Abstract
There is a critical need to establish reference response rates following bladder-sparing therapies administered in the setting of bacillus Calmete-Guerin (BCG)-unresponsive non–muscle-invasive bladder cancer (NMIBC). We sought to determine the efficacy of different interventions in recent trials accruing patients fulfilling the strict BCG-unresponsive definition established by the US Food and Drug Administration. We performed a systematic review and meta-analysis for clinical trials in the BCG-unresponsive disease space to include published and presented results. The primary endpoints were complete response rate for CIS±Ta/T1 tumors, recurrence-free rate for patients with papillary-only disease, and disease-free rate in studies enrolling both papillary CIS tumors (Ta/T1/CIS). I2 was used for assessing heterogeneity. Eleven studies using 9 different therapeutic agents in a total of 909 patients with BCG-unresponsive NMIBC were identified. The resulting outcomes at 3, 6, and 12 months were 44%, 38%, and 25% complete response rate in CIS±Ta/T1 tumors; 73%, 58%, and 48% recurrence-free rate in papillary-only; and 48%, 22%, and 43% disease-free rate in combined Ta/T1/CIS, respectively. Relatively low levels of heterogeneity were observed amongst studies restricted to papillary-only or CIS±Ta/T1 tumors. Future randomized controlled studies are needed and will likely require stratification between papillary-only and CIS±Ta/T1 tumors.
Introduction
