
Global, Regional and National Burden of Human Cystic Echinococcosis from 1990 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019




Abstract
:1. Background
2. Methods
2.1. Data Source
2.2. Statistical Analysis
3. Results
3.1. Global Trends in the Disease Burden of Cystic Echinococcosis
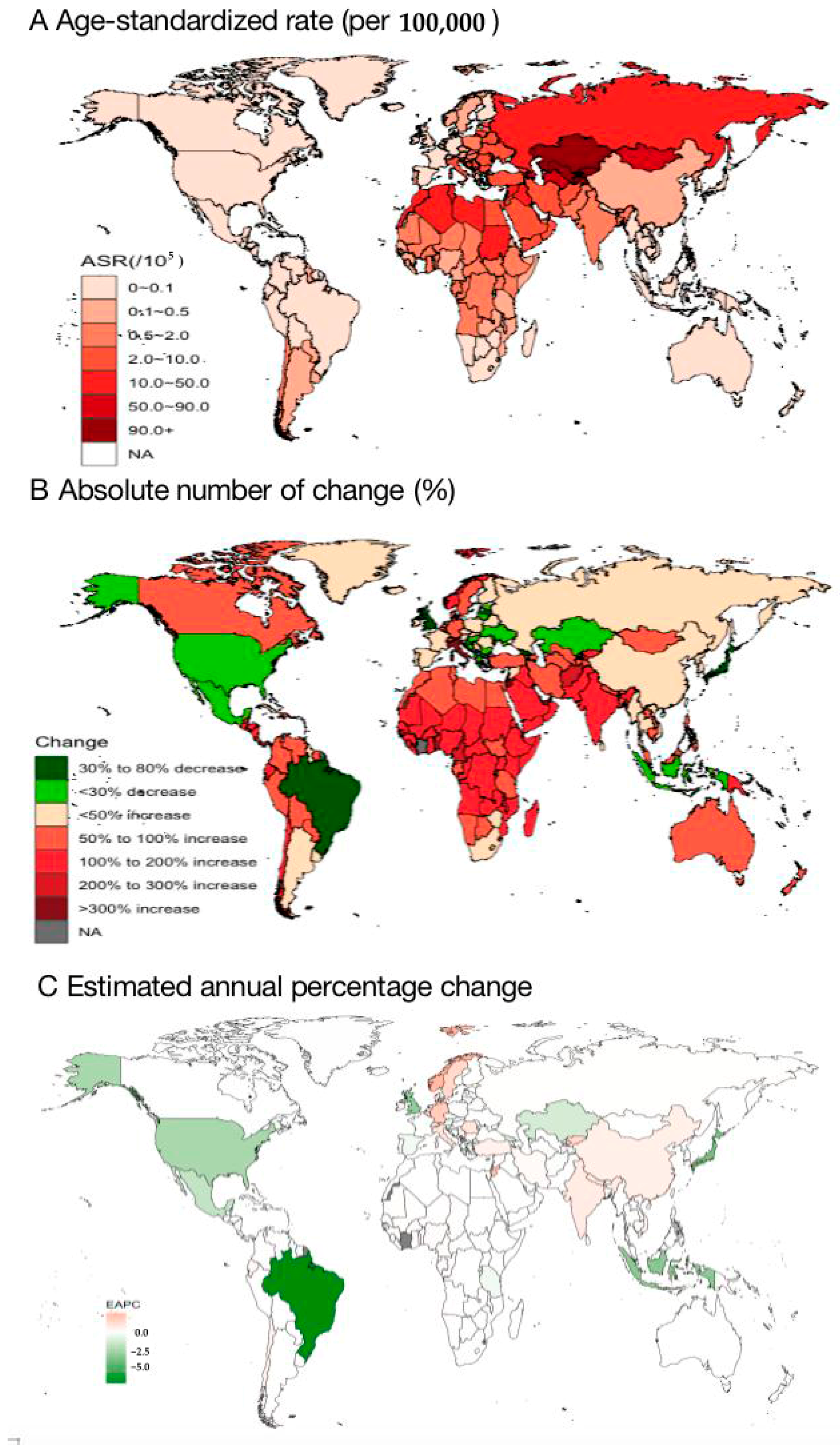
3.2. Country-Specific ASIRs of Cystic Echinococcosis
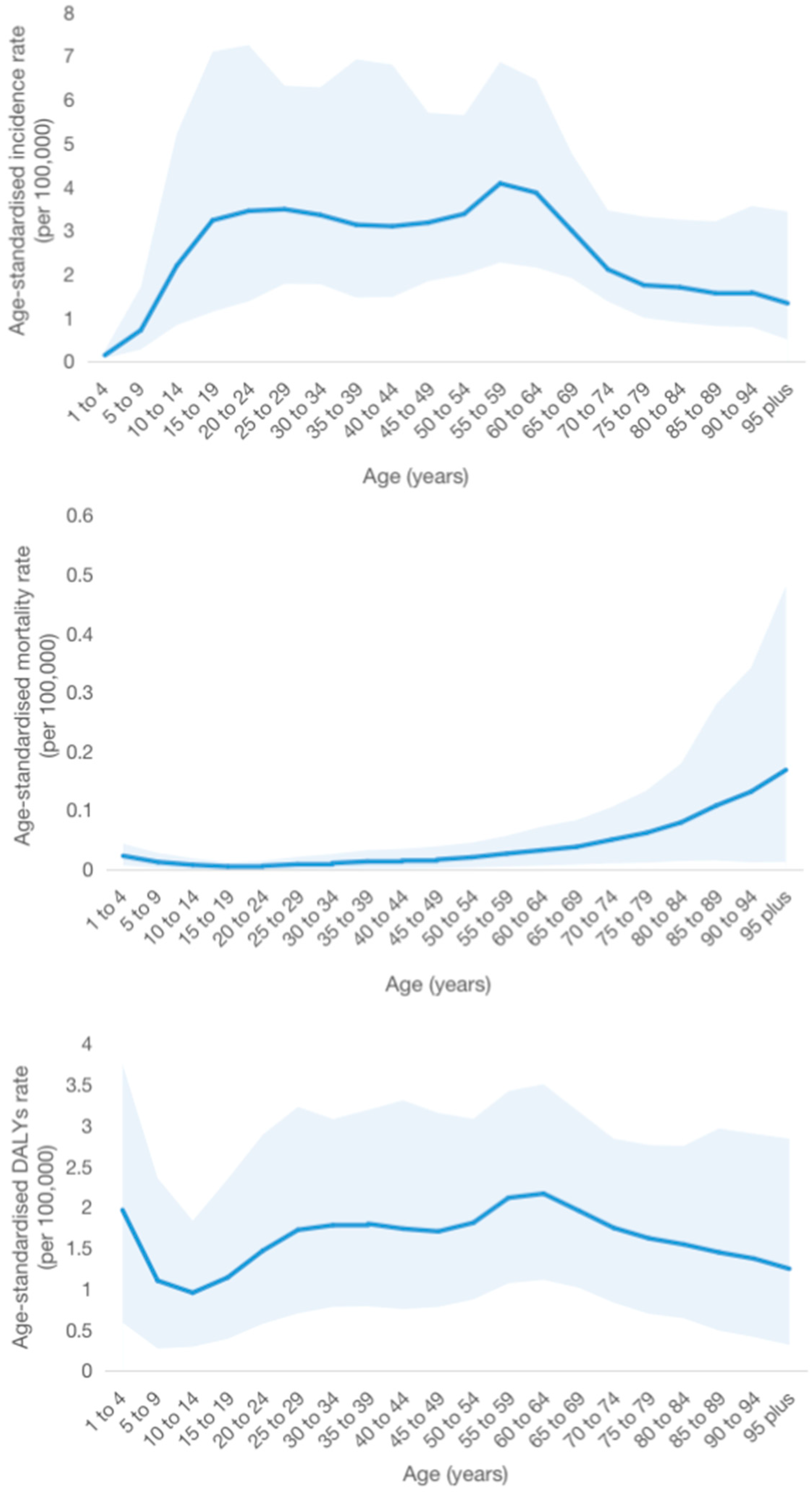
3.3. Age-Specific Burdens of Cystic Echinococcosis
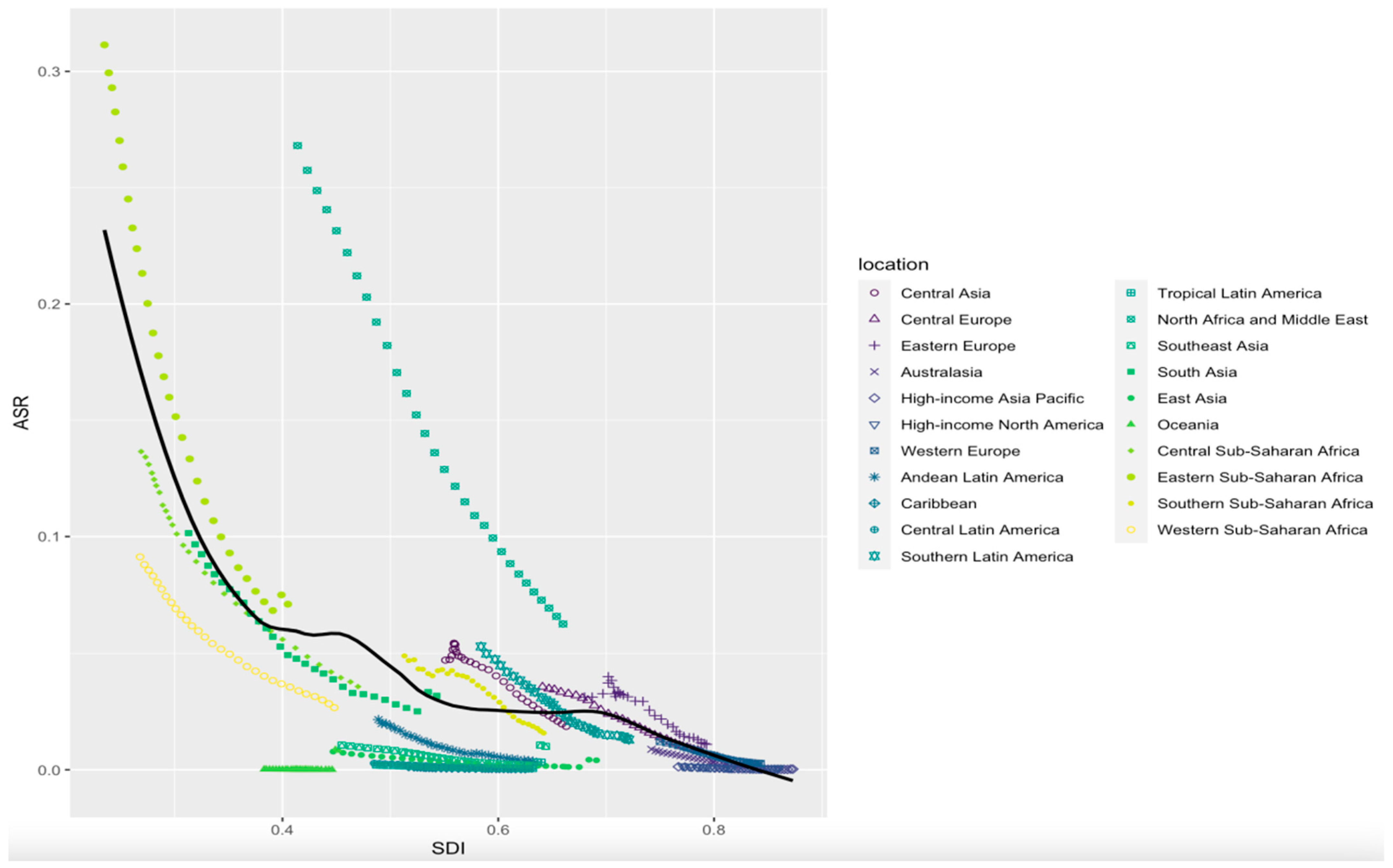
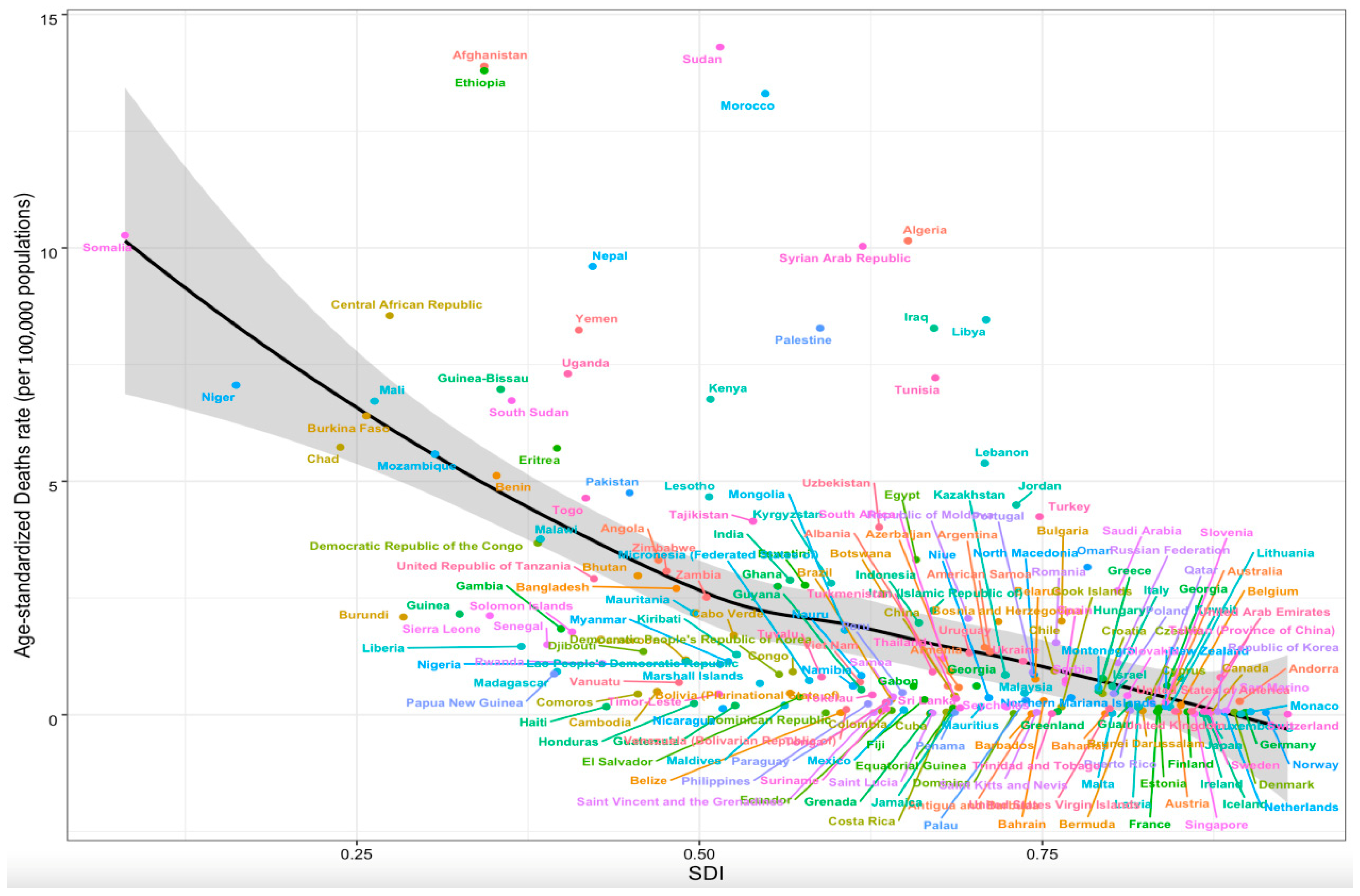
3.4. Association between Age-Specific Burdens of Cystic Echinococcosis and SDI
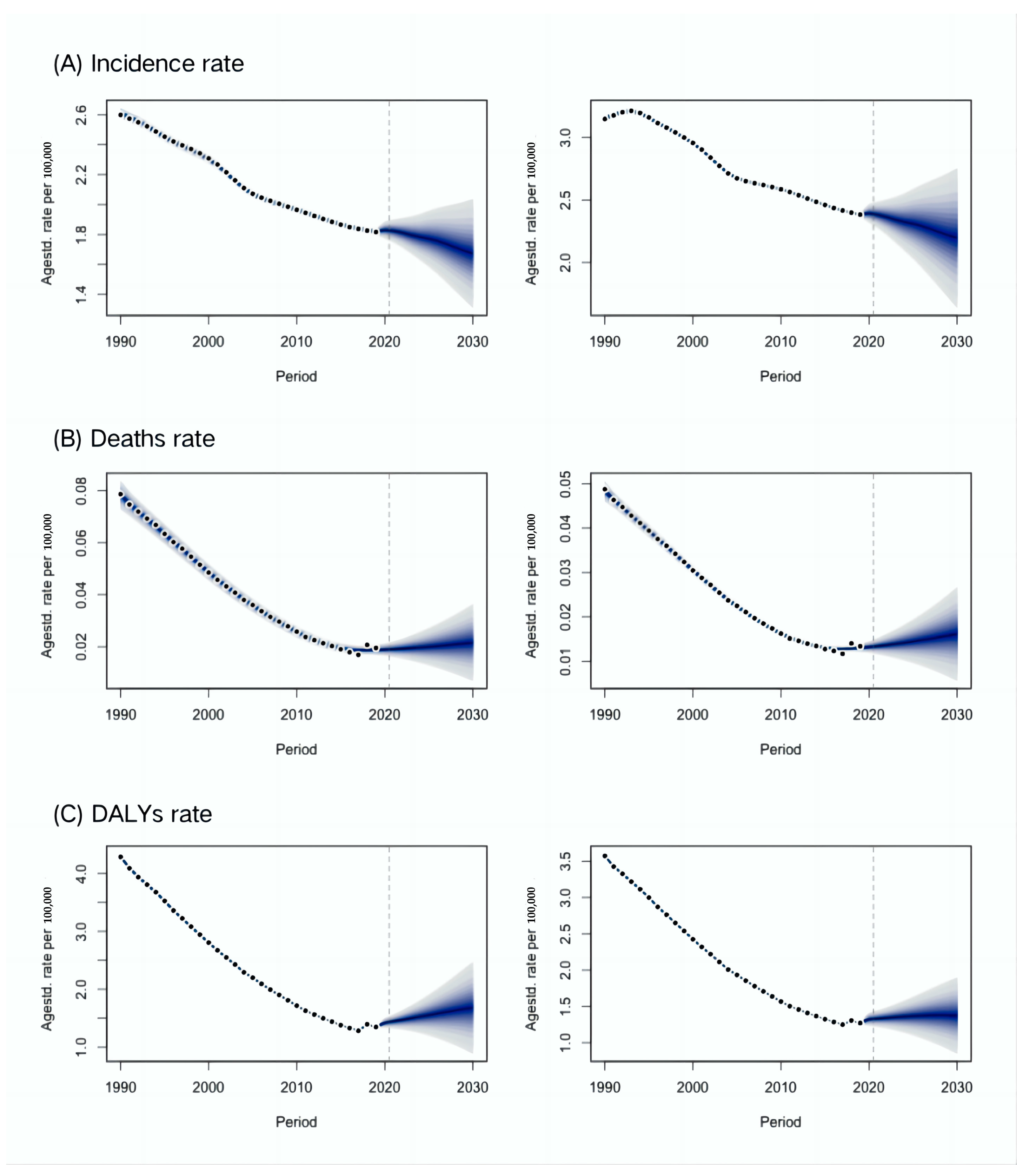
3.5. Projections of the Global Burden Due to Cystic Echinococcosis from 2020 to 2030
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Restrepo, A.M.C.; Yang, Y.R.; McManus, D.P.; Gray, D.J.; Giraudoux, P.; Barnes, T.S.; Williams, G.M.; Soares Magalhães, R.J.; Hamm, N.A.; Clements, A.C. The landscape epidemiology of echinococcoses. Infect. Dis. Poverty 2016, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Wen, H.; Vuitton, L.; Tuxun, T.; Li, J.; Vuitton, D.A.; Zhang, W.; McManus, D.P. Echinococcosis: Advances in the 21st Century. Clin. Microbiol. Rev. 2019, 32, e00075-18. [Google Scholar] [CrossRef] [PubMed]
- Lymbery, A.J. Phylogenetic pattern, evolutionary processes and species eelimitation in the genus Echinococcus. Adv. Parasitol. 2017, 95, 111–145. [Google Scholar] [PubMed]
