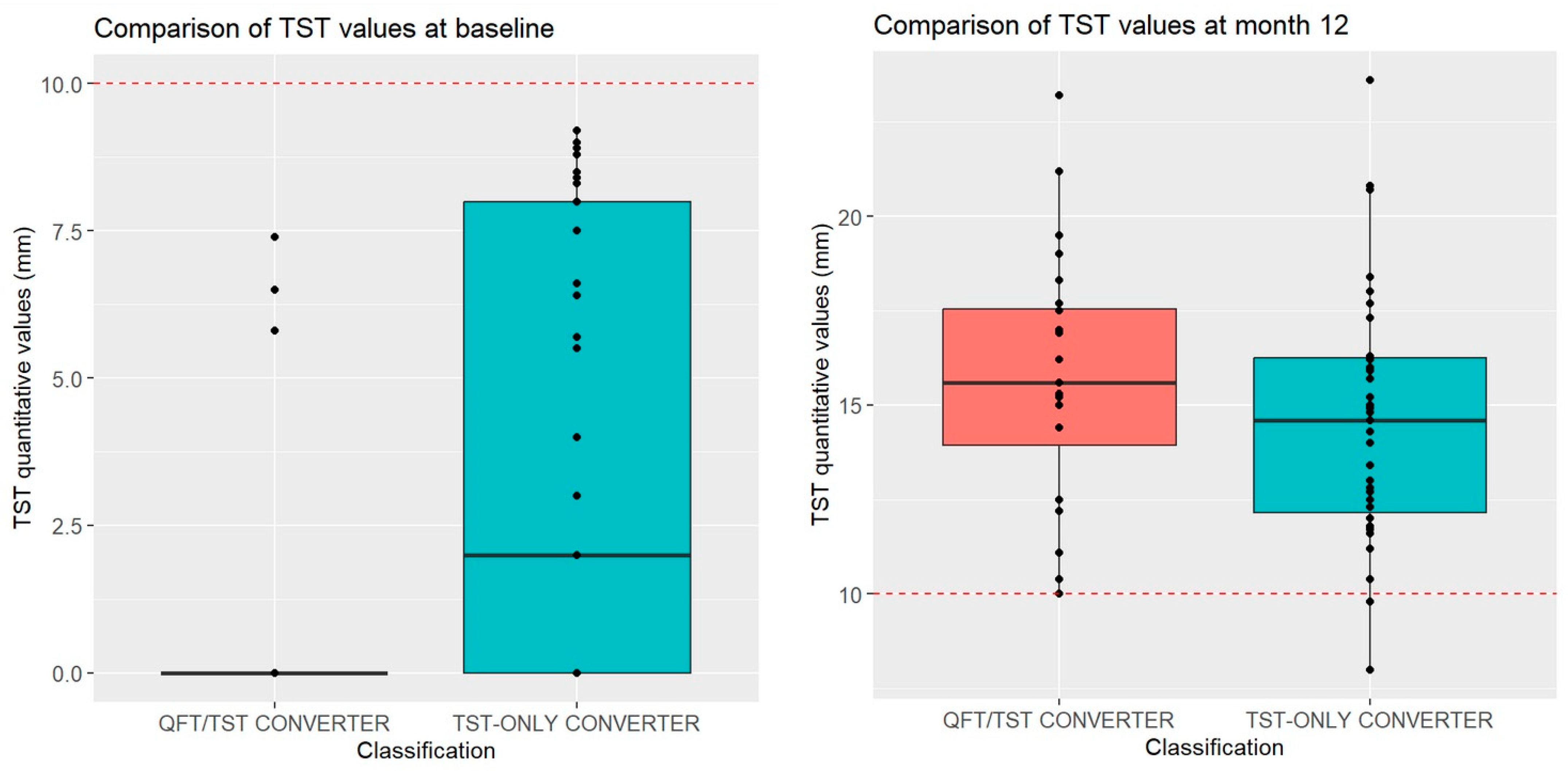
3.4. Quantitative QFT and TST Values for TST, QFT, and TST/QFT Converters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2023; World Health Organization: Geneva, Switzerland, 2023.