The decision of the United States Food and Drug Administration (FDA) to accept single-arm phase II/III clinical trials of novel agents for the treatment of BCG-unresponsive non–muscle-invasive bladder cancer (NMIBC) in tumors with CIS emphasizes the importance of reference efficacy rates to help frame the decision for approval. A previous systematic review that aimed to provide such reference benchmarks uncovered significant heterogeneity in patients enrolled in previous NMIBC clinical trials regarding the number and timing of intravesical BCG instillation and the pathology of the subsequent recurrent tumor[1]. One method to circumvent these barriers is to homogenize the study population by using the standard BCG-unresponsive definition adopted by the FDA in clinical trial design[2]. Results from recent trials enrolling such patients will provide context for the interpretation of emerging data from ongoing clinical trials conducted in the BCG-unresponsive space.
Methods
We performed a systematic review and meta-analysis in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement recommendations. An updated search was performed using the previously published protocol (PROSPERO CRD42019130553)[1]. Full search protocol, study review methodology, risk of bias assessment, and data synthesis are presented in Supplementary Materials (siuj.org). We included unpublished studies from phase II-III clinical trials presented at national urologic/oncology conferences that strictly accrued patients with BCG-unresponsive disease. The primary endpoints were complete response rate (CRR) for CIS±Ta/T1 tumors, recurrence-free rate (RFR) for patients with papillary-only disease, and disease-free rate (DFR) in studies enrolling both papillary (Ta/T1) and CIS-containing patients as previously described (Ta/T1/CIS)[1,2]. We performed a meta-analysis of proportions with command metaprop and inverse method with logit transformed proportions and senstivity analysis. Information was pooled with a random effect meta-analysis according to the heterogeneity expected. I2 was used for assessing heterogeneity.
Results
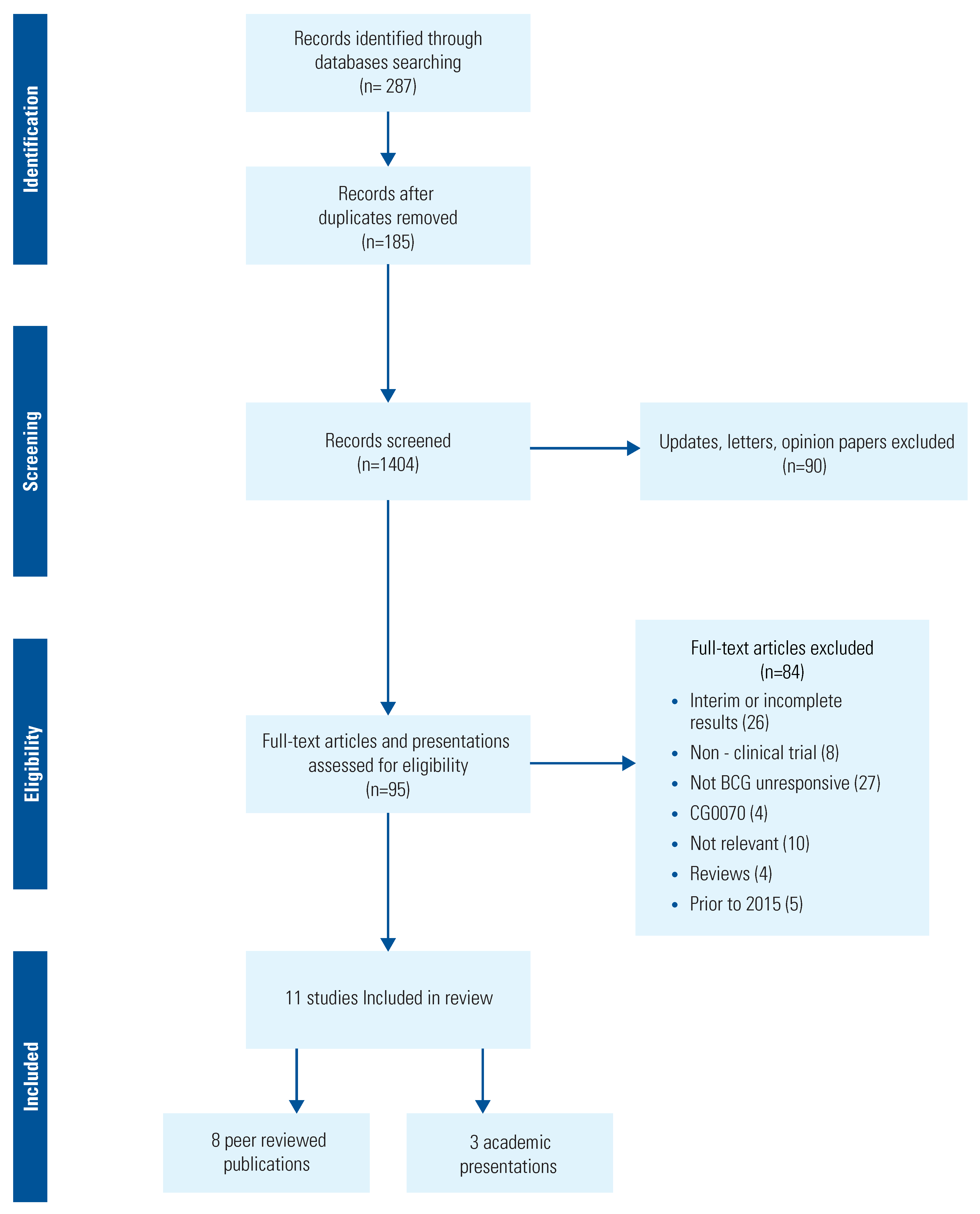
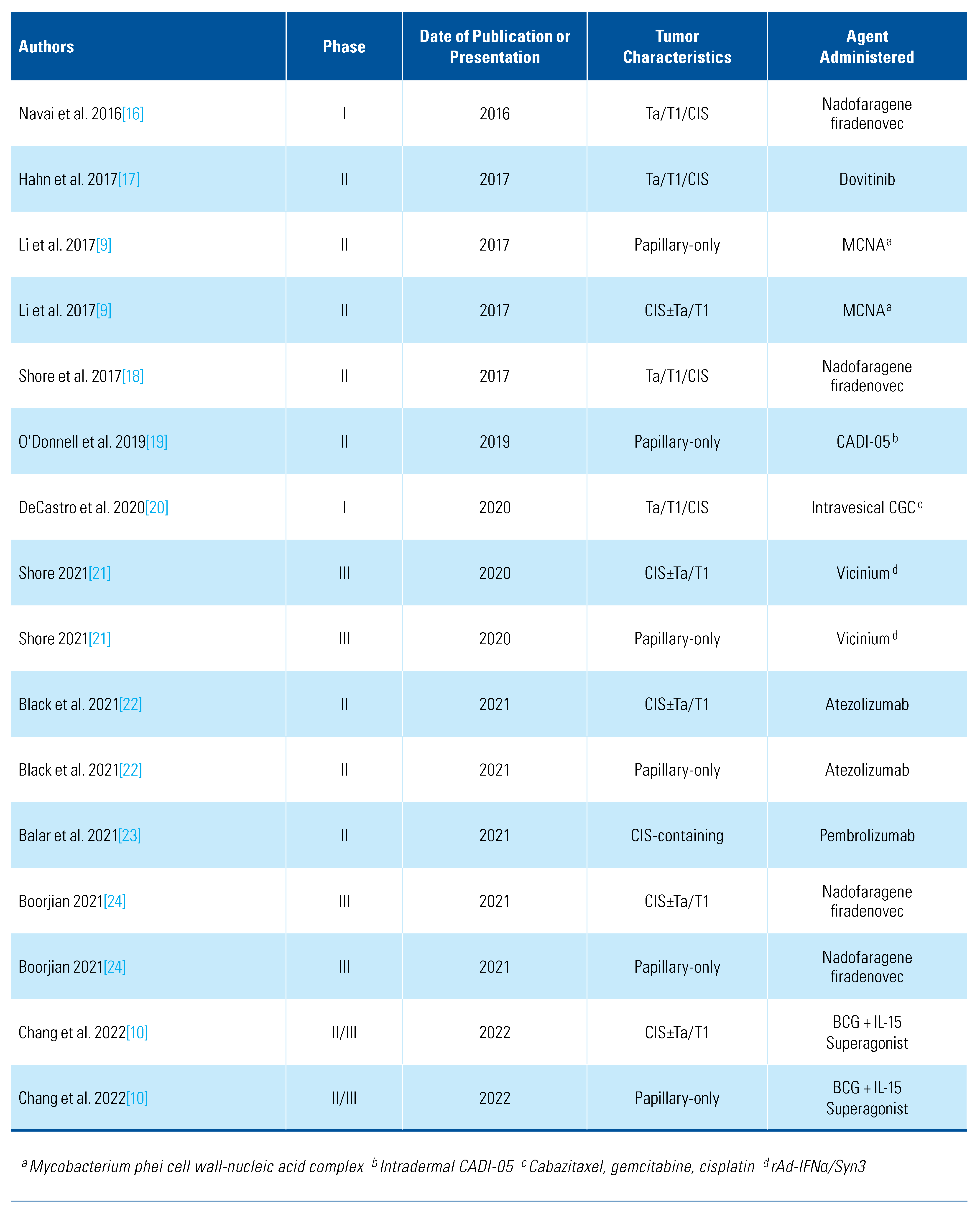
The initial search yielded 287 studies. After screening, 11 relevant studies were selected for analysis (Figure 1). Six studies were excluded in total. Four studies performed before the establishment of the BCG-unresponsive definition in 2015 were excluded as they enrolled patients with low-grade recurrences following BCG [3,4,5,6]. Another trial using CG0070 was excluded because of incomplete reporting[7]. One study was excluded because of the inclusion of BCG-intolerant patients rather than strictly those with BCG-unresponsive disease[8]. Studies with cohorts consisting of CIS- CIS±Ta/T1 tumors and papillary-only disease were analyzed separately, as previously described[9]. The included studies used 9 different therapeutic agents in a total of 909 patients with BCG-unresponsive NMIBC (Table 1). Of the reported study arms, 6 enrolled CIS±Ta/T1 tumors, 6 papillary-only tumors, and 4 Ta/T1/CIS tumors conjointly.