- Islami Parkoohi, P.; Jahani, M.; Hosseinzadeh, F.; Taghian, S.; Rostami, F.; Mousavi, A.; Rezai, M.S. Epidemiology and clinical features of hydatid cyst in northern Iran from 2005 to 2015. Iran. J. Parasitol. 2018, 13, 310–316. [Google Scholar] [PubMed]
- Stojković, M.; Weber, T.F.; Junghanss, T. Clinical management of cystic echinococcosis: State of the art and perspectives. Curr. Opin. Infect. Dis. 2018, 31, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Deplazes, P.; Rinaldi, L.; Alvarez Rojas, C.A.; Torgerson, P.R.; Harandi, M.F.; Romig, T.; Antolova, D.; Schurer, J.M.; Lahmar, S.; Cringoli, G.; et al. Global distribution of alveolar and cystic echinococcosis. Adv. Parasitol. 2017, 95, 315–493. [Google Scholar] [PubMed]
- Noguera, Z.L.P.; Charypkhan, D.; Hartnack, S.; Torgerson, P.R.; Rüegg, S.R. The dual burden of animal and human zoonoses: A systematic review. PLoS Negl. Trop. Dis. 2022, 16, e0010540. [Google Scholar] [CrossRef]
- Budke, C.M.; Deplazes, P.; Torgerson, P.R. Global socioeconomic impact of cystic echinococcosis. Emerg. Infect. Dis. 2006, 12, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.S.; Hegglin, D.; Lightowlers, M.W.; Torgerson, P.R.; Wang, Q. Echinococcosis: Control and prevention. Adv. Parasitol. 2017, 96, 55–158. [Google Scholar]
- Velasco-Tirado, V.; Romero-Alegria, A.; Pardo-Lledías, J.; Alonso-Sardón, M.; Lopez-Bernus, A.; Sampedro, J.Q.; Bellvis, L.M.; Iglesias Gomez, A.; Muro, A.; Muñoz Bellido, J.L.; et al. Management of cystic echinococcosis in the last two decades: What have we learned? Trans. R. Soc. Trop. Med. Hyg. 2018, 112, 207–215. [Google Scholar] [CrossRef]