- World Health Organization. Implementing the End TB Strategy: The Essentials; World Health Organization: Geneva, Switzerland, 2016.
- Behr, M.A.; Kaufmann, E.; Duffin, J.; Edelstein, P.H.; Ramakrishnan, L. Latent Tuberculosis: Two Centuries of Confusion. Am. J. Respir. Crit. Care Med. 2021, 204, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Reichler, M.R.; Khan, A.; Sterling, T.R.; Zhao, H.; Chen, B.; Yuan, Y.; Moran, J.; McAuley, J.; Mangura, B.; Tuberculosis Epidemiologic Studies Consortium Task Order 2 Team; et al. Risk Factors for Tuberculosis and Effect of Preventive Therapy Among Close Contacts of Persons With Infectious Tuberculosis. Clin. Infect. Dis. 2020, 70, 1562–1572. [Google Scholar] [CrossRef]
- Sloot, R.; van der Loeff, M.F.S.; Kouw, P.M.; Borgdorff, M.W. Risk of tuberculosis after recent exposure. A 10-year follow-up study of contacts in Amsterdam. Am. J. Respir. Crit. Care Med. 2014, 190, 1044–1052. [Google Scholar] [CrossRef] [PubMed]
- Behr, M.A.; Edelstein, P.H.; Ramakrishnan, L. Revisiting the timetable of tuberculosis. BMJ 2018, 362, k2738. [Google Scholar] [CrossRef] [PubMed]
- Zellweger, J.P.; Sotgiu, G.; Corradi, M.; Durando, P. The diagnosis of latent tuberculosis infection (LTBI): Currently available tests, future developments, and perspectives to eliminate tuberculosis (TB). Med. Lav. 2020, 111, 170–183. [Google Scholar]
- Stein, C.M.; Mayanja-Kizza, H.; Hawn, T.R.; Boom, W.H. Importance of Study Design and Phenotype Definition in Ongoing Studies of Resistance to Latent Mycobacterium tuberculosis Infection. J. Infect. Dis. 2020, 221, 1025–1026. [Google Scholar] [CrossRef]
- Behr, M.A.; Edelstein, P.H.; Ramakrishnan, L. Is Mycobacterium tuberculosis infection life long? BMJ 2019, 367, l5770. [Google Scholar] [CrossRef]
- Boom, W.H.; Schaible, U.E.; Achkar, J.M. The knowns and unknowns of latent Mycobacterium tuberculosis infection. J. Clin. Investig. 2021, 131, l5770. [Google Scholar] [CrossRef] [PubMed]
- Chee, C.B.; KhinMar, K.W.; Gan, S.H.; Barkham, T.M.; Koh, C.K.; Shen, L.; Wang, Y.T. Tuberculosis treatment effect on T-cell interferon-gamma responses to Mycobacterium tuberculosis-specific antigens. Eur. Respir. J. 2010, 36, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Takenami, I.; Finkmoore, B.; Machado, A., Jr.; Emodi, K.; Riley, L.W.; Arruda, S. Levels of interferon-gamma increase after treatment for latent tuberculosis infection in a high-transmission setting. Pulm. Med. 2012, 2012, 757152. [Google Scholar] [CrossRef] [PubMed]
- Dyrhol-Riise, A.M.; Gran, G.; Wentzel-Larsen, T.; Blomberg, B.; Haanshuus, C.G.; Morkve, O. Diagnosis and follow-up of treatment of latent tuberculosis; the utility of the QuantiFERON-TB Gold In-tube assay in outpatients from a tuberculosis low-endemic country. BMC Infect. Dis. 2010, 10, 57. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kim, O.H.; Jo, K.W.; Park, S.; Jo, Y.H.; Kim, M.N.; Sung, H.; Shim, T.S. Comparison of the change in QuantiFERON-TB Gold Plus and QuantiFERON-TB Gold In-Tube results after preventive therapy for latent tuberculosis infection. PLoS ONE 2020, 15, e0234700. [Google Scholar] [CrossRef]