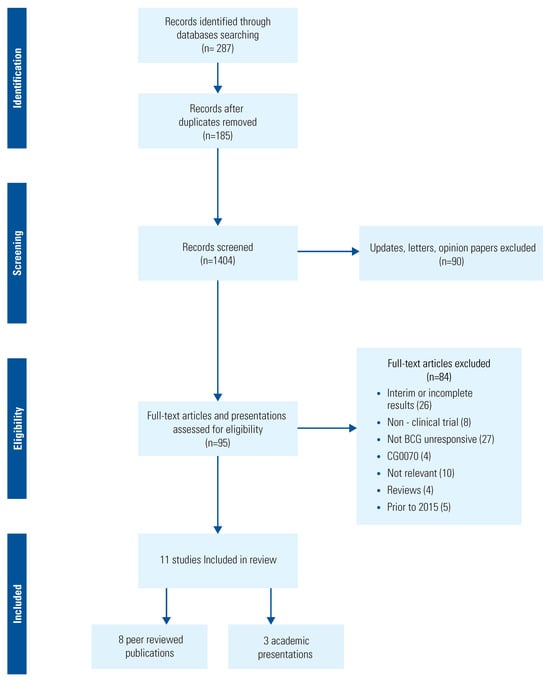
Figure 1.
Flow diagram of literature review for BCG-unresponsive non-muscle-invasive bladder cancer studies.

Table 1.
Presentations and publications in BCG-unresponsive NMIBC.
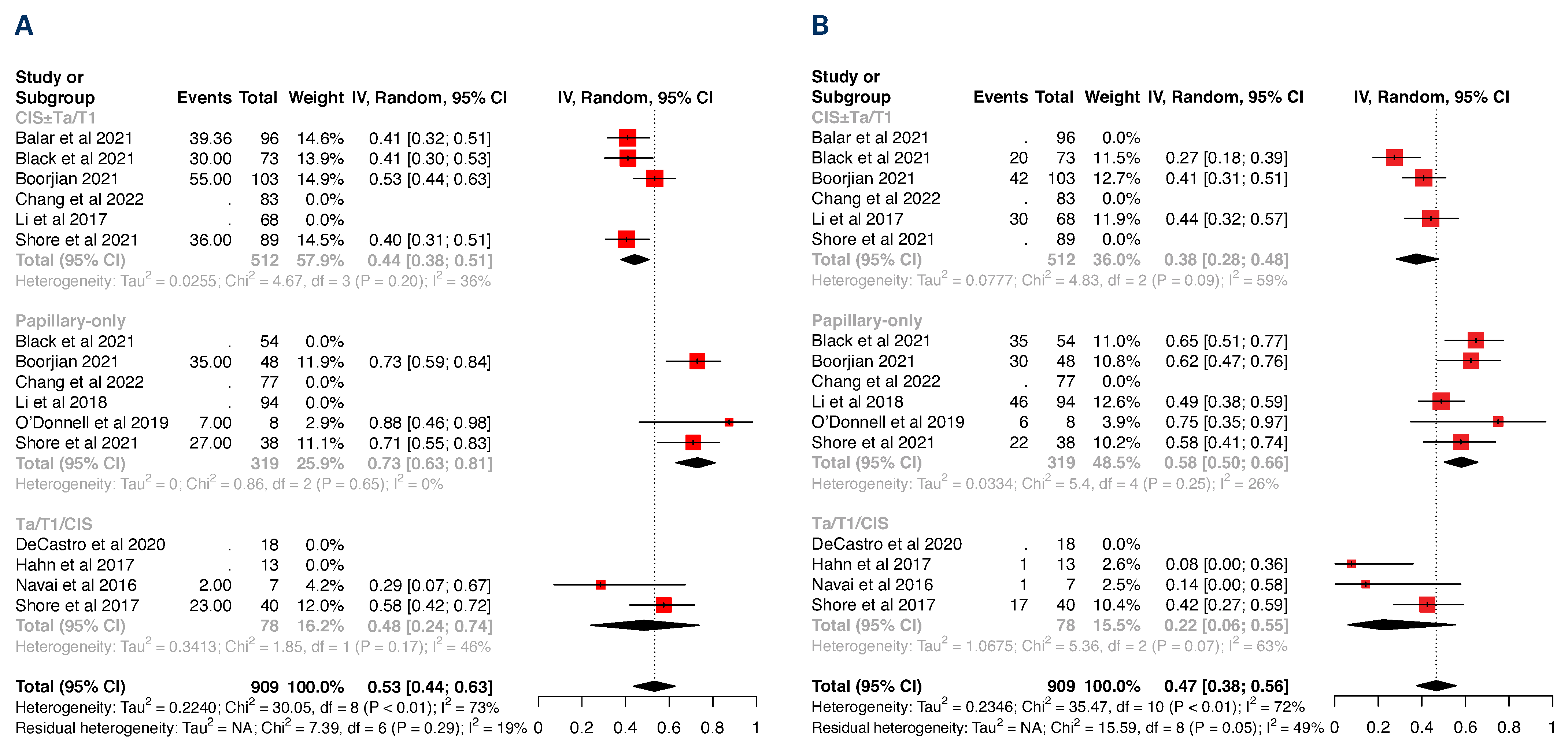
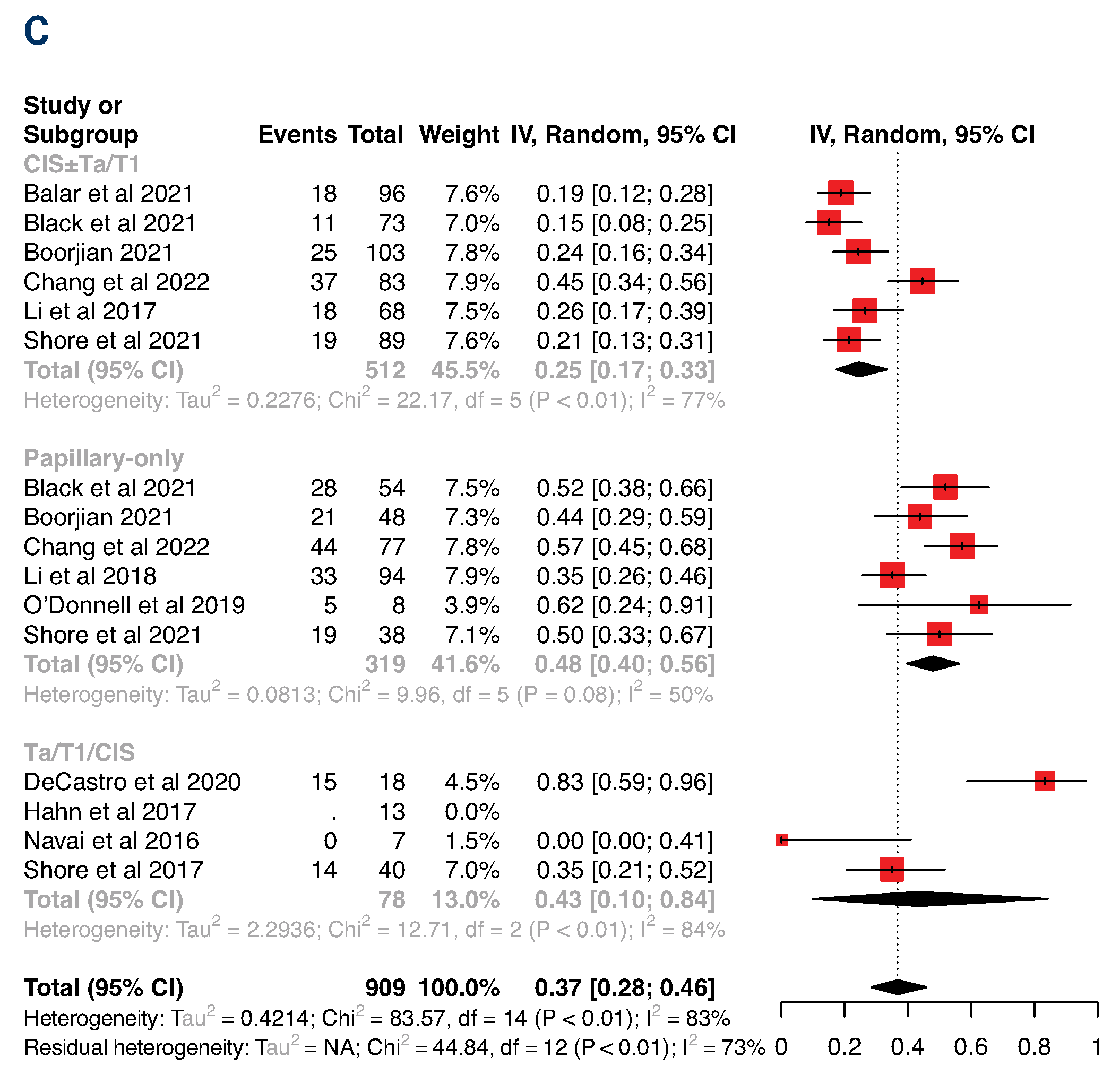
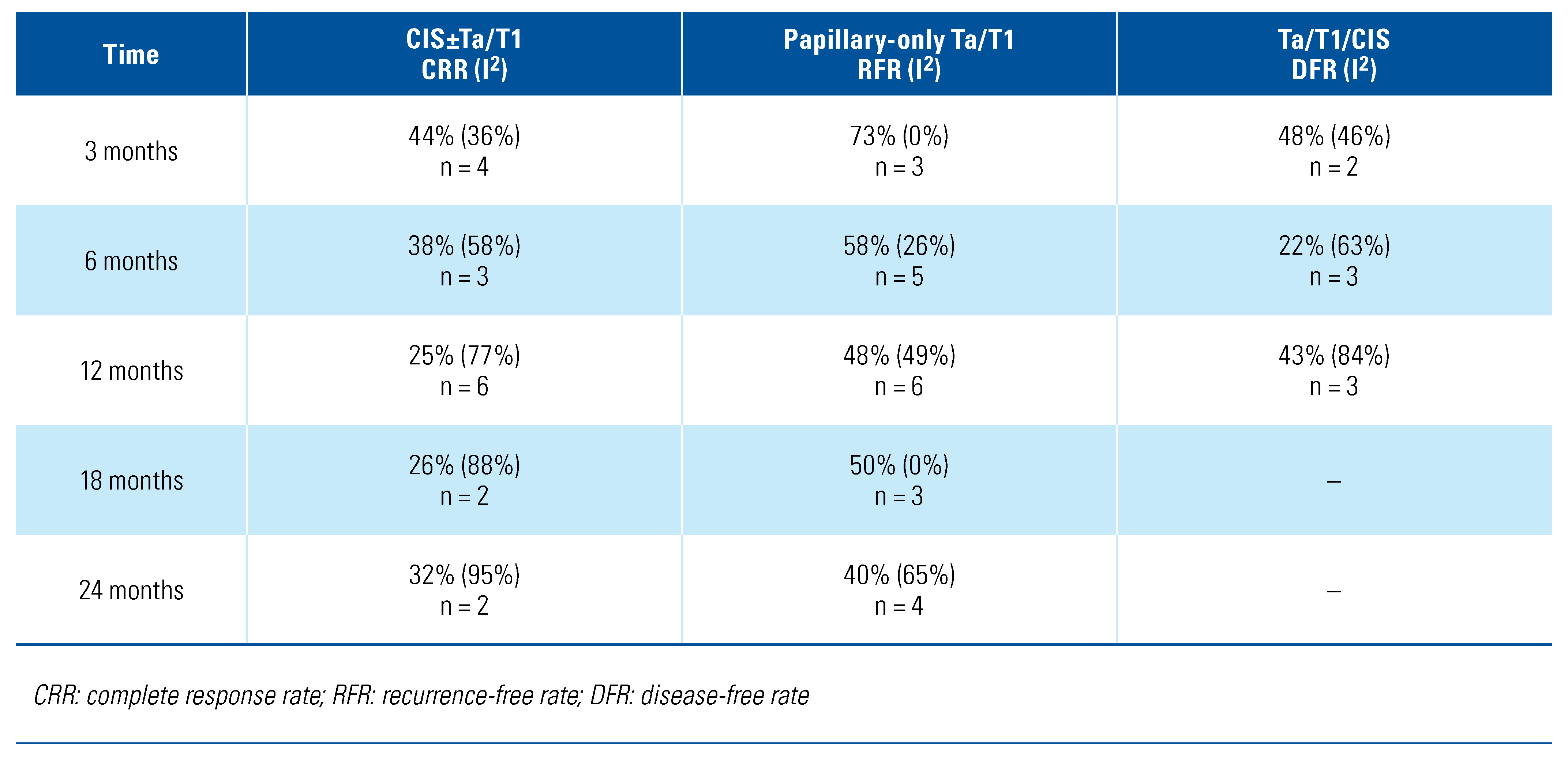
The primary endpoints for CIS±Ta/T1, Ta/T1, and Ta/T1/CIS are listed by timepoints following therapy in Table 2 and illustrated in the forest plots in Figure 2. Only the durable 12-month CRR from QUILT 3.032 study[10] was used in the meta-analysis as this was the only timepoint unequivocally reported. By limiting the analysis to studies enrolling patients fulfilling the BCG-unresponsive definition, we found more uniform but divergent response rates within the CIS±Ta/T1 and papillary-only cohorts, with 3-month, 6-month, and 12-month benchmarks that can help to inform emerging data from ongoing studies. The only deviation was the 12-month CRR of 44% reported in the QUILT 3.032[10], increasing the over- all 12-month CRR from 21% to 25% and the I2 from 0% to 77% (Figure 2). In contrast, results from studies conglomerating durable response rates between the 2 cohorts were marked by higher heterogeneity, supporting the differential responsiveness to bladder-sparing treatment between CIS±Ta/T1 