- Casulli, A. New global targets for NTDs in the WHO roadmap 2021-2030. PLoS Negl. Trop. Dis. 2021, 15, e0009373. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Zhan, J.; Chen, L.; Chen, H.; Cheng, S. Global, regional, and national dengue burden from 1990 to 2017: A systematic analysis based on the global burden of disease study 2017. eClinicalMedicine 2021, 32, 100712. [Google Scholar] [CrossRef]
- GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef] [PubMed]
- Riebler, A.; Held, L. Projecting the future burden of cancer: Bayesian age-period-cohort analysis with integrated nested Laplace approximations. Biom. J. 2017, 59, 531–549. [Google Scholar] [CrossRef]
- Pavletic, C.F.; Larrieu, E.; Guarnera, E.A.; Casas, N.; Irabedra, P.; Ferreira, C.; Sayes, J.; Gavidia, C.M.; Caldas, E.; Lise, M.L.Z.; et al. Cystic echinococcosis in South America: A call for action. Rev. Panam. De Salud Publica 2017, 41, e42. [Google Scholar]
- Li, K.; Shahzad, M. Epidemiology of cystic echinococcosis in China (2004–2016). Travel Med. Infect. Dis. 2020, 33, 101466. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, J.; Wang, X.; Ahmed, H.; Shen, Y.J.; Cao, J.P. Molecular epidemiology and the control and prevention of cystic echinococcosis in China: What is known from current research. Zoonoses 2023, 3, 24. [Google Scholar] [CrossRef]