- Ewer, K.; Deeks, J.; Alvarez, L.; Bryant, G.; Waller, S.; Andersen, P.; Monk, P.; Lalvani, A. Comparison of T-cell-based assay with tuberculin skin test for diagnosis of Mycobacterium tuberculosis infection in a school tuberculosis outbreak. Lancet 2003, 361, 1168–1173. [Google Scholar] [CrossRef]
- Lalvani, A.; Pathan, A.A.; McShane, H.; Wilkinson, R.J.; Latif, M.; Conlon, C.P.; Pasvol, G.; Hill, A.V. Rapid detection of Mycobacterium tuberculosis infection by enumeration of antigen-specific T cells. Am. J. Respir. Crit. Care Med. 2001, 163, 824–828. [Google Scholar] [CrossRef] [PubMed]
- Brock, I.; Weldingh, K.; Lillebaek, T.; Follmann, F.; Andersen, P. Comparison of tuberculin skin test and new specific blood test in tuberculosis contacts. Am. J. Respir. Crit. Care Med. 2004, 170, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Pai, M.; Zwerling, A.; Menzies, D. Systematic review: T-cell-based assays for the diagnosis of latent tuberculosis infection: An update. Ann. Intern. Med. 2008, 149, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Lalvani, A. Diagnosing tuberculosis infection in the 21st century: New tools to tackle an old enemy. Chest 2007, 131, 1898–1906. [Google Scholar] [CrossRef]
- Drobniewski, F.; Cobelens, F.; Zellweger, J.P.; Workshop, K.N.E. Use of Gamma-interferon assays in low- and medium-prevalence countries in Europe: A consensus statement of a Wolfheze Workshop organised by KNCV/EuroTB, Vilnius Sept 2006. Euro Surveill. 2007, 12, E070726.2. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.C.; Wang, P.H.; Chen, K.T. Use of the QuantiFERON-TB Gold In-Tube Test in the Diagnosis and Monitoring of Treatment Efficacy in Active Pulmonary Tuberculosis. Int. J. Environ. Res. Public Health 2017, 14, 236. [Google Scholar] [CrossRef] [PubMed]
- Moses, M.W.; Zwerling, A.; Cattamanchi, A.; Denkinger, C.M.; Banaei, N.; Kik, S.V.; Metcalfe, J.; Pai, M.; Dowdy, D. Serial testing for latent tuberculosis using QuantiFERON-TB Gold In-Tube: A Markov model. Sci. Rep. 2016, 6, 30781. [Google Scholar] [CrossRef]
- Stein, C.M.; Hall, N.B.; Malone, L.L.; Mupere, E. The household contact study design for genetic epidemiological studies of infectious diseases. Front. Genet. 2013, 4, 61. [Google Scholar] [CrossRef]
- Garcia-Basteiro, A.L.; White, R.G.; Tait, D.; Schmidt, A.C.; Rangaka, M.X.; Quaife, M.; Nemes, E.; Mogg, R.; Hill, P.C.; Harris, R.C.; et al. End-point definition and trial design to advance tuberculosis vaccine development. Eur. Respir. Rev. 2022, 31, 220044. [Google Scholar] [CrossRef] [PubMed]
- Aceng, J.R. The Uganda National Tuberculosis Prevalence Survey, 2014–2015; The Republic of Uganda, Ministry of Health: Kampala, Uganda, 2016.