and papillary-only NMIBC. These results may reflect different molecular pathways leading to the development of CIS (originating from chromosome 9p+q loss and TP53 and RB mutations) and papillary tumors (originating from FGFR alterations and 9q loss)[11]. Alternatively, diver- gent response and recurrence rates likely also reflect the fact that papillary tumors are amenable to complete trans- urethral resection but CIS usually is not[12].
Table 2.
Meta-analysis results by tumor characteristic and months following administration.
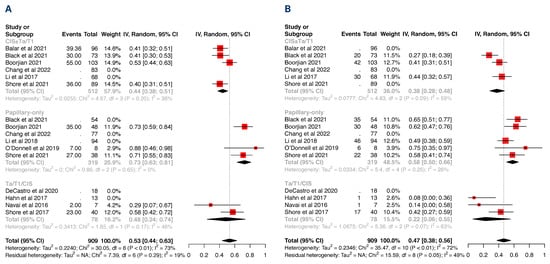
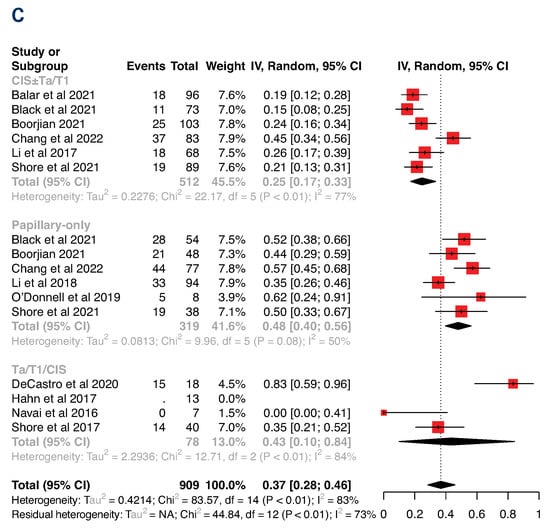
Figure 2.
Forest plots of response rates from meta-analysis, stratified by tumor characteristic at 3 months (A), 6 months (B), and 12 months (C).
The lack of uniformity amongst trial results further underscores differences in the mechanisms of action between the investigational agents and indicate differences therapeutic efficacy. To further eliminate risks of bias and increase the rigor of the analysis, randomized controlled trials (RCT) are likely required in the future. As there is no universally accepted bladder-preserving therapy for BCG-unresponsive NMIBC, there is a need to standardize treatment used in the control arm. Recent FDA approval suggests pembrolizumab is an option; however, many consider its efficacy insufficient to offset the observed toxicity profile and the significant cost[13]. Intravesical gemcitabine/docetaxel has also been proposed as an alternative by some on the basis of “expert opinion,” although its efficacy has not yet been established in prospective clinical trials. Moreover, shortages of BCG in many countries have hampered administration according to the SWOG protocol, limiting the number of patients fulfilling the BCG-unresponsive definition and creating a bottleneck for completing RCTs in this disease setting.
This is the first meta-analysis to investigate the available studies that meet the strict definition of the BCG-unresponsive NMIBC definition adopted by the FDA in 2018[2]. Our results demonstrate a weighted average CRR of 38% at 6 months and 25% at 12 months in CIS±Ta/T1 BCG-unresponsive NMIBC. Of all completed trials, only one[10] achieved the 50% 6-month and 30% 12-month thresholds previously proposed to be clinically relevant[14,15] Notably, CRRs observed in trials using the 2 currently FDA-approved agents, pembrolizumab and valrubicin, fell short of these benchmarks regarding the 12-month duration of response. Several agents tested in similarly designed single-arm trials are currently under review by the FDA and have reported CRR rates and 12-month durability that meet or exceed this bar. With the emerging data from recently completed and ongoing clinical trials, the CRR and durability threshold required for approval, particularly for patients with CIS, remains a moving target. If one or more new drugs receive FDA approval, this will provide clarity around these endpoints.