- Casulli, A.; Abela-Ridder, B.; Petrone, D.; Fabiani, M.; Bobić, B.; Carmena, D.; Šoba, B.; Zerem, E.; Gargaté, M.J.; Kuzmanovska, G.; et al. Unveiling the incidences and trends of the neglected zoonosis cystic echinococcosis in Europe: A systematic review from the MEmE project. Lancet Infect. Dis. 2023, 23, e95–e107. [Google Scholar] [CrossRef]
- Karlas, T.; Reinhardt, F.; Blank, V.; Lippmann, N.; Seehofer, D.; Lübbert, C. Frequency and clinical presentation of alveolar and cystic echinococcosis in a tertiary medical center in Germany 2004–2018: Lessons from a low-prevalence area. Z. Gastroenterol. 2019, 57, 1281–1290. [Google Scholar] [CrossRef]
- Torgerson, P.R.; Budke, C.M. Echinococcosis—An international public health challenge. Res. Vet. Sci. 2003, 74, 191–202. [Google Scholar] [CrossRef]
- WHO. Accelerating Work to Overcome the Global Impact of Neglected Tropical Diseases—A Roadmap for Implementation. Available online: https://www.who.int/publications/i/item/WHO-HTM-NTD-2012.1 (accessed on 1 March 2023).
- WHO. Ending the Neglect to Attain the Sustainable Development Goals: A Road Map for Neglected Tropical Diseases 2021–2030. Available online: https://www.who.int/publications/i/item/9789240010352 (accessed on 1 March 2023).
- WHO. London Declaration on Neglected Tropical Diseases. Available online: https://unitingtocombatntds.org/resource-hub/who-resources/london-declaration-neglected-tropical-diseases/ (accessed on 1 March 2023).