- Sekandi, J.N.; List, J.; Luzze, H.; Yin, X.P.; Dobbin, K.; Corso, P.S.; Oloya, J.; Okwera, A.; Whalen, C.C. Yield of undetected tuberculosis and human immunodeficiency virus coinfection from active case finding in urban Uganda. Int. J. Tuberc. Lung Dis. 2014, 18, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Reporter, R.M. The Deluxe “Muzigo”—Single Bedroom House; Real Muloodi News Network: Kampala, Uganda, 2021. [Google Scholar]
- Kroon, E.E.; Kinnear, C.J.; Orlova, M.; Fischinger, S.; Shin, S.; Boolay, S.; Walzl, G.; Jacobs, A.; Wilkinson, R.J.; Alter, G.; et al. An observational study identifying highly tuberculosis-exposed, HIV-1-positive but persistently TB, tuberculin and IGRA negative persons with M. tuberculosis specific antibodies in Cape Town, South Africa. EBioMedicine 2020, 61, 103053. [Google Scholar] [CrossRef] [PubMed]
- Hanifa, Y.; Grant, A.D.; Lewis, J.; Corbett, E.L.; Fielding, K.; Churchyard, G. Prevalence of latent tuberculosis infection among gold miners in South Africa. Int. J. Tuberc. Lung Dis. 2009, 13, 39–46. [Google Scholar]
- Chihota, V.N.; Ntshiqa, T.; Maenetje, P.; Mansukhani, R.; Velen, K.; Hawn, T.R.; Wallis, R.; Grant, A.D.; Churchyard, G.J.; Fielding, K. Resistance to Mycobacterium tuberculosis infection among highly TB exposed South African gold miners. PLoS ONE 2022, 17, e0265036. [Google Scholar] [CrossRef]
- Davies, L.R.L.; Smith, M.T.; Cizmeci, D.; Fischinger, S.; Lee, J.S.-L.; Lu, L.L.; Layton, E.D.; Grant, A.D.; Fielding, K.; Stein, C.M.; et al. IFN-gamma independent markers of Mycobacterium tuberculosis exposure among male South African gold miners. EBioMedicine 2023, 93, 104678. [Google Scholar] [CrossRef]
- Baliashvili, D.; Gandhi, N.R.; Kim, S.; Hughes, M.; Mave, V.; Mendoza-Ticona, A.; Gonzales, P.; Narunsky, K.; Selvamuthu, P.; Badal-Faesen, S.; et al. Resistance to Mycobacterium tuberculosis Infection Among Household Contacts: A Multinational Study. Clin. Infect. Dis. 2021, 73, 1037–1045. [Google Scholar] [CrossRef] [PubMed]
- Menzies, D. Interpretation of repeated tuberculin tests. Boosting, conversion, and reversion. Am. J. Respir. Crit. Care Med. 1999, 159, 15–21. [Google Scholar] [CrossRef]
- Lu, L.L.; Smith, M.T.; Yu, K.K.Q.; Luedemann, C.; Suscovich, T.J.; Grace, P.S.; Cain, A.; Yu, W.H.; McKitrick, T.R.; Lauffenburger, D.; et al. IFN-gamma-independent immune markers of Mycobacterium tuberculosis exposure. Nat. Med. 2019, 25, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Mandalakas, A.M.; Kirchner, H.L.; Lombard, C.; Walzl, G.; Grewal, H.M.; Gie, R.P.; Hesseling, A.C. Well-quantified tuberculosis exposure is a reliable surrogate measure of tuberculosis infection. Int. J. Tuberc. Lung Dis. 2012, 16, 1033–1039. [Google Scholar] [CrossRef] [PubMed]
- Ma, N.; Zalwango, S.; Malone, L.L.; Nsereko, M.; Wampande, E.M.; Thiel, B.A.; Okware, B.; Igo, R.P., Jr.; Joloba, M.L.; Mupere, E.; et al. Clinical and epidemiological characteristics of individuals resistant to M. tuberculosis infection in a longitudinal TB household contact study in Kampala, Uganda. BMC Infect. Dis. 2014, 14, 352. [Google Scholar] [CrossRef] [PubMed]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2010. [Google Scholar]
- Ribeiro-Rodrigues, R.; Kim, S.; da Silva, F.D.C.; Uzelac, A.; Collins, L.; Palaci, M.; Alland, D.; Dietze, R.; Ellner, J.J.; Jones-Lopez, E.; et al. Discordance of tuberculin skin test and interferon gamma release assay in recently exposed household contacts of pulmonary TB cases in Brazil. PLoS ONE 2014, 9, e96564. [Google Scholar] [CrossRef] [PubMed]
- Farhat, M.; Greenaway, C.; Pai, M.; Menzies, D. False-positive tuberculin skin tests: What is the absolute effect of BCG and non-tuberculous mycobacteria? Int. J. Tuberc. Lung Dis. 2006, 10, 1192–1204. [Google Scholar] [PubMed]