Limitations of our study include a relatively low sample size of studies using a variety of different treatment agents. Additionally, variability in study protocols allowing for therapeutic re-induction following initial non-response and/or mandating post-therapy random bladder biopsy may affect response rates seen. Lastly, it is difficult to determine whether adjudication between CIS±Ta/T1 and papillary-only tumors was performed by central review in all included studies. Despite the heterogeneity in the treatment agents used, we were successful in delineating a relatively narrow range of response rates at clinically relevant timepoints stratified by tumor stage to provide a frame-of-reference for emerging results from ongoing BCG-unresponsive clinical trials.
Conclusion
Our study indicates relatively uniform but disparate response rates to bladder-sparing therapies in BCG-unresponsive CIS±Ta/T1 and papillary-only NMIBC. To reduce risks of bias, randomized controlled studies with appropriate stratification of the 2 disease entities are likely to be required in the future. Consensus is also needed on the ideal therapeutic agent to be used in the control arm. Our results will help to formulate designs of future clinical trials and inform the interpretation of emerging data in this exciting treatment space.
Supplementary Materials
The following are available online at https://www.mdpi.com/2563-6499/3/5/333/s1.
Competing Interests
None declared.
References
- Li, R.; Sundi, D.; Zhang, J.; Kim, Y.; Sylvester, R.J.; Spiess, P.E.; et al. Systematic review of the therapeutic efficacy of bladder-preserving treatments for non-muscle-invasive bladder cancer following intravesical bacillus Calmette-Guerin. Eur. Urol. 2020, 78, 387–399. [Google Scholar] [CrossRef] [PubMed]
- United States Food and Drug Administration. BCG-unresponsive nonmuscle invasive bladder cancer: Developing drugs and biologics for treatment guidance for industry; 2018; pp. 1–10. [Google Scholar]
- Gacci, M.; Bartoletti, R.; Cai, T.; Nerozzi, S.; Pinzi, N.; Repetti, F.; et al. Intravesical gemcitabine in BCG-refractory T1G3 transitional cell carcinoma of the bladder: A pilot study. Urol. Int. 2006, 76, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Gunelli, R.; Bercovich, E.; Nanni, O.; Ballardini, M.; Frassineti, G.L.; Giovannini, N.; et al. Activity of endovesical gemcitabine in BCG-refractory bladder cancer patients: A translational study. Br. J. Cancer 2007, 97, 1499–1504. [Google Scholar] [PubMed]
- Perdona, S.; Di Lorenzo, G.; Cantiello, F.; Damiano, R.; De Sio, M.; Masala, D.; et al. Is gemcitabine an option in BCG-refractory nonmuscle- invasive bladder cancer? A single-arm prospective trial. Anticancer. Drugs 2010, 21, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Skinner, E.C.; Goldman, B.; Sakr, W.A.; Petrylak, D.P.; Lenz, H.J.; Lee, C.T.; et al. SWOG S0353: Phase II trial of intravesical gemcitabine in patients with nonmuscle invasive bladder cancer and recurrence after 2 prior courses of intravesical bacillus Calmette-Guerin. J. Urol. 2013, 190, 1200–1204. [Google Scholar] [CrossRef] [PubMed]
- Packiam, V.T.; Lamm, D.L.; Barocas, D.A.; Trainer, A.; Fand, B.; Davis, R.L., 3rd; et al. An open label, single-arm, phase II multicenter study of the safety and efficacy of CG0070 oncolytic vector regimen in patients with BCG-unresponsive non-muscle-invasive bladder cancer: Interim results. Urol. Oncol. 2018, 36, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Hurle, R.G.G.; Colombo, P.; Santoro, A.; De Cobelli, O.; Trapani, E.; Nohales, G.; Llorente, C.; Duran-Merino, R.; Lazzeri, M. Editor Oncofid-P-B for the treatment of BCG unresponsive carcinoma in situ (CIS) of the bladder: Preliminary results of European multicentre phase 1 study at the end of 12 consecutive weeks intensive course and during ongoing monthly maintenance phase. American Urologic Association; 2020. J. Urol. 2020. [Google Scholar]
- Li, R.; Amrhein, J.; Cohen, Z.; Champagne, M.; Kamat, A.M. Efficacy of mycobacterium phlei cell wall-nucleic acid complex (MCNA) in BCG-unresponsive patients. Bladder Cancer 2017, 3, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.S.; Chamie, K.; Gonzalgo, M.L.; Kramolowsky, E.V.; Sexton, W.J.; Reddy, S.K.; et al. Positive efficacy and safety phase 3 results in both CIS and papillary cohorts BCG-unresponsive nonmuscle invasive bladder cancer (NMIBC) after IL-15RαFc superagonist N-803 (Anktiva) and BCG infusion. J. Clin. Oncol. 2022, 40 (Suppl. 6), 431. [Google Scholar] [CrossRef]