- Brunetti, E.; Kern, P.; Vuitton, D.A.; Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010, 114, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Larrieu, E.; Uchiumi, L.; Salvitti, J.C.; Sobrino, M.; Panomarenko, O.; Tissot, H.; Mercapide, C.H.; Sustercic, J.; Arezo, M.; Mujica, G.; et al. Epidemiology, diagnosis, treatment and follow-up of cystic echinococcosis in asymptomatic carriers. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.C.; Negron, M.E.; Pieracci, E.G.; Deressa, A.; Bekele, W.; Regassa, F.; Wassie, B.A.; Afera, B.; Hajito, K.W.; Walelign, E.; et al. One Health collaborations for zoonotic disease control in Ethiopia. Rev. Sci. Tech. 2019, 38, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimipour, M.; Budke, C.M.; Harandi, M.F. Control of cystic echinococcosis in Iran: Where do we stand? Trends Parasitol. 2020, 36, 578–581. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Huang, Y.; Huang, L.; Yu, W.; He, W.; Zhong, B.; Li, W.; Zeng, X.; Vuitton, D.A.; Giraudoux, P.; et al. Review of risk factors for human echinococcosis prevalence on the Qinghai-Tibet Plateau, China: A prospective for control options. Infect. Dis. Poverty 2014, 3, 3. [Google Scholar] [CrossRef]
- Possenti, A.; Manzano-Román, R.; Sánchez-Ovejero, C.; Boufana, B.; La Torre, G.; Siles-Lucas, M.; Casulli, A. Potential risk factors associated with human cystic echinococcosis: Systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2016, 10, e0005114. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Quzhen, G.; Xue, C.Z.; Han, S.; Chen, W.Q.; Yan, X.L.; Li, Z.J.; Quick, M.L.; Huang, Y.; Xiao, N.; et al. Epidemiological survey of echinococcosis in Tibet Autonomous Region of China. Infect. Dis. Poverty 2019, 8, 29. [Google Scholar] [CrossRef]
- Abdelbaset, A.E.; Yagi, K.; Nonaka, N.; Nakao, R. Cystic echinococcosis in humans and animals in Egypt: An epidemiological overview. Curr. Res. Parasitol. Vector Borne Dis. 2021, 1, 100061. [Google Scholar] [CrossRef] [PubMed]
- Paternoster, G.; Boo, G.; Wang, C.; Minbaeva, G.; Usubalieva, J.; Raimkulov, K.M.; Zhoroev, A.; Abdykerimov, K.K.; Kronenberg, P.A.; Müllhaupt, B.; et al. Epidemic cystic and alveolar echinococcosis in Kyrgyzstan: An analysis of national surveillance data. Lancet Glob. Health 2020, 8, e603–e611. [Google Scholar] [CrossRef]
- Mastrandrea, S.; Stegel, G.; Piseddu, T.; Ledda, S.; Masala, G. A retrospective study on burden of human echinococcosis based on Hospital Discharge Records from 2001 to 2009 in Sardinia, Italy. Acta Trop. 2012, 123, 184–189. [Google Scholar] [CrossRef]
- Khan, A.; Naz, K.; Ahmed, H.; Simsek, S.; Afzal, M.S.; Haider, W.; Ahmad, S.S.; Farrakh, S.; Weiping, W.; Yayi, G. Knowledge, attitudes and practices related to cystic echinococcosis endemicity in Pakistan. Infect. Dis. Poverty 2018, 7, 4. [Google Scholar] [CrossRef] [PubMed]
- Qucuo, N.; Wu, G.; He, R.; Quzhen, D.; Zhuoga, C.; Deji, S.; Zhang, L.; Zhao, Z.; Du, Z. Knowledge, attitudes and practices regarding echinococcosis in Xizang Autonomous Region, China. BMC Public Health 2020, 20, 483. [Google Scholar] [CrossRef] [PubMed]
- Lutz, W.; Sanderson, W.; Scherbov, S. The coming acceleration of global population ageing. Nature 2008, 451, 716–719. [Google Scholar] [CrossRef] [PubMed]
- Larrieu, E.; Gavidia, C.M.; Lightowlers, M.W. Control of cystic echinococcosis: Background and prospects. Zoonoses Public Health 2019, 66, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Widdicombe, J.; Basáñez, M.G.; Entezami, M.; Jackson, D.; Larrieu, E.; Prada, J.M. The economic evaluation of cystic echinococcosis control strategies focused on zoonotic hosts: A scoping review. PLoS Negl. Trop. Dis. 2022, 16, e0010568. [Google Scholar] [CrossRef] [PubMed]
- Parandin, F.; Heydarpour, F.; Mohebali, M.; Hanafi-Bojd, A.A.; Sari, A.A.; Zeynali, M.; Alizadeh, A.; Nazari, N.; Kaveh, F.; Rokni, M.B. Estimation of Burden of Cystic Echinococcosis in Iran Using Disability Adjusted Life Years (DALYs) in 2018. Iran. J. Public Health 2021, 50, 2302–2308. [Google Scholar] [CrossRef] [PubMed]
- Doszhanova, G.; Colpani, A.; Duisenova, A.; De Vito, A.; Zholdybay, Z.; Juszkiewicz, K.; Brunetti, E.; Katarbayev, A.; Kaniyev, S.; Zhakenova, Z.; et al. The high burden of pediatric cystic echinococcosis in Kazakhstan: Epidemiological and clinical consequences. Trans. R. Soc. Trop. Med. Hyg. 2023, 117, 875–877. [Google Scholar] [CrossRef] [PubMed]