- Hemmati, M.; Ghadiri, K.; Rezaei, M. Tuberculin Reactivity in School Age Children; Five-year Follow-up in Iran. Iran J. Pediatr. 2011, 21, 39–44. [Google Scholar]
- Pong, A.L.; Anders, B.J.; Moser, K.S.; Starkey, M.; Gassmann, A.; Besser, R.E. Tuberculosis screening at 2 San Diego high schools with high-risk populations. Arch. Pediatr. Adolesc. Med. 1998, 152, 646–650. [Google Scholar] [CrossRef] [PubMed]
- Martinez, L.; Arman, A.; Haveman, N.; Lundgren, A.; Cabrera, L.; Evans, C.A.; Pelly, T.F.; Saito, M.; Callacondo, D.; Oberhelman, R.; et al. Changes in tuberculin skin test positivity over 20 years in periurban shantytowns in Lima, Peru. Am. J. Trop. Med. Hyg. 2013, 89, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Saito, M.; Bautista, C.T.; Gilman, R.H.; Bowering, A.; Levy, M.Z.; Evans, C.A. The value of counting BCG scars for interpretation of tuberculin skin tests in a tuberculosis hyperendemic shantytown, Peru. Int. J. Tuberc. Lung Dis. 2004, 8, 842–847. [Google Scholar]
- Mori, T.; Leung, C.C. Tuberculosis in the global aging population. Infect. Dis. Clin. N. Am. 2010, 24, 751–768. [Google Scholar] [CrossRef]
- Chan-Yeung, M.; Dai, D.L.; Cheung, A.H.; Chan, F.H.; Kam, K.M.; Tam, C.M.; Leung, C.C. Tuberculin skin test reaction and body mass index in old age home residents in Hong Kong. J. Am. Geriatr. Soc. 2007, 55, 1592–1597. [Google Scholar] [CrossRef] [PubMed]
- Lienhardt, C.; Fielding, K.; Hane, A.A.; Niang, A.; Ndao, C.T.; Karam, F.; Fletcher, H.; Mbow, F.; Gomis, J.F.; Diadhiou, R.; et al. Evaluation of the prognostic value of IFN-gamma release assay and tuberculin skin test in household contacts of infectious tuberculosis cases in Senegal. PLoS ONE 2010, 5, e10508. [Google Scholar] [CrossRef]
- Mahomed, H.; Hawkridge, T.; Verver, S.; Abrahams, D.; Geiter, L.; Hatherill, M.; Ehrlich, R.; Hanekom, W.A.; Hussey, G.D. The tuberculin skin test versus QuantiFERON TB Gold(R) in predicting tuberculosis disease in an adolescent cohort study in South Africa. PLoS ONE 2011, 6, e17984. [Google Scholar] [CrossRef]
- Bakir, M.; Millington, K.A.; Soysal, A.; Deeks, J.J.; Efee, S.; Aslan, Y.; Dosanjh, D.P.; Lalvani, A. Prognostic value of a T-cell-based, interferon-gamma biomarker in children with tuberculosis contact. Ann. Intern. Med. 2008, 149, 777–787. [Google Scholar] [CrossRef] [PubMed]
- Harstad, I.; Winje, B.A.; Heldal, E.; Oftung, F.; Jacobsen, G.W. Predictive values of QuantiFERON-TB Gold testing in screening for tuberculosis disease in asylum seekers. Int. J. Tuberc. Lung Dis. 2010, 14, 1209–1211. [Google Scholar] [PubMed]
- Kik, S.V.; Franken, W.P.; Mensen, M.; Cobelens, F.G.; Kamphorst, M.; Arend, S.M.; Erkens, C.; Gebhard, A.; Borgdorff, M.W.; Verver, S. Predictive value for progression to tuberculosis by IGRA and TST in immigrant contacts. Eur. Respir. J. 2010, 35, 1346–1353. [Google Scholar] [CrossRef]
- Diel, R.; Loddenkemper, R.; Niemann, S.; Meywald-Walter, K.; Nienhaus, A. Negative and positive predictive value of a whole-blood interferon-gamma release assay for developing active tuberculosis: An update. Am. J. Respir. Crit. Care Med. 2011, 183, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Leung, C.C.; Yam, W.C.; Yew, W.W.; Ho, P.L.; Tam, C.M.; Law, W.S.; Au, K.F.; Tsui, P.W. T-Spot.TB outperforms tuberculin skin test in predicting tuberculosis disease. Am. J. Respir. Crit. Care Med. 2010, 182, 834–840. [Google Scholar] [CrossRef]
- World Health Organization. Rapid Communication: TB Antigen-Based Skin Tests for the Diagnosis of TB Infection; World Health Organization: Geneva, Switzerland, 2022.