- Knowles, M.A.; Hurst, C.D. Molecular biology of bladder cancer: New insights into pathogenesis and clinical diversity. Nat. Rev. Cancer 2015, 15, 25–41. [Google Scholar] [CrossRef]
- Dalbagni, G. The management of superficial bladder cancer. Nat. Clin. Pract. Urol. 2007, 4, 254–260. [Google Scholar] [CrossRef]
- Wymer, K.M.; Sharma, V.; Saigal, C.S.; Chamie, K.; Litwin, M.S.; Packiam, V.T.; et al. Cost-effectiveness analysis of pembrolizumab for bacillus Calmette-Guerin-unresponsive carcinoma in situ of the bladder. J. Urol. 2021, 205, 1326–1335. [Google Scholar] [CrossRef]
- Jarow, J.P.; Lerner, S.P.; Kluetz, P.G.; Liu, K.; Sridhara, R.; Bajorin, D.; et al. Clinical trial design for the development of new therapies for nonmuscle-invasive bladder cancer: Report of a Food and Drug Administration and American Urological Association public workshop. Urology 2014, 83, 262–264. [Google Scholar] [CrossRef]
- Kamat, A.M.; Sylvester, R.J.; Bohle, A.; Palou, J.; Lamm, D.L.; Brausi, M.; et al. Definitions, end points, and clinical trial designs for non-muscle- invasive bladder cancer: Recommendations from the International Bladder Cancer Group. J. Clin. Oncol. 2016, 34, 1935–1944. [Google Scholar] [CrossRef]
- Navai, N.; Benedict, W.F.; Zhang, G.; Abraham, A.; Ainslie, N.; Shah, J.B.; et al. Phase 1b trial to evaluate tissue response to a second dose of intravesical recombinant adenoviral interferon alpha2b formulated in syn3 for failures of bacillus Calmette-Guerin (BCG) therapy in nonmuscle invasive bladder cancer. Ann Surg Oncol. 2016, 23, 4110–4114. [Google Scholar]
- Hahn, N.M.; Bivalacqua, T.J.; Ross, A.E.; Netto, G.J.; Baras, A.; Park, J.C.; et al. A phase II trial of dovitinib in BCG-unresponsive urothelial carcinoma with FGFR3 mutations or overexpression: Hoosier Cancer Research Network Trial HCRN 12-157. Clin. Cancer Res. 2017, 23, 3003–3011. [Google Scholar] [CrossRef]
- Shore, N.D.; Boorjian, S.A.; Canter, D.J.; Ogan, K.; Karsh, L.I.; Downs, T.M.; et al. Intravesical rAd-IFNalpha/Syn3 for patients with high-grade, bacillus Calmette-Guerin-refractory or relapsed non-muscle-invasive bladder cancer: A phase II randomized study. J. Clin. Oncol. 2017, 35, 3410–3416. [Google Scholar] [CrossRef]
- O’Donnell, M.A.; Singh, S.; Sood, R.; Amlani, J.; Krishnamoorthy, H.; Shukla, K.; et al. A clinical trial of the intradermal TLR2 agonist CADI-05 for BCG recurrent and unresponsive non-muscle invasive bladder cancer. Bladder Cancer 2019, 5, 171–180. [Google Scholar] [CrossRef]
- DeCastro, G.J.; Sui, W.; Pak, J.S.; Lee, S.M.; Holder, D.; Kates, M.M.; et al. A phase I trial of intravesical cabazitaxel, gemcitabine and cisplatin for the treatment of nonmuscle invasive bacillus Calmette-Guerin unresponsive or recurrent/relapsing urothelial carcinoma of the bladder. J. Urol. 2020, 204, 247–253. [Google Scholar] [CrossRef]
- Shore, N.D. (Ed.) Phase 3 results of vicinium in BCG-unresponsive non-muscle invasive bladder cancer. In Proceedings of the American Urologic Association Annual Meeting, Virtual, June 2020. [Google Scholar]
- Black, P.C.; Tangen, C.M.; Singh, P.; McConkey, D.J.; Lucia, S.; Lowrance, W.T.; et al. Phase II trial of atezolizumab in BCG-unresponsive non-muscle invasive bladder cancer: SWOG S1605 (NCT #02844816). J. Clin. Oncol. 2021, 39 (Suppl. 15), 4541. [Google Scholar]
- Balar, A.V.; Kamat, A.M.; Kulkarni, G.S.; Uchio, E.M.; Boormans, J.L.; Roumiguie, M.; et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): An open-label, single-arm, multicentre, phase 2 study. Lancet Oncol. 2021, 22, 919–930. [Google Scholar] [CrossRef]
- Boorjian, S.A.; Alemozaffar, M.; Konety, B.R.; Shore, N.D.; Gomella, L.G.; Kamat, A.M.; et al. Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: A single-arm, open-label, repeat-dose clinical trial. Lancet Oncol. 2021, 22, 107–117. [Google Scholar] [CrossRef]
This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2022 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.