- Alho, A.M.; Dias, M.C.; Cardo, M.; Aguiar, P.; de Carvalho, L.M. The Evolution of Cystic Echinococcosis in Humans and Ruminants in Portugal-A One Health Approach. Vet. Sci. 2023, 10, 584. [Google Scholar] [CrossRef]
- Khan, A.; Ahmed, H.; Amjad, S.; Afzal, M.S.; Haider, W.; Simsek, S.; Khawaja, M.R.; Khan, D.H.; Naz, S.; Durrance-Bagale, A.; et al. Community Based Assessment of Behavior and Awareness of Risk Factors of Cystic Echinococcosis in Major Cities of Pakistan: A One Health Perspective. Front. Public Health 2021, 9, 648900. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | Incidence | Mortality | DALYs | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number (95% CI) | ASR, per 105 (95% CI) | Number (95% CI) | ASR, per 105 (95% CI) | Number (95% CI) | ASR, per 105 (95% CI) | |||||||
| 1990 | 2019 | 1990 | 2019 | 1990 | 2019 | 1990 | 2019 | 1990 | 2019 | 1990 | 2019 | |
| Global | 134,980 (93,141–195,144) | 207,368 (137,807–303,233) | 2.65 (1.87–3.7) | 2.6 (1.72–3.79) | 2839 (2218–3497) | 1349 (987–1762) | 0.06 (0.04–0.07) | 0.02 (0.01–0.02) | 210,044 (166,434–261,084) | 122,457 (89,244–168,556) | 3.82 (3.05–4.7) | 1.56 (1.14–2.15) |
| Gender | ||||||||||||
| Male | 55,004 (36,334–84,605) | 83,318 (52,851–127,144) | 2.12 (1.43–3.1) | 2.09 (1.34–3.21) | 1480 (1105–1879) | 726 (455–1030) | 0.06 (0.04–0.08) | 0.02 (0.01–0.03) | 103,864 (78,388–133,209) | 58,532 (40,465–81,788) | 3.74 (2.86–4.75) | 1.49 (1.04–2.1) |
| Female | 79,977 (56,335–113,027) | 124,050 (84,455–175,220) | 3.17 (2.28–4.31) | 3.1 (2.1–4.38) | 1359 (995–1776) | 623 (385–879) | 0.05 (0.04–0.07) | 0.02 (0.01–0.02) | 103,864 (78,388–133,209) | 63,925 (43,062–87,764) | 3.9 (2.99–4.94) | 1.62 (1.08–2.25) |
| Socio-demographic index | ||||||||||||
| Low | 5079 (3391–7571) | 12,430 (8169–18,540) | 1.11 (0.78–1.61) | 1.2 (0.83–1.71) | 1019 (739–1378) | 438 (303–592) | 0.2 (0.15–0.26) | 0.05 (0.04–0.07) | 70,767 (50,134–97,271) | 27,923 (18,880–38,026) | 10.91 (8.1–14.56) | 2.58 (1.88–3.36) |
| Low-middle | 21,426 (12,586–34,881) | 41,908 (25,494–64,714) | 2.17 (1.36–3.3) | 2.37 (1.47–3.62) | 1000 (798–1230) | 455 (338–587) | 0.1 (0.08–0.13) | 0.03 (0.02–0.04) | 67,621 (53,616–85,566) | 31,737 (23,685–42,274) | 5.62 (4.58–6.86) | 1.87 (1.41–2.43) |
| Middle | 48,647 (24,709–87,978) | 85,224 (45,368–144,835) | 2.95 (1.58–4.89) | 3.38 (1.8–5.84) | 437 (333–537) | 276 (195–373) | 0.03 (0.02–0.04) | 0.01 (0.01–0.02) | 38,780 (27,433–54,650) | 36,915 (22,015–63,062) | 2.35 (1.73–3.23) | 1.45 (0.86–2.47) |
| High-middle | 58,010 (47,824–69,658) | 64,390 (53,694–76,666) | 4.96 (4.1–5.92) | 4.03 (3.35–4.8) | 348 (244–463) | 161 (112–220) | 0.03 (0.02–0.04) | 0.01 (0.01–0.01) | 30,961 (23,984–39,200) | 24,106 (17,621–32,569) | 2.7 (2.1–3.39) | 1.46 (1.05–1.98) |
| High | 1799 (1083–2828) | 3359 (1985–5352) | 0.21 (0.13–0.35) | 0.34 (0.19–0.54) | 34 (20–51) | 19 (11–28) | 0 (0–0.01) | 0 (0–0) | 1849 (1287–2529) | 1733 (1123–2638) | 0.22 (0.15–0.3) | 0.16 (0.1–0.25) |
| GBD region | ||||||||||||
| High-income Asia Pacific | 93 (35–254) | 51 (33–91) | 0.05 (0.02–0.14) | 0.03 (0.01–0.05) | 2 (1–4) | 1 (1–2) | 0 (0–0) | 0 (0–0) | 127 (79–201) | 42 (27–61) | 0.07 (0.04–0.11) | 0.02 (0.01–0.03) |
| Central Asia | 65,909 (43,716–102,773) | 95102 (56,969–152,588) | 103.28 (68.82–152.04) | 100.32 (61.06–159.16) | 27 (17–38) | 15 (9–21) | 0.05 (0.03–0.07) | 0.02 (0.01–0.03) | 21,147 (12,039–36,064) | 30,110 (15,271–54,362) | 33.74 (19.48–56.19) | 31.68 (16.44–56) |
| East Asia | 5072 (1560–11,800) | 6793 (3000–13,654) | 0.4 (0.13–0.88) | 0.45 (0.18–0.94) | 78 (65–92) | 74 (61–88) | 0.01 (0.01–0.01) | 0 (0–0) | 5541 (4037–8534) | 4395 (2897–7336) | 0.47 (0.35–0.67) | 0.26 (0.17–0.45) |
| South Asia | 7321 (4559–13,128) | 14,984 (9539–28,274) | 0.8 (0.51–1.52) | 0.86 (0.56–1.64) | 930 (727–1162) | 478 (340–630) | 0.1 (0.08–0.13) | 0.03 (0.02–0.04) | 59,185 (46,325–73,797) | 23,798 (17,893–30,900) | 4.99 (3.96–6.16) | 1.39 (1.05–1.8) |
| Southeast Asia | 664 (164–2059) | 574 (163–1533) | 0.14 (0.04–0.38) | 0.08 (0.02–0.23) | 39 (25–54) | 61 (37–89) | 0.01 (0.01–0.01) | 0.01 (0.01–0.01) | 2265 (1534–3264) | 2460 (1557–3556) | 0.5 (0.34–0.7) | 0.37 (0.24–0.52) |
| Australasia | 5 (4–7) | 9 (7–13) | 0.02 (0.02–0.03) | 0.02 (0.02–0.03) | 2 (1–3) | 1 (0–1) | 0.01 (0–0.01) | 0 (0–0) | 60 (35–88) | 23 (15–33) | 0.28 (0.16–0.4) | 0.06 (0.04–0.09) |