- Aggerbeck, H.; Ruhwald, M.; Hoff, S.T.; Borregaard, B.; Hellstrom, E.; Malahleha, M.; Siebert, M.; Gani, M.; Seopela, V.; Diacon, A.; et al. C-Tb skin test to diagnose Mycobacterium tuberculosis infection in children and HIV-infected adults: A phase 3 trial. PLoS ONE 2018, 13, e0204554. [Google Scholar] [CrossRef]
- Starshinova, A.; Dovgalyk, I.; Malkova, A.; Zinchenko, Y.; Pavlova, M.; Belyaeva, E.; Basantsova, N.; Nazarenko, M.; Kudlay, D.; Yablonskiy, P. Recombinant tuberculosis allergen (Diaskintest((R))) in tuberculosis diagnostic in Russia (meta-analysis). Int. J. Mycobacteriol. 2020, 9, 335–346. [Google Scholar] [CrossRef]
- Lu, P.; Wu, K.; Zhou, H.; Yu, H.; Yuan, J.; Dong, L.; Liu, Q.; Ding, X.; Lu, W.; Yang, H.; et al. Evaluation of ESAT6-CFP10 Skin Test for Mycobacterium tuberculosis Infection among Persons Living with HIV in China. J. Clin. Microbiol. 2023, 61, e0181622. [Google Scholar] [CrossRef] [PubMed]
- Hamada, Y.; Kontsevaya, I.; Surkova, E.; Wang, T.T.; Wan-Hsin, L.; Matveev, A.; Ziganshina, L.E.; Denkinger, C.M.; Korobitsyn, A.; Ismail, N.; et al. A Systematic Review on the Safety of Mycobacterium tuberculosis-Specific Antigen-Based Skin Tests for Tuberculosis Infection Compared With Tuberculin Skin Tests. Open Forum Infect. Dis. 2023, 10, ofad228. [Google Scholar] [CrossRef] [PubMed]



| QFT-Based Classification | |||||
| TST-based Classification | N (%) | Converter | LTBI | “Resister” | Total |
| Converter | 24 (64.9%) a | 27 (15.0%) b | 12 (12.4%) b | 63 (20.1%) | |
| LTBI | 11 (29.7%) c | 149 (82.8%) d | 13 (13.4%) e | 173 (55.1%) | |
| “Resister” | 2 (5.4%) c | 4 (2.2%) e | 72 (74.2%) f | 78 (24.8%) | |
| Total | 37 (100%) | 180 (100%) | 97 (100%) | 314 (100%) | |
| QFT-Only Converters | TST-Only Converters | QFT/TST Converters | “Resisters” | p-Value (Test) | Relevant Pairwise p-Value | |
|---|---|---|---|---|---|---|
| N | 13 | 39 | 24 | 72 | NA | NA |
| Individual Characteristics | ||||||
| Age | 26 [20–36] | 32 [20–47] | 26.5 [23–39.3] | 23 [19.8–36.5] | 0.04 * (KW test) | TST-only vs. “Resister”: 0.006 *¶ |
| Sex (female) | 8 (61.5%) | 21 (53.8%) | 19 (79.2%) | 43 (59.7%) | 0.23 (Fisher’s) | NA |
| BCG scar present | 12 (92.3%) | 31 (81.6%) | 14 (58.3%) | 53 (75.7%) | 0.08 (Fisher’s) | NA |
| HIV positive | 0 (0%) | 3 (7.7%) | 3 (12.5%) | 4 (5.6%) | 0.57 (Fisher’s) | NA |
| BMI | 22.2 [19.6–28.3] | 23.6 [19.5–27.0] | 22.5 [20.5–28.1] | 22.8 [21.0–25.2] | 0.93 (KW test) | NA |
| TB Risk score | 7 [6–8] | 6 [6–7] | 7 [6–7] | 6 [6–7] | 0.15 (KW test) | NA |
| Quantitative IGRA values at conversion | 2.0 [0.9–3.8] | 3.4 [0.3–9.3] | 4.1 [1.7–10] | NA | 0.15 (KW test) | NA |
| No history of smoking | 12 (92.3%) | 37 (94.9%) | 23 (95.8%) | 61 (84.7%) | 0.09 (Fisher’s) | NA |
| Spouse to Index | 4 (30.8%) | 7 (17.9%) | 5 (20.8%) | 8 (11.1%) | 0.26 (Χ2) | NA |
| Household Characteristics | ||||||
| Living in Muzigo | 9 (69.2%) | 20 (51.3%) | 9 (37.5%) | 21 (29.2%) | 0.02 * (Fisher’s) | QFT-only vs. “Resister”: 0.01 * TST-only vs. “Resister”: 0.04 * |
| Cooking inside home | 1 (7.7%) | 10 (25.6%) | 11(45.8%) | 28 (38.9%) | 0.05 * (Fisher’s) | QFT-only vs. QFT/TST: 0.03 * QFT-only vs. “Resister”: 0.03 * |
| Number of windows | 1 [0–2] | 1 [1–3] | 2.5 [1–6] | 3 [1–4] | 0.007 *# (KW test) | QFT-only vs. QFT/TST: 0.003 *# QFT-only vs. “Resister”: 0.003 *# |
| People per room | 2.5 [2–3] | 2 [1.33–3] | 1.67 [1–2.25] | 2 [1.3–2.67] | 0.08 (KW test) | NA |
| Sleeping in same room | 11 (84.6%) | 21 (53.8%) | 15 (62.5%) | 33 (45.8%) | 0.053 (Χ2) | NA |
| Sleeping in same bed | 5 (38.5%) | 6 (15.4%) | 6 (25%) | 12 (16.7%) | 0.23 (Χ2) | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutierrez, J.; Nsereko, M.; Malone, L.L.; Mayanja-Kizza, H.; Kisingo, H.; Boom, W.H.; Bark, C.M.; Stein, C.M. Capturing Recent Mycobacterium tuberculosis Infection by Tuberculin Skin Test vs. Interferon-Gamma Release Assay. Trop. Med. Infect. Dis. 2024, 9, 81. https://doi.org/10.3390/tropicalmed9040081
Gutierrez J, Nsereko M, Malone LL, Mayanja-Kizza H, Kisingo H, Boom WH, Bark CM, Stein CM. Capturing Recent Mycobacterium tuberculosis Infection by Tuberculin Skin Test vs. Interferon-Gamma Release Assay. Tropical Medicine and Infectious Disease. 2024; 9(4):81. https://doi.org/10.3390/tropicalmed9040081
Chicago/Turabian StyleGutierrez, Jesús, Mary Nsereko, LaShaunda L. Malone, Harriet Mayanja-Kizza, Hussein Kisingo, W. Henry Boom, Charles M. Bark, and Catherine M. Stein. 2024. "Capturing Recent Mycobacterium tuberculosis Infection by Tuberculin Skin Test vs. Interferon-Gamma Release Assay" Tropical Medicine and Infectious Disease 9, no. 4: 81. https://doi.org/10.3390/tropicalmed9040081
APA StyleGutierrez, J., Nsereko, M., Malone, L. L., Mayanja-Kizza, H., Kisingo, H., Boom, W. H., Bark, C. M., & Stein, C. M. (2024). Capturing Recent Mycobacterium tuberculosis Infection by Tuberculin Skin Test vs. Interferon-Gamma Release Assay. Tropical Medicine and Infectious Disease, 9(4), 81. https://doi.org/10.3390/tropicalmed9040081