| Caribbean | 18 (14–24) | 22 (17–28) | 0.06 (0.04–0.07) | 0.04 (0.04–0.06) | 0 (0–1) | 0 (0–1) | 0 (0–0) | 0 (0–0) | 33 (16–56) | 22 (15–31) | 0.09 (0.05–0.15) | 0.05 (0.03–0.07) |
| Central Europe | 2279 (1879–2734) | 2326 (1988–2686) | 1.74 (1.41–2.1) | 1.76 (1.49–2.06) | 48 (30–69) | 15 (8–24) | 0.04 (0.02–0.05) | 0.01 (0–0.01) | 2313 (1716–2976) | 1166 (847–1534) | 1.74 (1.29–2.23) | 0.81 (0.59–1.08) |
| Eastern Europe | 23,796 (19,659–28,303) | 24,583 (20,301–29,406) | 9.48 (7.9–11.19) | 9.68 (8.14–11.47) | 79 (43–119) | 32 (17–50) | 0.03 (0.02–0.05) | 0.01 (0.01–0.02) | 10,065 (7392–13,113) | 8648 (6168–11,751) | 3.99 (2.94–5.19) | 3.31 (2.36–4.51) |
| Western Europe | 870 (657–1242) | 4635 (3933–5435) | 0.21 (0.16–0.31) | 0.86 (0.73–1.02) | 63 (37–90) | 24 (13–38) | 0.01 (0.01–0.02) | 0 (0–0) | 1997 (1343–2741) | 1764 (1303–2337) | 0.45 (0.3–0.6) | 0.31 (0.22–0.4) |
| Andean Latin America | 7 (5–10) | 13 (10–16) | 0.02 (0.02–0.03) | 0.02 (0.02–0.03) | 7 (4–10) | 2 (1–3) | 0.02 (0.01–0.03) | 0 (0–0.01) | 394 (193–630) | 85 (48–133) | 0.99 (0.55–1.49) | 0.14 (0.08–0.21) |
| Central Latin America | 92 (34–256) | 91 (50–188) | 0.06 (0.02–0.17) | 0.04 (0.02–0.08) | 3 (2–5) | 3 (2–4) | 0 (0–0) | 0 (0–0) | 220 (114–341) | 133 (83–194) | 0.14 (0.08–0.21) | 0.05 (0.03–0.08) |
| Southern Latin America | 336 (279–400) | 569 (483–666) | 0.69 (0.58–0.82) | 0.79 (0.67–0.93) | 24 (16–33) | 10 (6–15) | 0.05 (0.04–0.07) | 0.01 (0.01–0.02) | 949 (669–1236) | 476 (345–619) | 1.97 (1.39–2.57) | 0.65 (0.47–0.84) |
| Tropical Latin America | 816 (265–2027) | 192 (112–346) | 0.63 (0.23–1.74) | 0.08 (0.05–0.15) | 2 (1–3) | 8 (4–12) | 0 (0–0) | 0 (0–0) | 349 (170–748) | 332 (206–469) | 0.27 (0.14–0.64) | 0.14 (0.09–0.2) |
| North Africa and Middle East | 23,763 (14,395–37,029) | 48,205 (29,717–72,394) | 7.61 (4.76–11.23) | 7.81 (4.98–11.44) | 689 (541–854) | 287 (211–374) | 0.27 (0.21–0.33) | 0.06 (0.05–0.08) | 45,756 (35,616–58,030) | 26,631 (18,912–37,908) | 13.58 (10.88–16.64) | 4.53 (3.3–6.27) |
| High-income North America | 130 (74–239) | 118 (75–193) | 0.04 (0.02–0.08) | 0.03 (0.02–0.04) | 5 (3–8) | 4 (2–6) | 0 (0–0) | 0 (0–0) | 202 (129–289) | 154 (99–214) | 0.07 (0.04–0.1) | 0.04 (0.02–0.05) |
| Oceania | 0 (0–1) | 1 (0–1) | 0 (0–0.01) | 0 (0–0.01) | 0 (0–0) | 1 (0–1) | 0 (0–0) | 0.01 (0–0.01) | 0 (0–1) | 42 (22–68) | 0.01 (0.01–0.01) | 0.34 (0.19–0.53) |
| Central Sub-Saharan Africa | 811 (518–1201) | 2030 (1294–3011) | 1.69 (1.18–2.33) | 1.7 (1.18–2.34) | 71 (50–99) | 29 (19–41) | 0.14 (0.09–0.18) | 0.04 (0.02–0.05) | 5105 (3621–7210) | 2047 (1430–2771) | 7.45 (5.35–10.23) | 1.76 (1.28–2.33) |
| Eastern Sub-Saharan Africa | 1477 (1124–1890) | 3260 (2485–4157) | 0.81 (0.64–1.01) | 0.8 (0.63–0.99) | 558 (383–784) | 191 (130–266) | 0.31 (0.22–0.42) | 0.07 (0.05–0.1) | 38,989 (26,530–56,175) | 11,813 (7615–16,493) | 16.61 (11.77–23.09) | 3.04 (2.1–4.1) |
| Southern Sub-Saharan Africa | 20 (15–27) | 29 (22–38) | 0.04 (0.03–0.05) | 0.04 (0.03–0.05) | 20 (11–29) | 10 (6–15) | 0.05 (0.03–0.07) | 0.02 (0.01–0.02) | 1074 (540–1686) | 456 (246–695) | 2.15 (1.2–3.21) | 0.6 (0.34–0.9) |
| Western Sub-Saharan Africa | 1499 (941–2276) | 3781 (2342–5797) | 0.88 (0.59–1.25) | 0.91 (0.61–1.29) | 191 (117–283) | 103 (60–157) | 0.09 (0.06–0.13) | 0.03 (0.02–0.04) | 14,274 (8226–22,125) | 7858 (4459–12,066) | 5.46 (3.48–7.96) | 1.54 (0.99–2.2) |
| Items | Incidence | Mortality | DALYs | |||
|---|---|---|---|---|---|---|
| Annual Rate of Change (%, 95% CI) | EAPC (%, 95% CI) | Annual Rate of Change (%, 95% CI) | EAPC (%, 95% CI) | Annual Rate of Change (%, 95% CI) | EAPC (%, 95% CI) | |
| Global | 0.54 (0.42–0.7) | −0.18 (−0.24–0.12) | −0.52 (−0.66–0.34) | −4.64 (−4.85–4.43) | −0.42 (−0.57–0.23) | −3.38 (−3.5–3.26) |
| Gender | ||||||
| Male | 0.51 (0.39–0.7) | −0.08 (−0.13–0.02) | −0.51 (−0.7–0.24) | −4.54 (−4.75–4.32) | −0.44 (−0.62–0.21) | −3.47 (−3.6–3.35) |
| Female | 0.55 (0.43–0.71) | −0.24 (−0.31–0.18) | −0.54 (−0.73–0.27) | −4.78 (−4.99–4.57) | −0.4 (−0.58–0.15) | −3.3 (−3.43–3.18) |
| Socio-demographic index | ||||||
| Low | 1.39 (1.26–1.51) | 0.24 (0.22–0.26) | −0.57 (−0.71–0.37) | −4.81 (−4.97–4.65) | −0.61 (−0.74–0.41) | −5.18 (−5.31–5.06) |
| Low-middle | 0.94 (0.76–1.16) | 0.38 (0.35–0.42) | −0.54 (−0.67–0.38) | −4.81 (−5.08–4.54) | −0.53 (−0.66–0.37) | −4.16 (−4.37–3.96) |
| Middle | 0.74 (0.49–1.03) | 0.48 (0.44–0.51) | −0.37 (−0.58–0.08) | −4.64 (−5.08–4.2) | −0.05 (−0.32–0.24) | −1.94 (−2.14–1.74) |
| High-middle | 0.11 (0.05–0.17) | −1.04 (−1.19–0.89) | −0.54 (−0.71–0.3) | −5.17 (−5.37–4.96) | −0.22 (−0.35–0.08) | −2.51 (−2.66–2.35) |
| High | 0.87 (0.52–1.36) | 1.67 (1.54–1.81) | −0.45 (−0.71–0.05) | −4.01 (−4.17–3.86) | −0.06 (−0.39–0.38) | −1.14 (−1.34–0.94) |
| GBD region | ||||||
| High-income Asia Pacific | −0.45 (−0.66–0.02) | −2.9 (−3.51–2.28) | −0.52 (−0.78–0.02) | −6.76 (−7.52–6) | −0.67 (−0.79–0.46) | −5.66 (−6.32–5.01) |
| Central Asia | 0.44 (0.28–0.67) | −0.2 (−0.28–0.12) | −0.45 (−0.7–0.01) | −3.61 (−4.11–3.11) | 0.42 (0.22–0.68) | −0.35 (−0.42–0.27) |
| East Asia | 0.34 (−0.05–1.06) | 0.56 (0.49–0.64) | −0.05 (−0.27–0.24) | −5.35 (−6.64–4.05) | −0.21 (−0.38–0.04) | −2.77 (−3.28–2.26) |
| South Asia | 1.05 (0.87–1.25) | 0.32 (0.25–0.39) | −0.49 (−0.64–0.3) | −4.74 (−5.05–4.42) | −0.6 (−0.71–0.46) | −4.92 (−5.18–4.67) |
| Southeast Asia | −0.14 (−0.32–0.21) | −2.35 (−2.77–1.94) | 0.59 (−0.09–1.76) | −4.35 (−5.96–2.72) | 0.09 (−0.37–0.93) | −4.66 (−6.03–3.26) |
| Australasia | 0.76 (0.61–0.89) | 0.01 (−0.06–0.07) | −0.56 (−0.79–0.1) | −5.42 (−5.56–5.29) | −0.62 (−0.79–0.27) | −5.26 (−5.42–5.1) |
| Caribbean | 0.18 (0.06–0.32) | −0.73 (−0.78–0.68) | −0.17 (−0.6–0.82) | −2.98 (−3.59–2.37) | −0.33 (−0.65–0.41) | −2.69 (−3.04–2.35) |
| Central Europe | 0.02 (−0.05–0.1) | 0.09 (−0.02–0.19) | −0.69 (−0.85–0.43) | −5.52 (−5.72–5.33) | −0.5 (−0.64–0.29) | −2.86 (−2.95–2.77) |
| Eastern Europe | 0.03 (−0.02–0.08) | 0.09 (0.08–0.09) | −0.6 (−0.81–0.2) | −4.39 (−5.01–3.76) | −0.14 (−0.27–0.01) | −0.92 (−1.07–0.77) |
| Western Europe | 4.33 (3.04–5.61) | 0.45 (−0.87–1.79) | −0.62 (−0.81–0.25) | −5.2% (−5.31–5.15) | −0.12 (−0.42–0.43) | −2.49 (−2.85–2.13) |
| Andean Latin America | 0.78 (0.6–0.99) | −0.12 (−0.13–0.12) | −0.68 (−0.84–0.37) | −5.98 (−6.1–5.85) | −0.78 (−0.9–0.51) | −6.71 (−6.82–6.6) |
| Central Latin America | −0.02 (−0.33–0.62) | −1.28 (−1.8–0.75) | −0.21 (−0.6–0.54) | −4.16 (−4.67–3.65) | −0.39 (−0.66–0.2) | −3.97% (−4.43–3.51) |
| Southern Latin America | 0.69 (0.61–0.78) | 0.3 (−0.02–0.63) | −0.58 (−0.76–0.31) | −4.77 (−4.84–4.7) | −0.5 (−0.66–0.23) | −3.75% (−3.79–3.7) |
| Tropical Latin America | −0.77 (−0.85–0.56) | −6.29 (−6.7–5.87) | 2.65 (0.82–6.16) | −2.7 (−4.52–0.84) | −0.05 (−0.55–1.14) | −4.5% (−5.7–3.29) |
| North Africa and Middle East | 1.03 (0.81–1.29) | 0.03 (−0.01–0.08) | −0.58 (−0.7–0.43) | −5.09 (−5.17–5.01) | −0.42 (−0.59–0.2) | −3.91% (−4–3.83) |
| High-income North America | −0.09 (−0.3–0.17) | −1.95 (−2.38–1.53) | −0.19 (−0.6–0.64) | −3.54 (−4.06–3.01) | −0.24 (−0.55–0.29) | −3.07% (−3.55–2.59) |
| Oceania | 0.9 (0.58–1.2) | −0.19 (−0.22–0.16) | 108.72 (52.51–219.73) | 0.62 (−4.47–5.98) | 92.41 (41.29–182.94) | 2.01% (−2.69–6.94) |
| Central Sub-Saharan Africa | 1.5 (1.42–1.59) | 0.04 (0.03–0.04) | −0.59 (−0.74–0.37) | −4.65 (−4.95–4.36) | −0.6 (−0.73–0.4) | −5.02% (−5.3–4.74) |
| Eastern Sub-Saharan Africa | 1.21 (1.16–1.26) | −0.07 (−0.1–0.03) | −0.66 (−0.78–0.48) | −5.54 (−5.73–5.34) | −0.7 (−0.81–0.52) | −6.19% (−6.36–6.03) |
| Southern Sub-Saharan Africa | 0.45 (0.36–0.58) | −0.05 (−0.07–0.03) | −0.48 (−0.74–0.02) | −3.8 (−4.24–3.35) | −0.58 (−0.8–0.07) | −4.27% (−4.72–3.82) |
| Western Sub-Saharan Africa | 1.52 (1.46–1.58) | 0.12 (0.1–0.14) | −0.46 (−0.71–0.03) | −4.2 (−4.29–4.11) | −0.45 (−0.72–0.02) | −4.31% (−4.39–4.23) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tian, T.; Miao, L.; Wang, W.; Zhou, X. Global, Regional and National Burden of Human Cystic Echinococcosis from 1990 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Trop. Med. Infect. Dis. 2024, 9, 87. https://doi.org/10.3390/tropicalmed9040087
Tian T, Miao L, Wang W, Zhou X. Global, Regional and National Burden of Human Cystic Echinococcosis from 1990 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Tropical Medicine and Infectious Disease. 2024; 9(4):87. https://doi.org/10.3390/tropicalmed9040087
Chicago/Turabian StyleTian, Tian, Liyuan Miao, Wei Wang, and Xiaonong Zhou. 2024. "Global, Regional and National Burden of Human Cystic Echinococcosis from 1990 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019" Tropical Medicine and Infectious Disease 9, no. 4: 87. https://doi.org/10.3390/tropicalmed9040087
APA StyleTian, T., Miao, L., Wang, W., & Zhou, X. (2024). Global, Regional and National Burden of Human Cystic Echinococcosis from 1990 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Tropical Medicine and Infectious Disease, 9(4), 87. https://doi.org/10.3390/tropicalmed9040087